



Introduction
Lung cancer is the leading cause of cancer death [1]. Approximately 80% to 85% of lung cancer cases were NSCLC [2]. In 2020, nearly 2.20 million people were diagnosed with lung cancer, and approximately 1.80 million people died from lung cancer [1]. The high mortality of lung cancer is closely related to its biological characteristics of easy metastasis and recurrence. Sugimura and co-workers found that more than 40% NSCLC patients who underwent complete resection experienced cancer recurrence and the median disease-free survival (DFS) was 11.5 months, while the median survival time was 8.1 months after the recurrence of tumor [3]. In terms of the mechanism of tumor recurrence and metastasis, some research believe that the blood hypercoagulable state is closely related to immune escape, adhesion and metastasis of tumor cells [4–6]. Choi PJ and Farge D reported that elevated preoperative platelet (PLT) levels increase the risk of NSCLC progression [7, 8]. Lin Y and Can Hou indicated that D-dimer and fibrinogen (FIB) may play important roles in predicting the tumor prognosis [9, 10], and patients with at least two of three coagulation indicators elevated (D-dimer, FIB and PLT) have a significantly higher risk of cancer progression than those of patients with one coagulation indicator elevated.
There are many syndrome types in stage II–III NSCLC patients, such as blood stasis, Qi deficiency, Qi stagnation, toxin retention, generation of dampness, and so on [11–13]. Above findings that hypercoagulable state increases the risk of tumor recurrence and metastasis are highly consistent with the Traditional Chinese Medicine (TCM) theory that blood stasis syndrome promotes tumor recurrence and metastasis. Therefore, as the crystallization of TCM theory, varieties of Chinese patent medicine (CPM) such as heat-clearing and detoxicating medicine, medicine of promoting blood circulation and removing blood stasis, and medicine of nourishing healthy qi and eliminating blood stasis are widely used to treat the tumor. However, it is challenging to assess the efficacy of most anti-tumor Chinese medicine, which largely attributed to the lack of rigorous clinical research design and the characteristics of complex component, multi-target, and low-medium action intensity of TCM. In addition, most of the previous studies ignore the effective exposure dose (cumulative treatment duration) of TCM, which somewhat limits the further development of CPM. Encouragingly, several researchers have focused on these issues by conducting rigorous prospective cohort studies. The results have shown that the more extended use of TCM, the higher survival rate of patients with stage II and III colorectal cancer would be [14], and long-term use of TCM was a protective factor for preventing the recurrence and metastasis of NSCLC [15].
Huisheng oral solution, a CPM composed of 34 Chinese medicine components, is commonly prescribed to treat tumor in China. Previous experiments demonstrated that HSOS exerted anti-tumor effect via enhancing body immunity, promoting blood circulation and removing blood stasis [16–19] and reduce the level of PLT and FIB in SD rats [20]. Another animal experiment found that HSOS showed benefits in reducing the level of FIB, down-regulating the expression of related factors in C57 mice, and improving blood hypercoagulative state, thus achieved anti-tumor effects [21]. However, few epidemiologic studies have focused on the association between different cumulative treatment durations of CPM/HSOS and NSCLC patient’s survival rate. Therefore, this study was conducted to evaluate the effect of CPM/HSOS on four-year survival rate of patients with stage II and III NSCLC, and to figure out the relationship between blood coagulation indicators and survival outcomes.
Materials and Methods
Participants
1301 patients were diagnosed with lung cancer in Sichuan Provincial People’s Hospital during 2015–2016. 313 patients among them were finally included in statistical analysis according to the inclusion and exclusion criteria. The follow-up period was 48 months, 170 (54.3%) patients died in 4 years, 43 (13.7%) patients lost to follow-up, and 100 (31.9%) patients were still alive until the end of this study. The study was reviewed and approved by the Ethics Committee of Sichuan Provincial People’s Hospital (Number: 2019-205). Written informed consent for participation was acquired.
