



Introduction
Non-small-cell lung carcinoma (NSCLC) is the most common type of lung cancer (LC), which accounts for 85% of all lung cancer cases [1–3]. Surgery is the prior treatment for early-stage NSCLC patients. However, nearly 75% patients are in advanced stages when they are first diagnosed. The National Comprehensive Cancer Network (NCCN) [4] guideline recommend tyrosine-kinase inhibitor (TKI) therapy to patients with EGFR mutation. All NSCLCs today are divided according to EGFR status positive and negative as shown by EGFR and polymorphisms having significance [5–7]. Immunotherapy (IO) is applied for EGFR negatives. Several studies, such as KEYNOTE 024, IMpower110, EMPOWER-Lung1, KEYNOTE189, KEYNOTE 407, have shown that IO not only could prolong the PFS, but also could improve the OS [8–12]. However, patients with EGFR mutation who treated with IO had limited efficacy. Previous meta-analysis study showed that IO did not benefit patients with EGFR mutation, but increased adverse reactions [13]. And the latest phase II single arm trial had been ended early because of lacking significant clinical efficacy [14]. The efficacy of adding IO to the treatment of patients with EGFR mutation in advanced NSCLC is still controversial.
Whether IO should be added to the regimen of advanced NSCLC with EGFR mutated remains unclear. It is also unclear why adding IO to advanced NSCLC with EGFR mutated decreases the efficacy of treatment. It may be related to the immune microenvironment. Hyperthermia is an effective measure to overcome tumor hypoxic cells, and it mainly kills the S phase cells, which were resistant to radiotherapy. Moreover, it can reduced the production of immunosuppressive cells. Guo et al. [15] found that hyperthermia could transform Treg cells into Th17 cells by increasing IL-6 levels. Wendt MK [16] found hyperthermia could also indirectly reduce TGF-β by up-regulating the expression of miR-10b to inhibit breast cancer cell proliferation. Guo et al. [17] found hyperthermia could not only activate Cytotoxic T lymphocyte (CTL) by increasing the expression of B7 molecules and ICAM-1, but it could also increase CD+4 /CD+8 ratio. Therefore, hyperthermia can improve the tumor microenvironment (TME), and promote the efficacy of IO in advanced NSCLC.
On the basis of these theories, we hypothesis that patients with EGFR mutation may not benefit from hyperthermia. Our study aims to explore the prognosis of adding hyperthermia to the treatment of advanced NSCLC with different EGFR mutated states and evaluate the efficacy of adding hyperthermia as the first-line treatment method or as a posterior-line method.
Results
Characteristics of patients
The median follow-up was 22 months. A total of 205 patients were included the study. Among the 205 III-IV NSCLC patients, 77 patients in the hyperthermia group and 128 patients in the non- hyperthermia group. The baseline characteristics of the two groups were shown in Table 1. There were 162(79.1%) cases of adenocarcinoma (AC) and 43(20.9%) cases of squamous cell carcinoma (SCC); among them, there were 63(30.7%) patients in stage III, whereas 142(69.3%) patients in stage IV. There were 69(33.7%) patients with EGFR mutation and 136(66.3%) patients in EGFR wild-type or undetected genes or other mutated gene.
Table 1. Baseline characteristics of hyperthermia group and non- hyperthermia group.
| Characteristic | Hyperthermia group (N=77) | Non- hyperthermia group (N=128) | P value |
| Gender | 0.419 | ||
| Male | 53(68.8%) | 81(63.3%) | |
| Female | 24(31.2%) | 47(36.7%) | |
| Age | 0.812 | ||
| <60 | 35(45.5%) | 56(43.7%) | |
| ≥60 | 42(54.5%) | 72(56.3%) | |
| Smoke | 0.302 | ||
| YES | 32(41.6%) | 44(34.4%) | |
| NO | 45(58.4%) | 84(65.6%) | |
| ECOG score | 0.137 | ||
| ≤1 | 75(97.4%) | 117(91.4%) | |
| >1 | 2(2.6%) | 11(8.6%) | |
| Pathology | 0.376 | ||
| adenocarcinoma | 58(75.3%) | 104(81.3%) | |
| squamous carcinoma | 19(24.7%) | 24(18.7%) | |
| Stage | 0.175 | ||
| III | 28(36.4%) | 35(27.3%) | |
| IV | 49(63.6%) | 93(72.7%) | |
| EGFR mutation state | 0.879 | ||
| EGFR mutation | 25(32.5%) | 44(34.4%) | |
| EGFR no mutation or others | 52(67.5%) | 84(65.6%) | |
| Treatment | 0.286 | ||
| combined treatment without EGFR-TKI | 55(71.4%) | 81(63.3%) | |
| combined treatment with EGFR-TKI | 22(28.6%) | 47(36.7%) |
Failure patients
Up to September 2021, there were 29 patients (14.1%) lost to follow-up. Twenty-six patients (33.8%) died, 16 patients (20.8%) encountered recurrences, 14 patients (18.2%) occurred distant metastasis and 7 patients (9.1%) encountered recurrences and distant metastasis in hyperthermia group. In terms of non- hyperthermia group, 81 (63.3%)of 128 patients died,52(40.6%) of 128 patients were relapsed, 16(12.5%) of 128 patients had distant metastasis and 24(18.8%) of 128 patients encountered recurrences and distant metastasis (Table 2).
