



Introduction
Hepatocellular carcinoma (HCC) is one of the leading causes of global cancer-related mortality, constituting a significant portion of liver cancer cases. According to the World Health Organization, there are over 840,000 newly diagnosed cases of liver cancer globally each year, with approximately 780,000 deaths, highlighting the persistently high mortality and incidence rates of liver cancer. Particularly in East Asia and Africa, where the prevalence of hepatitis virus infections is high, the incidence of HCC remains elevated [1–3]. The symptoms of liver cancer in the early stages are often subtle, leading to the late detection of many patients who miss the optimal window for surgical intervention. The choice of treatment strategies such as surgical resection, radiofrequency ablation, or liver transplantation is often constrained by tumor size, quantity, location, and the patient’s liver function. While these treatment modalities achieve partial efficacy, the overall cure rate is suboptimal due to significant surgical trauma, potential postoperative complications, and high rates of lesion recurrence [4, 5]. For advanced-stage liver cancer patients opting for targeted therapies such as sorafenib, regorafenib, and cabozantinib, although these treatments extend survival and improve quality of life, they fail to completely eliminate lesions and are plagued by issues of drug resistance [6–8]. In recent years, there has been an increasing emphasis on early diagnosis and therapeutic efficacy monitoring in liver cancer. Conventional imaging studies and the measurement of tumor markers such as AFP (Alpha-fetoprotein), CA125 (Cancer Antigen 125), and CA19-9 remain the mainstays of liver cancer diagnosis. However, the sensitivity and specificity of these methods are significantly limited, failing to meet the demands for early, reliable, and accurate liver cancer diagnosis [9, 10]. Moreover, traditional monitoring methods, such as repetitive imaging examinations, often fall short in detecting minuscule recurrent lesions. Assessing treatment effectiveness typically requires a waiting period for confirmation through imaging or biochemical markers, which may lead to disease progression or the persistence of ineffective treatment strategies [11–13]. Therefore, the exploration of new diagnostic and therapeutic approaches for hepatocellular carcinoma holds paramount clinical significance.
Circulating tumor DNA (ctDNA) comprises fragments of tumor-derived DNA released into the bloodstream upon tumor cell death. These fragments offer insights into the genomic status and dynamic alterations of the tumor [14, 15]. In contrast to conventional tissue biopsies, ctDNA analysis presents a non-invasive avenue for monitoring the epigenetic traits of tumors, encompassing mutations, copy number variations, and methylation patterns [16–18]. This analytical approach not only serves in early screening and diagnosis but also facilitates the assessment of therapeutic efficacy and the prediction of disease recurrence during the treatment process [19, 20]. In tumors, the generation of ctDNA primarily involves the processes of apoptosis and necrosis of tumor cells. When tumor cells die, their DNA is released into the bloodstream, forming ctDNA. Additionally, active tumor cells can also release DNA through the secretion of small vesicles, further increasing the concentration of ctDNA in the blood [21, 22]. Research has revealed that ctDNA can serve as a biomarker for early diagnosis and screening of cancers such as colorectal cancer and non-small cell lung cancer, and it can be detected before the onset of relevant clinical symptoms [23, 24]. Therefore, the detection and analysis of ctDNA can provide molecular characteristic information of the tumor, contributing to early cancer diagnosis and monitoring of therapeutic efficacy [25].
In recent years, significant progress has been made in the study of circulating tumor DNA (ctDNA) with the development of high-throughput sequencing technologies. The analysis of mutation information in ctDNA allows for early cancer diagnosis and monitoring of therapeutic efficacy. Furthermore, the Tagged-Amplicon Deep Sequencing (TAm-Seq) method has been demonstrated as a viable approach for non-invasively identifying gene mutations in blood, capable of amplifying and sequencing large genomic regions, even from a single copy of ctDNA. This method enables the detection of low-frequency mutations, including those in cancer-associated genes such as TP53, EGFR, BRAF, and KRAS [26]. Analysis of mutation sites in ctDNA can also unveil the molecular mechanisms underlying tumor resistance to therapy, thereby providing a basis for developing novel treatment strategies [27]. Moreover, ctDNA can be utilized to detect the presence of residual tumor cells post-surgery or radiation therapy, which holds significant importance in predicting tumor recurrence and guiding subsequent treatment [28, 29].
During the apoptosis process of tumor cells, DNA is fragmented by enzymes and released into the surrounding environment. Additionally, the necrosis of tumor cells can lead to the release of a large amount of DNA into the bloodstream. These released DNA fragments undergo a series of modifications and stabilization processes to form ctDNA. Researchers have also found that factors such as inflammation and angiogenesis in the tumor microenvironment may influence the release and circulation of ctDNA. In recent years, numerous studies have demonstrated the potential of ctDNA mutation analysis in early diagnosis of HCC [30, 31]. Researchers have discovered the presence of common hepatocellular carcinoma (HCC)-associated gene mutations, such as TP53, CTNNB1, and AXIN1, in blood samples from HCC patients [32–34]. These mutations play crucial roles in the occurrence and progression of HCC. Moreover, analysis of ctDNA in the blood samples of 77.3% of HCC patients undergoing anti-PD-1 therapy revealed the presence of >1 genetic alterations, with TP53 being the most common mutated gene, observed in 11 patients [35]. Evaluation of ctDNA mutations can not only be utilized for early screening of HCC but also serves as a vital tool for treatment selection and efficacy monitoring. Specific mutations in ctDNA, such as specific deletions/insertions in the EZH2 gene, can assess the efficacy of chemotherapy in gastric cancer. Similarly, the association between the detection of IDH1 mutations and clinical response offers a new perspective on the treatment of intrahepatic cholangiocarcinoma (IHC). Furthermore, monitoring the mutation spectrum of ctDNA aids in evaluating the diagnostic efficacy of early to intermediate stage non-small cell lung cancer (NSCLC) patients and correlates with tumor size and clinical staging [36].
In this review, we summarized the current understanding of the molecular mechanisms and clinical applications of ctDNA mutation in the occurrence and development of hepatocellular carcinoma, with a focus on its value in early diagnosis and monitoring therapeutic efficacy.
ctDNA mutation analysis techniques
The mutation analysis of circulating tumor DNA (ctDNA) is an important non-invasive detection method that can be used for early diagnosis and monitoring therapeutic efficacy in hepatocellular carcinoma (HCC) [37, 38]. Over the past few years, significant improvements and innovations have been made in ctDNA mutation analysis methods along with technological advancements. This section will focus on the collection and extraction methods of ctDNA, as well as commonly used ctDNA mutation analysis techniques, including next-generation sequencing (NGS), digital PCR, and TAm-Seq techniques.
Blood sample collection is one of the most commonly used methods for ctDNA collection [39]. ctDNA extraction methods primarily include nucleic acid extraction and ctDNA enrichment. Nucleic acid extraction involves extracting total DNA from plasma or serum, including DNA released from both normal and tumor cells. Common nucleic acid extraction methods include commercial DNA extraction kits and magnetic bead-based methods. On the other hand, ctDNA enrichment methods involve enriching ctDNA from total DNA using specific techniques to enhance detection sensitivity. Presently, methods for ctDNA enrichment primarily comprise Single-Strand Binding Polymerase Chain Reaction (SSB-PCR), probe detection systems based on the IV endonuclease, rolling circle amplification technology, digital PCR, hybrid capture methods, and detection using internal reference nucleic acid probes, as detailed in Table 1.
