



Introduction
Ischemic stroke, defined as a clinical syndrome of sudden central nervous system dysfunction, seriously threatens human life and imposes a great mental and economic burden on society, families, and individuals [1]. With the increase in the population of older adults in China, stroke-induced disability continues to increase and is the leading cause of death; therefore, developing new stroke treatment methods, including neuroprotective strategies [2]. Although more than 700 drugs have been described for experimental stroke, only tissue-type plasminogen activators have been shown to be effective in human studies [3, 4]. These disadvantages include the risk of bleeding, short effective time window, and unsuitability for many patients [5]. Therefore, it is necessary to investigate other drugs for treating ischemic stroke.
The Na-K-2Cl cotransporter, NKCC1, initially thought to be a small transmembrane protein, is expressed in both immature and diseased central neurons [6–8]. Immunostaining and RNA data indicate that NKCC1 is highly expressed in developing and mature oligodendrocytes (OLs) of the adult mouse brain and is readily detectable in microglia, astrocytes, developing pericytes, and dentate gyrus (DG) progenitor cells [9]. In the hippocampus of adult mice, NKCC1 activity in OLs mediates changes in axonal conduction, which, in turn, modifies synaptic plasticity [10]. It also plays an important role in maintaining electrical neutrality, normal cell volume, and fluid balance in the brain tissues. Moreover, ischemia-induced NKCC1 stimulation plays an important role in stroke pathophysiology, leading to Na+ overload and apoptotic cell death [11]. The diuretic drug bumetanide is a selective inhibitor of NKCC1 that specifically blocks NKCC1 in the brain. Animal experiments have revealed that bumetanide administration can reduce the severity of neuronal and oligodendrocyte damage and create a favorable environment for neurogenesis and axon growth [12–15]. Other studies have shown that bumetanide can reduce cerebral edema and nerve cell injury in rats with focal ischemia-reperfusion injury [16–18]. Several clinical studies have been conducted to evaluate the efficacy of bumetanide for spectrum disorder (ASD), Parkinson’s disease (PD), and neonatal seizures [19–21]. Unfortunately, the results were negative. Moreover, although several studies have suggested that bumetanide may be beneficial in rodents of ischemic stroke, no large clinical trials have explored the effects of bumetanide on stroke, nor have there been systematic reviews and meta-analyses of preclinical stroke literature [22–25]. A systematic review of the effects of bumetanide treatment on ischemic models in an objective and quantitative manner may provide credible and reliable evidence for the use of bumetanide in the clinical treatment of stroke. We systematically assessed the bias in the included studies and summarized the optimal pattern of bumetanide therapy. This meta-analysis may provide significant information for patients with cerebrovascular diseases and reduce disability rates. Our study aimed to systematically determine the efficacy of bumetanide in reducing infarct volume, cerebral edema, and neurological function in rodent models of ischemic stroke and to observe the neuroprotective effects of bumetanide in stroke model and duration subgroups.
Materials and Methods
Search strategy
We selected relevant studies from publications in PubMed, Embase, and Web of Science from their inception to February 2024. The search terms used were (stroke OR cerebrovascular OR cerebral infarct OR ischemia OR middle cerebral artery OR middle cerebral artery occlusion) AND (rodent OR mouse OR rat) AND (bumetanide OR NKCC1). The language of the publications was limited to English. Two investigators (Jiadi Hou and Haichun Xu) independently retrieved the literature. Disputes that arose during the selection process were discussed and resolved by both parties.
Inclusion and exclusion criteria and data extraction
The studies included in this meta-analysis and review met the following criteria:
(1) Permanent or transient middle cerebral artery occlusion (pMCAO or tMCAO), ET-1 stroke model, or other focal stroke models were performed on rodents; (2) a control group was set up with a placebo; (3) adequate data on functional outcomes were provided; and (4) experimental studies were presented in the original research articles. The exclusion criteria were as follows: (1) animals treated with bumetanide analogs; (2) neonatal rodents and those using non-rodent models, ex vivo and in vitro preparations, or humans; (3) hemorrhagic stroke models; (4) not reporting the number of animals in groups; (5) review, editorial, conference abstract, and non-English publications; and (6) repeated publications or duplicate reports and abstracts without full text.
The following details were extracted from each study: (1) document elements: first author and year of publication; (2) experimental animal elements: animal species; (3) MCAO model elements: stroke model and ischemia duration; (4) intervention elements: administration route, dosage, and intervention time point; and (5) experimental outcomes. Studies had to provide data on at least one of the following outcome measures: (1) cerebral infarction volume; (2) brain edema or water content (%); and (3) functional outcomes. The data were presented graphically rather than reported as text and were obtained using a digital ruler software (Universal Desktop Ruler). For each comparison, we extracted the means and standard deviations. All data were independently extracted by two participants, and any discrepancies were resolved by consensus or consultation with a third reviewer (Xiao-Yu Sun).
Quality assessment
Quality assessment of the studies was performed by two independent reviewers (Jiadi Hou and Haichun Xu). Any discrepancies were resolved through consultation with a third reviewer (Xiao-Yu Sun). We evaluated the methodological quality of the included studies by applying a previously published 11-item quality scale [26], modified as follows: (1) Peer review publication. (2) Strength-response relationship; (3) Random assignment study; (4) Blinded treatment administration; (5) Blind evaluation of results; (6) Physiological parameters monitoring; (7) Sample size calculation; (8) ≥2 outcome parameters were evaluated; (9) Avoidance of anesthetics with marked intrinsic neuroprotective properties (ketamine); (10) Comply with animal welfare regulations; and (11) Statement of potential conflict of interest. Thus, the studies were classified into three quality categories (category I, 8–11 items; category II, 4–7 items; and category III, 0–3 items).
Statistical analysis
The results of the included trials were analyzed for each endpoint: infarct volume, cerebral edema, and neurological outcomes, including neurological score, memory, and limb function. All analyses were performed using STATA 15.0 software. The I2 statistic was used for heterogeneity assessment. When heterogeneity was strong and could not be eliminated, a random-effects model was used instead of a fixed-effects model to obtain the overall MD/SMD and 95% CI [12, 27]. A subgroup analysis was conducted to examine the effect of bumetanide according to the stroke model (permanent or temporary) and time point of intervention (pre-treatment or post-treatment). A leave-one-out sensitivity analysis was performed to evaluate the robustness of the results. Publication bias was checked by a funnel plot, and asymmetry was estimated by Egger’s test and the trim and fill method [28]. Funnel plots were generated to assess the publication bias. If the p-value was < 0.01, the significance of all the analyses was accepted.