Inclusion criteria
Patients included in the study had to meet the following items: (1) Patients diagnosed with stage II and III NSCLC (2015 NCCN Guidelines: Non-Small Cell Lung Cancer, [22]) in Sichuan Provincial People’s Hospital during 2015–2016. (2) Patients who had a proper compliance of the study with no less than 2 records of return visit.
Exclusion criteria
The patients were manually excluded if any of the following items were met: (1) Patients not meeting the inclusion criteria; (2) Patients with other solid tumor or hematological tumor; (3) Patients with a history of thrombosis, or complicated with severe cardiovascular and cerebrovascular diseases, severe coagulation dysfunction, and severe rheumatic diseases; (4) Patients with other conditions deemed unsuitable for inclusion by the researchers; (5) Patients who had serious complications (heart failure, respiratory failure and deep coma not caused by venous thrombus embolism) or died within 30 days after enrollment or surgery; (6) Patients with uncontrollable neurological, psychiatric or mental disorders; (7) Patients with no follow-up record after admission.
Groups
(1) To compare the survival outcomes between the patients who received CPM for less than 3 months and those who received CPM for more than 3 months; (2) To compare the survival outcomes between the patients who received CPM for less than 3 months and those who received CPM for more than 6 months; (3) To compare the survival outcomes between the patients who received HSOS less than 3 months and those who received HSOS more than 3 months. The treatment duration was defined as the cumulative days of receiving such treatment recorded in the Hospital Information System (HIS) during the study period.
Follow-up
The follow-up period was 48 months (4 years), and there were 7 data collection points and 1 final telephone follow-up point. All kinds of examination, medication records and outcome of each patient were collected at the time of enrollment, and 1 month, 3 months, 6 months, 1 year, 2 years, and 4 years after enrollment respectively.
Outcomes
The primary endpoint was death caused by NSCLC in 4 years. Blood routine and preoperative coagulation indicators were also collected at each observation point.
Statistical analysis
The number of cases, mean, standard deviation, t-value and F value of continuous quantitative variables were calculated, and the baseline of continuous quantitative variables were evaluated by single factor analysis of variance. As for qualitative variables, the frequency, composition ratio and chi-square statistics were calculated under each category, and the chi-square test was used to evaluate the baseline of qualitative variables in different groups. Kaplan-Meier method was utilized to plot survival curves, and Cox proportional hazard model was applied to analyze the factors that might affect the prognosis for patients with stage II and III NSCLC. All tests were two-sided, and were performed by R 4.0.3. The abbreviation list was shown in Supplementary Table 1.
Procedures
1301 patients were diagnosed with lung cancer in Sichuan Provincial People’s Hospital during 2015–2016, and 313 patients with stage II and III NSCLC were included in statistical analysis according to the inclusion and exclusion criteria (Supplementary Table 2). Firstly, the status of combination use of CPM and Western medicine was analyzed, including the frequency of using each treatment and classification analysis according to the characteristics of each CPM’s formula. Secondly, the differences of primary outcome between the patients who received CPM for less than 3 months, more than 3 months, and more than 6 months were compared, and the difference of primary outcome between the patients who received HSOS for less than 3 months and more than 3 months was also compared. Finally, Kaplan-Meier method and Cox proportional hazard model were applied to analyze the effect of other factors on patients’ outcomes. The follow-up period was 48 months (4 years). 43 patients lost to follow-up. The rate of lost to follow-up was 13.7% (Figure 1).