Table 2. Failure patients of two group.
| No. of patients(%) | ||
| Pattern of failures | Hyperthermia group (77) | Non- hyperthermia group (128) |
| Died | 26(33.8%) | 81(63.3%) |
| Relapsed | 16(20.8%) | 52(40.6%) |
| Distant metastasis | 14(18.2%) | 16(12.5%) |
| Relapsed and distant metastasis | 7(9.1%) | 24(18.8%) |
The outcomes of survival
The 1-year OS and PFSfirst rates of hyperthermia group and non- hyperthermia group were 83.3% versus 71.5% (P=0.010, Figure 1A) and 62.0% versus 42.7% (P=0.001, Figure 1B).
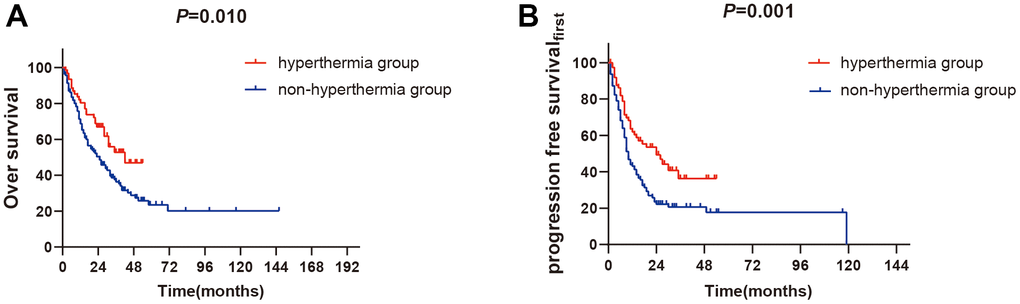
Figure 1. The outcomes of survival between hyperthermia group and non-hyperthermia group. (A) 1-year OS rates between two groups (P<0.05). (B) 1-year PFSfirst rates between two groups (P<0.01).
Subgroups analysis
The subgroups analyses have shown that the 1-year OS rate in hyperthermia group and in non- hyperthermia group was 79.1% versus 65.2% (P=0.037, Figure 2A) in the non- EGFR mutant subset, while the 1-year PFSfirst rate in hyperthermia group and non- hyperthermia group were 64.2% versus 36.5% (P=0.001, Figure 2B). The outcomes had significant difference between the two groups.
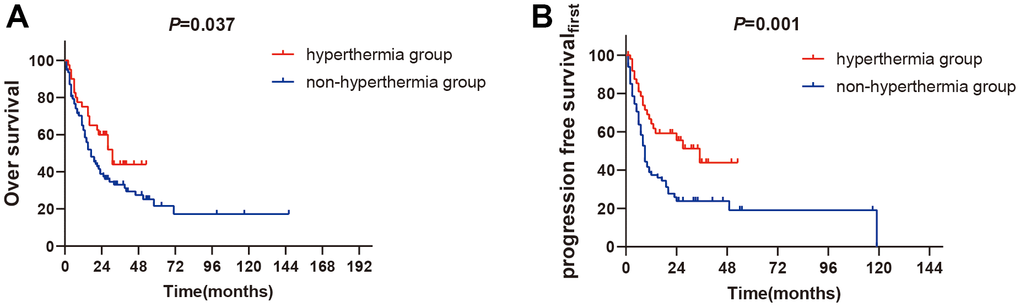
Figure 2. The subgroups analysis of non-EGFR mutation between two groups. (A) 1-year OS rates of non-EGFR mutation between two groups (P<0.05). (B) 1-year PFSfirst rates of non-EGFR mutation between two groups (P<0.01).
For patients with EGFR mutation, the 1-year OS and PFSfirst rates did not significantly differ between the two groups (the 1-year OS rate: 91.7% vs. 83.5%, P=0.094, Figure 3A. the 1-year PFSfirst rate: 57.9% vs. 53.8%, P=0.190, Figure 3B).
