



Introduction
Liver cancer, of which hepatocellular carcinoma (HCC) is the most common type, is the second cause of cancer-related deaths worldwide in 2018 [1]. Even though transplant and surgical resection treatment are the most popular strategies for HCC, there are still considerable patients diagnosed at an advanced stage who have lost the chance [2]. In the past few years, trans-arterial (chemo)-embolization (TAE/TACE) has been a prioritized treatment option for HCC patients who were at an intermediate stage, and the strategy has been proven to be effective and safe [3]. Patients treated by TAE/TACE demonstrated an acceptable general status with a relatively lower rate of liver insufficiency [4].
Patients who were diagnosed with HCC usually suffered from changes in muscle, which included changes in quantity, such as sarcopenia, and changes in structural composition, such as myosteatosis, which could affect curative effectiveness of TAE/TACE in HCC patients. More than 90% of HCC patients were diagnosed with cirrhosis, which was usually associated with sarcopenia [5]. Sarcopenia was usually calculated by normalized cross-sectional muscle area at the level of L3 on an abdominal CT scan before embolization by patient’s height and was defined as a lower skeletal muscle index (SMI) or psoas muscle index (PMI) [6]. Recent studies pointed out that sarcopenia was related to a lower overall survival and objective response rates in HCC patients who were treated by TAE/TACE, and the SMI and PMI can be adopted as predictive indicators. Nonetheless, conclusions varied since other studies reached contradictory opinions on the predictive values of sarcopenia in the prognosis of HCC [7–16]. In addition to the loss of muscle, fatty infiltration of muscle is another important clinical outcome of HCC and is usually related to a worse prognosis, however, evidence from the relative studies were limited and the ultimate conclusion still needs to be further validated [17, 18]. Myosteatosis is used to describe fatty infiltration and can be diagnosed by CT scanning using muscle radiation attenuation.
To further clarify the predictive values of the changes of muscle, both the changes of quantity and quality of muscle in the HCC patients who were treated by TAE or TACE, we conducted a meta-analysis to provide the evidence-based results for the predictive values of sarcopenia, SMI, PMI and the myosteatosis in regard to the impact of survival outcomes and tumor response in HCC patients treated by TAE or TACE, thereby assisting in optimizing therapeutic strategies and maximizing clinical benefits for HCC patients.
Methods
Literature search strategies
The present study was conducted strictly with the instruction of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. In this meta-analysis, databases including PubMed (https://pubmed.ncbi.nlm.nih.gov/), EMBASE (https://www.embase.com/), Cochrane Library (https://www.cochranelibrary.com/) were adopted to complete the literature review before June 19, 2023. Mesh terms and entry terms included “sarcopenia” (Mesh), “skeletal muscle index”, “psoas muscle index”, “SMI”, “PMI”, “subcutaneous adipose index”, “SAI”, “subcutaneous fat index”, “SFI”, “visceral adipose index”, “VAI”, “visceral fat index”, “VFI”, “intramuscular adipose index”, “IMAI”, “intramuscular fat index”, “IMFI”, “muscle surface area”, “MSA”, “skeletal muscle density”, “SMD”, “myosteatosis”, “sarcopenic”, “myopenia”, “transarterial embolization”, “TAE”, “transcatheter intra-arterial therapy”, “transcatheter intra-arterial therapies”, “Transcatheter arterial chemoembolization”, “transarterial chemoembolization”, “trans-arterial chemoembolization”, “TACE”, and those terms were searched. Besides, Google Scholar was also used to complete a gray literature search and we also manually retrieved the relative reference of the qualified publications to find more targeted reports. The specific search strategy in PubMed is shown in Supplementary File 1.
Inclusion and exclusion criteria
For the literature review, the inclusion criteria include: (1) patients diagnosed with HCC; (2) patients treated with TAE or TACE; (3) studies evaluated the predictive values of sarcopenia, myosteatosis, SMI, and PMI; (4) researches provided at least one of the following outcomes (overall survival (OS), objective response rate (ORR), disease control rates (DCR)). The exclusion criteria include: (1) duplicated reports; (2) conference abstracts, case reports, and comments; (3) studies with overlapping patient populations. Only articles with the most complete data and rigorous methodology were selected.
Data extraction and quality assessment
Data extraction mainly focused on the authors, study design, study period, treatment, study region, sample size, gender, the age of patients, outcomes, and so on. We used the Newcastle–Ottawa Scale (NOS) score to assess the quality of collected studies [19]. Studies with scores higher than six were classified as high-quality research. All of the above steps, i.e., literature search, screening, data extraction, and literature quality assessment were done independently and cross-checked by two authors, and the senior author was consulted in case of disputes.
Statistical analysis
Stata 15.0 was used to conduct statistical analyses. The relationships between the sarcopenia, myosteatosis, SMI, PMI and the overall survival in TAE or TACE treated HCC patients were calculated by the hazard ratio (HR) with a 95% confidence interval (95% CI). The odds ratio (OR) with a 95% CI was used to describe the relationship between above indicators and the ORR or DCR in TAE or TACE treated HCC patients. Include four studies reported ORR by combining partial response and complete response. The statistical heterogeneity was calculated using the chi-squared test. p < 0.1 and I2 > 50% were defined as high heterogeneity and a random effect model would be applied when it occurred. Otherwise, the fixed effect model was used [20]. The tests of Egger [21] and Begg [22] were employed to evaluate publication bias. The sensitivity analysis was conducted by the leave-one-out method to evaluate the stability of results [23].
Results
Characteristics of included studies
As shown in Figure 1, a total of 167 studies were collected. After removing 62 duplicate articles, 105 studies were assessed by title and abstract with 19 qualified articles. After reading full texts, one repeated publication and 6 unrelated studies were excluded. 12 studies involving 2559 participants were included in the systematic review ultimately. More detailed information about the eligible assessment of studies is provided in Figure 1. The baseline information of included studies is shown in Table 1. All the studies were evaluated with scores of more than six, which represented high-quality studies. Included in all studies was the use of CT to assess body composition at the third lumbar level.