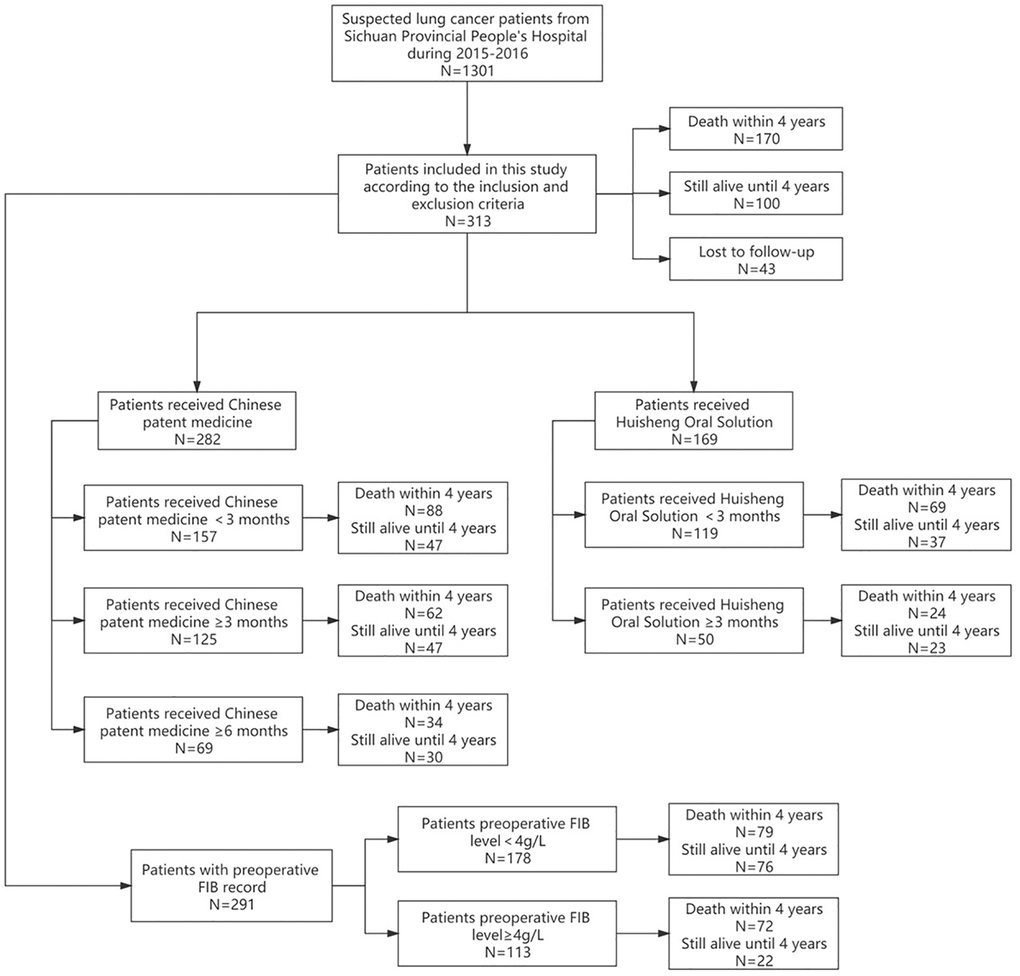
Figure 1. Research profile.
Results
The summary of all treatment used in patients diagnosed with NSCLC in Sichuan Provincial People’s Hospital during 2015–2016
The frequency of each treatment used in 313 patients
The frequency of all kinds of treatments for patients diagnosed with stage II and III NSCLC in Sichuan Provincial People’s Hospital during 2015–2016 was shown in Figure 2. The frequency of surgery was 65%, chemotherapy was 61%, radiotherapy was 23%, targeted therapy was 5%, oral CPM was 70%, TCM decoction was 9%, CPM injection was 75%, and oral anticoagulant drug was 10%. None of patients received immunotherapy.