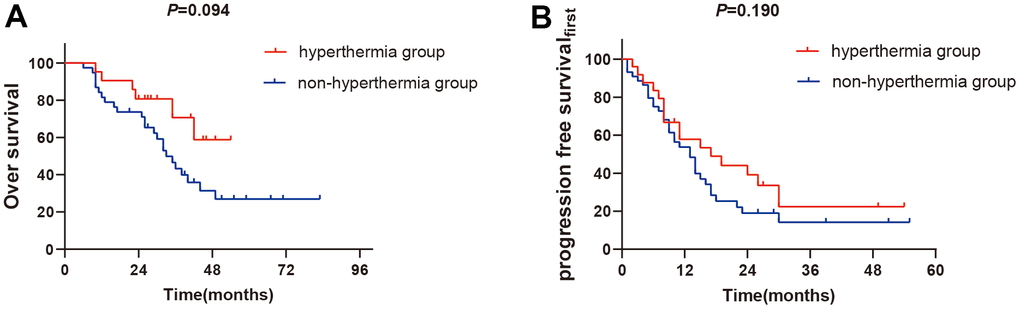
Figure 3. The subgroups analysis of EGFR mutation between two groups. (A) 1-year OS rates of EGFR mutation between two groups (P>0.05). (B) 1-year PFSfirst rates of EGFR mutation between two groups (P>0.05).
Prognostic factors
Multivariate Cox regression analysis demonstrated that smoke, clinical stage and hyperthermia were the independent prognostic factors for PFSfirst and OS (Tables 3, 4).
Table 3. Multivariate analysis of progression-free survival.
| Variable | Hazard ration | 95% CI | P value |
| Gender | 1.039 | 0.648-1.666 | 0.875 |
| Age | 0.863 | 0.601-1.238 | 0.423 |
| Smoke | 0.497 | 0.312-0.790 | 0.003 |
| Pathology | 1.116 | 0.684-1.820 | 0.660 |
| Stage | 0.355 | 0.226-0.557 | 0.000 |
| ECOG score | 1.084 | 0.494-2.382 | 0.840 |
| Hyperthermia | 1.940 | 1.291-2.914 | 0.001 |
| Target Therapy | 1.481 | 0.880-2.491 | 0.139 |
| Radiotherapy | 0.974 | 0.668-1.421 | 0.892 |
| Chemotherapy | 0.963 | 0.608-1.526 | 0.873 |
| EGFR mutation state | 0.739 | 0.469-1.162 | 0.190 |
Table 4. Multivariate analysis of overall survival.
| Variable | Hazard ration | 95% CI | P value |
| Gender | 0.752 | 0.448-1.263 | 0.281 |
| Age | 1.121 | 0.755-1.666 | 0.571 |
| Smoke | 0.583 | 0.359-0.947 | 0.029 |
| Pathology | 0.997 | 0.589-1.688 | 0.992 |
| Stage | 0.395 | 0.244-0.640 | 0.000 |
| ECOG score | 0.523 | 0.275-0.995 | 0.048 |
| hyperthermia | 1.671 | 1.036-2.693 | 0.035 |
| Targeted | 1.838 | 1.004-3.366 | 0.048 |
| Radiotherapy | 1.135 | 0.736-1.748 | 0.567 |
| Chemotherapy | 2.108 | 1.314-3.383 | 0.002 |
| EGFR mutation state | 1.706 | 0.986-2.954 | 0.056 |
Posterior-line analysis
Of patients who occurred progress and had not received hyperthermia in first-line treatment, twenty-nine patients were treated with hyperthermia as a posterior-line treatment method. Of the 29 patients, 12(41.4%) relapsed, 2 (6.9%) had distant metastasis and 6(20.7%) both had recurrences and distant metastasis. The median PFS were no significant difference between the first-line treatment and posterior-line treatment (24m VS 21m, P = 0.225, Figure 4).
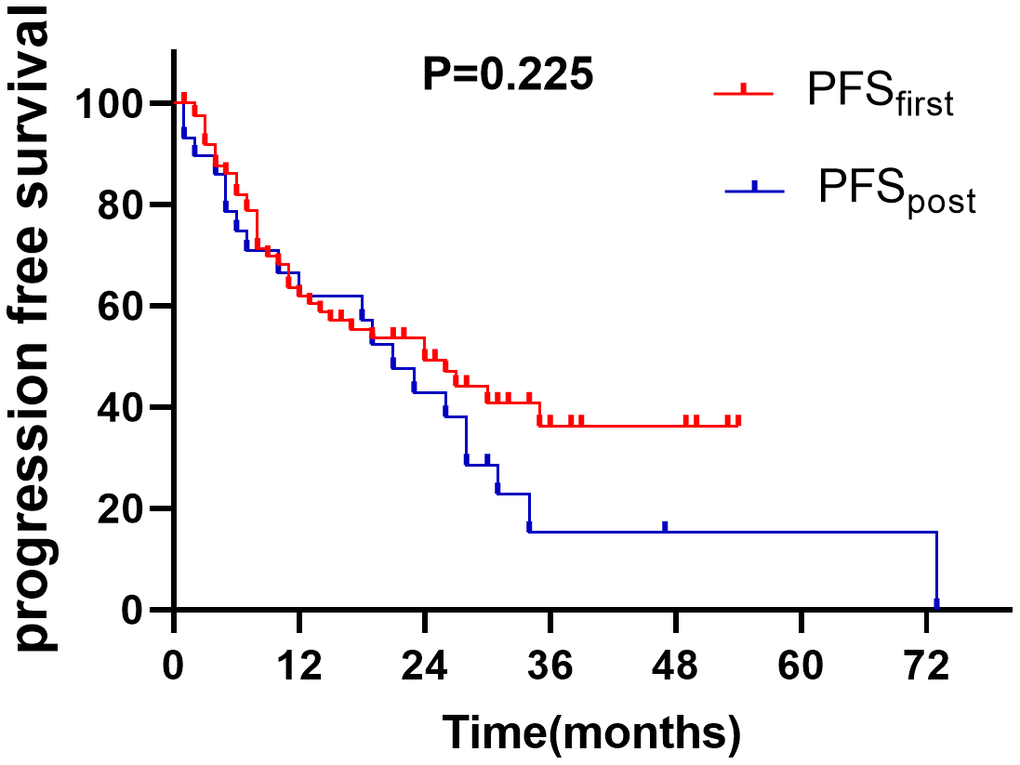
Figure 4. The PFS of adding hyperthermia in first-line and posterior-line treatment (P>0.05).