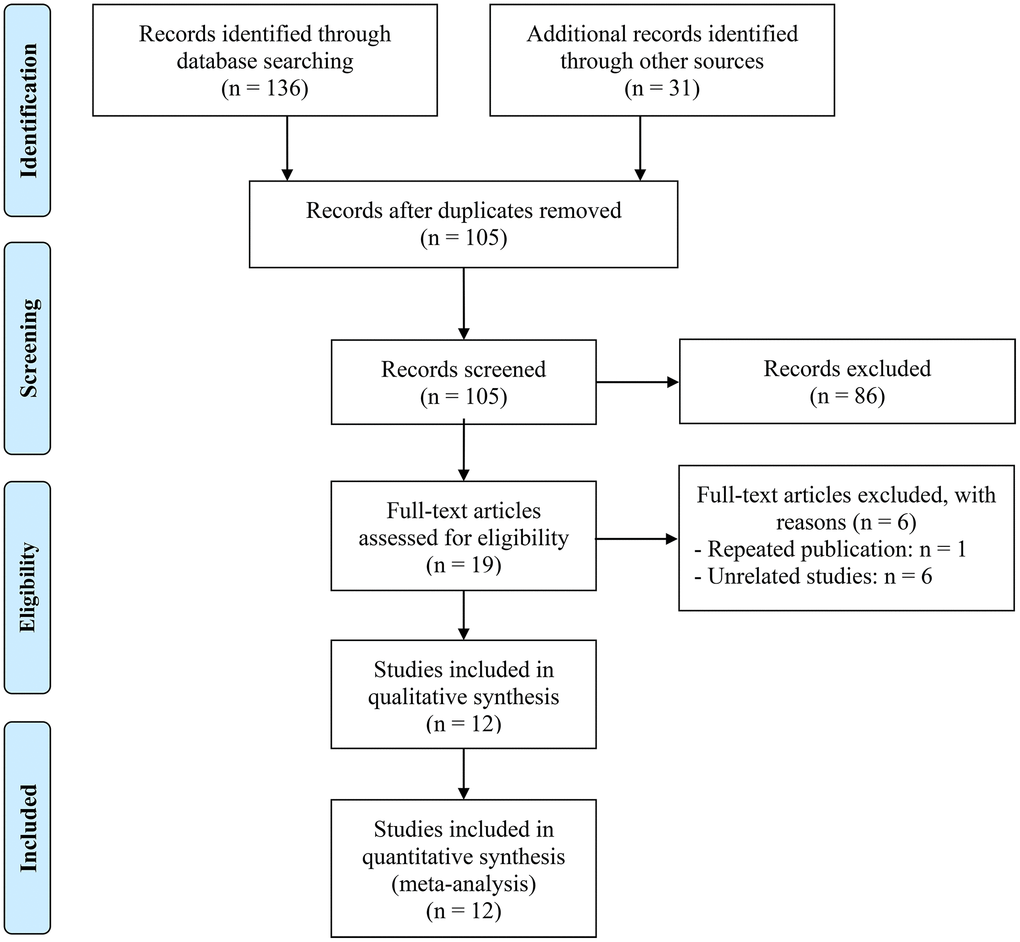
Figure 1. The flowchart of the literature review.
Table 1. Main characteristics of the studies included.
| Study | Study design | Study period | Treatment | Study region | Sample size | Gender (male/female) | Age (years) | Outcomes | Methods, sites, and cut-off (male/female) | NOS Score | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wang et al. 2023 | R | 06/2013–12/2019 | TACE | China | 364 | 300/64 | 58 (50–66)a | SMI (OS) | CT, L3, 49/36 cm2/m2 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Loosen et al. 2023 | R | 2011–2021 | TACE | Germany | 89 | 61/28 | 69 (23–90)b | SMI (OS) | CT, L3, CV | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bannangkoon et al. 2023 | R | 01/2008–12/2019 | TACE | Thailand | 611 | 445/166 | 61.4 ± 10.9 | SMI (OS, ORR), Myosteatosis (OS) | CT, L3, 36.2/29.6 cm2/m2; 44.4/39.3 HU | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Zhang et al. 2022 | R | 01/2018–03/2019 | TACE | China | 228 | 175/53 | 58.9 ± 11.0 | SMI (OS), PMI (OS) | CT, L3, 46/34 cm2/m2; 42.3/37.4 mm/m2 | 8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yang et al. 2022 | R | 01/2015–12/2020 | TACE | China | 62 | 49/13 | 59.4 ± 10.6 | SMI (OS) | CT, L3, 42/38 cm2/m2 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Roth et al. 2022 | R | 12/2007–12/2014 | TACE/TAE | France | 225 | 200/25 | 65 (58–75)a | SMI (OS, ORR, DCR) | CT, L3, 50/39 cm2/m2 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Masetti et al. 2022 | R | 03/2011–07/2019 | TAE | Italy | 151 | 116/35 | 73.2 ± 9.3 | Myosteatosis (OS) | CT, L3, 0.44/0.31c | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chien et al. 2022 | R | 01/2010–08/2015 | TACE | Taiwan | 260 | 192/68 | 64.0 ± 18.0 | PMI (OS) | CT, L3, 6.4/3.9 cm2/m2 | 8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Li et al. 2021 | R | 2008–2018 | TACE | China | 192 | 157/35 | 60 (52–67)a | SMI (OS) | CT, L3, CV | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lanza et al. 2020 | R | 03/2011–07/2019 | TAE | Italy | 142 | 110/32 | 73 (40–88)b | SMI (OS) | CT, L3, 55/39 cm2/m2 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Loosen et al. 2019 | R | 2013–2018 | TACE | Germany | 56 | 44/12 | 65 (30–89)b | PMI (OS, ORR) | CT, L3, 11.8/11.8 mm/m2 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fujita et al. 2019 | R | 01/2006–03/2017 | TACE | Japan | 179 | 130/49 | 72 (64–78)a | PMI (OS, ORR, DCR) | CT, L3, 6.0/3.4 cm2/m2 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| amedians (interquartile range); bmedians (ranges); cmyosteatosis were intramuscular adipose tissue content (IMAC) > −0.44 in males and > −0.31 in females. Abbreviations: R: retrospective analysis; TACE: trans-arterial chemoembolization; TAE: trans-arterial embolization; SMI: skeletal muscle index; PMI: psoas muscle index; OS: overall survival; ORR: objective response rate; DCR: disease control rates; L3: third lumbar vertebra; CT: computed tomography; CV: continuous variable. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The predictive value of sarcopenia in TAE or TACE treated HCC patients
Eight studies including 2559 patients reported the relationship between sarcopenia and overall survival. There was no significant heterogeneity found among included studies, so a fixed-effect model was applied. As shown in Figure 2A, the meta-analysis assisted that the sarcopenia was significantly related to a shorter OS of HCC patients who were treated by TAE or TACE (HR: 1.46, 95% CI: 1.30–1.64, p < 0.001). In the subgroup analysis, six studies using multivariate analysis supported that the sarcopenia was devoted to a shorter OS (HR: 1.42, 95% CI: 1.24–1.62, p < 0.001). In the univariate analysis group, which included only three studies, sarcopenia was also significantly associated with shorter OS (HR: 1.64, 95% CI: 1.26–2.14, p < 0.001). In all, sarcopenia could predict a shorter OS in HCC patients who were treated by TAE or TACE. More detailed information about the subgroup analysis is provided in Figure 2B.