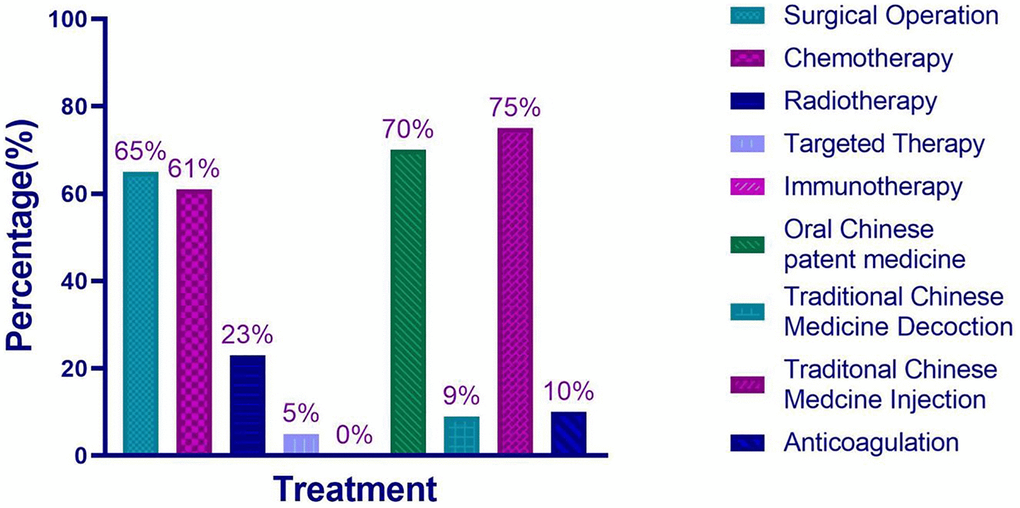
Figure 2. The frequency of each treatment used for 313 patients diagnosed with NSCLC in Sichuan Provincial People’s Hospital during 2015–2016.
Analysis of different types of Chinese patent medicine
In view of the fact that syndrome differentiation for patients was not the same, we conducted further analysis of different types of Chinese patent medicine received by patients with stage II and III NSCLC. A total of 8 kinds of Chinese patent medicine related to tumor treatment were prescribed in Sichuan Provincial People’s Hospital, and all of these Chinese patent medicines were classified into “Jiedu Kangai (解毒抗癌)” and “Fuzheng Quyu (扶正祛瘀)” according to the effect and characteristics of their formula. The results were listed as follows (Table 1).
Table 1. The treatment duration of two types of Chinese patent medicine for 313 patients (month).
| Type | Never used | Treatment duration <3 M | 3 M ≤ Treatment duration <6 M | Treatment duration ≥6 M | Total |
| Jiedu kangai | |||||
| Cinobufacin capsule | 296 (94.6%) | 7 (2.2%) | 3 (1.0%) | 7 (2.2%) | 313 |
| Fructus bruccae emulsion | 134 (42.8%) | 176 (56.2%) | 3 (1.0%) | 0 (0%) | 313 |
| Fuzheng quyu | |||||
| Huisheng oral solution | 144 (46.0%) | 119 (38.0%) | 17 (5.4%) | 33 (10.6%) | 313 |
| Fu-fangbanmao capsule | 173 (55.3%) | 129 (41.2%) | 5 (1.6%) | 6 (1.9%) | 313 |
| Kanglixin capsule | 238 (76.1%) | 52 (16.6%) | 11 (3.5%) | 12 (3.8%) | 313 |
| Aidi injection | 179 (57.2%) | 134 (42.8%) | 0 (0%) | 0 (0%) | 313 |
Comparison of baseline characteristics among patients who received CPM/HSOS for different durations (less than 3 months vs. more than 3 months vs. more than 6 months)
Baseline characteristics among patients who received CPM for different durations (less than 3 months vs. more than 3 months vs. more than 6 months)
There was no statistical significance between the baseline characteristics of three groups. The patients between three groups were comparable. Results were listed as follows (Table 2).