Discussion
The relationship between tumor stroma cells is very important and that certain cytokines play an important role in the relationship between tumor hosts [18]. This study compared the efficacy of adding hyperthermia to the current regimens or without hyperthermia in advanced NSCLC. Our results showed that patients who received hyperthermia had better PFSfirst and OS than those without hyperthermia. A retrospective study [19] showed that hyperthermia combined with RT had a better prognosis and did not increase side effects. The author found the objective response rate (ORR) and 3-year OS rates between two groups were 97% versus 70% and 37% versus 6.7%, retrospectively (P<0.05). Italian scholars [20] were the first to report that hyperthermia combined with Chemoradiotherapy in LC in 1998, the results demonstrated that stage IV patients who received hyperthermia had longer OS (13.2m vs 8.4m, P<0.01). However, the simple size was small and these studies were retrospective studies. A review showed hyperthermia could exert synergistic effect with other treatments [21], Which were similar to our study. The mechanisms of hyperthermia enhance the anticancer effects of radiotherapy are as below: 1. DNA double-strand breaks (DSB) are the most critical radiation-induced damage, which is the main cause of cell death. It can inhibit the repair of DSB in NSCLC cell line, promotes apoptosis and inhibits the invasion of tumor cells when radiotherapy combined with hyperthermia [22]. 2. Hyperthermia can ameliorate the TME such as low PH, hypoxia, and vascular immaturity through increases blood flow and perfusion [23]. 3. Cells in the S phase which are insensitive to radiotherapy, are sensitive to hyperthermia. Hyperthermia increases the effectiveness of chemotherapy by increasing the concentration of chemotherapy drugs, inhibiting DNA repair, increasing the release of free radicals, reversing the drug resistance of chemotherapy drugs and so on [24].
The subgroup analyses in our study revealed that patients didn’t have EGFR mutant who received hyperthermia had significantly higher 1 year OS and PFSfirst rates than those treated with non- hyperthermia (P=0.001). And for patients with EGFR mutation, there was no significant difference between the two groups. The results were consistent with our expected results. Microwave ablation (MWA) as another method of Heat therapies has been widely used in many malignant tumors [25–27]. Wei et al. [28] conducted a retrospective study on 61 NSCLC patients who were known EGFR status treated MWA combined with chemotherapy / EGFR-TKI. The results showed that the median PFS of EGFR mutant and wild-type patients were 8.3 months and 5.4 months respectively (P = 0.162), and the median OS were 17.8 months and 27.2 months (P = 0.209). The results showed that patients with EGFR mutation could not benefit from MWA, our findings were consistent with them. However, the sample size of that study was small and only compared the effects of MWA combine with other treatments based on different EGFR status. Therefore, they [29] further performed on 58 EGFR mutant patients, who treated with TKI with or without MWA. The results revealed that no significant difference in objective response rate (ORR), PFS and OS between the two groups (P=0.230, 0.640 and 0.288 respectively). As a result, they suggested that MWA should not be recommended for unselected patients with EGFR-sensitive mutations. Our study further explored the efficacy of adding hyperthermia for NSCLC patients with different EGFR states and our outcomes are consistent with the results of the above studies.