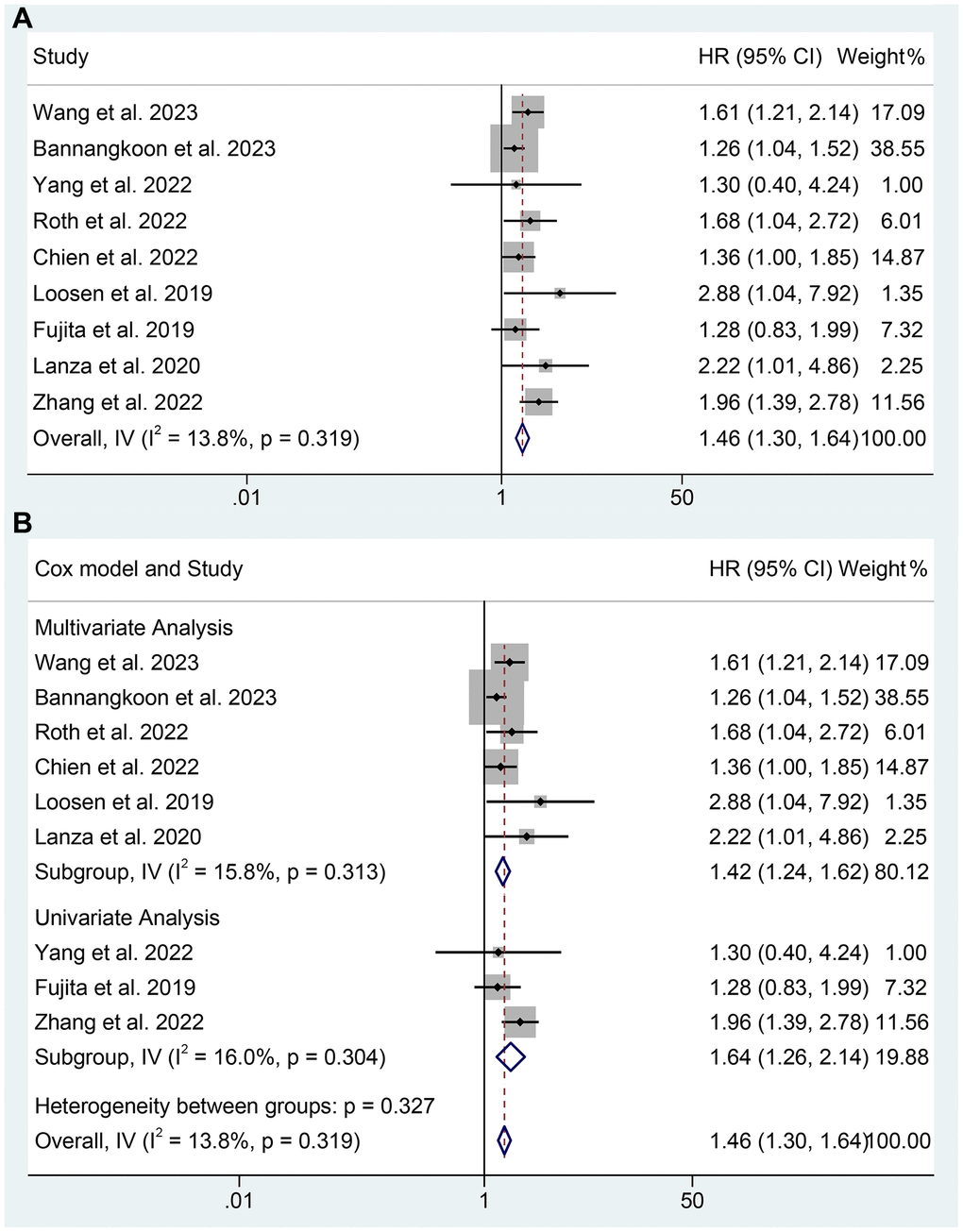
Figure 2. The relationship between sarcopenia and OS in TAE or TACE treated HCC patients. (A) The overall analysis; (B) Subgroup analysis including multivariate analysis and univariate analysis.
Apart from the OS, four studies provided the ORR and 2 studies provided DCR of TAE or TACE treated HCC patients. As shown in Figure 3, the meta-analysis suggested that sarcopenia was significantly associated with lower ORR of TAE or TACE treated HCC patients (OR: 0.80, 95% CI: 0.65–0.98, p = 0.032). However, there was no statistical difference in DCR (OR: 0.63, 95% CI: 0.39–1.03, p = 0.064). In consideration of the limited sample size and studies of DCR, the conclusion should be further validated.