Table 2. Comparison of baseline characteristics between 3 groups with different treatment duration of Chinese patent medicine for 313 patients.
| Variable | Treatment duration <3 M | Treatment duration ≥3 M | Treatment duration ≥6 M | Statistics | P-value |
| Gender | |||||
| Male | 132 | 100 | 52 | χ2 = 3.816 | P = 0.148 |
| Female | 56 | 25 | 17 | ||
| Age | 63.22 (±9.85) | 62.89 (±9.96) | 63.59 (±10.30) | F = 0.115 | P = 0.892 |
| Stage | |||||
| II | 72 | 46 | 25 | χ2 = 0.124 | P = 0.940 |
| III | 116 | 79 | 44 | ||
| Pathological types | |||||
| Squamous carcinoma | 62 | 50 | 22 | Fisher’s exact test | P = 0.214 |
| Adenocarcinoma | 83 | 59 | 38 | ||
| Poor differentiated carcinoma | 9 | 5 | 3 | ||
| Large cell carcinoma | 0 | 1 | 0 | ||
| Spindle cell carcinoma | 1 | 0 | 0 | ||
| Other types | 33 | 10 | 6 | ||
| Blood routine | |||||
| PLT | 209.34 (±83.02) | 211.71 (±86.22) | 205.79 (±94.2) | F = 0.102 | P = 0.813 |
| Coagulation indicators | |||||
| FIB | 3.90 (±1.42) | 3.80 (±1.26) | 3.82 (±1.33) | F = 0.207 | P = 0.989 |
| D-Dimer | 0.92 (±2.31) | 1.22 (±4.16) | 2.13 (±5.96) | F = 0.581 | P = 0.561 |
| TT | 18.26 (±2.20) | 18.27 (±1.96) | 18.17 (±1.83) | F = 0.059 | P = 0.942 |
| PT | 11.40 (±0.99) | 11.21 (±0.84) | 11.23 (±0.89) | F = 1.031 | P = 0.359 |
| APTT | 28.20 (±4.23) | 28.33 (±4.70) | 28.15 (±4.35) | F = 0.027 | P = 0.974 |
Baseline characteristics between patients who received HSOS for less than 3 months and patients who received HSOS for more than 3 months
There was no statistical significance in the difference of baseline characteristics, which indicated that the patients were comparable between two groups. The results were listed as follows (Table 3).
Table 3. Comparison of baseline characteristics between 2 groups with different treatment duration of Huisheng oral solution for 169 patients.
| Variable | Treatment duration <3 M | Treatment duration ≥3 M | Statistics | P-value |
| Gender | ||||
| Male | 91 | 36 | χ2 = 0.642 | P = 0.423 |
| Female | 26 | 14 | ||
| Age | 62.28 (±10.11) | 63.88 (±9.62) | t = −0.949 | P = 0.344 |
| Stage | ||||
| II | 47 | 17 | χ2 = 0.564 | P = 0.453 |
| III | 70 | 33 | ||
| Pathological types | ||||
| Squamous carcinoma | 49 | 16 | Fisher’s exact test | P = 0.583 |
| Adenocarcinoma | 51 | 27 | ||
| Poor differentiated carcinoma | 3 | 3 | ||
| Large cell carcinoma | 1 | 0 | ||
| Spindle cell carcinoma | 1 | 0 | ||
| Other types | 12 | 4 | ||
| Blood routine | ||||
| PLT | 216.44 (±80.84) | 200.80 (±104.00) | t = 1.034 | P = 0.302 |
| Coagulation indicators | ||||
| FIB | 3.88 (±1.34) | 3.72 (±1.33) | t = 0.696 | P = 0.488 |
| D-Dimer | 0.58 (±0.65) | 2.78 (±7.46) | t = −1.473 | P = 0.151 |
| TT | 18.43 (±1.98) | 18.11 (±1.87) | t = 0.953 | P = 0.342 |
| PT | 11.32 (±0.98) | 11.17 (±0.74) | t = 0.740 | P = 0.461 |
| APTT | 27.81 (±3.94) | 28.59 (±4.70) | t = −0.834 | P = 0.407 |
4-year survival rate for patients treated with different durations of CPM/HSOS
Survival analysis of patients who received CPM for less than 3 months and patients who received CPM for more than 3 months
188 patients received CPM less than 3 months, 105 of them died during the study. The one-year, two-year, three-year, and four-year survival rate were 70%, 51%, 41%, and 31%, respectively. 125 patients received CPM for more than 3 months, and 62 of them died during the study. The one-year; two-year; three-year and four-year survival rate were 83%, 63%, 50%, and 42%, respectively. Kaplan-Meier method was applied to analyze the difference of outcomes between two groups, and the results showed that the difference between two groups was statistically significant (P = 0.021), which indicated that the 4-year survival rate of patients with CPM used for ≥3 months was higher than that of patients with CPM used for <3 months (Figure 3). The shadow of two survival curves in different color represented the 95% confidence interval of survival probability for each curve, which also applied to Figures 4 and 5.