The reason why patients with EGFR mutation could not benefit from hyperthermia now is still unclear. We suppose hyperthermia had a positive effect on immune microenvironment as we described previously, and the special immune microenvironment in patients with EGFR mutation. Dong et al. [30] performed a pool-analysis of 3283 patients from 15 studies to systematically assessed the association between EGFR mutation and PD-L1 expression. They found that EGFR wild-type tumors were more likely to be PD-L1-positive than EGFR mutant tumors (OR: 1.79; 95% CI 1.10–2.93; P = 0.02). They analyzed the protein and mRNA profiles of PD-L1 in the repository (The Cancer Genome Atlas; TCGA) and internal (Guangdong Lung Cancer Institute; GLCI) databases and performed IHC detection of PD-L1 in resected NSCLC tissues found same results. What’s more, they explored the correlation between EGFR status and CD8+ T-cell infiltration. Analysis of mRNA profiles in the GLCI cohort indicated that patients with EGFR mutations had a lower CD8A expression than those with EGFR wild-type (P = 0.031). IHC analysis of CD8+ TILs in the 255 resected NSCLC specimens confirmed that EGFR mutant tumors showed lesser T-cell infiltration than EGFR wild-type ones (P = 0.003). They also found patients with sensitive EGFR mutation display low immunogenicity and show impaired response to PD-1 blockade. Eri Sugiyama et al. [31] have shown that tumor mutation burden (TMB) was decreased and regulatory T cells (Treg) was increased in EGFR-mutated lung adenocarcinomas (LUADs). Thus, we suspected low TMB, low tumor infiltrating lymphocytes (TILs) and high Treg in patients with EGFR mutation may resulted in poor efficacy of IO of them. Hyperthermia can promote the efficacy of IO in advanced NSCLC by improving the TME, which may lead to patients with EGFR mutation do not benefit from hyperthermia. But more basic researches should be carried out to clarify the mechanisms.
Moreover, our study also investigated the best time to add hyperthermia. The outcomes demonstrated that the PFSfirst in first-line and PFSpost in posterior-line was no significant difference between the entire groups. Takayuki Ohguri et al. [32] carried out a study to assess the efficacy of re-irradiation plus regional hyperthermia for 33 recurrent NSCLC patients, the results showed that the median disease PFS after re-irradiation were 6.7 months. In contrast, our median PFSpost was 21 months.
However, our study was a retrospective clinical study. The sample size was small and the follow-up time was short. Some patients did not detect EGFR or combined with other gene mutations may impact on the results. It need more prospectively, large sample size, randomized controlled trails to confirm the results.
Conclusions
This retrospective study revealed that adding hyperthermia to the treatment of NSCLC patients without EGFR mutation had better prognosis than those who didn’t adding hyperthermia to the regimen. Moreover, adding hyperthermia in first-line or in posterior-line treatment was no significant difference. However, these results need more prospective studies to confirm the conclusions.
Materials and Methods
Patients
We retrospectively collected patients from the Second Affiliated Hospital of Guangxi Medical University and Liuzhou Worker’s Hospital between January 2018 and December 2019. All patients had pathologically confirmed adenocarcinoma (AC) and squamous cell carcinoma (SCC) of lung and stage III-IV disease by the staging criteria of the 8th edition of the American Joint Committee on Cancer Staging System (AJCC) and the International Union Against Cancer (UICC) [33]. The inclusion criteria were as follows: 1) Patients aged 18 to 70 years old, 2) ECOG score ≤ 2, 3) Patients with complete clinical data, 4) Stage III -IV disease restaged by the 8th edition of AJCC/UICC TNM staging system, 5) Patients previously didn’t received any treatment, 6) Patients didn’t have any malignancies before. Exclusion criteria were: 1) ECOG score ≥3, 2) Patients with severe hepatic, renal and pulmonary dysfunction, 3) The pathological type was not adenocarcinoma or squamous cell carcinoma,4) Cognitive dysfunction. A total of 205 patients were included in this study based on the inclusion and exclusion criteria. On the basis of adding hyperthermia or not to the regimen in the advanced NSCLC before first progression, we divided all the eligible patients into hyperthermia group (N= 77) and non- hyperthermia group (N = 128). There were 25(32.5%) patients had EGFR mutation in hyperthermia group while 44(34.4%) patients in non- hyperthermia group among the groups. The patients’ base-line characteristics were shown in Table 1.
Treatment
Surgery
Lobectomy or partial or total pneumonectomy± lymph node dissection through thoracotomy or thoracoscopy.
Chemotherapy
Chemotherapy schemes were as follows: cisplatin or carboplatin + pemetrexed (AP), gemcitabine + cisplatin or carboplatin (GP or GC), docetaxel or paclitaxel or albumin bound paclitaxel 2+ cisplatin or carboplatin (TP), repeated every three weeks, 4-6 cycles.
