



Introduction
Sex is defined by biological differences in the chromosomes, reproductive organs, and sex steroid levels between men and women, while gender is determined by behaviors and activity differences in human society or culture between male and female [1]. In many cancer types, significant sex disparities in cancer incidence, survival, and prevalence and treatment responses have also been reported [2, 3]. Sex disparities in cancer are presumably induced by sex hormones, especially estrogen, which are known to modulate gene expression in many cancers [4, 5]. Genomic mutation, may be key factors for sex-biased disparities in mortality and incidence of cancers [6]. Most prior research on genomic determinants of sex differences have focused on TMB [7]. However, the mutant genes related to sex disparity have yet to be elucidated.
Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment, showing higher efficacy than standard therapies in the management of several difficult-totreat malignancies, including malignant melanoma, non-small-cell lung cancer, bladder cancer, and head and neck cancer, among many others [8]. Recently, sex-based ICI efficacy dimorphism has been found in various cancers, suggesting that male cancer patients benefit from ICIs more than female cancer patients [9, 10]. However, only a subset of patients respond well to ICIs. Recent studies suggested that TMB was an efficient pan-cancer biomarker for ICI response and was preferentially useful in female patients [11]. However, due to the non-uniform calculation, various sequencing approaches and exorbitant expenses, TMB is not an optimal indicator to ICIs responses in some types of cancer. Therefore, new biomarkers are desperately needed to identify the group of patients who may be more likely to benefit from ICIs.
Telomerase reverse transcriptase (TERT) mutations lead to aberrantly upregulate TERT expression, and ultimately enable telomere maintenance, which achieve unlimited proliferative capacity of tumor cells [12, 13]. Moreover, TERT mutations are identified as biomarkers of tumor aggressiveness and poor prognosis in several human cancer types [14–17]. Recently, a study on bladder cancer suggested that TERT promoter mutation has been identified as a potential predictive marker of Bacillus Calmette-Guérin (BCG) treatment which was regarded as one of the first and most successful of all oncological immunotherapies [18]. However, a comprehensive analysis of TERT mutation and their predictive value for ICIs has never been elucidated to date.
With the availability of the cBioPortal database, we firstly compared the mutant genes related to sex disparity, and then analyzed the frequency of TERT mutation between different sex groups in different cancer types. Finally, we explored the effect of TERT mutation and sex disparity on the efficacy of immunotherapy in pan cancer, especially melanoma.
Results
The differential mutant genes related to sex disparity
Scatter plots all showed differences in genetic mutations between different sex groups (Figure 1A). The blue dots indicated that the p and q values were statistically significant, and the gray dots were not significant. We also showed the top 10 genes with the greatest difference of mutations in female and male. As shown in Figure 1B, the mutation frequency of PIK3CA, ATRX, CDH1, GATA3, MAP3K1, and ESR1 was higher in the female than in the male group (p <0.05). In TERT, ERG, VHL, and TMPRSS2, the mutation frequency was higher in the male than in the female group, and the difference was also statistically significant (p <0.05).
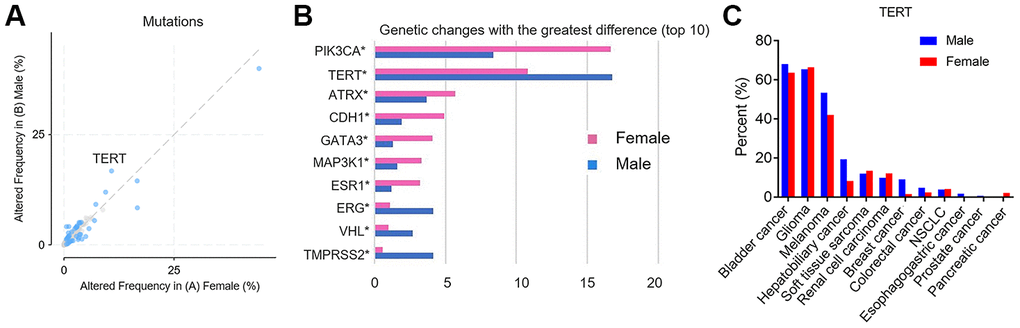
Figure 1. The differential mutant genes between female vs male group. (A) Scatter plots, the altered frequency of genetic mutations between female vs male group (%). The X axis represents altered frequency in female. The Y axis represents altered frequency in male. The blue dots indicate that the p and q values are statistically significant. (B) The top 10 genes with the greatest difference of mutations between female vs male group. The X axis represents genetic changes with the greatest difference. The Y axis represents differential mutant genes. The red histogram indicates female and the blue histogram indicates male. (C) The frequency of TERT mutations between female vs male group in different cancer types. X-axis represents common types of cancer. The Y axis represents percent of TERT mutation. The red histogram indicates female and the blue histogram indicates male.