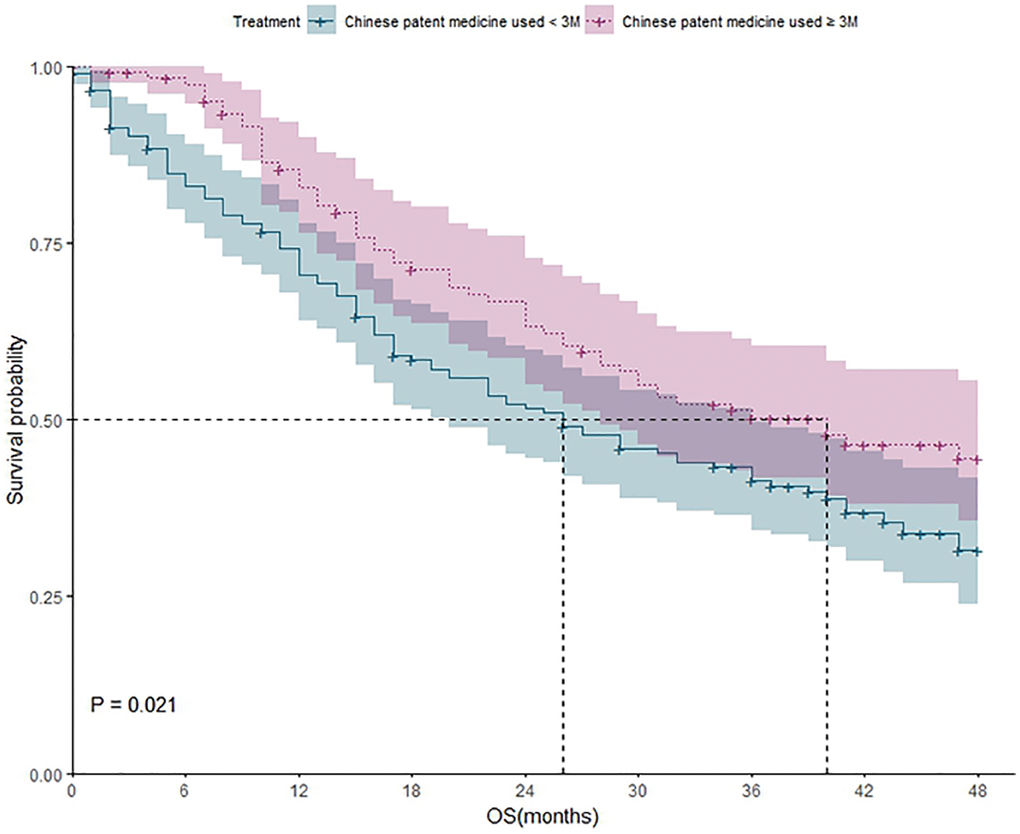
Figure 3. The survival analysis of patients who received CPM for different durations (less than 3 months vs. more than 3 months).