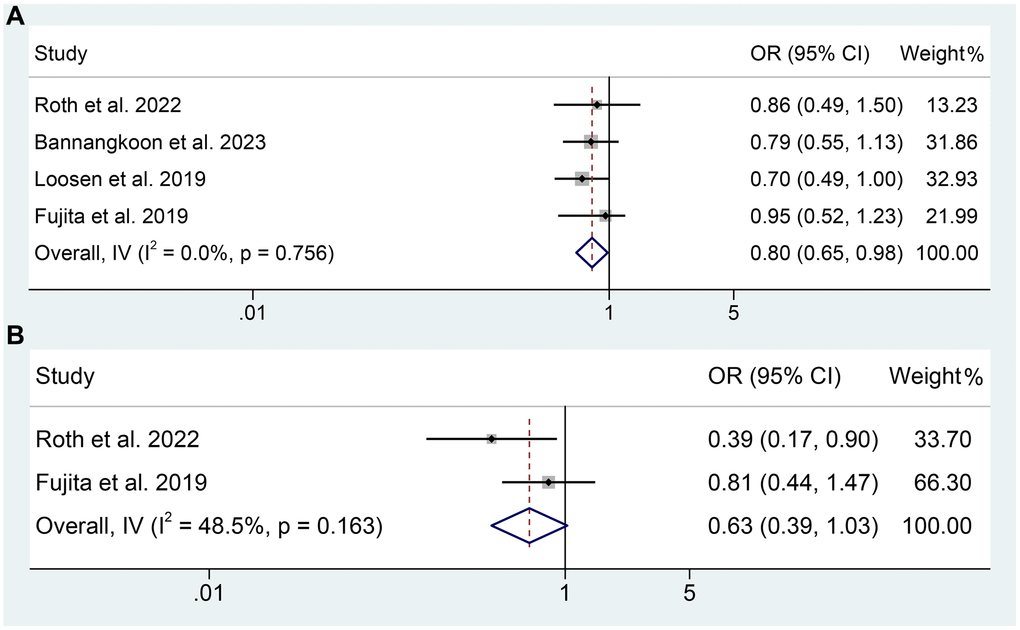
Figure 3. (A) The relationship between sarcopenia and ORR in TAE or TACE treated HCC patients; (B) The relationship between sarcopenia and DCR in TAE or TACE treated HCC patients.
The Cochran Q test and I2 statistics showed no significant heterogeneity (overall OS: I2 = 13.8%, p = 0.319; multivariate analysis of OS: I2 = 15.8%, p = 0.313; univariate analysis of OS: I2 = 16.0%, p = 0.304; ORR: I2 = 0, p = 0.756; DCR: I2 = 48.5%, p = 0.163), thus a fixed-effect model was utilized.
The predictive value of SMI in TAE or TACE treated HCC patients
In the meta-analysis, six studies provided the SMI level of patients. Taking the SMI as a binary variable, the low SMI was related to a shorter OS of TAE or TACE treated HCC patients (HR: 1.48, 95% CI: 1.29–1.69, p < 0.001). The subgroup analysis reached the same conclusion (multivariate analysis, HR: 1.41, 95% CI: 1.22–1.63, p < 0.001; univariate analysis, HR: 1.90, 95% CI: 1.36–2.65, p < 0.001). In conclusion, the SMI could effectively predict the OS of TAE or TACE treated HCC patients (Figure 4). There was no significant heterogeneity was found (overall OS: I2 = 28.3%, p = 0.222; multivariate analysis of OS: I2 = 24.8%, p = 0.262; univariate analysis of OS: I2 = 0, p = 0.515), thus a fixed-effect model was used.
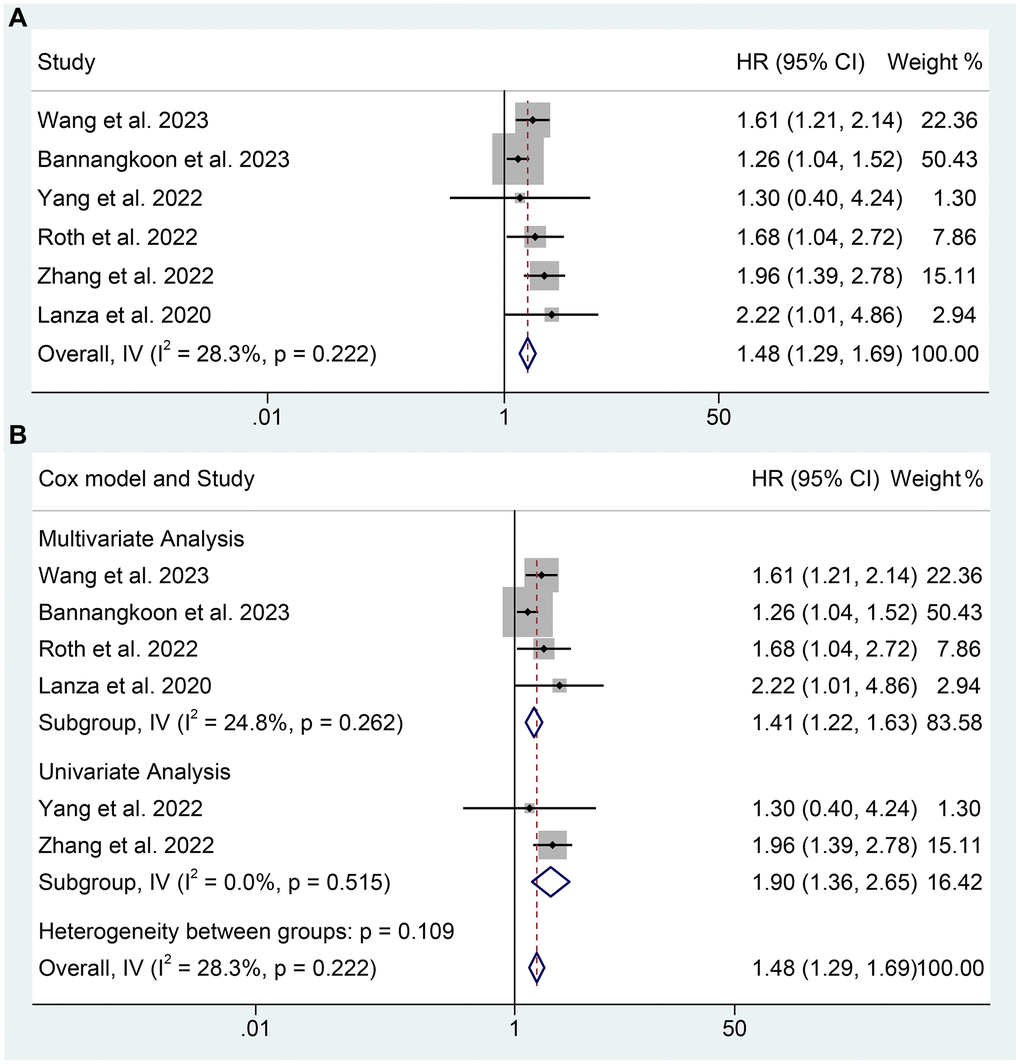
Figure 4. The relationship between SMI and OS in TAE or TACE treated HCC patients. (A) Taking the SMI as a binary variable; (B) Subgroup analysis of figure A.