Radiotherapy (RT)
All included patients were received 6 MV-X ray liner accelerator intensity modulated radiation therapy (IMRT), and the treatment steps were as follows: (1) Patients were positioned and fixed, scanned and positioned with simulated CT (Philips, Brilliance, Netherlands and Siemens, AS Definition Open20, Germany) and the scanning layer spacing was 3mm. (2) Target delineation: We used Treatment planning system (TPS) 13.6 (Varian, Vitalbeam, USA) and Raystaion4.7.5 (Varian, Trilogy, USA and Elekta, Precise, UK) to delineate the target volumes. According to ICRU Report No. 83, the target area included: ① gross tumor volume (GTV): the range of primary lesions determined according to imaging, including primary lung lesions (GTV) and regional lymph node metastasis (GTVnd). ② Clinical tumor volume (CTV): it included GTV, subclinical lesions and areas that may be invaded by tumors. ③ Planning tumor volume (PTV) was the range determined according to organ movement and daily positioning error to ensure the treatment dose. ④ Dangerous organs: dangerous organs included: left lung, right lung, double lungs, heart, trachea, esophagus, brain stem, spinal cord, optic nerve, optic chiasm, etc. 3) According to the NCCN guidelines, the prescription dose and organ endangering limit were given, and the plan was evaluated: ① prescription dose: radical radiotherapy for lung lesions: PGTV: 60gy-66Gy/30-33 f, PTV1: 50-54Gy/ 30-33 fractions at 5 fractions per week during a period of 6-7 weeks. SBRT:60Gy/10f. Palliative radiotherapy for lung lesions: PGTV: 45-50Gy, PTV1: 36-40Gy/25-27 fractions. Other lesions such as whole brain radiotherapy, vertebral body and bone: PTV: 30Gy / 10f or 40Gy/20f. ② Limit of Organ at risk (OAR): the maximum dose of brain stem was less than 54Gy; The maximum dose of spinal cord < 45Gy; The maximum dose of optic nerve and optic chiasm < 50Gy; Single lung V5 ≤ 65%, V20 ≤ 30%, V30 ≤ 20%; Heart V30 ≤ 30%, average cardiac irradiation dose ≤ 35Gy; Esophageal V50 ≤ 50%, average dose ≤ 34 Gy. The maximum dose of trachea was less than 60 Gy.
Target therapy
(1) Oral Gefitinib 250mg / time, once a day, (2) Erlotinib 150mg / time, once a day, (3) Ektinib 125mg / time, three times a day, (4) Ositinib 80mg / time, once a day, (5) Afatinib 40mg / time, once a day, (6) Kezotinib 250mg / time, twice a day.
Hyperthermia
One hour before other treatment, Jilin Maida medical radiofrequency hyperthermia system NRL-004 was used to patients for 60 minutes, the temperature was controlled at 42° C, twice a week, with an average of 4-8 times.
Endpoints
The primary endpoint of this study was 1-year PFS. PFSfirst defined as the time from the diagnosis of the disease to the first progression or death from any cause. PFSpost in the Posterior line therapy adding hyperthermia was defined as from disease first progression to the last progression or death from any cause. The secondary endpoint was 1-year OS, which defined as the time from disease diagnosis to death or the last follow-up.
Statistical analysis
SPSS 22.0 software (IBM) and graphpad prism 8 software were used to analyze the data. Chi-square test was used for continuous variables, and t-test was used for categorical variables. Kaplan-Meier method was conducted for the analysis of the time-to-event endpoints, and the log-rank test was used to compare the differences between the two groups. Multivariate analysis were performed in the detection of prognostic factors related to the endpoints. Using graphpad prism 8 to draw the survival curve. All statistical tests were two-sided, and P<0.05 was considered statistically significant.
Ethics approval
The study was approved by the ethics committees of The Second Affiliated Hospital of Guangxi Medical University, and The Liuzhou Worker’s Hospital.
Author Contributions
Yanhua Zhou, Chunhui Wang, Binglin Chen, Menghua Chen, and Yihe Li collect the data. Yanhua Zhou and Qiulu Zhong carried out the final analysis. Yanhua Zhou and Qiulu Zhong wrote the original draft. Wenqi Liu, Dongning Huang, Li Qin and Jian Huang administrated the project. All authors read and approved the final manuscript. Thank you for all my colleagues.
Conflicts of Interest
All the authors have declared no conflicts of interest.
Funding
This work were supported by Guangxi key research and development program (No: GKAB18221080), Agricultural, rural and social development science and technology projects (No: 2020NBAB0810) and the project of Middle-aged and Young Teachers’ Basic Ability Promotion Project of Guangxi (CN) (No: 2020KY03023).