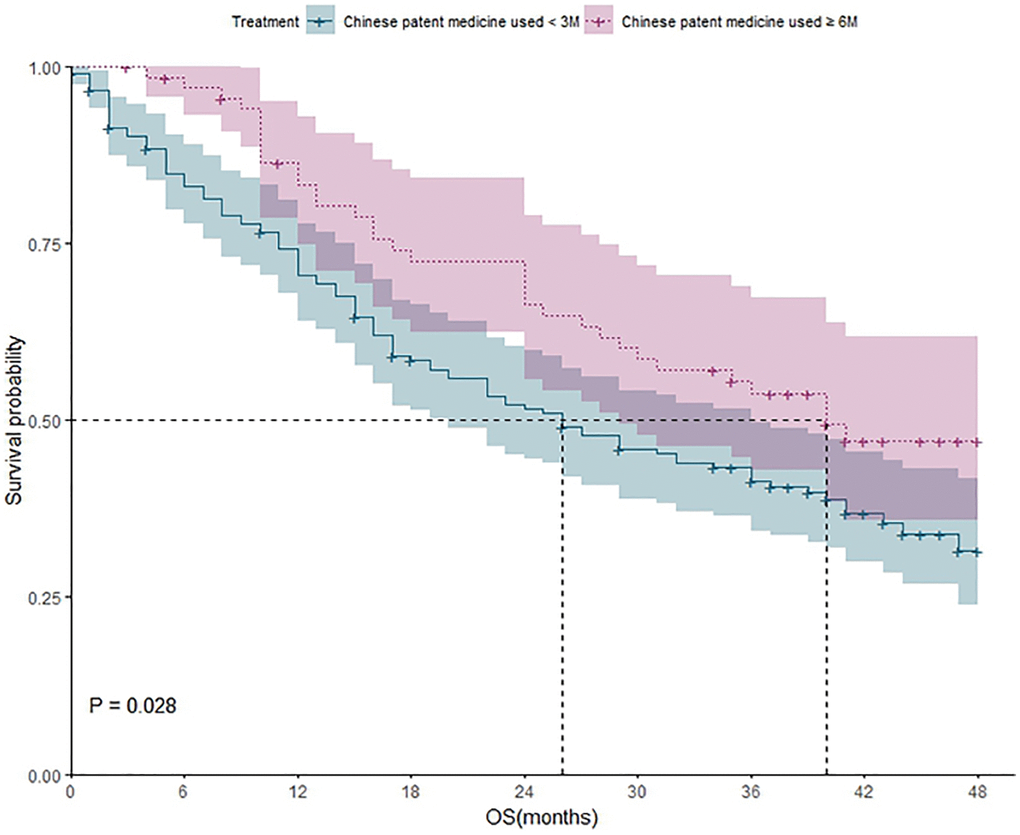
Figure 4. The survival analysis of patients who received CPM for different durations (less than 3 months vs. more than 6 months).