We further analyzed the frequency of TERT mutations between different sex groups in different cancer types. Figure 1C showed that Bladder Cancer, Glioma and Melanoma were the top three of TERT mutation frequency, while Esophagogastric cancer, Prostate cancer, and Pancreatic cancer were the last three. Notably, for Melanoma and Hepatobiliary cancer, TERT mutation frequency was higher in male patients than female patients.
Relationship between TERT mutation and sex disparity and immunotherapy
We first explored the association between sex and overall survival (OS) in the immunotherapy cohort. As shown in Figure 2A, male patients had significantly better median OS than female patients (19 months vs 15 months, p =0.047). From the above results, we found that TERT mutation was related to sex disparity. We also explored the predictive value of TERT mutation on the efficacy of immunotherapy. Surprisingly, patients in the TERT altered group showed a significantly longer median OS than unaltered group (Figure 2B, 24 months vs 17 months, p =0.002).
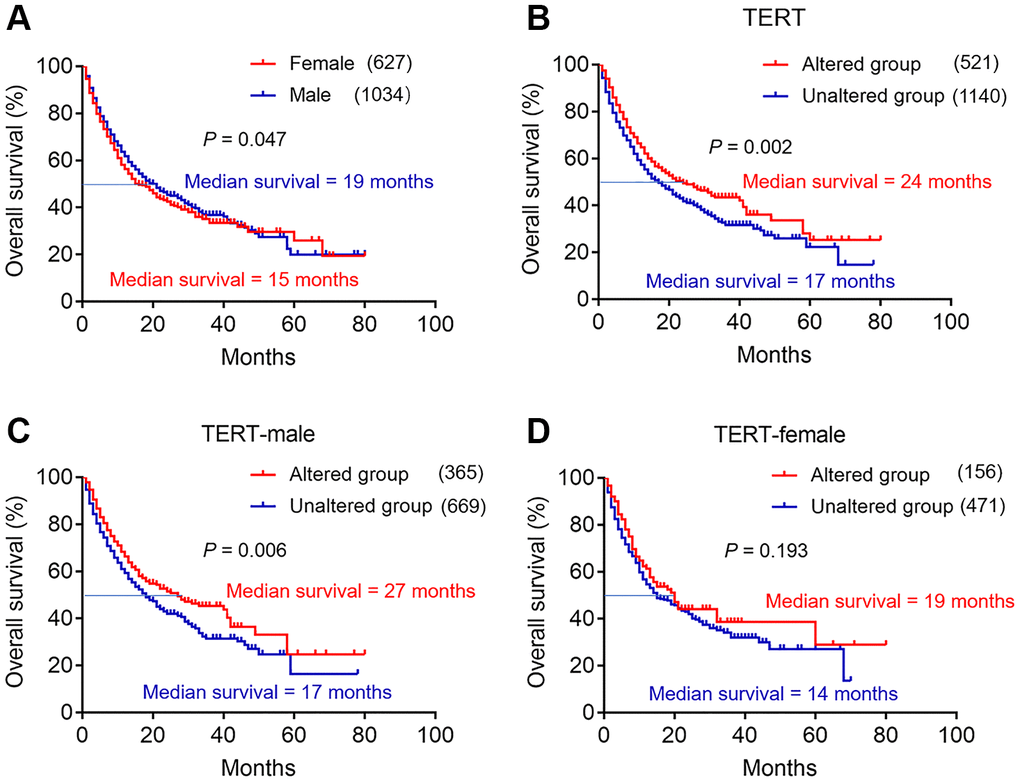
Figure 2. The effect of TERT mutation and sex disparity on the efficacy of immunotherapy in cBioPortal database. (A) Kaplan-Meier survival analysis between female and male patients in ICI treatment cohort. The red curve represents female group, and the blue curve represents male group. (B) Kaplan-Meier survival analysis between TERT altered and unaltered group in ICI treatment cohort. The red curve represents TERT altered group, and the blue curve represents unaltered group. (C) Kaplan-Meier survival analysis between TERT altered and unaltered group in the TERT-male cohort. The red curve represents TERT altered group, and the blue curve represents unaltered group. (D) Kaplan-Meier survival analysis between TERT altered and unaltered group in the TERT-female cohort. The red curve represents TERT altered group, and the blue curve represents unaltered group.