Editorial Note
This corresponding author has a verified history of publications using a personal email address for correspondence
References
- 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016; 66:7–30. https://doi.org/10.3322/caac.21332 [PubMed]
- 2. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66:115–32. https://doi.org/10.3322/caac.21338 [PubMed]
- 3. Reck M, Rabe KF. Precision Diagnosis and Treatment for Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2017; 377:849–61. https://doi.org/10.1056/NEJMra1703413 [PubMed]
- 4. Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman J, Chirieac LR, D’Amico TA, DeCamp MM, Dilling TJ, Dobelbower M, Doebele RC, Govindan R, Gubens MA, et al. Non-Small Cell Lung Cancer, Version 5.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017; 15:504–35. https://doi.org/10.6004/jnccn.2017.0050 [PubMed]
- 5. Jurisic V, Vukovic V, Obradovic J, Gulyaeva LF, Kushlinskii NE, Djordjević N. EGFR Polymorphism and Survival of NSCLC Patients Treated with TKIs: A Systematic Review and Meta-Analysis. J Oncol. 2020; 2020:1973241. https://doi.org/10.1155/2020/1973241 [PubMed]
- 6. Obradovic J, Todosijevic J, Jurisic V. Application of the conventional and novel methods in testing EGFR variants for NSCLC patients in the last 10 years through different regions: a systematic review. Mol Biol Rep. 2021; 48:3593–604. https://doi.org/10.1007/s11033-021-06379-w [PubMed]
- 7. Kit OI, Vodolazhsky DI, Timoshkina NN, Vladimirova LY, Turkin IN, Kutsyn KA, Enin YS, Panina SB, Jurisic V. EGFR mutations and tumor metastases in patients with nonsmall cell lung cancer in the South of Russia. J BUON. 2017; 22:1410–5. [PubMed]
- 8. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O’Brien M, Rao S, Hotta K, et al, and KEYNOTE-024 Investigators. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016; 375:1823–33. https://doi.org/10.1056/NEJMoa1606774 [PubMed]
- 9. Herbst RS, Giaccone G, de Marinis F, Reinmuth N, Vergnenegre A, Barrios CH, Morise M, Felip E, Andric Z, Geater S, Özgüroğlu M, Zou W, Sandler A, et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N Engl J Med. 2020; 383:1328–39. https://doi.org/10.1056/NEJMoa1917346 [PubMed]
- 10. Sezer A, Kilickap S, Gümüş M, Bondarenko I, Özgüroğlu M, Gogishvili M, Turk HM, Cicin I, Bentsion D, Gladkov O, Clingan P, Sriuranpong V, Rizvi N, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021; 397:592–604. https://doi.org/10.1016/S0140-6736(21)00228-2 [PubMed]
- 11. Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, Domine M, Clingan P, Hochmair MJ, Powell SF, Cheng SY, Bischoff HG, Peled N, et al, and KEYNOTE-189 Investigators. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N Engl J Med. 2018; 378:2078–92. https://doi.org/10.1056/NEJMoa1801005 [PubMed]
- 12. Paz-Ares L, Luft A, Vicente D, Tafreshi A, Gümüş M, Mazières J, Hermes B, Çay Şenler F, Csőszi T, Fülöp A, Rodríguez-Cid J, Wilson J, Sugawara S, et al, and KEYNOTE-407 Investigators. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N Engl J Med. 2018; 379:2040–51. https://doi.org/10.1056/NEJMoa1810865 [PubMed]
- 13. Lee CK, Man J, Lord S, Links M, Gebski V, Mok T, Yang JC. Checkpoint Inhibitors in Metastatic EGFR-Mutated Non-Small Cell Lung Cancer-A Meta-Analysis. J Thorac Oncol. 2017; 12:403–7. https://doi.org/10.1016/j.jtho.2016.10.007 [PubMed]
- 14. Lisberg A, Cummings A, Goldman JW, Bornazyan K, Reese N, Wang T, Coluzzi P, Ledezma B, Mendenhall M, Hunt J, Wolf B, Jones B, Madrigal J, et al. A Phase II Study of Pembrolizumab in EGFR-Mutant, PD-L1+, Tyrosine Kinase Inhibitor Naïve Patients With Advanced NSCLC. J Thorac Oncol. 2018; 13:1138–45. https://doi.org/10.1016/j.jtho.2018.03.035 [PubMed]
- 15. Guo D, Chen Y, Wang S, Yu L, Shen Y, Zhong H, Yang Y. Exosomes from heat-stressed tumour cells inhibit tumour growth by converting regulatory T cells to Th17 cells via IL-6. Immunology. 2018; 154:132–43. https://doi.org/10.1111/imm.12874 [PubMed]
- 16. Wendt MK, Tian M, Schiemann WP. Deconstructing the mechanisms and consequences of TGF-β-induced EMT during cancer progression. Cell Tissue Res. 2012; 347:85–101. https://doi.org/10.1007/s00441-011-1199-1 [PubMed]
- 17. Guo J, Men CJ, Wang SZ, Gao XD, Cheng Z, Mao ZY, Wang DZ. [Influence of thermochemotherapy on the activity of cytotoxic T lymphocyte in oral maxillofacial cancer patients]. Hua Xi Kou Qiang Yi Xue Za Zhi. 2007; 25:441–3. [PubMed]