Table 1. Comparison of ctDNA enrichment methods.
| Method | Principle | Advantages | Reference |
| SSB-PCR | Specific inhibition chains and primers are designed to selectively enrich low-abundance short DNA strands. | Effective differentiation of fetal wild-type homozygous short DNA, heterozygous short DNA, and mutant homozygous short DNA even at abundances as low as 2%. | [49, 50] |
| Probe detection based on IV endonuclease | Utilizes the ability of the IV endonuclease to recognize probe vacancies and cleave them, enabling simultaneous detection of multiple mutations at inconsistent detection temperatures through specific probe designs. | Effective discrimination between wild-type DNA and mutant DNA, with effective discrimination among 6 mismatches, demonstrating good universality and accuracy. | [51] |
| Rolling circle amplification (RCA) | Under the action of polymerases with strand displacement properties, amplification is consistently performed using the initial circular DNA as a template, ensuring that errors generated in each round of amplification are not passed on to the next round. | Capable of enriching trace amounts of cfDNA and amplifying the frequency of low-frequency mutations in ctDNA in allelic genes. | [52] |
| Digital PCR (dPCR) and hybrid capture | Enriches target DNA by specific probes or antibodies binding to the target DNA sequence, demonstrating superior performance in target enrichment, especially in coverage of target sites across all samples. | Demonstrates superior performance in target enrichment, especially in coverage of target sites across all samples. | [53, 54] |
| Detection using internal reference probes | Constructs self-sequences as references, unaffected by irrelevant sequences, capable of effectively distinguishing between wild-type and mutant DNA. | Enables quantitative detection of mutation abundance at different concentrations, demonstrating good quantitative limits and accuracy. | [55, 56] |
Next-generation sequencing (NGS) is a high-throughput sequencing technology that allows simultaneous analysis of mutations in multiple genes. The advantages of NGS lie in its high sensitivity and specificity, enabling the detection of low-frequency mutations [40]. In the analysis of ctDNA mutations, NGS can be employed for whole exome sequencing, targeted gene sequencing, and quantitative analysis of mutation sites. Through NGS technology, a comprehensive understanding of the tumor mutation profile can be achieved, providing a basis for personalized therapy [41, 42]. Research has shown that Next-Generation Sequencing (NGS) can detect ctDNA mutations with allele frequencies as low as 0.1% and has been successfully applied in ctDNA analysis for various cancer types, including lung cancer, gastric cancer, and intrahepatic cholangiocarcinoma (ICC) [43]. The application of NGS extends beyond the detection of mutations in single genes, encompassing extensive analysis of the entire genome or specific gene regions, thereby uncovering more potential therapeutic targets [44]. Digital PCR (dPCR) is a PCR technology based on the principle of molecular counting, facilitating quantitative analysis of mutation sites in ctDNA. Compared to traditional quantitative PCR techniques, dPCR exhibits higher sensitivity and accuracy. In ctDNA mutation analysis, dPCR can be utilized to detect low-frequency mutations and assess mutation burden. dPCR has been demonstrated to exhibit good accuracy and sensitivity in detecting specific mutations such as KRAS G12D, TP53 C242S, and IDH1 R132C. Additionally, dPCR has been utilized in the development of a novel 5-plex copy number droplet digital PCR (ddPCR) detection platform targeting BRAF or CCND1 copy number amplifications, enhancing the monitoring capabilities for resistance mechanisms [45]. With dPCR technology, precise quantification of ctDNA mutations can be achieved, offering more accurate results for early diagnosis and treatment monitoring of hepatocellular carcinoma [46]. Tagged-amplicon deep sequencing (TAm-Seq) is a deep sequencing method specifically designed for ctDNA, capable of identifying single-copy ctDNA fragments at extremely low allele frequencies. This technology has been applied in ctDNA analysis for various cancers, including high-grade serous ovarian cancer, successfully identifying low-level TP53 mutations and mutations in other key genes [47, 48]. An improved version of TAm-Seq further enhances its ability to detect low-level mutations, making it a crucial tool for monitoring disease progression and treatment response. A comparison of the advantages and disadvantages of three ctDNA mutation analysis techniques is provided in Table 2.
Table 2. Comparison of advantages and disadvantages of ctDNA mutation analysis techniques.
| Analysis technique | Principle | Advantages | Disadvantages |
| NGS (Next-Generation Sequencing) | Utilizes high-throughput sequencing technology to analyze ctDNA for detecting tumor mutations. | Relatively low cost, wide coverage range; simultaneous detection of multiple genes and mutation types; easy operation, suitable for large-scale sample analysis [57]. | Detection sensitivity limited by ctDNA abundance; limited ability to detect low-frequency mutations; requires complex bioinformatics analysis to interpret results [58, 59]. |
| Digital PCR (dPCR) | Divides samples into thousands of microreaction units, where PCR amplification and fluorescence-labeled probe detection are independently performed in each unit, achieving high sensitivity and specificity for specific mutations. | High sensitivity and specificity; capable of detecting extremely low abundance of ctDNA; high accuracy, suitable for Minimal Residual Disease (MRD) detection. | High equipment cost; complex sample preparation process; requires high technical expertise from operators [60]. |
| TAm-Seq (Tagged-Amplicon Deep Sequencing) | Amplifies target regions in ctDNA using specific primers designed, followed by analysis of these amplicons using deep sequencing technology to identify low-frequency mutations. | Capable of detecting mutations with allele frequencies as low as 0.1%; high sensitivity for single-copy ctDNA; provides abundant variant information in a short time [48]. | Requires design and optimization of primers for different tumor types and gene loci; may still have detection limitations for extremely low abundance of ctDNA or specific types of mutations; relatively high cost. |
In conclusion, ctDNA mutation analysis techniques hold significant value in the early diagnosis and treatment monitoring of HCC. The collection and extraction methods for ctDNA, along with commonly used mutation analysis technologies such as next-generation sequencing (NGS), digital PCR (dPCR), and Tagged-amplicon deep sequencing (TAm-Seq), serve as reliable tools for ctDNA mutation analysis. As technology continues to advance and research deepens, ctDNA mutation analysis techniques are poised to further propel the progress of early diagnosis and treatment monitoring for HCC. They will provide more precise guidance for personalized therapy.
The application of ctDNA mutation analysis in early diagnosis of hepatocellular carcinoma
In recent years, the analysis of circulating tumor DNA (ctDNA) mutations has emerged as a promising non-invasive detection method, providing new opportunities for the early diagnosis of HCC. This section will focus on the selection and validation of ctDNA mutation markers, a comparison between ctDNA mutation analysis and traditional diagnostic methods, and the clinical application of ctDNA mutation analysis in early HCC diagnosis through case studies.
The selection and validation of ctDNA mutation markers are critical steps in early diagnosis of HCC. Analysis of mutation sites in ctDNA allows for the identification of mutated genes and mutation frequencies associated with HCC [61, 62]. Currently, numerous studies have identified ctDNA mutation markers associated with HCC, such as TP53, CTNNB1, AXIN1, and others [32–34], as shown in Table 3.
Table 3. Functional description of ctDNA mutation markers associated with HCC.
| ctDNA | Function | Source | Reference |
| TERT Promoter Mutations | Promote cellular proliferation and avoid senescence, associated with HCC development | Hepatocytes | [75, 76] |
| TP53 Mutations | Regulate cell cycle, DNA repair, and apoptosis | Hepatocytes and surrounding tissues | [32, 77] |
| CTNNB1 Mutations | Control cell adhesion and signaling, associated with HCC development | Hepatocytes | [32, 78, 79] |
| ARID1A Mutations | Involved in chromatin remodeling and gene expression regulation, related to liver carcinogenesis | Hepatocytes | [80] |
| PIK3CA Mutations | Activate signaling pathways for cell growth and survival, implicated in HCC | Hepatocytes | [81, 82] |
| RAS Mutations | Involved in cell signaling pathways that control cell growth, mutations often found in HCC | Hepatocytes | [83, 84] |
| ALB-Fusions | Abnormal albumin gene fusions, unique to liver cancer and can be used as a biomarker | Hepatocytes | [85] |
| APOB Mutations | A pattern of mutations suggesting activity of APOBEC cytidine deaminases, which can contribute to cancer genome mutations | Hepatocytes and immune cells | [86] |
The TP53 gene encodes the p53 protein, a tumor suppressor protein capable of inhibiting tumor development by inducing apoptosis or halting cell cycle progression. TP53 mutations typically result in loss of p53 function, thereby promoting proliferation and survival of tumor cells, increasing malignancy and metastatic risk [63]. Studies have shown that TP53 mutations are commonly present in non-small cell lung cancer (NSCLC) and are closely associated with patient prognosis. Additionally, TP53 mutations may also affect patient response to certain treatments such as radiation therapy and chemotherapy [64]. Furthermore, the CTNNB1 gene encodes β-catenin, a cytoskeletal protein involved in regulating the Wnt signaling pathway. CTNNB1 mutations may lead to aberrant activation of the Wnt signaling pathway, promoting proliferation, invasion, and metastasis of tumor cells. However, current research evidence regarding the specific role and clinical significance of CTNNB1 mutations in HCC is relatively limited. The KRAS gene encodes a small G protein involved in various cell signaling pathways, including the insulin-like growth factor-1 (IGF-1) and epidermal growth factor (EGF) signaling pathways. KRAS mutations mainly occur in codons 12 and 13 of exon 2, leading to sustained activation of the KRAS protein, promoting proliferation, invasion, and angiogenesis of tumor cells. KRAS mutations are considered significant adverse prognostic markers in tumors such as colorectal cancer (CRC) and NSCLC [65]. Additionally, KRAS mutations directly impact patient response to anti-EGFR therapy [66].