Results
Characteristics of included studies
Screening was performed in two phases: initial screening based on title and abstract, followed by full-text screening of eligible articles for final inclusion. The initial database search identified 39 eligible studies. After removing the duplicates, 31 unique references were identified. The full texts of the remaining 31 records were retrieved for further assessment. Among them, 18 records were excluded because they were reviews, case reports, editorials, inadequate outcomes, neonatal ischemia, and duplicate publications. Finally, 13 studies were included in the meta-analysis (Figure 1 and Table 1) [13–18, 29–35]. Two studies intervened before stroke induction, ten intervened after ischemia induction, and one intervened before and after ischemia. Infarct size was calculated in more than 180 animals, and neurobehavioral deficits were assessed in more than 200 animals. Meta-analysis was performed based on data from 11 studies, and the effects of stroke model and treatment initiation time on infarct volume were analyzed in subgroups.
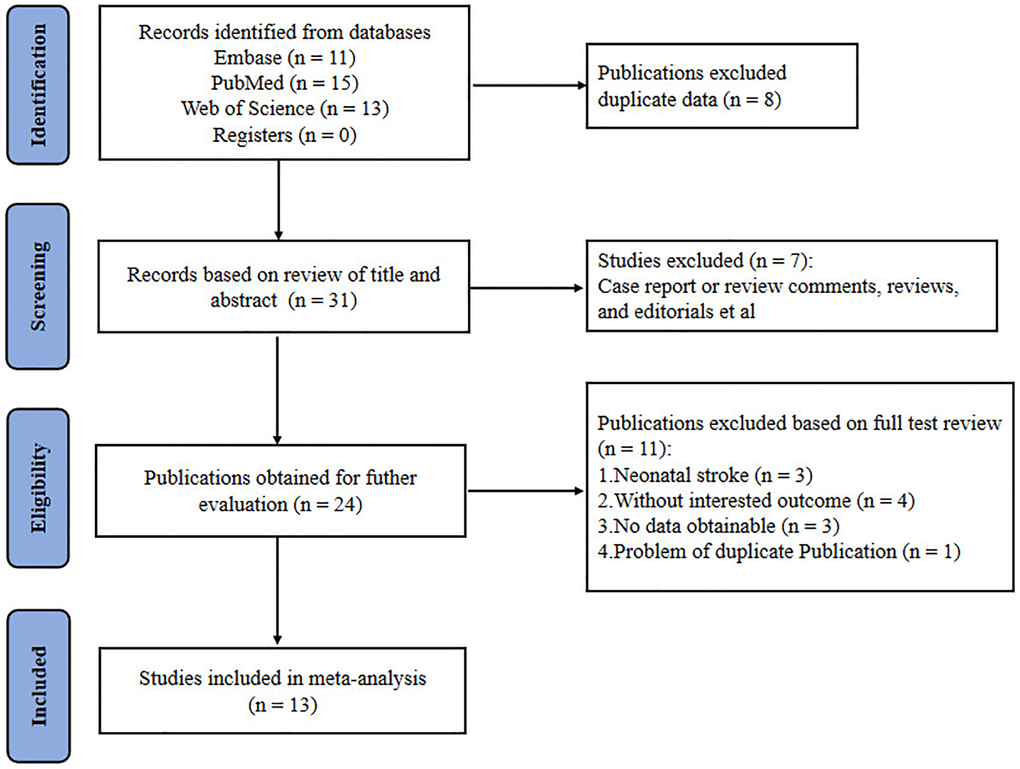
Figure 1. Flow chart for selection of studies.
Table 1. Basic characteristics of the included studies.
| Author | Year | Animal species | Stroke model | Dose range (mg/kg) | Method of administration | Control intervention | Outcome measures | Quality category | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Jun Wang | 2022 | C57Bl/6J mice | tMCAO (60 min) | 10 mg/kg body weight/day | i.p. | DMSO | Infarct volume | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fudong Liu | 2010 | C57BL6 male mice | MCAO (2 hours) | 30.4 mg/kg immediately after MCAO and at reperfusion. | i.v. | Vehicle | Infarct volume Neurological deficits | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Genbao Wang | 2014 | Adult Wistar male rats | MCAO (2 hours) | 30 mg/kg through tail vein 10 min before cerebral ischemia inducing. | i.v. | Saline | Infarct volume brain edema neurological function score | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gulnaz Begum | 2015 | C57Bl/6J male mice | MCAO (60-minutes) | 10 mg/kg was injected intraperitoneally at 3, 24 and 48 h Rp, at 3 h reperfusion, and then daily (every 24 h) at the same dose. | i.p. | NKCC1 KO mice | Infarct volume neurological function deficit scoring analysis brain edema | I | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hai Chen | 2005 | Adult male rats | MCAO (2 hours) | 5 to10 mmol/L bumetanide after MCAO | i.p. | NKCC1−/− mice | Infarct volume brain edema | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Huachen Huang | 2019 | C57BL/6J mice | t-MCAO for 50 min | 10 mg/kg body weight per day was given at 3 hours and the second half dose at 8 hours post-MCAO and twice daily for 1 to 5 days. | i.p. | DMSO | Infarct volume Neurological score | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Martha E. O’Donnell | 2004 | Sprague-Dawley rats | MCAO | 7.6–30.4 mg/kg in one to four doses of 7.6 mg/kg 20 minutes before initiation of MCAO. | i.v. | Vehicle | Infarct volume brain edema | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mohammad Iqbal H Bhuiyan | 2017 | Adult male Wistar rats | MCAO (2 hours) | The initial dose of 5 mg/kg at 3 h and the second dose of 5 mg/kg at 8-h post-reperfusion were followed by two daily injections | i.p. | Saline | Infarct volume latency times in the turn-alley test Neurological deficit scores | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mu XP | 2017 | Adult male Wistar rats | ET-1 stroke model | 0.2 mg/kg/day for 3 weeks on postoperative day 7 | micro-injection pump | Saline | Infarct volume Tapered/ledged beam walking test Cylinder test | I | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wang-shu Xu | 2016 | Adult male Wistar rats | ET-1 stroke model | 25 μg/μL of bumetanide was pumped every day, for 21 consecutive days on postoperative day 7 | micro-injection pump | Saline | Infarct volume Morris water maze test | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wangshu Xu (Mol Neurobiol) | 2017 | Adult male Wistar rats | ET-1 Stroke Model | 0.2 mg/kg/day at 7 days after ischemia | mini-osmotic pumps | Saline | Infarct Volume Beam-Walking Test | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yiping Yan | 2003 | Male rats | MCAO (2 hours) | 100 mM bumetanide mi-crodialyzed from 1 h prior to ischemia to 2-h MCA occlusion (pre-ischemic treatment), or during 24-h reperfusion (post-ischemic treatment). | Brain microdialysis procedures | aCSF | Infarct volume brain edema | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yiping Yan | 2001 | Male rats | MCAO (2 hours) | 100 mol/L bumetanide solution was made in aCSF throughout the 2-hour MCA occlusion and 24-hour reperfusion. | Brain microdialysis procedures | aCSF | Infarct volume brain edema | II | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: MCAO: middle cerebral artery occlusion; ET-1: Endothelin-1; t-MCAO: transient middle cerebral artery occlusion; DMSO: Dimethyl sulfoxide; aCSF: artificial cerebral spinal fluid; IV: intravenous; i.p.: intraperitoneal. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Effect of the study quality
The results of the quality evaluation are shown in Figure 1. Overall, the median quality (range scale 0–11) of the 13 included studies was moderate (8; interquartile range, 6–8). None of the studies received a score of 0 or were of high quality (9–11). Eleven studies were randomized. Eight studies (61.5%) reported temperature control during surgery, but only four studies (30.8%) reported concealing treatment from the investigator during outcome assessments. In addition, all studies used a blinded treatment with bumetanide.