Besides, three studies by Loosen et al. (HR: 0.90, 95% CI: 0.83–0.98, p = 0.014), Roth et al. (HR: 0.99, 95% CI: 0.97–1.01, p = 0.19), and Li et al. (HR: 0.98, 95% CI: 0.97–1.00, p = 0.028), which considered SMI as a continuous variable, also found the lower SMI contributed to the shorter OS of TAE or TACE-treated HCC patients.
The predictive value of PMI and myosteatosis in TAE or TACE treated HCC patients
As for the PMI, four studies reported the relationship between the PMI and OS of TAE or TACE treated HCC patients. As shown in Figure 5A, the meta-analysis results indicated that lower PMI was closely related to a shorter OS (HR: 1.45, 95% CI: 1.19–1.77, p < 0.001). No significant heterogeneity was observed among the included studies (I2 = 5.8%, p = 0.495). As a result, a fixed-effects model was employed.
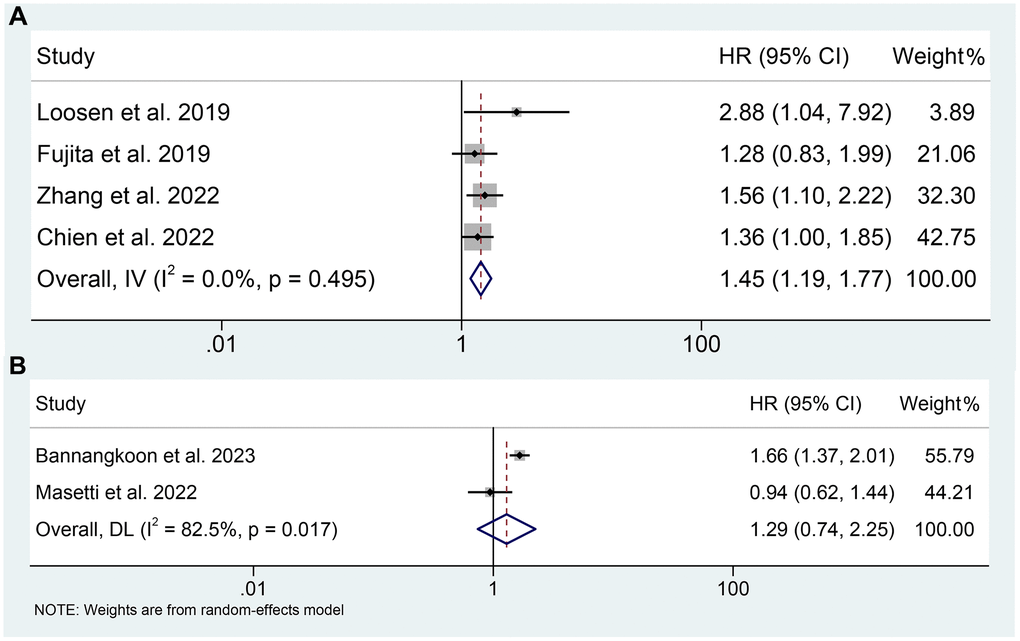
Figure 5. (A) The relationship between PMI and OS in TAE or TACE treated HCC patients; (B) The relationship between myosteatosis and OS in TAE or TACE treated HCC patients.
After the literature review, there were two studies reported the relationship between the myosteatosis and the OS of TAE or TACE treated HCC patients. However, their conclusions were contradictory. The meta-analysis using pooled data from 762 patients supported that there was no significant association between myosteatosis and OS (HR: 1.29, 95% CI: 0.74–2.25, p = 0.366). More detailed information is provided in Figure 5B. There was an obvious heterogeneity among the included studies and a random-forest model was adopted for analysis.
Publication bias and sensitivity analysis
The funnel plot was provided in Figure 6 which described the publication bias. There was no significant publication bias found in Egger’s test (sarcopenia and OS, p = 0.109; SMI and OS, p = 0.234) or Begg’s test (sarcopenia and OS, p = 0.348; SMI and OS, p = 1.000).
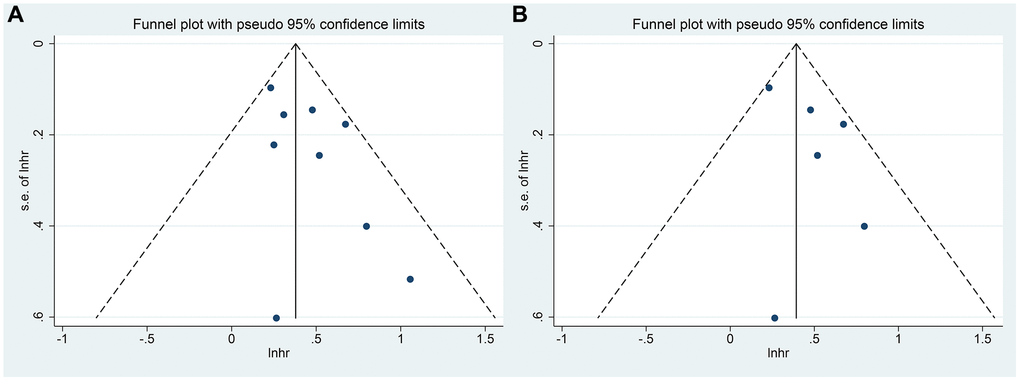
Figure 6. (A) The funnel plot of the impact of sarcopenia on OS in TAE or TACE treated HCC patients; (B) The funnel plot of the impact of SMI on OS in TAE or TACE treated HCC patients.
In the present study, we adopted the leave-one-out method to conduct the sensitivity analysis to evaluate the impact of each included study on the combined results. The impact of sarcopenia and SMI on the OS of TAE/TACE treated HCC patients was the primary endpoint that we investigated in the meta-analysis, as a result, we conducted the sensitivity analysis of studies concerning the relationship between sarcopenia, SMI and the OS. HR from the pooled data has not significantly changed after excluding one study at a time, ranging from 1.40 (95% CI: 1.24–1.59, after omitting Zhang et al. 2022) to 1.60 (95% CI: 1.38–1.86, after omitting Bannangkoon et al. 2023). A similar conclusion was reached in the SMI, of which the HR ranged from 1.41 (95% CI: 1.22–1.63, after omitting Zhang et al. 2022) to 1.75 (95% CI: 1.44–2.11, after omitting Bannangkoon et al. 2023). The aforementioned analysis proved that conclusions of the meta-analysis we conducted were stable and reliable. Figure 7 provides detailed information on the sensitivity analysis.