The clinical significance of TP53, CTNNB1, and KRAS gene mutations in HCC patients mainly manifests in their influence on tumor biology, predictive value for treatment response, and impact on prognosis, as depicted in Figure 1. The specific mechanisms of action of these gene mutations suggest the importance of personalized treatment strategies and also offer the potential for the development of new therapeutic targets. Future research needs to further explore the mechanisms of action of these gene mutations in different subtypes of HCC and their impact on treatment outcomes, aiming to provide more precise treatment options for HCC patients.
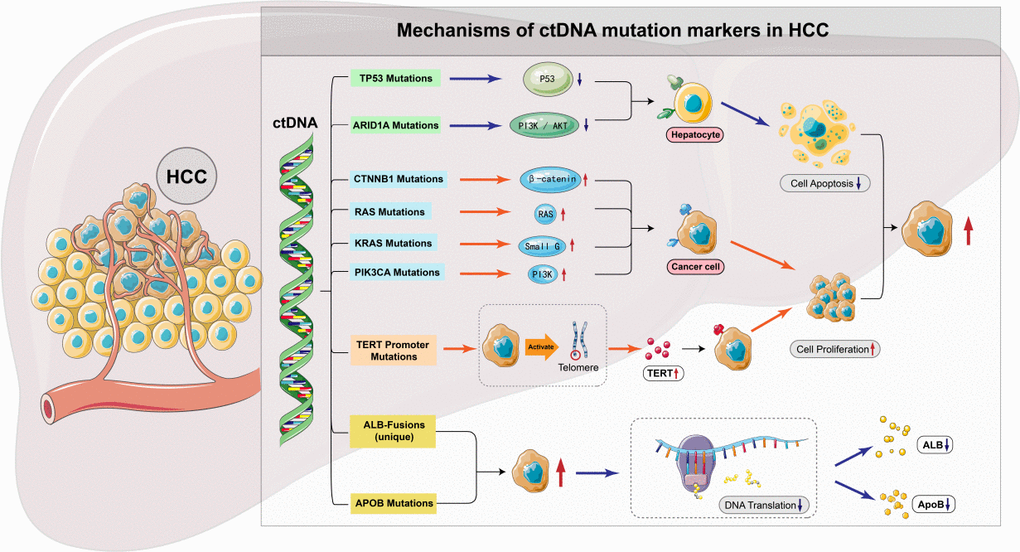
Figure 1. ctDNA mutation markers associated with HCC.
Compared to traditional diagnostic methods, ctDNA mutation analysis offers several advantages. Firstly, ctDNA mutation analysis is a non-invasive detection method that only requires a blood sample from patients, avoiding the trauma and risks associated with traditional tissue biopsies. Secondly, ctDNA mutation analysis exhibits high sensitivity and specificity, enabling the detection of low levels of tumor DNA and accurate diagnosis even at early stages of the disease. Additionally, ctDNA mutation analysis can provide genetic information about the tumor, such as mutation burden and mutation profile, which can guide personalized therapy [67, 68]. In comparison to traditional tumor markers such as AFP, ctDNA mutation analysis demonstrates higher sensitivity and specificity in early diagnosis of HCC. A study comparing ctDNA mutation analysis with AFP in early HCC diagnosis showed that the sensitivity and specificity of ctDNA mutation analysis were 85% and 92% respectively, while AFP exhibited sensitivity and specificity of 60% and 80% respectively. This indicates that ctDNA mutation analysis can provide more accurate and reliable early diagnosis results [69, 70].
A study analyzing the ctDNA mutation profile of 100 HCC patients identified several mutated genes associated with HCC, such as TP53, CTNNB1, and AXIN1 [71]. Another study found that ctDNA mutation burden in the blood sample of HCC patients was closely related to tumor size, staging, and prognosis, indicating that ctDNA mutation analysis could be used to evaluate patients’ prognosis and treatment response [72]. In addition to early diagnosis, ctDNA mutation analysis can also be utilized to monitor HCC patients’ treatment efficacy. A study analyzing the changes in ctDNA mutation burden after HCC patients received radiation therapy or targeted treatments found that the reduction of mutation burden was closely related to treatment response and survival rate improvement. This indicates that ctDNA mutation analysis could be used to evaluate treatment efficacy and predict the risk of recurrence [73, 74].
Therefore, as an emerging, non-invasive detection method, ctDNA mutation analysis shows great potential in early diagnosis of HCC. Through the selection and validation of ctDNA mutation markers, accurate guidance for individualized treatment and early diagnosis of HCC can be achieved. Clinical studies have already confirmed the potential of ctDNA mutation analysis in early diagnosis and treatment monitoring of HCC. With ongoing development of technology and research, ctDNA mutation analysis will provide more accurate and reliable methods for early diagnosis and treatment monitoring of HCC.
Application of ctDNA mutation analysis in treatment monitoring of hepatocellular carcinoma
Treatment monitoring is crucial for clinical decision-making in HCC, as it plays a significant role in evaluating treatment efficacy, guiding subsequent treatment strategies, and predicting patient prognosis [87]. The latest advancements in ctDNA mutation assessment in monitoring the therapeutic efficacy of HCC primarily encompass its significance as a tumor biomarker, its application in immunotherapy, its relationship with hepatocellular carcinoma, and its potential in treatment response monitoring. These advancements offer new perspectives and approaches for the diagnosis, treatment, and prognosis assessment of HCC. This section will focus on the association between ctDNA mutation burden and treatment response, the application of ctDNA mutation analysis in targeted therapies, and its utilization in radiation therapy and chemotherapy.
The ctDNA mutation burden refers to the quantity and frequency of mutation sites in ctDNA. Studies indicate a close correlation between ctDNA mutation burden and tumor size, staging, and prognosis. During the course of hepatocellular carcinoma (HCC) treatment, changes in ctDNA mutation burden can reflect treatment efficacy and predict the risk of recurrence [88]. An analysis of HCC patients undergoing radiation therapy or targeted treatment revealed a significant correlation between the reduction in mutation burden and improved treatment response and survival rates [89]. This suggests that ctDNA mutation burden serves as a crucial indicator for evaluating treatment efficacy.
Targeted therapy is a treatment method directed at specific molecular targets, aiming to enhance treatment efficacy and reduce side effects. The application of ctDNA mutation analysis in targeted therapy can assist in selecting suitable targeted drugs and monitoring treatment efficacy. By analyzing mutation sites in ctDNA, the mutational spectrum of HCC patients and the targets for targeted therapy can be identified. A study revealed a close correlation between EGFR mutations in HCC patients and sensitivity to targeted therapy. Through ctDNA mutation analysis, patients with EGFR-positive mutations can be identified and appropriate targeted drugs can be selected for treatment [90]. Another study found a close correlation between BRAF mutations in HCC patients and sensitivity to targeted therapy. Through ctDNA mutation analysis, patients with BRAF-positive mutations can be identified, and suitable targeted drugs can be selected for treatment [91]. Radiation therapy and chemotherapy are common treatment methods for HCC, but there are limitations in monitoring their efficacy. The application of ctDNA mutation analysis in radiation therapy and chemotherapy can provide more accurate and dynamic information on treatment efficacy. An analysis of HCC patients undergoing radiation therapy revealed a significant correlation between the reduction in mutation burden and improved treatment response and survival rates [92]. This indicates that ctDNA mutation analysis can be utilized to assess the efficacy of radiation therapy and predict the risk of recurrence. Another study found a significant correlation between the reduction in ctDNA mutation burden and improved treatment response and survival rates in HCC patients undergoing chemotherapy, further confirming the value of ctDNA mutation analysis in chemotherapy [93].