Primary outcome assessment: the effect of bumetanide on cerebral infarction volume
The effect of bumetanide upregulation on cerebral infarction volume was assessed in eleven studies (Table 1) [13–16, 18, 29–33, 35]. These studies measured the cerebral infarction volume by histological assessment of excised brain (tetrazolium chloride (TTC), cresyl violet) and were recorded in mm3. Meta-analysis indicated that compared with the effects of a vehicle, bumetanide significantly reduced cerebral infarction volume (SMD for overall effect: −0.42; 95% CI: −0.75 to −0.09; p = 0.000; I2 = 83%; Figure 2). Subgroup analysis showed that bumetanide reduced infarct volume in transient, but not permanent ischemic models (SMD: −1.03; 95% CI: −1.47 to −0.58; p = 0.000; I2 = 83.6% and SMD:0.34, 95% CI: −0.16 to 0.83; p = 0.999; I2 = 0%, p = 0.999 respectively; Figure 2A). Bumetanide administration after ischemia induction significantly reduced the volume of cerebral infarction relative to administration before ischemia (SMD: −0.21; 95% CI: −0.57 to 0.15; p = 0.000; I2 = 84.5% and SMD: −1.59, 95% CI: −2.43 to 0.74; p = 0.109; I2 = 54.9%, respectively; Figure 2B). Sensitivity analyses showed that the overall findings did not substantially reverse after removing any one trial, indicating that the results were reliable.
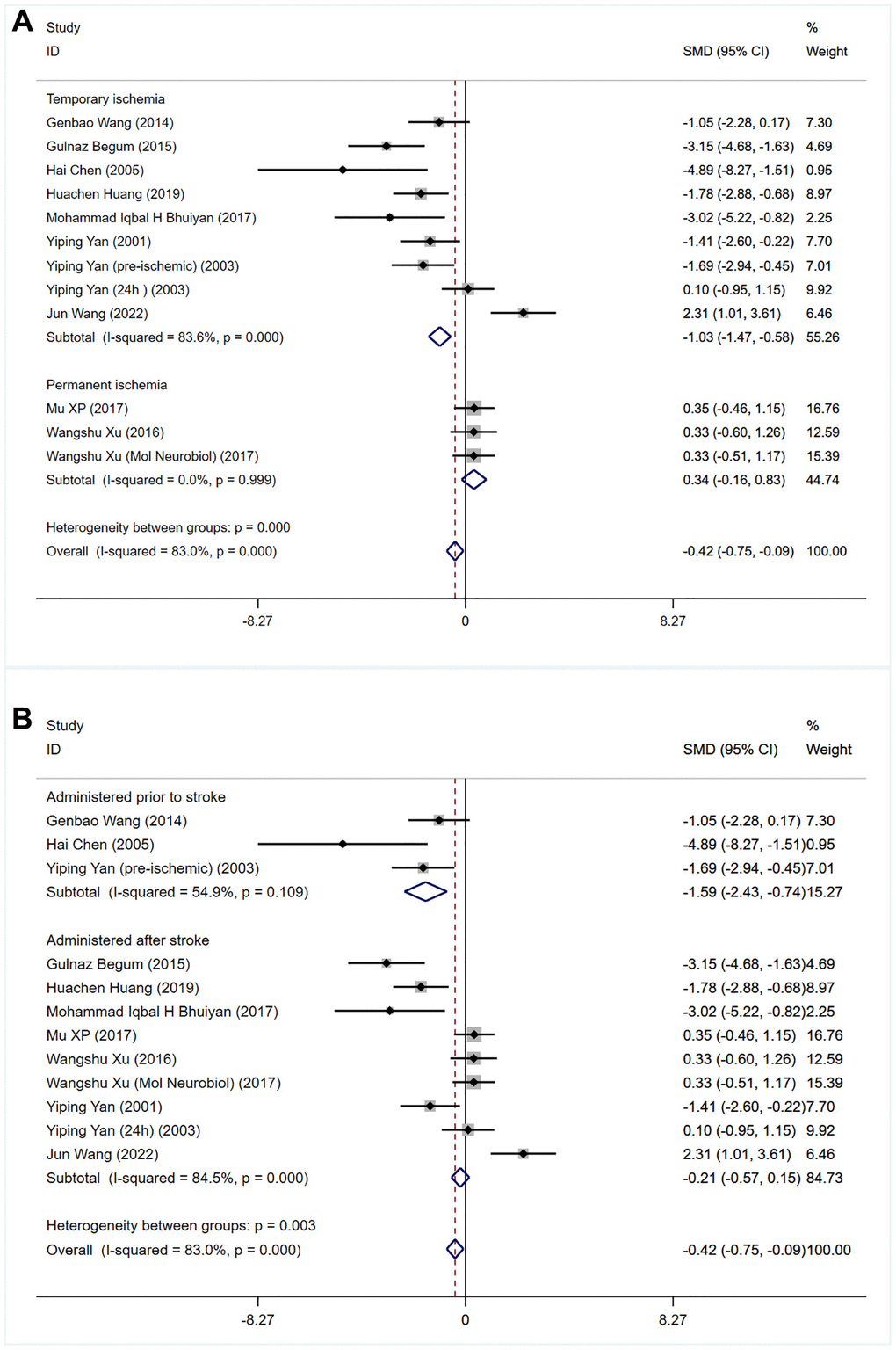
Figure 2. Meta-analysis of infarct volume in rodents treated with bumetanide versus controls was performed, divided by (A) duration of ischemia (permanent vs. transient) and (B) timing of treatment before or after the onset of ischemia.