In order to further understand whether male and female patients with TERT mutation can benefit from immunotherapy. We next conducted subgroup analysis in the TERT-male and TERT-female cohort. Notably, in TERT-male group, male patients in the TERT altered group had longer median OS than unaltered group (Figure 2C, 27 months vs 17 months, p =0.006). Similar results were obtained in TERT-female cohort, female patients in the TERT altered group had longer median OS trend than unaltered group, but not statistically significant (Figure 2D, 19 months vs 14 months, p =0.193).
Relationship between TERT mutation and immunotherapy in different sex groups of melanoma
To explore the predictive value of TERT mutation on the efficacy of immunotherapy in certain cancer types. The cancer types including non-small cell lung cancer, melanoma, bladder cancer, renal cell carcinoma, head and neck cancer, esophagogastric cancer, glioma and colorectal cancer were further analyzed. However, the result showed that only male melanoma patients in the TERT altered group had longer median OS than unaltered group (Figure 3A, 49 months vs 27 months, p<0.001). Similar to pan cancer analysis, the statistically OS significant was not found for female melanoma patients in the TERT altered group (Figure 3B, 60 months vs 44 months, p =0.511). Other tumor types did not get a positive result, and the data were not given.
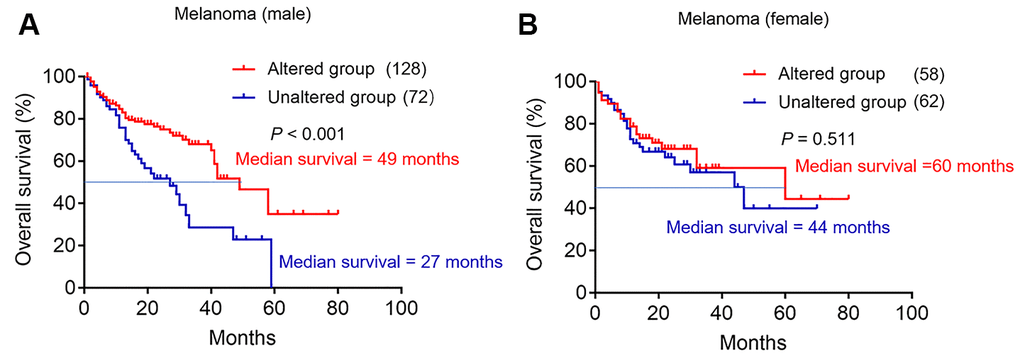
Figure 3. The effect of TERT mutation on the efficacy of immunotherapy in melanoma database. (A) Kaplan-Meier survival analysis between TERT altered and unaltered group in the male cohort. The red curve represents TERT altered group, and the blue curve represents unaltered group. (B) Kaplan-Meier survival analysis between TERT altered and unaltered group in the female cohort. The red curve represents TERT altered group, and the blue curve represents unaltered group.
Discussion
Sex disparities were biologically related to cancer diagnosis, prognosis, severity, and prediction of treatment response [2, 3]. Genomics studies showed a variation in the expression of autosomal genes between males and females [19, 20]. TMB, as a biomarker of response to ICIs, has been considered to be more predictive of the efficacy of immunotherapy in female patients [11]. However, due to the limitations of TMB application, we needed to explored new biomarkers related to sex disparity to better predict ICIs response.