In summary, ctDNA mutation analysis, as an emerging non-invasive detection method, demonstrates significant potential in the monitoring of treatment efficacy for hepatocellular carcinoma (HCC). The association between ctDNA mutation burden and treatment response suggests that analyzing mutation sites in ctDNA can assess treatment efficacy and predict the risk of recurrence. In targeted therapy, ctDNA mutation analysis can assist in selecting suitable targeted drugs and monitoring treatment effectiveness. In radiation therapy and chemotherapy, ctDNA mutation analysis can offer more accurate and dynamic information on treatment efficacy. As technology continues to advance and research deepens, ctDNA mutation analysis will provide more accurate and reliable methods for monitoring the treatment efficacy of HCC, offering precise guidance for personalized treatment.
Challenges and future development of ctDNA mutation analysis
As the application of circulating tumor DNA (ctDNA) mutation analysis in the early diagnosis and monitoring of treatment efficacy for hepatocellular carcinoma (HCC) continues to develop, some challenges and future development directions are gradually emerging. This section will focus on the improvement of detection sensitivity and specificity of ctDNA, standardization and calibration of ctDNA mutation analysis, the combined use of ctDNA mutation analysis with other biomarkers, and the prospects of ctDNA mutation analysis in personalized treatment.
In the analysis of ctDNA mutations, the key metrics are the detection sensitivity and specificity [94]. Despite notable progress to date, several challenges persist. Firstly, due to the extremely low abundance of ctDNA in blood, the development of more sensitive detection methods is imperative to enhance sensitivity. Secondly, given the sequence similarity between ctDNA and normal cell DNA, there is a need to further improve specificity to prevent misdiagnosis and errors in judgment. Future research endeavors may explore innovative technologies and approaches, such as amplifying the signal of ctDNA, increasing sequencing depth, and utilizing more specific mutation markers, to enhance the sensitivity and specificity of ctDNA detection. Standardization and calibration of ctDNA mutation analysis are crucial for ensuring accuracy and reproducibility. Standardized methods and procedures need to be established, as the lack of uniformity in experimental conditions and analytical methods across different laboratories and research teams has resulted in poor comparability and consistency of results [25, 62]. Therefore, the establishment of a unified standardization and calibration approach is paramount. This includes standardizing the collection, processing, and storage of samples, as well as experiment conditions and analytical procedures. Additionally, the creation of reference standards and a quality control system is essential. Through standardization and calibration, the reliability and reproducibility of ctDNA mutation analysis can be enhanced, providing more dependable results for clinical applications.
The combined application of ctDNA mutation analysis with other biomarkers holds the potential to further enhance the accuracy and reliability of early diagnosis and treatment monitoring for hepatocellular carcinoma (HCC). For instance, incorporating serum markers such as alpha-fetoprotein (AFP) and hepatocellular carcinoma-related antigen (HCC-RA) can improve the sensitivity and specificity of early diagnosis [95]. Additionally, integrating imaging modalities such as ultrasound, CT, and MRI can provide a more comprehensive overview of tumor information [96]. Future research endeavors should explore the synergistic use of ctDNA mutation analysis with other biomarkers to elevate the accuracy and reliability of diagnosing and monitoring the treatment efficacy of hepatocellular carcinoma. The prospect of ctDNA mutation analysis in personalized therapy lies in tailoring treatment plans based on individual patient differences and the genetic characteristics of tumors. By providing genetic information about the tumor, such as mutation load and mutational lineage, ctDNA mutation analysis serves as a foundation for personalized treatment decisions. Analyzing mutation sites in ctDNA allows for the identification of mutational lineages and targets for targeted therapy. Future studies can further investigate the application of ctDNA mutation analysis in personalized therapy, including the selection of appropriate targeted drugs, monitoring treatment effectiveness, and predicting patient prognosis.
In summary, ctDNA mutation analysis has made significant progress in the early diagnosis and treatment monitoring of hepatocellular carcinoma (HCC). However, several challenges and future directions exist. These include improving the detection sensitivity and specificity of ctDNA, standardizing and calibrating the methods and procedures for ctDNA mutation analysis, exploring the combined application of ctDNA mutation analysis with other biomarkers, and further leveraging the role of ctDNA mutation analysis in personalized therapy. With the continuous advancement of technology and deeper research, it is believed that ctDNA mutation analysis will provide more accurate and reliable methods for the early diagnosis and treatment monitoring of HCC, offering more precise guidance for personalized therapy.
Conclusion
ctDNA mutation analysis holds significant value in the early diagnosis of hepatocellular carcinoma (HCC). Early diagnosis has been a massive challenge due to the hidden nature and lack of specific symptoms of HCC. However, as a non-invasive detection method, ctDNA mutation analysis can achieve early diagnosis by analyzing mutation sites in ctDNA. By screening and validating ctDNA mutation markers, it is possible to identify HCC-related mutated genes and mutation frequencies, thereby enhancing the accuracy and reliability of early diagnosis. Additionally, ctDNA mutation analysis has important applications in monitoring the treatment efficacy of hepatocellular carcinoma. Treatment monitoring is vital for assessing treatment responses, guiding subsequent treatment strategies, and predicting patient prognosis. By analyzing changes in ctDNA mutation load, treatment effectiveness can be evaluated, and the risk of recurrence can be predicted. Research indicates a close correlation between a decrease in ctDNA mutation load and improved treatment response and survival rates. Therefore, ctDNA mutation analysis can serve as a non-invasive monitoring method, providing more accurate and reliable results for the treatment monitoring of hepatocellular carcinoma.
Furthermore, future research directions and prospects are worth considering. Firstly, there is a need to further improve the detection sensitivity and specificity of ctDNA mutation analysis to enhance the accuracy of early diagnosis and treatment monitoring. Secondly, standardized methods and procedures need to be established to ensure the reliability and reproducibility of ctDNA mutation analysis. Additionally, exploring the combined application of ctDNA mutation analysis with other biomarkers can enhance the accuracy and reliability of the diagnosis and treatment monitoring of hepatocellular carcinoma. Lastly, ctDNA mutation analysis has potential in personalized therapy, enabling the selection of the most suitable treatment plan based on individual patient differences and the genetic characteristics of tumors.
In summary, ctDNA mutation analysis holds significant value in the early diagnosis and treatment monitoring of hepatocellular carcinoma (HCC). By improving the accuracy and reliability of early diagnosis, as well as evaluating treatment effectiveness and predicting patient prognosis, ctDNA mutation analysis can provide more precise personalized treatment guidance for HCC patients. Future research efforts should focus on further advancing the technology and methods of ctDNA mutation analysis, promoting its clinical application, and strengthening multi-center collaboration and large-sample studies to validate its potential in the early diagnosis and treatment monitoring of HCC. It is believed that with continuous technological advancements and in-depth research, ctDNA mutation analysis will provide more accurate and reliable methods for the early diagnosis and treatment monitoring of HCC, leading to a significant improvement in patient survival rates and quality of life.
Author Contributions
Jing Yang, Na Lin and Miaomiao Niu were responsible for reviewing the literature, synthesizing the information in the literature and writing the first draft. Boshu Yin was responsible for reviewing the final draft.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
No funding was provided for this study.