Secondary outcome assessment: the effect of bumetanide on brain edema
Six of the 13 eligible studies, which included 64 rodents, assessed the effects of bumetanide treatment on brain edema (water content (%)) [16–18, 32, 33, 35]. A meta-analysis of findings demonstrated that brain edema was significantly lower in animals treated with bumetanide than in controls (SMD: −1.39; 95% CI: −2.06 to −0.72; p = 0.000; I2 = 82.5%; Figure 3).
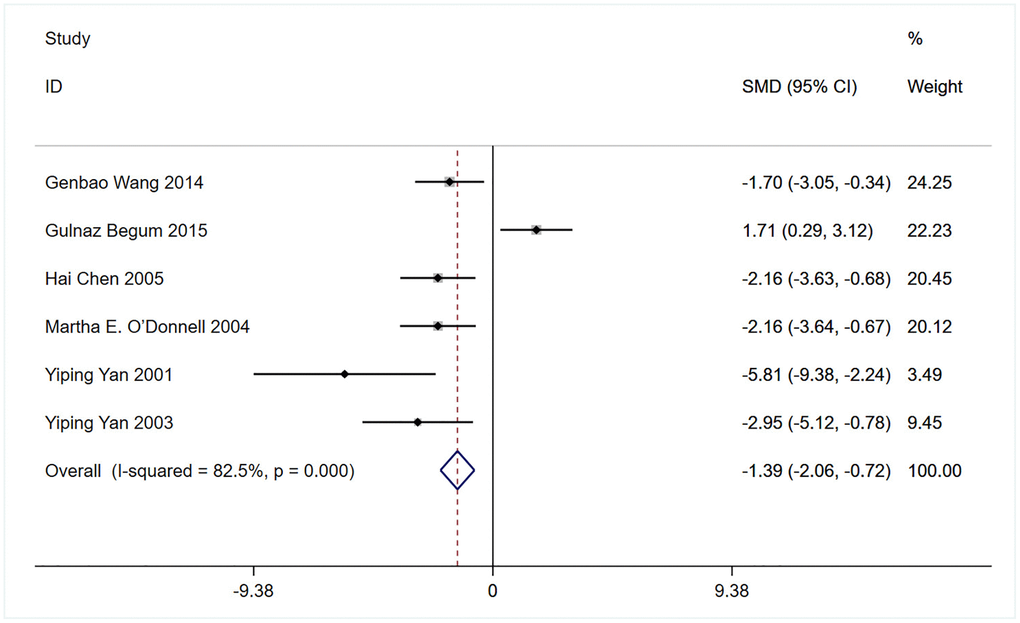
Figure 3. Meta-analysis comparing brain edema (Water content (%)) in rodents receiving bumetanide intervention compared to controls.
Secondary outcome assessment: the effect of bumetanide on neurological function
Eight studies assessed the effects of bumetanide on the neurological function in stroke models (Figure 4) [13–15, 30–34]. Two studies repeatedly assessed the neurological function during the follow-up period. Overall, bumetanide treatment was shown to have a protective effect by improving neurological function compared with the control group (SMD: −2.35; 95% CI: −2.72 to −1.97; p = 0.000; I2 = 86%). Subgroup analyses suggested that bumetanide treatment improved neurological deficit scores and limb function compared to the control group (SMD: −1.77; 95% CI: −2.22 to −1.32; p = 0.000; I2 = 83.7%; SMD: −4.45, 95% CI: −5.41 to −3.50; p = 0.000; I2 = 86.6%, respectively; Figure 4), but not improved cognitive function (SMD: −2.95; 95% CI: −3.97 to −1.93; p = 0.157; I2 = 50.1%). Moreover, the different species did not affect the improvement of neurological function (SMD: −1.77, 95% CI: −2.22 to −1.32; p = 0.000; I2 = 83.7%; Supplementary Figure 1). Sensitivity analyses showed that the exclusion of other studies did not affect the results of the overall analysis.
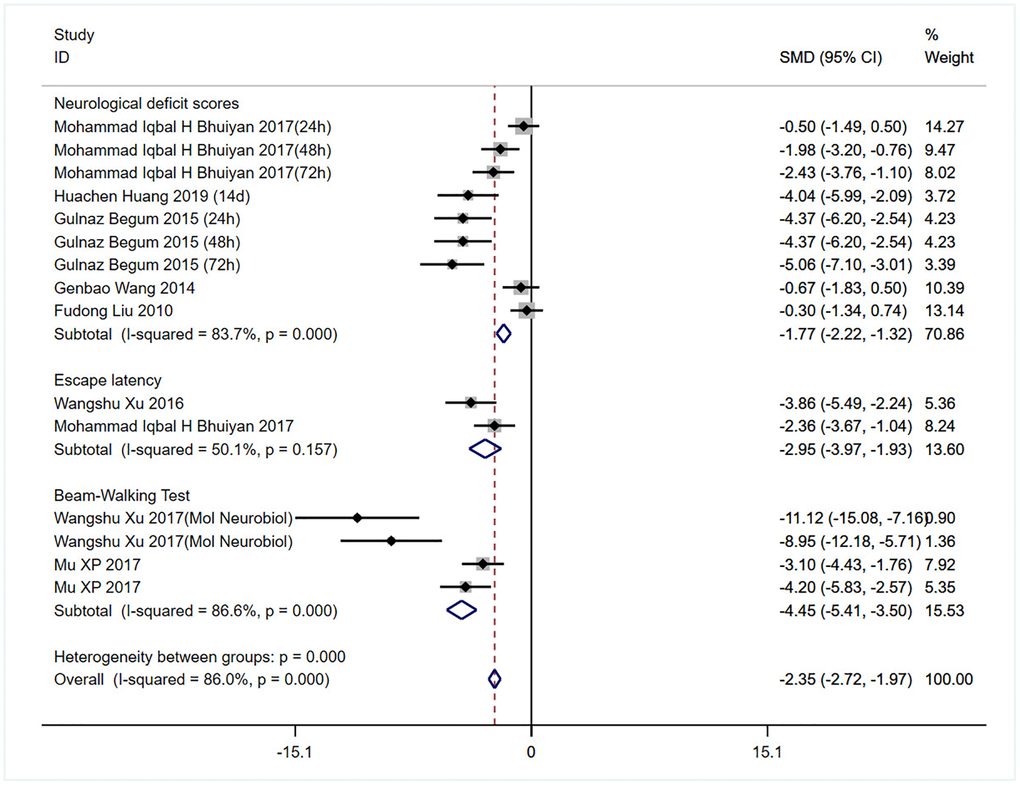
Figure 4. Meta-analysis comparing neurobehavioral function indicated by neurological score, Morris water maze test and tapered/ledged beam walking test in rodents receiving bumetanide intervention compared to controls.