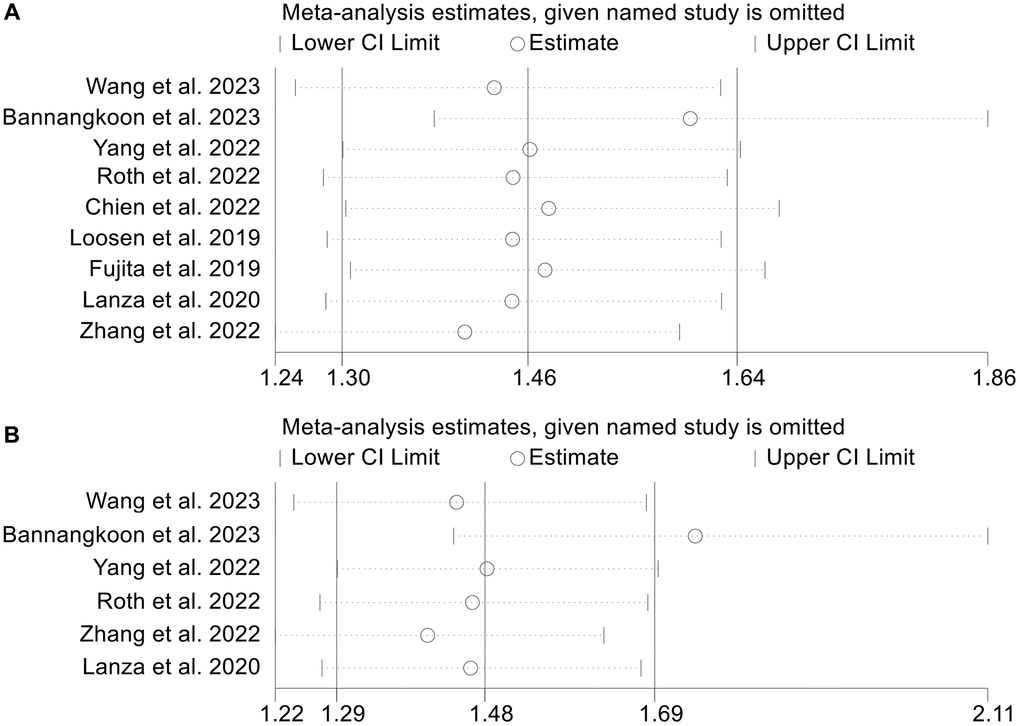
Figure 7. (A) The sensitivity analysis of the impact of sarcopenia on OS in TAE or TACE treated HCC patients; (B) The sensitivity analysis of the impact of SMI on OS in TAE or TACE treated HCC patients.
Discussion
In the present study, we conducted a meta-analysis with several subgroup analyses to investigate the relationship between sarcopenia, SMI, PMI, myosteatosis, and the prognosis of TAE or TACE treated HCC patients. Sarcopenia is a significant predictive indicator for the worse prognosis of TAE or TACE treated HCC patients both in the OS and the ORR. As important diagnostic indicators of sarcopenia, the SMI and PMI could also effectively predict the OS of TAE/TACE treated HCC patients. Different from sarcopenia which mainly represents the progressive loss of muscle mass and strength, myosteatosis is used to describe the fatty infiltration of muscle assessed by CT scanning, both in myocytes (intramyocellular fat) and in muscle fascia (intermuscular fat). Different from SMI, PMI and sarcopenia, the present meta-analysis didn’t find any impact of myosteatosis on OS of TAE or TACE treated HCC patients. Hence, may it be the loss of muscle rather than the fatty infiltration of muscle that contributes to the poor prognosis of TAE/TACE treated HCC patients. However in consideration of the limited number of myosteatosis studies, the conclusion should be further validated.
Previous studies pointed out that sarcopenia was related to worse outcomes when patients underwent major surgery [5, 24, 25] and it was an unfavorable prognostic factor for patients with cirrhosis and HCC treated by TAE or TACE [7]. It remains debatable whether sarcopenia could impact the prognosis of HCC undergoing TAE or TACE. Some studies did not find a relationship between sarcopenia and prognosis of HCC patients [8, 16]. In contrast, studies with larger sample sizes and lower heterogeneous patient populations revealed that sarcopenia was an independent predictive indicator for TAE/TACE treated HCC patients [7, 10, 12–14, 17]. In our meta-analysis, pooled data from 1932 patients supported that sarcopenia was an independent poor prognostic factor for TAE or TACE treated HCC patients both in OS and in ORR. Usually, we can observe a high prevalence of sarcopenia in TAE or TACE treated HCC patients. Especially, HCC in sarcopenic patients was in a more advanced stage with larger tumor size and number [6]. Thus, along with TACE or not, systemic therapy with either tyrosine kinase inhibitors checkpoint inhibitors, or radiotherapy should be considered for sarcopenic patients with unresectable HCC in an advanced stage to maximize the benefits for patients [26, 27]. It is noteworthy that even though sarcopenia is an independent poor prognostic factor of TAE or TACE treated HCC patients, it is not associated with a higher rate of post-TAE or TACE complications so that it does not impair the safety of the TAE or TACE. Therefore, sarcopenia should not be treated as an exclusion criterion for TAE or TACE in HCC patients [13].
Older age, male tendency, and lower BMI were found to be closely related to sarcopenia. Nasimi et al. found older age and lower BMI increased the risk of SMI. As the main diagnostic indicator of sarcopenia, SMI has cut-off values for sarcopenia at ≤39 cm2/m2 for women and ≤55 cm2/m2 for men. When taking SMI as a binary variable following the above cut-off value, it could effectively predict the OS of TAE or TACE treated HCC patients according to present meta-analysis. In clinical practice, more efforts should be put into the increase of SMI to improve the OS of TAE or TACE treated HCC patients. According to previous studies, physical exercises could help to strengthen the muscles and significantly increase SMI [28, 29]. Similar to SMI, PMI, as one of the important indicators for muscle loss and the other diagnostic criterion of sarcopenia, also demonstrated a close association with prognosis in HCC in the study. Both SMI and PMI are famous prognostic predictors and are simple to assess. However, in previous studies, SMI seemed to be more robust and it could completely measure the muscle mass and was more popular in predicting the prognosis of various diseases compared to PMI [11, 13, 30].