References
- 1. Vogel A, Meyer T, Sapisochin G, Salem R, Saborowski A. Hepatocellular carcinoma. Lancet. 2022; 400:1345–62. https://doi.org/10.1016/S0140-6736(22)01200-4 [PubMed]
- 2. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018; 391:1301–14. https://doi.org/10.1016/S0140-6736(18)30010-2 [PubMed]
- 3. Ganesan P, Kulik LM. Hepatocellular Carcinoma: New Developments. Clin Liver Dis. 2023; 27:85–102. https://doi.org/10.1016/j.cld.2022.08.004 [PubMed]
- 4. Anwanwan D, Singh SK, Singh S, Saikam V, Singh R. Challenges in liver cancer and possible treatment approaches. Biochim Biophys Acta Rev Cancer. 2020; 1873:188314. https://doi.org/10.1016/j.bbcan.2019.188314 [PubMed]
- 5. Zhou H, Song T. Conversion therapy and maintenance therapy for primary hepatocellular carcinoma. Biosci Trends. 2021; 15:155–60. https://doi.org/10.5582/bst.2021.01091 [PubMed]
- 6. Tang W, Chen Z, Zhang W, Cheng Y, Zhang B, Wu F, Wang Q, Wang S, Rong D, Reiter FP, De Toni EN, Wang X. The mechanisms of sorafenib resistance in hepatocellular carcinoma: theoretical basis and therapeutic aspects. Signal Transduct Target Ther. 2020; 5:87. https://doi.org/10.1038/s41392-020-0187-x [PubMed]
- 7. Lu Y, Chan YT, Tan HY, Zhang C, Guo W, Xu Y, Sharma R, Chen ZS, Zheng YC, Wang N, Feng Y. Epigenetic regulation of ferroptosis via ETS1/miR-23a-3p/ACSL4 axis mediates sorafenib resistance in human hepatocellular carcinoma. J Exp Clin Cancer Res. 2022; 41:3. https://doi.org/10.1186/s13046-021-02208-x [PubMed]
- 8. Méndez-Blanco C, Fondevila F, García-Palomo A, González-Gallego J, Mauriz JL. Sorafenib resistance in hepatocarcinoma: role of hypoxia-inducible factors. Exp Mol Med. 2018; 50:1–9. https://doi.org/10.1038/s12276-018-0159-1 [PubMed]
- 9. Ayuso C, Rimola J, Vilana R, Burrel M, Darnell A, García-Criado Á, Bianchi L, Belmonte E, Caparroz C, Barrufet M, Bruix J, Brú C. Diagnosis and staging of hepatocellular carcinoma (HCC): current guidelines. Eur J Radiol. 2018; 101:72–81. https://doi.org/10.1016/j.ejrad.2018.01.025 [PubMed]
- 10. Zhang YC, Xu Z, Zhang TF, Wang YL. Circulating microRNAs as diagnostic and prognostic tools for hepatocellular carcinoma. World J Gastroenterol. 2015; 21:9853–62. https://doi.org/10.3748/wjg.v21.i34.9853 [PubMed]
- 11. Li Z, Cheng J, Huang P, Song W, Nong L, Huang L, Lin W. Imaging and Detection of Hepatocellular Carcinoma with a Hepatocyte-Specific Fluorescent Probe. Anal Chem. 2022; 94:3386–93. https://doi.org/10.1021/acs.analchem.1c05540 [PubMed]
- 12. Feng B, Ma XH, Wang S, Cai W, Liu XB, Zhao XM. Application of artificial intelligence in preoperative imaging of hepatocellular carcinoma: Current status and future perspectives. World J Gastroenterol. 2021; 27:5341–50. https://doi.org/10.3748/wjg.v27.i32.5341 [PubMed]
- 13. Wang K, Chen XY, Zhang B, Yue Y, Wen XL, Yang Y, Yang YS, Zhu HL, Liu HJ, Zhang AG. Near-infrared imaging of hepatocellular carcinoma and its medicinal treatment with a γ-glutamyl transpeptidase-monitoring fluorescence probe. Biosens Bioelectron. 2023; 241:115721. https://doi.org/10.1016/j.bios.2023.115721 [PubMed]
- 14. Cescon DW, Bratman SV, Chan SM, Siu LL. Circulating tumor DNA and liquid biopsy in oncology. Nat Cancer. 2020; 1:276–90. https://doi.org/10.1038/s43018-020-0043-5 [PubMed]
- 15. Franczak C, Filhine-Tresarrieu P, Gilson P, Merlin JL, Au L, Harlé A. Technical considerations for circulating tumor DNA detection in oncology. Expert Rev Mol Diagn. 2019; 19:121–35. https://doi.org/10.1080/14737159.2019.1568873 [PubMed]
- 16. Tzanikou E, Lianidou E. The potential of ctDNA analysis in breast cancer. Crit Rev Clin Lab Sci. 2020; 57:54–72. https://doi.org/10.1080/10408363.2019.1670615 [PubMed]
- 17. Chang YS, Fang HY, Hung YC, Ke TW, Chang CM, Liu TY, Chen YC, Chao DS, Huang HY, Chang JG. Correlation of genomic alterations between tumor tissue and circulating tumor DNA by next-generation sequencing. J Cancer Res Clin Oncol. 2018; 144:2167–75. https://doi.org/10.1007/s00432-018-2747-9 [PubMed]
- 18. Hahn AW, Gill DM, Maughan B, Agarwal A, Arjyal L, Gupta S, Streeter J, Bailey E, Pal SK, Agarwal N. Correlation of genomic alterations assessed by next-generation sequencing (NGS) of tumor tissue DNA and circulating tumor DNA (ctDNA) in metastatic renal cell carcinoma (mRCC): potential clinical implications. Oncotarget. 2017; 8:33614–20. https://doi.org/10.18632/oncotarget.16833 [PubMed]
- 19. Chakrabarti S, Xie H, Urrutia R, Mahipal A. The Promise of Circulating Tumor DNA (ctDNA) in the Management of Early-Stage Colon Cancer: A Critical Review. Cancers (Basel). 2020; 12:2808. https://doi.org/10.3390/cancers12102808 [PubMed]
- 20. Chakrabarti S, Kasi AK, Parikh AR, Mahipal A. Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)-Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC). Cancers (Basel). 2022; 14:3078. https://doi.org/10.3390/cancers14133078 [PubMed]
- 21. Dang DK, Park BH. Circulating tumor DNA: current challenges for clinical utility. J Clin Invest. 2022; 132:e154941. https://doi.org/10.1172/JCI154941 [PubMed]
- 22. Bratman SV, Yang SY, Iafolla MA, Liu Z, Hansen AR, Bedard PL, Lheureux S, Spreafico A, Razak AA, Shchegrova S, Louie M, Billings P, Zimmermann B, et al. Personalized circulating tumor DNA analysis as a predictive biomarker in solid tumor patients treated with pembrolizumab. Nat Cancer. 2020; 1:873–81. https://doi.org/10.1038/s43018-020-0096-5 [PubMed]
- 23. Wong R, Tie J, Lee M, Cohen J, Wang Y, Li L, Ma S, Christie M, Kosmider S, Tomasetti C, Papadopoulos N, Kinzler KW, Vogelstein B, Gibbs P. The potential role of circulating tumor DNA (ctDNA) in the further investigation of colorectal cancer patients with nonspecific findings on standard investigations. Int J Cancer. 2019; 145:540–7. https://doi.org/10.1002/ijc.32117 [PubMed]
- 24. Shields MD, Chen K, Dutcher G, Patel I, Pellini B. Making the Rounds: Exploring the Role of Circulating Tumor DNA (ctDNA) in Non-Small Cell Lung Cancer. Int J Mol Sci. 2022; 23:9006. https://doi.org/10.3390/ijms23169006 [PubMed]
- 25. Rodda AE, Parker BJ, Spencer A, Corrie SR. Extending Circulating Tumor DNA Analysis to Ultralow Abundance Mutations: Techniques and Challenges. ACS Sens. 2018; 3:540–60. https://doi.org/10.1021/acssensors.7b00953 [PubMed]
- 26. Forshew T, Murtaza M, Parkinson C, Gale D, Tsui DW, Kaper F, Dawson SJ, Piskorz AM, Jimenez-Linan M, Bentley D, Hadfield J, May AP, Caldas C, et al. Noninvasive identification and monitoring of cancer mutations by targeted deep sequencing of plasma DNA. Sci Transl Med. 2012; 4:136ra68. https://doi.org/10.1126/scitranslmed.3003726 [PubMed]