Publication bias
Finally, we sought to identify whether the effect of small studies may contribute to publication bias in bumetanide analysis. Funnel plot (Figure 5) evidenced asymmetry, indicating a potential publication bias. Through Egger’s test, the publication bias existed in infarction volume and neurological function data (p = 0.030, p = 0.000 respectively). Therefore, trim and fill analysis was further used to estimate the risk of publication bias on the results, but no significant bias was detected.
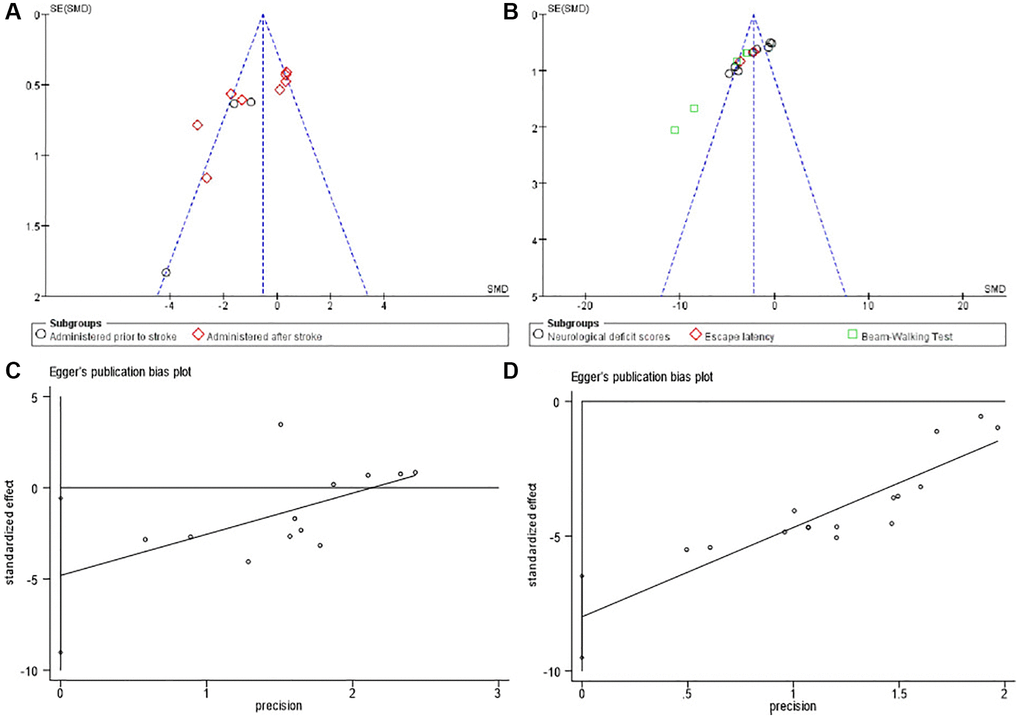
Figure 5. Bias assessment plot for the effect of bumetanide on infarct volumes and neurological function by funnel blot (A, B) and Egger’s test (C, D).
Discussion
Our systematic review and meta-analysis highlight the value of bumetanide in the treatment of cerebral ischemia, with evidence that it can significantly reduce infarct size and cerebral edema and improve neurological function. Subgroup analysis suggested that a transient ischemic model and post-stroke pharmacotherapy may be more effective. Funnel plots showed low published bias for the main outcomes (cerebral infarction volume and neurological function); however, this was difficult to evaluate objectively because relatively few studies were included [36]. Finally, infarct volume was the primary outcome indicator in this meta-analysis, as it is the most widely reported outcome indicator associated with stroke severity in clinical studies and has translational potential.
Clinical investigations have suggested that infarct size is associated with stroke severity [37]. Therefore, reducing infarct size has the potential to treat ischemic stroke. The data from the present review suggest that bumetanide promotes the recovery of infarct size. However, the possibility that bumetanide reduced infarct volume cannot be entirely attributed to reduced edema. For example, bumetanide may promote neurogenesis, strengthen existing neuronal networks, and modulate signaling. The exact mechanisms underlying the beneficial effects of bumetanide need to be fully explored in further studies to provide a new therapeutic target for reducing neurological damage that occurs after stroke. The timing of bumetanide administration is another important factor that needs to be considered. Our meta-analysis showed that bumetanide uses after the acute phase of stroke reduced the size of the cerebral infarction. However, Wang et al. showed bumetanide treatment was most effective in alleviating behavioral changes when administered 10 min before cerebral ischemia induction, and this dosing period had a larger effect size [33]. Whereas this is very difficult to transform it clinically because bumetanide cannot be administered in advance without cerebral infarction. Our meta-analysis also showed that the transient focal cerebral ischemic stroke model may exert higher efficacy because it closely mimics ischemic stroke [38]. In addition, we defined the animal model and outcome indicators before the meta-analysis, which reduced bias in the selection of the included studies. However, while 50% or more of the analyzed studies were produced in the laboratory of Dandan Sun in Pittsburgh, whose reputation is outstanding, the potential for bias was also enhanced.