In our study, we showed the top 10 genes with the greatest difference of mutations, which were related to sex disparity. This variation (genetic mutation) may help facilitate the identification of sex-specific cancer biomarkers. We found that PIK3CA and TERT were genes with the greatest differences between different sex groups. Strikingly, TERT mutation could be frequent in many malignancies and be identified as biomarkers of tumor aggressiveness and poor prognosis in several human cancer types [14–17]. We further analyzed the frequency of TERT mutations between different sex groups in different cancer types. The result showed that Bladder Cancer, Glioma and Melanoma were the top three of TERT mutation frequency, while Esophagogastric cancer, Prostate cancer, and Pancreatic cancer were the last three. Consistent results have also been confirmed the high prevalence of TERT mutation in bladder cancer, Glioma and Melanoma and a lower mutation frequency of breast cancer and prostate cancer, although they occurred with different frequencies [21–25]. Moreover, we also found that TERT mutation frequency of Melanoma and Hepatobiliary cancer was higher in male patients than female patients. Lee et al analyzed TERT promoter mutation in 162 tumor samples of the patients with HCC by sequencing and real-time PCR, respectively. The result showed that the TERT promoter mutation rate was 28.8% (46/160) in HCC and was associated with males (p =0.027) [26]. Egberts et al also found highly recurrent TERT promoter mutations in malignant melanomas, and the prevalence of its TERT-promoter mutations was associated with the patient's sex [23 (51.1%) men, 10 (21.3%) women; p = 0.004] [27]. The above results suggested that TERT mutation might be closely related to sex, although efforts are still needed to evaluate the clinical utility of sex-biased TERT mutation in a larger patient cohort.
But for patients who received ICIs, what was the relationship between TERT mutation and OS? We evaluated the effect of TERT mutation and sex disparity on the efficacy of immunotherapy. Our results demonstrated that male patients and patients with TERT mutation all had significantly better median OS. More importantly, male patients with TERT mutation had longer median OS. Current study has revealed that sex-based dimorphism on the efficacy of ICIs in various cancers and confirmed that male patients can benefit more from immunotherapy [8, 28, 29]. As we all know, not all male patients can benefit from immunotherapy, and new biomarkers are still needed to predict the efficacy of immunotherapy. Our study reported that male patients with TERT mutation may be more likely to benefit from immunotherapy in a multitude of cancers.
Our study has not only found a high frequency of TERT mutations in melanoma, but also a higher frequency of mutations in male melanoma patients. In addition, effect of sex on immunotherapy may exist in specific cancer types rather than all cancer types [30, 31]. TERT mutation should also be like this. Our result showed that only male melanoma patients with TERT mutation had longer median OS. Therefore, male melanoma patients with TERT mutation may benefit from immunotherapy.
This study also has certain limitations. Firstly, our study was only a bioinformatic based on public databases. The next step is to confirm whether male patients with TERT mutation could benefit from immunotherapy through prospective or retrospective studies. Secondly, the immunotherapy data we collected for each cancer type was very limited. Although we did immunotherapy analyses in certain cancer types, the same conclusion was only obtained in melanoma. As for other tumor types, we need to determine whether male patients with TERT mutations benefit from immunotherapy.
In conclusion, using the cBioPortal database, we identified that TERT mutation may serve as a sex-specific cancer biomarker and TERT mutation frequency of melanoma was higher in male patients. Notably, we found that male patients with TERT mutation may be more likely to benefit from immunotherapy, especially for melanoma. However, the potential role of TERT mutation as biomarkers for immunotherapy are still needed to confirm by further clinical trials.
Materials and Methods
All data in this study were selected from the cBioPortal database (https://www.cbioportal.org) [32]. To analyze the differences of gene mutation according to sex disparity, we used the MSK-IMPACT Clinical Sequencing Cohort [33], which contain 10336 patients/10945 samples with available mutation and sex status information.