- 27. Eluri M, Kopetz S, Parseghian CM. Truncal Dynamics May Trump: Serial ctDNA to Predict Early Therapeutic Response. Clin Cancer Res. 2023; 29:302–4. https://doi.org/10.1158/1078-0432.CCR-22-2793 [PubMed]
- 28. Liu Y, Li L, Tian Y, Zhu X, Sun A, Sun Y, Qiao Y, Qi X, Wang T. Analysis of KRAS mutations in circulating tumor DNA and colorectal cancer tissue. Biotech Histochem. 2021; 96:376–83. https://doi.org/10.1080/10520295.2020.1810775 [PubMed]
- 29. Zhou H, Liu H, Li J, Wang J, Fu X, Li Y, Mao S, Du J. Postoperative circulating tumor DNA detection and CBLB mutations are prognostic biomarkers for gastric cancer. Genes Genomics. 2023; 45:1037–46. https://doi.org/10.1007/s13258-023-01412-7 [PubMed]
- 30. Wen X, Pu H, Liu Q, Guo Z, Luo D. Circulating Tumor DNA-A Novel Biomarker of Tumor Progression and Its Favorable Detection Techniques. Cancers (Basel). 2022; 14:6025. https://doi.org/10.3390/cancers14246025 [PubMed]
- 31. Mouliere F, Thierry AR. The importance of examining the proportion of circulating DNA originating from tumor, microenvironment and normal cells in colorectal cancer patients. Expert Opin Biol Ther. 2012; 12 Suppl 1:S209–15. https://doi.org/10.1517/14712598.2012.688023 [PubMed]
- 32. Yang C, Huang X, Li Y, Chen J, Lv Y, Dai S. Prognosis and personalized treatment prediction in TP53-mutant hepatocellular carcinoma: an in silico strategy towards precision oncology. Brief Bioinform. 2021; 22:bbaa164. https://doi.org/10.1093/bib/bbaa164 [PubMed]
- 33. Chen L, Zhou Q, Liu J, Zhang W. CTNNB1 Alternation Is a Potential Biomarker for Immunotherapy Prognosis in Patients With Hepatocellular Carcinoma. Front Immunol. 2021; 12:759565. https://doi.org/10.3389/fimmu.2021.759565 [PubMed]
- 34. Meng GX, Yang CC, Yan LJ, Yang YF, Yan YC, Hong JG, Chen ZQ, Dong ZR, Li T. The somatic mutational landscape and role of the ARID1A gene in hepatocellular carcinoma. Heliyon. 2023; 9:e14307. https://doi.org/10.1016/j.heliyon.2023.e14307 [PubMed]
- 35. Moldogazieva NT, Zavadskiy SP, Terentiev AA. Genomic Landscape of Liquid Biopsy for Hepatocellular Carcinoma Personalized Medicine. Cancer Genomics Proteomics. 2021; 18:369–83. https://doi.org/10.21873/cgp.20266 [PubMed]
- 36. Nikanjam M, Kato S, Kurzrock R. Liquid biopsy: current technology and clinical applications. J Hematol Oncol. 2022; 15:131. https://doi.org/10.1186/s13045-022-01351-y [PubMed]
- 37. Mouliere F, Chandrananda D, Piskorz AM, Moore EK, Morris J, Ahlborn LB, Mair R, Goranova T, Marass F, Heider K, Wan JC, Supernat A, Hudecova I, et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci Transl Med. 2018; 10:eaat4921. https://doi.org/10.1126/scitranslmed.aat4921 [PubMed]
- 38. Tukachinsky H, Madison RW, Chung JH, Gjoerup OV, Severson EA, Dennis L, Fendler BJ, Morley S, Zhong L, Graf RP, Ross JS, Alexander BM, Abida W, et al. Genomic Analysis of Circulating Tumor DNA in 3,334 Patients with Advanced Prostate Cancer Identifies Targetable BRCA Alterations and AR Resistance Mechanisms. Clin Cancer Res. 2021; 27:3094–105. https://doi.org/10.1158/1078-0432.CCR-20-4805 [PubMed]
- 39. Tivey A, Church M, Rothwell D, Dive C, Cook N. Circulating tumour DNA - looking beyond the blood. Nat Rev Clin Oncol. 2022; 19:600–12. https://doi.org/10.1038/s41571-022-00660-y [PubMed]
- 40. Ziogas DE, Kyrochristos ID, Lykoudis EG, Roukos DH. Early solid tumor diagnosis through next-generation sequencing of cell-free DNA. Biomark Med. 2018; 12:1197–201. https://doi.org/10.2217/bmm-2018-0269 [PubMed]
- 41. Tarazona N, Gimeno-Valiente F, Gambardella V, Zuñiga S, Rentero-Garrido P, Huerta M, Roselló S, Martinez-Ciarpaglini C, Carbonell-Asins JA, Carrasco F, Ferrer-Martínez A, Bruixola G, Fleitas T, et al. Targeted next-generation sequencing of circulating-tumor DNA for tracking minimal residual disease in localized colon cancer. Ann Oncol. 2019; 30:1804–12. https://doi.org/10.1093/annonc/mdz390 [PubMed]
- 42. Liang W, Zhao Y, Huang W, Gao Y, Xu W, Tao J, Yang M, Li L, Ping W, Shen H, Fu X, Chen Z, Laird PW, et al. Non-invasive diagnosis of early-stage lung cancer using high-throughput targeted DNA methylation sequencing of circulating tumor DNA (ctDNA). Theranostics. 2019; 9:2056–70. https://doi.org/10.7150/thno.28119 [PubMed]
- 43. Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, Bartlett BR, Wang H, Luber B, Alani RM, Antonarakis ES, Azad NS, Bardelli A, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med. 2014; 6:224ra24. https://doi.org/10.1126/scitranslmed.3007094 [PubMed]
- 44. Larribère L, Martens UM. Advantages and Challenges of Using ctDNA NGS to Assess the Presence of Minimal Residual Disease (MRD) in Solid Tumors. Cancers (Basel). 2021; 13:5698. https://doi.org/10.3390/cancers13225698 [PubMed]
- 45. Metzenmacher M, Hegedüs B, Forster J, Schramm A, Horn PA, Klein CA, Bielefeld N, Ploenes T, Aigner C, Theegarten D, Schildhaus HU, Siveke JT, Schuler M, Lueong SS. Combined multimodal ctDNA analysis and radiological imaging for tumor surveillance in Non-small cell lung cancer. Transl Oncol. 2022; 15:101279. https://doi.org/10.1016/j.tranon.2021.101279 [PubMed]
- 46. Postel M, Roosen A, Laurent-Puig P, Taly V, Wang-Renault SF. Droplet-based digital PCR and next generation sequencing for monitoring circulating tumor DNA: a cancer diagnostic perspective. Expert Rev Mol Diagn. 2018; 18:7–17. https://doi.org/10.1080/14737159.2018.1400384 [PubMed]
- 47. Kaisaki PJ, Cutts A, Popitsch N, Camps C, Pentony MM, Wilson G, Page S, Kaur K, Vavoulis D, Henderson S, Gupta A, Middleton MR, Karydis I, et al. Targeted Next-Generation Sequencing of Plasma DNA from Cancer Patients: Factors Influencing Consistency with Tumour DNA and Prospective Investigation of Its Utility for Diagnosis. PLoS One. 2016; 11:e0162809. https://doi.org/10.1371/journal.pone.0162809 [PubMed]
- 48. Gale D, Lawson ARJ, Howarth K, Madi M, Durham B, Smalley S, Calaway J, Blais S, Jones G, Clark J, Dimitrov P, Pugh M, Woodhouse S, et al. Development of a highly sensitive liquid biopsy platform to detect clinically-relevant cancer mutations at low allele fractions in cell-free DNA. PLoS One. 2018; 13:e0194630. https://doi.org/10.1371/journal.pone.0194630 [PubMed]
- 49. Loft M, To YH, Gibbs P, Tie J. Clinical application of circulating tumour DNA in colorectal cancer. Lancet Gastroenterol Hepatol. 2023; 8:837–52. https://doi.org/10.1016/S2468-1253(23)00146-2 [PubMed]
- 50. Swanton C, Bernard E, Abbosh C, André F, Auwerx J, Balmain A, Bar-Sagi D, Bernards R, Bullman S, DeGregori J, Elliott C, Erez A, Evan G, et al. Embracing cancer complexity: Hallmarks of systemic disease. Cell. 2024; 187:1589–616. https://doi.org/10.1016/j.cell.2024.02.009 [PubMed]