Cerebral edema after cerebral ischemia and hypoxia is a basic pathophysiological process and a common cause of aggravation, deterioration, and even death, with the incidence of ischemic cerebral edema accounting for 10%. It is defined as an increase in brain tissue volume due to increased fluid content in the brain tissue, which can be life-threatening [38]. Recent studies have shown that bumetanide can reduce the extent of brain necrosis, neurological function scores, and the degree of brain edema in rats after treatment. Similarly, our meta-analysis revealed that bumetanide administration reduced ischemia-induced brain edema. However, the mechanisms underlying cerebral edema remain unclear. Ion channels, transporters, and exchange proteins may be involved in the development of cerebral edema.
In addition to infarct volume, behavioral outcomes need to be assessed because they have the greatest clinical relevance [39]. Until now, it has been argued that bumetanide can alter behavioral recovery in patients with stroke. However, our meta-analysis showed that bumetanide improved neurological deficits, including limb motor function as assessed by the beam-walking test, nevertheless no effect on cognitive function as assessed by escape latency. In addition, the different species did not affect the improvement of the neurological function.
Although our systematic review and meta-analysis validated the ability of bumetanide to reduce infarct size and improve neurological function after ischemic stroke, the underlying mechanisms are poorly understood. Studies in rodent models have shown that bumetanide can promote neurogenesis and axon germination in stroke rats, thereby improving sensorimotor recovery, suggesting that the behavioral effects of bumetanide are related to neuroplasticity [14, 15]. Moreover, mice treated with reduced-subunit-containing GABAARs or low doses of GABAA antagonists have been reported to achieve better behavioral performance, suggesting that reducing excessive GABA-mediated tonics may benefit functional recovery after stroke [40, 41]. As mentioned above, bumetanide facilitates and enhances functional recovery after stroke through NKCC1-mediated GABAergic signaling in the acute phase. WNK3 is an upstream regulator of NKCC1 and activates NKCC1 via phosphorylation [32, 42]. Recent studies have shown that nerve injury can be alleviated, and neurological function recovery can be accelerated by reducing NKCC1 stimulation sites and downregulating NKCC1 expression on wNK3-induced cell surfaces [31, 32]. Therefore, bumetanide treatment had an effect similar to that of GABAA receptor antagonists and WNK3 knockout mice, which may promote functional recovery after stroke via neuroprotection [43].
Limitations
There are several limitations to drawing definitive conclusions. First, our study included only data published in English, which may have led to a certain degree of selection bias. Second, these findings must be interpreted with caution because of the small number of studies included, especially in the subgroup analyses. In addition, other indicators such as blood-brain barrier damage and cerebral perfusion were not evaluated due to the limited data. Third, we judged that the methodological differences in administration methods and doses were too great to justify the meta-analysis; therefore, the optimal dose for stroke treatment was unclear. Fourth, the heterogeneity between the included studies could not be evidently decreased, even if subgroup and sensitivity analyses were performed. Fifth, although all studies used blinding treatment with bumetanide, only four studies concealed treatment from the investigator during outcome assessments; therefore, there is a chance of overestimation of the results. Finally, we performed data extraction from the graphics using a digital ruler software, which may have altered the original data and affected the results.
Conclusions
The advantage of this study is that it is the first meta-analysis of the efficacy of bumetanide in the treatment of ischemic stroke in an animal model. In conclusion, our meta-analysis confirmed the effectiveness of bumetanide therapy in reducing infarct size and improving functional recovery after stroke. Subgroup analysis showed that transient ischemia may be more effective than permanent ischemia and that post-stroke therapy may be more effective than advanced treatment. Altogether, our findings may help to design future experimental and clinical studies.
Supplementary Materials
Author Contributions
HLQ conceived of the study. XYS and JDH collected data and drafted the manuscript. HCX conducted the subgroup analyses. All the authors have read and approved the manuscript.
Acknowledgments
All authors sincerely appreciate the reviewers and supporters of this article.
Conflicts of Interest
The authors declare that the study was conducted without any business or financial relationships that could be interpreted as a potential conflict of interest.
Funding
This study was supported by the Shenyang Science and Technology Planning Project (Grant No: 223213389), Shenyang Young and Middle-Aged Scientific and Technological Innovation Talent Cultivation Project (RC230653).
References
- 1. Yaşar E, Akalın Y, Aktaş İ, Çakmak T, Karakuş Y, Bayramoğlu A. The CHA2DS2-VASc risk score predicts successful endovascular treatment in patients with acute ischemic stroke. Acta Neurol Scand. 2022; 145:407–13. https://doi.org/10.1111/ane.13564 [PubMed]