Myosteatosis was also highly prevalent in HCC patients and has been proven to be an important prognostic factor for hepatobiliary and pancreatic malignancies [31]. However, its impact on prognosis is straightforward. In most relevant studies, myosteatosis did not demonstrate any impact on OS and complications [31]. In our study, the included two studies reached contrary conclusions. Bannangkoon et al. found myosteatosis was associated with the OS of TAE or TACE treated HCC patients [17], but the study from Masetti et al. pointed out there was no significant impact of myosteasis on the OS of TAE or TACE treated HCC patients [18], which was consistent with our meta-analysis. In consideration of the limited sample size and the long period of Masetti’s study, the impact of myosteasis on OS in TAE or TACE treated HCC should be further validated with a multicenter, larger sample size study in different populations.
There are some inherent limitations in our study. Firstly, the meta-analysis was conducted on published studies and the limited sample size constrained us from detailed subgroup analysis. There were only two studies involving myosteasis and the OS in TAE or TACE treated HCC. Also, the analysis of SMI, PMI, and myosteasis on ORR, and DCR was absent due to the lack of relevant studies. Secondly, all included studies were retrospectively designed. More strict prospective trials should be required to exclude confounding influence. Lastly, included studies of SMI, PMI and myosteasis did not adopt the same cut-off value for diagnosis, which should be optimized.
In conclusion, the present meta-analysis proved that sarcopenia with its diagnosis indicators, SMI and PMI were significant prognostic factors for TAE or TACE treated HCC patients. While myosteasis has a non-prognostic impact on the OS of TAE or TACE treated HCC patients. The findings could support more comprehensive therapeutic strategies to maximize the benefits for HCC patients in clinical practice.
Supplementary Materials
Author Contributions
Jing Long and Qiang Wang conceived and designed the study. Jing Long, Xin Zhang, and Wei Mi were responsible for the collection and assembly of data, data analysis, and interpretation. Jing Long, Jianjun Shi, and Hongwei Ren were involved in writing the manuscript. Jing Long and Qiang Wang revised the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement
All clinical information and data for the meta-analysis of the present manuscript were obtained from public databases, and therefore, the ethical approval and informed consent are not required and can be exempted.
Funding
This work was not supported by any funds.
References
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. https://doi.org/10.3322/caac.21492 [PubMed]
- 2. Zhang L, Feng J, Kuang T, Chai D, Qiu Z, Deng W, Dong K, Zhao K, Wang W. Blood biomarkers predict outcomes in patients with hepatocellular carcinoma treated with immune checkpoint Inhibitors: A pooled analysis of 44 retrospective sudies. Int Immunopharmacol. 2023; 118:110019. https://doi.org/10.1016/j.intimp.2023.110019 [PubMed]
- 3. Lee EW, Khan S. Recent advances in transarterial embolotherapies in the treatment of hepatocellular carcinoma. Clin Mol Hepatol. 2017; 23:265–72. https://doi.org/10.3350/cmh.2017.0111 [PubMed]
- 4. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018; 69:182–236. https://doi.org/10.1016/j.jhep.2018.03.019 [PubMed]
- 5. Fielding RA, Vellas B, Evans WJ, Bhasin S, Morley JE, Newman AB, Abellan van Kan G, Andrieu S, Bauer J, Breuille D, Cederholm T, Chandler J, De Meynard C, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011; 12:249–56. https://doi.org/10.1016/j.jamda.2011.01.003 [PubMed]
- 6. Carey EJ, Lai JC, Sonnenday C, Tapper EB, Tandon P, Duarte-Rojo A, Dunn MA, Tsien C, Kallwitz ER, Ng V, Dasarathy S, Kappus M, Bashir MR, Montano-Loza AJ. A North American Expert Opinion Statement on Sarcopenia in Liver Transplantation. Hepatology. 2019; 70:1816–29. https://doi.org/10.1002/hep.30828 [PubMed]
- 7. Chien TP, Huang SF, Chan WH, Pan KT, Yu MC, Lee WC, Tsai HI, Lin PT, Chen HY, Chen JH, Lee CW. The combination of sarcopenia and biochemical factors can predict the survival of hepatocellular carcinoma patients receiving transarterial chemoembolization. Front Oncol. 2022; 12:1005571. https://doi.org/10.3389/fonc.2022.1005571 [PubMed]
- 8. Yang S, Zhang Z, Su T, Yu J, Cao S, Wang H, Jin L. CT-based skeletal muscle loss for predicting poor survival in patients with hepatocellular carcinoma experiencing curative hepatectomy plus adjuvant transarterial chemoembolization: a preliminary retrospective study. Eur J Med Res. 2022; 27:131. https://doi.org/10.1186/s40001-022-00760-6 [PubMed]
- 9. Li Q, Zhang L, Hou ZH, Zhao DX, Li JB, Zhang S, Yin Y, Ni CF, Chen T. High Visceral Adipose Tissue Density Correlates With Unfavorable Outcomes in Patients With Intermediate-Stage Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. Front Cell Dev Biol. 2021; 9:710104. https://doi.org/10.3389/fcell.2021.710104 [PubMed]
- 10. Roth G, Teyssier Y, Benhamou M, Abousalihac M, Caruso S, Sengel C, Seror O, Ghelfi J, Seigneurin A, Ganne-Carrie N, Gigante E, Blaise L, Sutter O, et al. Impact of sarcopenia on tumor response and survival outcomes in patients with hepatocellular carcinoma treated by trans-arterial (chemo)-embolization. World J Gastroenterol. 2022; 28:5324–37. https://doi.org/10.3748/wjg.v28.i36.5324 [PubMed]
- 11. Zhang JX, Yan HT, Ding Y, Liu J, Liu S, Zu QQ, Shi HB. Low Psoas-Muscle index is associated with decreased survival in hepatocellular carcinoma treated with transarterial chemoembolization. Ann Med. 2022; 54:1562–9. https://doi.org/10.1080/07853890.2022.2081872 [PubMed]