- 51. Tan WB, Cheng W, Webber A, Bhambhani A, Duff MR, Kumar CV, McLendon GL. Endonuclease-like activity of heme proteins. J Biol Inorg Chem. 2005; 10:790–9. https://doi.org/10.1007/s00775-005-0028-y [PubMed]
- 52. Nguyen AH, Sim SJ. Nanoplasmonic biosensor: detection and amplification of dual bio-signatures of circulating tumor DNA. Biosens Bioelectron. 2015; 67:443–9. https://doi.org/10.1016/j.bios.2014.09.003 [PubMed]
- 53. Moreno-Manuel A, Calabuig-Fariñas S, Obrador-Hevia A, Blasco A, Fernández-Díaz A, Sirera R, Camps C, Jantus-Lewintre E. dPCR application in liquid biopsies: divide and conquer. Expert Rev Mol Diagn. 2021; 21:3–15. https://doi.org/10.1080/14737159.2021.1860759 [PubMed]
- 54. Sánchez-Martín V, López-López E, Reguero-Paredes D, Godoy-Ortiz A, Domínguez-Recio ME, Jiménez-Rodríguez B, Alba-Bernal A, Elena Quirós-Ortega M, Roldán-Díaz MD, Velasco-Suelto J, Linares-Valencia N, Garrido-Aranda A, Lavado-Valenzuela R, et al. Comparative study of droplet-digital PCR and absolute Q digital PCR for ctDNA detection in early-stage breast cancer patients. Clin Chim Acta. 2024; 552:117673. https://doi.org/10.1016/j.cca.2023.117673 [PubMed]
- 55. Tadimety A, Zhang Y, Kready KM, Palinski TJ, Tsongalis GJ, Zhang JX. Design of peptide nucleic acid probes on plasmonic gold nanorods for detection of circulating tumor DNA point mutations. Biosens Bioelectron. 2019; 130:236–44. https://doi.org/10.1016/j.bios.2019.01.045 [PubMed]
- 56. Das J, Ivanov I, Sargent EH, Kelley SO. DNA Clutch Probes for Circulating Tumor DNA Analysis. J Am Chem Soc. 2016; 138:11009–16. https://doi.org/10.1021/jacs.6b05679 [PubMed]
- 57. Lin C, Liu X, Zheng B, Ke R, Tzeng CM. Liquid Biopsy, ctDNA Diagnosis through NGS. Life (Basel). 2021; 11:890. https://doi.org/10.3390/life11090890 [PubMed]
- 58. Peng R, Zhang R, Li J. Continual Improvement of the Reliability of Next-Generation Sequencing-Based ctDNA Analysis: A Long-Term Comparison of ctDNA Detection in China. Clin Chem. 2022; 68:940–52. https://doi.org/10.1093/clinchem/hvac055 [PubMed]
- 59. Wu X, Zhu L, Ma PC. Next-Generation Novel Noninvasive Cancer Molecular Diagnostics Platforms Beyond Tissues. Am Soc Clin Oncol Educ Book. 2018; 38:964–77. https://doi.org/10.1200/EDBK_199767 [PubMed]
- 60. Akahori D, Inoue Y, Inui N, Karayama M, Yasui H, Hozumi H, Suzuki Y, Furuhashi K, Fujisawa T, Enomoto N, Nakamura Y, Suda T. Comparative assessment of NOIR-SS and ddPCR for ctDNA detection of EGFR L858R mutations in advanced L858R-positive lung adenocarcinomas. Sci Rep. 2021; 11:14999. https://doi.org/10.1038/s41598-021-94592-9 [PubMed]
- 61. Lyu X, Tsui YM, Ho DW, Ng IO. Liquid Biopsy Using Cell-Free or Circulating Tumor DNA in the Management of Hepatocellular Carcinoma. Cell Mol Gastroenterol Hepatol. 2022; 13:1611–24. https://doi.org/10.1016/j.jcmgh.2022.02.008 [PubMed]
- 62. Pelizzaro F, Cardin R, Penzo B, Pinto E, Vitale A, Cillo U, Russo FP, Farinati F. Liquid Biopsy in Hepatocellular Carcinoma: Where Are We Now? Cancers (Basel). 2021; 13:2274. https://doi.org/10.3390/cancers13092274 [PubMed]
- 63. Wu X, Li J, Gassa A, Buchner D, Alakus H, Dong Q, Ren N, Liu M, Odenthal M, Stippel D, Bruns C, Zhao Y, Wahba R. Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma. Int J Biol Sci. 2020; 16:1551–62. https://doi.org/10.7150/ijbs.44024 [PubMed]
- 64. Bearz A, Martini JF, Jassem J, Kim SW, Chang GC, Shaw AT, Shepard DA, Dall’O’ E, Polli A, Thurm H, Zalcman G, Garcia Campelo MR, Penkov K, et al. Efficacy of Lorlatinib in Treatment-Naive Patients With ALK-Positive Advanced NSCLC in Relation to EML4::ALK Variant Type and ALK With or Without TP53 Mutations. J Thorac Oncol. 2023; 18:1581–93. https://doi.org/10.1016/j.jtho.2023.07.023 [PubMed]
- 65. Judd J, Abdel Karim N, Khan H, Naqash AR, Baca Y, Xiu J, VanderWalde AM, Mamdani H, Raez LE, Nagasaka M, Pai SG, Socinski MA, Nieva JJ, et al. Characterization of KRAS Mutation Subtypes in Non-small Cell Lung Cancer. Mol Cancer Ther. 2021; 20:2577–84. https://doi.org/10.1158/1535-7163.MCT-21-0201 [PubMed]
- 66. Zhuang R, Li S, Li Q, Guo X, Shen F, Sun H, Liu T. The prognostic value of KRAS mutation by cell-free DNA in cancer patients: A systematic review and meta-analysis. PLoS One. 2017; 12:e0182562. https://doi.org/10.1371/journal.pone.0182562 [PubMed]
- 67. Cai Z, Chen G, Zeng Y, Dong X, Li Z, Huang Y, Xin F, Qiu L, Xu H, Zhang W, Su X, Liu X, Liu J. Comprehensive Liquid Profiling of Circulating Tumor DNA and Protein Biomarkers in Long-Term Follow-Up Patients with Hepatocellular Carcinoma. Clin Cancer Res. 2019; 25:5284–94. https://doi.org/10.1158/1078-0432.CCR-18-3477 [PubMed]
- 68. Cai ZX, Chen G, Zeng YY, Dong XQ, Lin MJ, Huang XH, Zhang D, Liu XL, Liu JF. Circulating tumor DNA profiling reveals clonal evolution and real-time disease progression in advanced hepatocellular carcinoma. Int J Cancer. 2017; 141:977–85. https://doi.org/10.1002/ijc.30798 [PubMed]
- 69. Pan A, Truong TN, Su YH, Dao DY. Circulating Biomarkers for the Early Diagnosis and Management of Hepatocellular Carcinoma with Potential Application in Resource-Limited Settings. Diagnostics (Basel). 2023; 13:676. https://doi.org/10.3390/diagnostics13040676 [PubMed]
- 70. Johnson P, Zhou Q, Dao DY, Lo YM. Circulating biomarkers in the diagnosis and management of hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2022; 19:670–81. https://doi.org/10.1038/s41575-022-00620-y [PubMed]
- 71. Xu Y, Cai J, Zhong K, Wen Y, Cai L, He G, Liao H, Zhang C, Fu S, Chen T, Cai J, Zhong X, Chen C, et al. Plasma-only circulating tumor DNA analysis detects minimal residual disease and predicts early relapse in hepatocellular carcinoma patients undergoing curative resection. Front Oncol. 2023; 13:1119744. https://doi.org/10.3389/fonc.2023.1119744 [PubMed]
- 72. Tang JC, Feng YL, Guo T, Xie AY, Cai XJ. Circulating tumor DNA in hepatocellular carcinoma: trends and challenges. Cell Biosci. 2016; 6:32. https://doi.org/10.1186/s13578-016-0100-z [PubMed]
- 73. Bardol T, Pageaux GP, Assenat E, Alix-Panabières C. Circulating Tumor DNA Clinical Applications in Hepatocellular Carcinoma: Current Trends and Future Perspectives. Clin Chem. 2024; 70:33–48. https://doi.org/10.1093/clinchem/hvad168 [PubMed]
- 74. Xu RH, Wei W, Krawczyk M, Wang W, Luo H, Flagg K, Yi S, Shi W, Quan Q, Li K, Zheng L, Zhang H, Caughey BA, et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat Mater. 2017; 16:1155–61. https://doi.org/10.1038/nmat4997 [PubMed]