- 2. Li J, Pan Y, Xu J, Li S, Wang M, Quan K, Meng X, Li H, Lin J, Wang Y, Zhao X, Liu L, Wang Y, and CNSR-III Investigators. Residual Inflammatory Risk Predicts Poor Prognosis in Acute Ischemic Stroke or Transient Ischemic Attack Patients. Stroke. 2021; 52:2827–36. https://doi.org/10.1161/STROKEAHA.120.033152 [PubMed]
- 3. Soliman R, Mamdouh H, Rashed L, Hussein M. The use of recombinant tissue plasminogen activator in in acute ischemic stroke is associated with increased level of BDNF. J Thromb Thrombolysis. 2021; 52:1165–72. https://doi.org/10.1007/s11239-021-02443-1 [PubMed]
- 4. Ooi YC, Miremadi BB, Mukarram F, Kaneko N, Nour M, Colby G, Jahan R, Tateshima S, Duckwiler G, Saver J, Szeder V. Role of Intravenous Tissue Plasminogen Activator in Acute Ischemic Stroke with Large Vessel Occlusion. World Neurosurg. 2021; 148:e321–5. https://doi.org/10.1016/j.wneu.2020.12.142 [PubMed]
- 5. Turner AC, Schwamm LH, Etherton MR. Acute ischemic stroke: improving access to intravenous tissue plasminogen activator. Expert Rev Cardiovasc Ther. 2020; 18:277–87. https://doi.org/10.1080/14779072.2020.1759422 [PubMed]
- 6. Kolbaev SN, Mohapatra N, Chen R, Lombardi A, Staiger JF, Luhmann HJ, Jedlicka P, Kilb W. NKCC-1 mediated Cl- uptake in immature CA3 pyramidal neurons is sufficient to compensate phasic GABAergic inputs. Sci Rep. 2020; 10:18399. https://doi.org/10.1038/s41598-020-75382-1 [PubMed]
- 7. Sulis Sato S, Artoni P, Landi S, Cozzolino O, Parra R, Pracucci E, Trovato F, Szczurkowska J, Luin S, Arosio D, Beltram F, Cancedda L, Kaila K, Ratto GM. Simultaneous two-photon imaging of intracellular chloride concentration and pH in mouse pyramidal neurons in vivo. Proc Natl Acad Sci U S A. 2017; 114:E8770–9. https://doi.org/10.1073/pnas.1702861114 [PubMed]
- 8. Blanquie O, Liebmann L, Hübner CA, Luhmann HJ, Sinning A. NKCC1-Mediated GABAergic Signaling Promotes Postnatal Cell Death in Neocortical Cajal-Retzius Cells. Cereb Cortex. 2017; 27:1644–59. https://doi.org/10.1093/cercor/bhw004 [PubMed]
- 9. Kurki SN, Uvarov P, Pospelov AS, Trontti K, Hübner AK, Srinivasan R, Watanabe M, Hovatta I, Hübner CA, Kaila K, Virtanen MA. Expression patterns of NKCC1 in neurons and non-neuronal cells during cortico-hippocampal development. Cereb Cortex. 2023; 33:5906–23. https://doi.org/10.1093/cercor/bhac470 [PubMed]
- 10. Yamazaki Y, Abe Y, Fujii S, Tanaka KF. Oligodendrocytic Na+-K+-Cl− co-transporter 1 activity facilitates axonal conduction and restores plasticity in the adult mouse brain. Nat Commun. 2021; 12:5146. https://doi.org/10.1038/s41467-021-25488-5 [PubMed]
- 11. Migliati E, Meurice N, DuBois P, Fang JS, Somasekharan S, Beckett E, Flynn G, Yool AJ. Inhibition of aquaporin-1 and aquaporin-4 water permeability by a derivative of the loop diuretic bumetanide acting at an internal pore-occluding binding site. Mol Pharmacol. 2009; 76:105–12. https://doi.org/10.1124/mol.108.053744 [PubMed]
- 12. von Hippel PT. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med Res Methodol. 2015; 15:35. https://doi.org/10.1186/s12874-015-0024-z [PubMed]
- 13. Xu W, Mu X, Wang H, Song C, Ma W, Jolkkonen J, Zhao C. Chloride Co-transporter NKCC1 Inhibitor Bumetanide Enhances Neurogenesis and Behavioral Recovery in Rats After Experimental Stroke. Mol Neurobiol. 2017; 54:2406–14. https://doi.org/10.1007/s12035-016-9819-0 [PubMed]
- 14. Mu XP, Wang HB, Cheng X, Yang L, Sun XY, Qu HL, Zhao SS, Zhou ZK, Liu TT, Xiao T, Song B, Jolkkonen J, Zhao CS. Inhibition of Nkcc1 promotes axonal growth and motor recovery in ischemic rats. Neuroscience. 2017; 365:83–93. https://doi.org/10.1016/j.neuroscience.2017.09.036 [PubMed]
- 15. Xu WS, Sun X, Song CG, Mu XP, Ma WP, Zhang XH, Zhao CS. Bumetanide promotes neural precursor cell regeneration and dendritic development in the hippocampal dentate gyrus in the chronic stage of cerebral ischemia. Neural Regen Res. 2016; 11:745–51. https://doi.org/10.4103/1673-5374.182700 [PubMed]
- 16. Chen H, Luo J, Kintner DB, Shull GE, Sun D. Na(+)-dependent chloride transporter (NKCC1)-null mice exhibit less gray and white matter damage after focal cerebral ischemia. J Cereb Blood Flow Metab. 2005; 25:54–66. https://doi.org/10.1038/sj.jcbfm.9600006 [PubMed]
- 17. O'Donnell ME, Tran L, Lam TI, Liu XB, Anderson SE. Bumetanide inhibition of the blood-brain barrier Na-K-Cl cotransporter reduces edema formation in the rat middle cerebral artery occlusion model of stroke. J Cereb Blood Flow Metab. 2004; 24:1046–56. https://doi.org/10.1097/01.WCB.0000130867.32663.90 [PubMed]
- 18. Yan Y, Dempsey RJ, Flemmer A, Forbush B, Sun D. Inhibition of Na(+)-K(+)-Cl(-) cotransporter during focal cerebral ischemia decreases edema and neuronal damage. Brain Res. 2003; 961:22–31. https://doi.org/10.1016/s0006-8993(02)03832-5 [PubMed]
- 19. Damier P, Degos B, Castelonovo G, Anheim M, Benatru I, Carrière N, Colin O, Defebvre L, Deverdal M, Eusebio A, Ferrier V, Giordana C, Houeto JL, et al. A Double-Blind, Randomized, Placebo-Controlled Trial of Bumetanide in Parkinson's Disease. Mov Disord. 2024; 39:618–22. https://doi.org/10.1002/mds.29726 [PubMed]
- 20. Staley KJ. Clarifications regarding bumetanide for neonatal seizures. Epilepsia. 2022; 63:1863–7. https://doi.org/10.1111/epi.17278 [PubMed]
- 21. Fuentes J, Parellada M, Georgoula C, Oliveira G, Marret S, Crutel V, Albarran C, Lambert E, Pénélaud PF, Ravel D, Ben Ari Y. Bumetanide oral solution for the treatment of children and adolescents with autism spectrum disorder: Results from two randomized phase III studies. Autism Res. 2023; 16:2021–34. https://doi.org/10.1002/aur.3005 [PubMed]