For the relationship analysis between gender, TERT mutation and immunotherapy, we also selected TMB and Immunotherapy Cohort [34], which contains 1661 patients with various cancer types (including 320 cases of melanoma) with available survival, immunotherapy, TERT mutation and sex status information. Data between two groups were compared using unpaired t-test or Wilcoxon rank-sum test. Kaplan-Meier method was used to calculate the survival probability and log-rank test was used to compare the survival curves. All reported p values are two-tailed, and for all analyses, p <0.05 is considered statistically significant. This study was mainly based on the cBioPortal database and personal privacy information was not involved, so the informed consent was not needed.
Author Contributions
Haiyong Wang designed the project and proposed the idea; Jia Li and Zhaoyan Li carried out data download and literature collection and wrote manuscript; Chenyue Zhang conducted bioinformatics analysis; Chenxing Zhang conducted chart and statistical processing. All authors read and approved the final manuscript.
Conflicts of Interest
All authors declare that there is no conflicts of interest.
Funding
This study was supported jointly by Special funds for Taishan Scholars Project (Grant no. tsqn201812149), Academic promotion programme of Shandong First Medical University (2019RC004).
References
- 1. Clayton JA, Tannenbaum C. Sex and gender reporting in research-reply. JAMA. 2017; 317:975. https://doi.org/10.1001/jama.2017.0151 [PubMed]
- 2. Zhu Y, Shao X, Wang X, Liu L, Liang H. Sex disparities in cancer. Cancer Lett. 2019; 466:35–38. https://doi.org/10.1016/j.canlet.2019.08.017 [PubMed]
- 3. Cook MB, McGlynn KA, Devesa SS, Freedman ND, Anderson WF. Sex disparities in cancer mortality and survival. Cancer Epidemiol Biomarkers Prev. 2011; 20:1629–37. https://doi.org/10.1158/1055-9965.EPI-11-0246 [PubMed]
- 4. Özdemir BC, Dotto GP. Sex hormones and anticancer immunity. Clin Cancer Res. 2019; 25:4603–10. https://doi.org/10.1158/1078-0432.CCR-19-0137 [PubMed]
- 5. Kim HI, Lim H, Moon A. Sex differences in cancer: epidemiology, genetics and therapy. Biomol Ther (Seoul). 2018; 26:335–42. https://doi.org/10.4062/biomolther.2018.103 [PubMed]
- 6. Mostertz W, Stevenson M, Acharya C, Chan I, Walters K, Lamlertthon W, Barry W, Crawford J, Nevins J, Potti A. Age- and sex-specific genomic profiles in non-small cell lung cancer. JAMA. 2010; 303:535–43. https://doi.org/10.1001/jama.2010.80 [PubMed]
- 7. Gupta S, Artomov M, Goggins W, Daly M, Tsao H. Gender disparity and mutation burden in metastatic melanoma. J Natl Cancer Inst. 2015; 107:djv221. https://doi.org/10.1093/jnci/djv221 [PubMed]
- 8. Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018; 359:1350–55. https://doi.org/10.1126/science.aar4060 [PubMed]
- 9. Conforti F, Pala L, Bagnardi V, De Pas T, Martinetti M, Viale G, Gelber RD, Goldhirsch A. Cancer immunotherapy efficacy and patients’ sex: a systematic review and meta-analysis. Lancet Oncol. 2018; 19:737–46. https://doi.org/10.1016/S1470-2045(18)30261-4 [PubMed]
- 10. Wang PF, Song HF, Zhang Q, Yan CX. Pan-cancer immunogenomic analyses reveal sex disparity in the efficacy of cancer immunotherapy. Eur J Cancer. 2020; 126:136–38. https://doi.org/10.1016/j.ejca.2019.12.008 [PubMed]