- 75. Oversoe SK, Clement MS, Pedersen MH, Weber B, Aagaard NK, Villadsen GE, Grønbæk H, Hamilton-Dutoit SJ, Sorensen BS, Kelsen J. TERT promoter mutated circulating tumor DNA as a biomarker for prognosis in hepatocellular carcinoma. Scand J Gastroenterol. 2020; 55:1433–40. https://doi.org/10.1080/00365521.2020.1837928 [PubMed]
- 76. Hirai M, Kinugasa H, Nouso K, Yamamoto S, Terasawa H, Onishi Y, Oyama A, Adachi T, Wada N, Sakata M, Yasunaka T, Onishi H, Shiraha H, et al. Prediction of the prognosis of advanced hepatocellular carcinoma by TERT promoter mutations in circulating tumor DNA. J Gastroenterol Hepatol. 2021; 36:1118–25. https://doi.org/10.1111/jgh.15227 [PubMed]
- 77. Li Y, Wu J, Li E, Xiao Z, Lei J, Zhou F, Yin X, Hu D, Mao Y, Wu L, Wenjun L. TP53 mutation detected in circulating exosomal DNA is associated with prognosis of patients with hepatocellular carcinoma. Cancer Biol Ther. 2022; 23:439–45. https://doi.org/10.1080/15384047.2022.2094666 [PubMed]
- 78. Oversoe SK, Clement MS, Weber B, Grønbæk H, Hamilton-Dutoit SJ, Sorensen BS, Kelsen J. Combining tissue and circulating tumor DNA increases the detection rate of a CTNNB1 mutation in hepatocellular carcinoma. BMC Cancer. 2021; 21:376. https://doi.org/10.1186/s12885-021-08103-0 [PubMed]
- 79. Kumar S, Nadda N, Quadri A, Kumar R, Paul S, Tanwar P, Gamanagatti S, Dash NR, Saraya A, Sh, Nayak B. Assessments of TP53 and CTNNB1 gene hotspot mutations in circulating tumour DNA of hepatitis B virus-induced hepatocellular carcinoma. Front Genet. 2023; 14:1235260. https://doi.org/10.3389/fgene.2023.1235260 [PubMed]
- 80. Kurzrock R, Aggarwal C, Weipert C, Kiedrowski L, Riess J, Lenz HJ, Gandara D. Prevalence of ARID1A Mutations in Cell-Free Circulating Tumor DNA in a Cohort of 71,301 Patients and Association with Driver Co-Alterations. Cancers (Basel). 2022; 14:4281. https://doi.org/10.3390/cancers14174281 [PubMed]
- 81. Labgaa I, Villacorta-Martin C, D’Avola D, Craig AJ, von Felden J, Martins-Filho SN, Sia D, Stueck A, Ward SC, Fiel MI, Mahajan M, Tabrizian P, Thung SN, et al. A pilot study of ultra-deep targeted sequencing of plasma DNA identifies driver mutations in hepatocellular carcinoma. Oncogene. 2018; 37:3740–52. https://doi.org/10.1038/s41388-018-0206-3 [PubMed]
- 82. Ge Z, Helmijr JC, Jansen MP, Boor PP, Noordam L, Peppelenbosch M, Kwekkeboom J, Kraan J, Sprengers D. Detection of oncogenic mutations in paired circulating tumor DNA and circulating tumor cells in patients with hepatocellular carcinoma. Transl Oncol. 2021; 14:101073. https://doi.org/10.1016/j.tranon.2021.101073 [PubMed]
- 83. Chan KC, Lai PB, Mok TS, Chan HL, Ding C, Yeung SW, Lo YM. Quantitative analysis of circulating methylated DNA as a biomarker for hepatocellular carcinoma. Clin Chem. 2008; 54:1528–36. https://doi.org/10.1373/clinchem.2008.104653 [PubMed]
- 84. Lim HY, Merle P, Weiss KH, Yau T, Ross P, Mazzaferro V, Blanc JF, Ma YT, Yen CJ, Kocsis J, Choo SP, Sukeepaisarnjaroen W, Gérolami R, et al. Phase II Studies with Refametinib or Refametinib plus Sorafenib in Patients with RAS-Mutated Hepatocellular Carcinoma. Clin Cancer Res. 2018; 24:4650–61. https://doi.org/10.1158/1078-0432.CCR-17-3588 [PubMed]
- 85. Wong IH, Leung T, Ho S, Lau WY, Chan M, Johnson PJ. Semiquantification of circulating hepatocellular carcinoma cells by reverse transcriptase polymerase chain reaction. Br J Cancer. 1997; 76:628–33. https://doi.org/10.1038/bjc.1997.436 [PubMed]
- 86. Nahmias Y, Goldwasser J, Casali M, van Poll D, Wakita T, Chung RT, Yarmush ML. Apolipoprotein B-dependent hepatitis C virus secretion is inhibited by the grapefruit flavonoid naringenin. Hepatology. 2008; 47:1437–45. https://doi.org/10.1002/hep.22197 [PubMed]
- 87. Temraz S, Nasr R, Mukherji D, Kreidieh F, Shamseddine A. Liquid biopsy derived circulating tumor cells and circulating tumor DNA as novel biomarkers in hepatocellular carcinoma. Expert Rev Mol Diagn. 2022; 22:507–18. https://doi.org/10.1080/14737159.2022.2094706 [PubMed]
- 88. Ng CK, Di Costanzo GG, Tosti N, Paradiso V, Coto-Llerena M, Roscigno G, Perrina V, Quintavalle C, Boldanova T, Wieland S, Marino-Marsilia G, Lanzafame M, Quagliata L, et al. Genetic profiling using plasma-derived cell-free DNA in therapy-naïve hepatocellular carcinoma patients: a pilot study. Ann Oncol. 2018; 29:1286–91. https://doi.org/10.1093/annonc/mdy083 [PubMed]
- 89. Marchio A, Amougou Atsama M, Béré A, Komas NP, Noah Noah D, Atangana PJ, Camengo-Police SM, Njouom R, Bekondi C, Pineau P. Droplet digital PCR detects high rate of TP53 R249S mutants in cell-free DNA of middle African patients with hepatocellular carcinoma. Clin Exp Med. 2018; 18:421–31. https://doi.org/10.1007/s10238-018-0502-9 [PubMed]
- 90. Zhang Y, Yao Y, Xu Y, Li L, Gong Y, Zhang K, Zhang M, Guan Y, Chang L, Xia X, Li L, Jia S, Zeng Q. Pan-cancer circulating tumor DNA detection in over 10,000 Chinese patients. Nat Commun. 2021; 12:11. https://doi.org/10.1038/s41467-020-20162-8 [PubMed]
- 91. Kaseb AO, Sánchez NS, Sen S, Kelley RK, Tan B, Bocobo AG, Lim KH, Abdel-Wahab R, Uemura M, Pestana RC, Qiao W, Xiao L, Morris J, et al. Molecular Profiling of Hepatocellular Carcinoma Using Circulating Cell-Free DNA. Clin Cancer Res. 2019; 25:6107–18. https://doi.org/10.1158/1078-0432.CCR-18-3341 [PubMed]
- 92. Park S, Lee EJ, Rim CH, Seong J. Plasma Cell-Free DNA as a Predictive Marker after Radiotherapy for Hepatocellular Carcinoma. Yonsei Med J. 2018; 59:470–9. https://doi.org/10.3349/ymj.2018.59.4.470 [PubMed]
- 93. Fujii Y, Ono A, Hayes CN, Aikata H, Yamauchi M, Uchikawa S, Kodama K, Teraoka Y, Fujino H, Nakahara T, Murakami E, Miki D, Okamoto W, et al. Identification and monitoring of mutations in circulating cell-free tumor DNA in hepatocellular carcinoma treated with lenvatinib. J Exp Clin Cancer Res. 2021; 40:215. https://doi.org/10.1186/s13046-021-02016-3 [PubMed]
- 94. Ng CK, Di Costanzo GG, Terracciano LM, Piscuoglio S. Circulating Cell-Free DNA in Hepatocellular Carcinoma: Current Insights and Outlook. Front Med (Lausanne). 2018; 5:78. https://doi.org/10.3389/fmed.2018.00078 [PubMed]
- 95. Ono A, Fujimoto A, Yamamoto Y, Akamatsu S, Hiraga N, Imamura M, Kawaoka T, Tsuge M, Abe H, Hayes CN, Miki D, Furuta M, Tsunoda T, et al. Circulating Tumor DNA Analysis for Liver Cancers and Its Usefulness as a Liquid Biopsy. Cell Mol Gastroenterol Hepatol. 2015; 1:516–34. https://doi.org/10.1016/j.jcmgh.2015.06.009 [PubMed]
- 96. Magbanua MJ, Li W, Wolf DM, Yau C, Hirst GL, Swigart LB, Newitt DC, Gibbs J, Delson AL, Kalashnikova E, Aleshin A, Zimmermann B, Chien AJ, et al. Circulating tumor DNA and magnetic resonance imaging to predict neoadjuvant chemotherapy response and recurrence risk. NPJ Breast Cancer. 2021; 7:32. https://doi.org/10.1038/s41523-021-00239-3 [PubMed]