- 22. Beuker C, Strecker JK, Rawal R, Schmidt-Pogoda A, Ruck T, Wiendl H, Klotz L, Schäbitz WR, Sommer CJ, Minnerup H, Meuth SG, Minnerup J. Immune Cell Infiltration into the Brain After Ischemic Stroke in Humans Compared to Mice and Rats: a Systematic Review and Meta-Analysis. Transl Stroke Res. 2021; 12:976–90. https://doi.org/10.1007/s12975-021-00887-4 [PubMed]
- 23. Aliena-Valero A, Baixauli-Martín J, Castelló-Ruiz M, Torregrosa G, Hervás D, Salom JB. Effect of uric acid in animal models of ischemic stroke: A systematic review and meta-analysis. J Cereb Blood Flow Metab. 2021; 41:707–22. https://doi.org/10.1177/0271678X20967459 [PubMed]
- 24. Davis CK, Laud PJ, Bahor Z, Rajanikant GK, Majid A. Systematic review and stratified meta-analysis of the efficacy of carnosine in animal models of ischemic stroke. J Cereb Blood Flow Metab. 2016; 36:1686–94. https://doi.org/10.1177/0271678X16658302 [PubMed]
- 25. Huber VJ, Tsujita M, Nakada T. Identification of aquaporin 4 inhibitors using in vitro and in silico methods. Bioorg Med Chem. 2009; 17:411–7. https://doi.org/10.1016/j.bmc.2007.12.040 [PubMed]
- 26. Minnerup J, Heidrich J, Wellmann J, Rogalewski A, Schneider A, Schäbitz WR. Meta-analysis of the efficacy of granulocyte-colony stimulating factor in animal models of focal cerebral ischemia. Stroke. 2008; 39:1855–61. https://doi.org/10.1161/STROKEAHA.107.506816 [PubMed]
- 27. Hartung J, Knapp G. On tests of the overall treatment effect in meta-analysis with normally distributed responses. Stat Med. 2001; 20:1771–82. https://doi.org/10.1002/sim.791 [PubMed]
- 28. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34. https://doi.org/10.1136/bmj.315.7109.629 [PubMed]
- 29. Wang J, Liu R, Hasan MN, Fischer S, Chen Y, Como M, Fiesler VM, Bhuiyan MIH, Dong S, Li E, Kahle KT, Zhang J, Deng X, et al. Role of SPAK-NKCC1 signaling cascade in the choroid plexus blood-CSF barrier damage after stroke. J Neuroinflammation. 2022; 19:91. https://doi.org/10.1186/s12974-022-02456-4 [PubMed]
- 30. Huang H, Bhuiyan MIH, Jiang T, Song S, Shankar S, Taheri T, Li E, Schreppel P, Hintersteininger M, Yang SS, Lin SH, Molyneaux BJ, Zhang Z, et al. A Novel Na+-K+-Cl− Cotransporter 1 Inhibitor STS66* Reduces Brain Damage in Mice After Ischemic Stroke. Stroke. 2019; 50:1021–5. https://doi.org/10.1161/STROKEAHA.118.024287 [PubMed]
- 31. Bhuiyan MIH, Song S, Yuan H, Begum G, Kofler J, Kahle KT, Yang SS, Lin SH, Alper SL, Subramanya AR, Sun D. WNK-Cab39-NKCC1 signaling increases the susceptibility to ischemic brain damage in hypertensive rats. J Cereb Blood Flow Metab. 2017; 37:2780–94. https://doi.org/10.1177/0271678X16675368 [PubMed]
- 32. Begum G, Yuan H, Kahle KT, Li L, Wang S, Shi Y, Shmukler BE, Yang SS, Lin SH, Alper SL, Sun D. Inhibition of WNK3 Kinase Signaling Reduces Brain Damage and Accelerates Neurological Recovery After Stroke. Stroke. 2015; 46:1956–65. https://doi.org/10.1161/STROKEAHA.115.008939 [PubMed]
- 33. Wang G, Huang H, He Y, Ruan L, Huang J. Bumetanide protects focal cerebral ischemia-reperfusion injury in rat. Int J Clin Exp Pathol. 2014; 7:1487–94. [PubMed]
- 34. Liu F, Akella P, Benashski SE, Xu Y, McCullough LD. Expression of Na-K-Cl cotransporter and edema formation are age dependent after ischemic stroke. Exp Neurol. 2010; 224:356–61. https://doi.org/10.1016/j.expneurol.2010.04.010 [PubMed]
- 35. Yan Y, Dempsey RJ, Sun D. Na+-K+-Cl- cotransporter in rat focal cerebral ischemia. J Cereb Blood Flow Metab. 2001; 21:711–21. https://doi.org/10.1097/00004647-200106000-00009 [PubMed]
- 36. Crossley NA, Sena E, Goehler J, Horn J, van der Worp B, Bath PM, Macleod M, Dirnagl U. Empirical evidence of bias in the design of experimental stroke studies: a metaepidemiologic approach. Stroke. 2008; 39:929–34. https://doi.org/10.1161/STROKEAHA.107.498725 [PubMed]
- 37. Laredo C, Zhao Y, Rudilosso S, Renú A, Pariente JC, Chamorro Á, Urra X. Prognostic Significance of Infarct Size and Location: The Case of Insular Stroke. Sci Rep. 2018; 8:9498. https://doi.org/10.1038/s41598-018-27883-3 [PubMed]
- 38. Hermann DM, Popa-Wagner A, Kleinschnitz C, Doeppner TR. Animal models of ischemic stroke and their impact on drug discovery. Expert Opin Drug Discov. 2019; 14:315–26. https://doi.org/10.1080/17460441.2019.1573984 [PubMed]
- 39. Balkaya M, Kröber JM, Rex A, Endres M. Assessing post-stroke behavior in mouse models of focal ischemia. J Cereb Blood Flow Metab. 2013; 33:330–8. https://doi.org/10.1038/jcbfm.2012.185 [PubMed]
- 40. Clarkson AN, Huang BS, Macisaac SE, Mody I, Carmichael ST. Reducing excessive GABA-mediated tonic inhibition promotes functional recovery after stroke. Nature. 2010; 468:305–9. https://doi.org/10.1038/nature09511 [PubMed]
- 41. Shulga A, Thomas-Crusells J, Sigl T, Blaesse A, Mestres P, Meyer M, Yan Q, Kaila K, Saarma M, Rivera C, Giehl KM. Posttraumatic GABA(A)-mediated [Ca2+]i increase is essential for the induction of brain-derived neurotrophic factor-dependent survival of mature central neurons. J Neurosci. 2008; 28:6996–7005. https://doi.org/10.1523/JNEUROSCI.5268-07.2008 [PubMed]
- 42. Kahle KT, Rinehart J, de Los Heros P, Louvi A, Meade P, Vazquez N, Hebert SC, Gamba G, Gimenez I, Lifton RP. WNK3 modulates transport of Cl- in and out of cells: implications for control of cell volume and neuronal excitability. Proc Natl Acad Sci U S A. 2005; 102:16783–8. https://doi.org/10.1073/pnas.0508307102 [PubMed]
- 43. Hermann DM, Chopp M. Promoting brain remodelling and plasticity for stroke recovery: therapeutic promise and potential pitfalls of clinical translation. Lancet Neurol. 2012; 11:369–80. https://doi.org/10.1016/S1474-4422(12)70039-X [PubMed]