- 12. Wang S, Zhang X, Chen Q, Jin ZC, Lu J, Guo J. A Novel Neutrophil-to-Lymphocyte Ratio and Sarcopenia Based TACE-Predict Model of Hepatocellular Carcinoma Patients. J Hepatocell Carcinoma. 2023; 10:659–71. https://doi.org/10.2147/JHC.S407646 [PubMed]
- 13. Lanza E, Masetti C, Messana G, Muglia R, Pugliese N, Ceriani R, Lleo de Nalda A, Rimassa L, Torzilli G, Poretti D, D'Antuono F, Politi LS, Pedicini V, Aghemo A, and Humanitas HCC Multidisciplinary Group. Sarcopenia as a predictor of survival in patients undergoing bland transarterial embolization for unresectable hepatocellular carcinoma. PLoS One. 2020; 15:e0232371. https://doi.org/10.1371/journal.pone.0232371 [PubMed]
- 14. Loosen SH, Jördens MS, Schoon B, Antoch G, Luedde T, Minko P, Loberg C, Roderburg C. Sarcopenia indicate poor survival in patients undergoing transarterial chemoembolization (TACE) for hepatic malignancies. J Cancer Res Clin Oncol. 2023; 149:6181–90. https://doi.org/10.1007/s00432-022-04519-8 [PubMed]
- 15. Loosen SH, Schulze-Hagen M, Bruners P, Tacke F, Trautwein C, Kuhl C, Luedde T, Roderburg C. Sarcopenia Is a Negative Prognostic Factor in Patients Undergoing Transarterial Chemoembolization (TACE) for Hepatic Malignancies. Cancers (Basel). 2019; 11:1503. https://doi.org/10.3390/cancers11101503 [PubMed]
- 16. Fujita M, Takahashi A, Hayashi M, Okai K, Abe K, Ohira H. Skeletal muscle volume loss during transarterial chemoembolization predicts poor prognosis in patients with hepatocellular carcinoma. Hepatol Res. 2019; 49:778–86. https://doi.org/10.1111/hepr.13331 [PubMed]
- 17. Bannangkoon K, Hongsakul K, Tubtawee T, Ina N, Chichareon P. Association of myosteatosis with treatment response and survival in patients with hepatocellular carcinoma undergoing chemoembolization: a retrospective cohort study. Sci Rep. 2023; 13:3978. https://doi.org/10.1038/s41598-023-31184-9 [PubMed]
- 18. Masetti C, Pugliese N, Lofino L, Colapietro F, Ceriani R, Lleo A, Poretti D, Pedicini V, De Nicola S, Torzilli G, Rimassa L, Aghemo A, Lanza E. Myosteatosis Is Not Associated with Complications or Survival in HCC Patients Undergoing Trans Arterial Embolization. J Clin Med. 2022; 12:262. https://doi.org/10.3390/jcm12010262 [PubMed]
- 19. Zhang L, Kuang T, Chai D, Deng W, Wang P, Wang W. The Use of Antibiotics During Immune Checkpoint Inhibitor Treatment Is Associated with Lower Survival in Advanced Esophagogastric Cancer. Int Immunopharmacol. 2023; 119:110200. https://doi.org/10.1016/j.intimp.2023.110200 [PubMed]
- 20. Zhang L, Ma W, Qiu Z, Kuang T, Wang K, Hu B, Wang W. Prognostic nutritional index as a prognostic biomarker for gastrointestinal cancer patients treated with immune checkpoint inhibitors. Front Immunol. 2023; 14:1219929. https://doi.org/10.3389/fimmu.2023.1219929 [PubMed]
- 21. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34. https://doi.org/10.1136/bmj.315.7109.629 [PubMed]
- 22. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994; 50:1088–101. [PubMed]
- 23. Zhang L, Jin Q, Chai D, Kuang T, Li C, Guan Y, Liu L, Wang W, Deng W. The correlation between probiotic use and outcomes of cancer patients treated with immune checkpoint inhibitors. Front Pharmacol. 2022; 13:937874. https://doi.org/10.3389/fphar.2022.937874 [PubMed]
- 24. Rangel EL, Rios-Diaz AJ, Uyeda JW, Castillo-Angeles M, Cooper Z, Olufajo OA, Salim A, Sodickson AD. Sarcopenia increases risk of long-term mortality in elderly patients undergoing emergency abdominal surgery. J Trauma Acute Care Surg. 2017; 83:1179–86. https://doi.org/10.1097/TA.0000000000001657 [PubMed]
- 25. Marasco G, Serenari M, Renzulli M, Alemanni LV, Rossini B, Pettinari I, Dajti E, Ravaioli F, Golfieri R, Cescon M, Festi D, Colecchia A. Clinical impact of sarcopenia assessment in patients with hepatocellular carcinoma undergoing treatments. J Gastroenterol. 2020; 55:927–43. https://doi.org/10.1007/s00535-020-01711-w [PubMed]
- 26. Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, Lencioni R, Koike K, Zucman-Rossi J, Finn RS. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021; 7:6. https://doi.org/10.1038/s41572-020-00240-3 [PubMed]
- 27. Shao YY, Wang SY, Lin SM, and Diagnosis Group, and Systemic Therapy Group. Management consensus guideline for hepatocellular carcinoma: 2020 update on surveillance, diagnosis, and systemic treatment by the Taiwan Liver Cancer Association and the Gastroenterological Society of Taiwan. J Formos Med Assoc. 2021; 120:1051–60. https://doi.org/10.1016/j.jfma.2020.10.031 [PubMed]
- 28. Phu S, Boersma D, Duque G. Exercise and Sarcopenia. J Clin Densitom. 2015; 18:488–92. https://doi.org/10.1016/j.jocd.2015.04.011 [PubMed]
- 29. Dolan E, Artioli GG, Pereira RMR, Gualano B. Muscular Atrophy and Sarcopenia in the Elderly: Is There a Role for Creatine Supplementation? Biomolecules. 2019; 9:642. https://doi.org/10.3390/biom9110642 [PubMed]
- 30. Beer L, Bastati N, Ba-Ssalamah A, Pötter-Lang S, Lampichler K, Bican Y, Lauber D, Hodge J, Binter T, Pomej K, Simbrunner B, Semmler G, Trauner M, et al. MRI-defined sarcopenia predicts mortality in patients with chronic liver disease. Liver Int. 2020; 40:2797–807. https://doi.org/10.1111/liv.14648 [PubMed]
- 31. Ahn H, Kim DW, Ko Y, Ha J, Shin YB, Lee J, Sung YS, Kim KW. Updated systematic review and meta-analysis on diagnostic issues and the prognostic impact of myosteatosis: A new paradigm beyond sarcopenia. Ageing Res Rev. 2021; 70:101398. https://doi.org/10.1016/j.arr.2021.101398 [PubMed]