- 18. Jurisic V. Multiomic analysis of cytokines in immuno-oncology. Expert Rev Proteomics. 2020; 17:663–74. https://doi.org/10.1080/14789450.2020.1845654 [PubMed]
- 19. Karasawa K, Muta N, Nakagawa K, Hasezawa K, Terahara A, Onogi Y, Sakata K, Aoki Y, Sasaki Y, Akanuma A. Thermoradiotherapy in the treatment of locally advanced nonsmall cell lung cancer. Int J Radiat Oncol Biol Phys. 1994; 30:1171–7. https://doi.org/10.1016/0360-3016(94)90325-5 [PubMed]
- 20. Rizzo S. Survival of chemo-radiotherapy-treated and thermotherapy-treated patients with unresectable lung cancer. Oncol Rep. 1998; 5:667–71. [PubMed]
- 21. Cheng Y, Weng S, Yu L, Zhu N, Yang M, Yuan Y. The Role of Hyperthermia in the Multidisciplinary Treatment of Malignant Tumors. Integr Cancer Ther. 2019; 18:1534735419876345. https://doi.org/10.1177/1534735419876345 [PubMed]
- 22. Zhao Y, Zhang S, Wu Z, Zhang J, Zhu L, Xu Y, Ma S. P2.05-029 Microwave Thermal Therapy Enhances Radiosensitivity of Highly Invasive Human Non-Small Cell Lung Cancer H460 Cells via Inhibiting DNA Repair: Topic: Multimodality Treatment. Journal of Thoracic Oncology. 2017; 12:S1048. https://doi.org/10.1016/j.jtho.2016.11.1464
- 23. Chen YD, Zhang Y, Dong TX, Xu YT, Zhang W, An TT, Liu PF, Yang XH. Hyperthermia with different temperatures inhibits proliferation and promotes apoptosis through the EGFR/STAT3 pathway in C6 rat glioma cells. Mol Med Rep. 2017; 16:9401–8. https://doi.org/10.3892/mmr.2017.7769 [PubMed]
- 24. Hurwitz M, Stauffer P. Hyperthermia, radiation and chemotherapy: the role of heat in multidisciplinary cancer care. Semin Oncol. 2014; 41:714–29. https://doi.org/10.1053/j.seminoncol.2014.09.014 [PubMed]
- 25. Deschamps F, Farouil G, Ternes N, Gaudin A, Hakime A, Tselikas L, Teriitehau C, Baudin E, Auperin A, de Baere T. Thermal ablation techniques: a curative treatment of bone metastases in selected patients? Eur Radiol. 2014; 24:1971–80. https://doi.org/10.1007/s00330-014-3202-1 [PubMed]
- 26. Yu J, Liang P, Yu XL, Cheng ZG, Han ZY, Mu MJ, Li QY, Liu YM. Local tumour progression after ultrasound-guided microwave ablation of liver malignancies: risk factors analysis of 2529 tumours. Eur Radiol. 2015; 25:1119–26. https://doi.org/10.1007/s00330-014-3483-4 [PubMed]
- 27. Gillams AR, Lees WR. Radiofrequency ablation of lung metastases: factors influencing success. Eur Radiol. 2008; 18:672–7. https://doi.org/10.1007/s00330-007-0811-y [PubMed]
- 28. Wei Z, Ye X, Yang X, Huang G, Li W, Wang J, Han X, Meng M, Ni Y. Advanced non small cell lung cancer: response to microwave ablation and EGFR Status. Eur Radiol. 2017; 27:1685–94. https://doi.org/10.1007/s00330-016-4474-4 [PubMed]
- 29. Wei Z, Ye X, Yang X, Zheng A, Huang G, Li W, Wang J, Han X, Meng M, Ni Y. Microwave ablation combined with EGFR-TKIs versus only EGFR-TKIs in advanced NSCLC patients with EGFR-sensitive mutations. Oncotarget. 2017; 8:56714–25. https://doi.org/10.18632/oncotarget.18083 [PubMed]
- 30. Dong ZY, Zhang JT, Liu SY, Su J, Zhang C, Xie Z, Zhou Q, Tu HY, Xu CR, Yan LX, Li YF, Zhong WZ, Wu YL. EGFR mutation correlates with uninflamed phenotype and weak immunogenicity, causing impaired response to PD-1 blockade in non-small cell lung cancer. Oncoimmunology. 2017; 6:e1356145. https://doi.org/10.1080/2162402X.2017.1356145 [PubMed]
- 31. Sugiyama E, Togashi Y, Takeuchi Y, Shinya S, Tada Y, Kataoka K, Tane K, Sato E, Ishii G, Goto K, Shintani Y, Okumura M, Tsuboi M, Nishikawa H. Blockade of EGFR improves responsiveness to PD-1 blockade in EGFR-mutated non-small cell lung cancer. Sci Immunol. 2020; 5:eaav3937. https://doi.org/10.1126/sciimmunol.aav3937 [PubMed]
- 32. Ohguri T, Imada H, Yahara K, Moon SD, Yamaguchi S, Yatera K, Mukae H, Hanagiri T, Tanaka F, Korogi Y. Re-irradiation plus regional hyperthermia for recurrent non-small cell lung cancer: a potential modality for inducing long-term survival in selected patients. Lung Cancer. 2012; 77:140–5. https://doi.org/10.1016/j.lungcan.2012.02.018 [PubMed]
- 33. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, Nicholson AG, Groome P, Mitchell A, Bolejack V, and International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions, and International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee Advisory Boards and Participating Institutions. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016; 11:39–51. https://doi.org/10.1016/j.jtho.2015.09.009 [PubMed]