- 11. Wang S, Zhang J, He Z, Wu K, Liu XS. The predictive power of tumor mutational burden in lung cancer immunotherapy response is influenced by patients’ sex. Int J Cancer. 2019; 145:2840–49. https://doi.org/10.1002/ijc.32327 [PubMed]
- 12. Weinrich SL, Pruzan R, Ma L, Ouellette M, Tesmer VM, Holt SE, Bodnar AG, Lichtsteiner S, Kim NW, Trager JB, Taylor RD, Carlos R, Andrews WH, et al. Reconstitution of human telomerase with the template RNA component hTR and the catalytic protein subunit hTRT. Nat Genet. 1997; 17:498–502. https://doi.org/10.1038/ng1297-498 [PubMed]
- 13. Lorbeer FK, Hockemeyer D. TERT promoter mutations and telomeres during tumorigenesis. Curr Opin Genet Dev. 2020; 60:56–62. https://doi.org/10.1016/j.gde.2020.02.001 [PubMed]
- 14. Osella-Abate S, Bertero L, Senetta R, Mariani S, Lisa F, Coppola V, Metovic J, Pasini B, Puig SS, Fierro MT, Manrique-Silva E, Kumar R, Nagore E, et al. TERT promoter mutations are associated with visceral spreading in melanoma of the trunk. Cancers (Basel). 2019; 11:452. https://doi.org/10.3390/cancers11040452 [PubMed]
- 15. Simon M, Hosen I, Gousias K, Rachakonda S, Heidenreich B, Gessi M, Schramm J, Hemminki K, Waha A, Kumar R. TERT promoter mutations: a novel independent prognostic factor in primary glioblastomas. Neuro Oncol. 2015; 17:45–52. https://doi.org/10.1093/neuonc/nou158 [PubMed]
- 16. Melo M, da Rocha AG, Vinagre J, Batista R, Peixoto J, Tavares C, Celestino R, Almeida A, Salgado C, Eloy C, Castro P, Prazeres H, Lima J, et al. TERT promoter mutations are a major indicator of poor outcome in differentiated thyroid carcinomas. J Clin Endocrinol Metab. 2014; 99:E754–65. https://doi.org/10.1210/jc.2013-3734 [PubMed]
- 17. Leão R, Lee D, Figueiredo A, Hermanns T, Wild P, Komosa M, Lau I, Mistry M, Nunes NM, Price AJ, Zhang C, Lipman T, Poyet C, et al. Combined genetic and epigenetic alterations of the TERT promoter affect clinical and biological behavior of bladder cancer. Int J Cancer. 2019; 144:1676–84. https://doi.org/10.1002/ijc.31935 [PubMed]
- 18. Batista R, Lima L, Vinagre J, Pinto V, Lyra J, Máximo V, Santos L, Soares P. TERT promoter mutation as a potential predictive biomarker in BCG-treated bladder cancer patients. Int J Mol Sci. 2020; 21:947. https://doi.org/10.3390/ijms21030947 [PubMed]
- 19. Shin JY, Jung HJ, Moon A. Molecular markers in sex differences in cancer. Toxicol Res. 2019; 35:331–41. https://doi.org/10.5487/TR.2019.35.4.331 [PubMed]
- 20. van Nas A, Guhathakurta D, Wang SS, Yehya N, Horvath S, Zhang B, Ingram-Drake L, Chaudhuri G, Schadt EE, Drake TA, Arnold AP, Lusis AJ. Elucidating the role of gonadal hormones in sexually dimorphic gene coexpression networks. Endocrinology. 2009; 150:1235–49. https://doi.org/10.1210/en.2008-0563 [PubMed]
- 21. Vinagre J, Almeida A, Pópulo H, Batista R, Lyra J, Pinto V, Coelho R, Celestino R, Prazeres H, Lima L, Melo M, da Rocha AG, Preto A, et al. Frequency of TERT promoter mutations in human cancers. Nat Commun. 2013; 4:2185. https://doi.org/10.1038/ncomms3185 [PubMed]
- 22. Liu X, Wu G, Shan Y, Hartmann C, von Deimling A, Xing M. Highly prevalent TERT promoter mutations in bladder cancer and glioblastoma. Cell Cycle. 2013; 12:1637–38. https://doi.org/10.4161/cc.24662 [PubMed]
- 23. Rachakonda PS, Hosen I, de Verdier PJ, Fallah M, Heidenreich B, Ryk C, Wiklund NP, Steineck G, Schadendorf D, Hemminki K, Kumar R. TERT promoter mutations in bladder cancer affect patient survival and disease recurrence through modification by a common polymorphism. Proc Natl Acad Sci USA. 2013; 110:17426–31. https://doi.org/10.1073/pnas.1310522110 [PubMed]
- 24. Killela PJ, Reitman ZJ, Jiao Y, Bettegowda C, Agrawal N, Diaz LA
Jr , Friedman AH, Friedman H, Gallia GL, Giovanella BC, Grollman AP, He TC, He Y, et al. TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc Natl Acad Sci USA. 2013; 110:6021–26. https://doi.org/10.1073/pnas.1303607110 [PubMed] - 25. Bell RJ, Rube HT, Xavier-Magalhães A, Costa BM, Mancini A, Song JS, Costello JF. Understanding TERT promoter mutations: a common path to immortality. Mol Cancer Res. 2016; 14:315–23. https://doi.org/10.1158/1541-7786.MCR-16-0003 [PubMed]
- 26. Lee HW, Park TI, Jang SY, Park SY, Park WJ, Jung SJ, Lee JH. Clinicopathological characteristics of TERT promoter mutation and telomere length in hepatocellular carcinoma. Medicine (Baltimore). 2017; 96:e5766. https://doi.org/10.1097/MD.0000000000005766 [PubMed]
- 27. Egberts F, Krüger S, Behrens HM, Bergner I, Papaspyrou G, Werner JA, Alkatout I, Haag J, Hauschild A, Röcken C. Melanomas of unknown primary frequently harbor TERT-promoter mutations. Melanoma Res. 2014; 24:131–36. https://doi.org/10.1097/CMR.0000000000000048 [PubMed]
- 28. Conforti F, Pala L, Bagnardi V, Viale G, De Pas T, Pagan E, Pennacchioli E, Cocorocchio E, Ferrucci PF, De Marinis F, Gelber RD, Goldhirsch A. Sex-based heterogeneity in response to lung cancer immunotherapy: a systematic review and meta-analysis. J Natl Cancer Inst. 2019; 111:772–81. https://doi.org/10.1093/jnci/djz094 [PubMed]
- 29. Wang S, Cowley LA, Liu XS. Sex differences in cancer immunotherapy efficacy, biomarkers, and therapeutic strategy. Molecules. 2019; 24:3214. https://doi.org/10.3390/molecules24183214 [PubMed]
- 30. Wu Y, Ju Q, Jia K, Yu J, Shi H, Wu H, Jiang M. Correlation between sex and efficacy of immune checkpoint inhibitors (PD-1 and CTLA-4 inhibitors). Int J Cancer. 2018; 143:45–51. https://doi.org/10.1002/ijc.31301 [PubMed]
- 31. Grassadonia A, Sperduti I, Vici P, Iezzi L, Brocco D, Gamucci T, Pizzuti L, Maugeri-Saccà M, Marchetti P, Cognetti G, De Tursi M, Natoli C, Barba M, Tinari N. Effect of gender on the outcome of patients receiving immune checkpoint inhibitors for advanced cancer: a systematic review and meta-analysis of phase III randomized clinical trials. J Clin Med. 2018; 7:542. https://doi.org/10.3390/jcm7120542 [PubMed]
- 32. Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, Sun Y, Jacobsen A, Sinha R, Larsson E, Cerami E, Sander C, Schultz N. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci Signal. 2013; 6:pl1. https://doi.org/10.1126/scisignal.2004088 [PubMed]
- 33. Zehir A, Benayed R, Shah RH, Syed A, Middha S, Kim HR, Srinivasan P, Gao J, Chakravarty D, Devlin SM, Hellmann MD, Barron DA, Schram AM, et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat Med. 2017; 23:703–13. https://doi.org/10.1038/nm.4333 [PubMed]
- 34. Samstein RM, Lee CH, Shoushtari AN, Hellmann MD, Shen R, Janjigian YY, Barron DA, Zehir A, Jordan EJ, Omuro A, Kaley TJ, Kendall SM, Motzer RJ, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet. 2019; 51:202–06. https://doi.org/10.1038/s41588-018-0312-8 [PubMed]