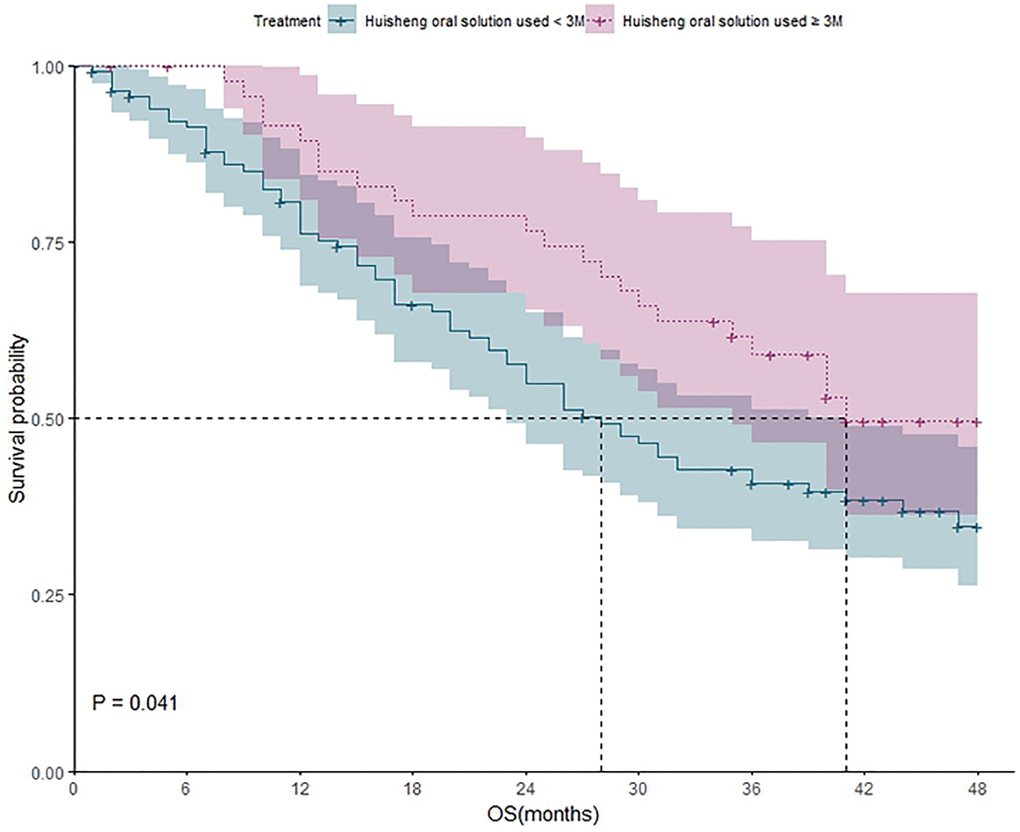
Figure 5. The survival analysis of patients who received HSOS for different durations (less than 3 months vs. more than 3 months).
Survival analysis of patients who received CPM for less than 3 months and patients who received CPM for more than 6 months
188 patients received CPM for less than 3 months, and 105 of them died during the study. The one-year, two-year three-year, and four-year survival rate were 70%; 51%; 41%, and 31%, respectively. 69 patients received CPM for more than 6 months, and 34 of them died during the study. The one-year, two-year, three-year, and four-year survival rate were 83%, 66%, 53%, and 43% respectively. Kaplan-Meier method was applied to analyze the difference of outcomes between two groups, and the result showed that the difference between the two groups was statistically significant (P = 0.028). It revealed that the 4-year survival rate of patients with CPM used for ≥6 months was higher than that of patients with CPM used for <3 months (Figure 4).
Survival analysis of patients who received HSOS less than 3 months and patients who received HSOS more than 3 months
117 patients received HSOS less than 3 months, and 68 of them died during the study. The one-year, two-year, three-year, and four-year survival rate were 75%, 54%, 40%, and 35%, respectively. 50 patients received HSOS more than 3 months, and 22 of whom died during the study. The one-year, two-year, three-year, and four-year survival rate were 89%, 77%, 60%, and 51%, respectively. Kaplan-Meier method was applied to analyze the difference of outcomes between two groups, and the result showed that the difference between two groups was statistically significant (P = 0.041), which demonstrated that the 4-year survival rate of patients with HSOS used for ≥3 months was higher than that of patients with HSOS used for <3 months (Figure 5).
Multivariate analysis via Cox proportional hazard model
The factors that might affect the survival outcome of patients were included in the Cox proportional hazard model. The results indicated that elevated preoperative FIB level (P < 0.01), surgery (P < 0.01), and patients received HSOS more than 3 months were statistically significant in the model (P < 0.01). The hazard of death for patients with preoperative FIB level more than 4 g/L was 1.98 times higher than that of patients with preoperative FIB level less than 4 g/L, and for patients without surgery was 2.76 times higher than that of patients underwent surgery. Besides, we also found that the hazard of death for patients who received HSOS more than 3 months was just half that of patients who received HSOS less than 3 months (Figure 6 and Table 4).
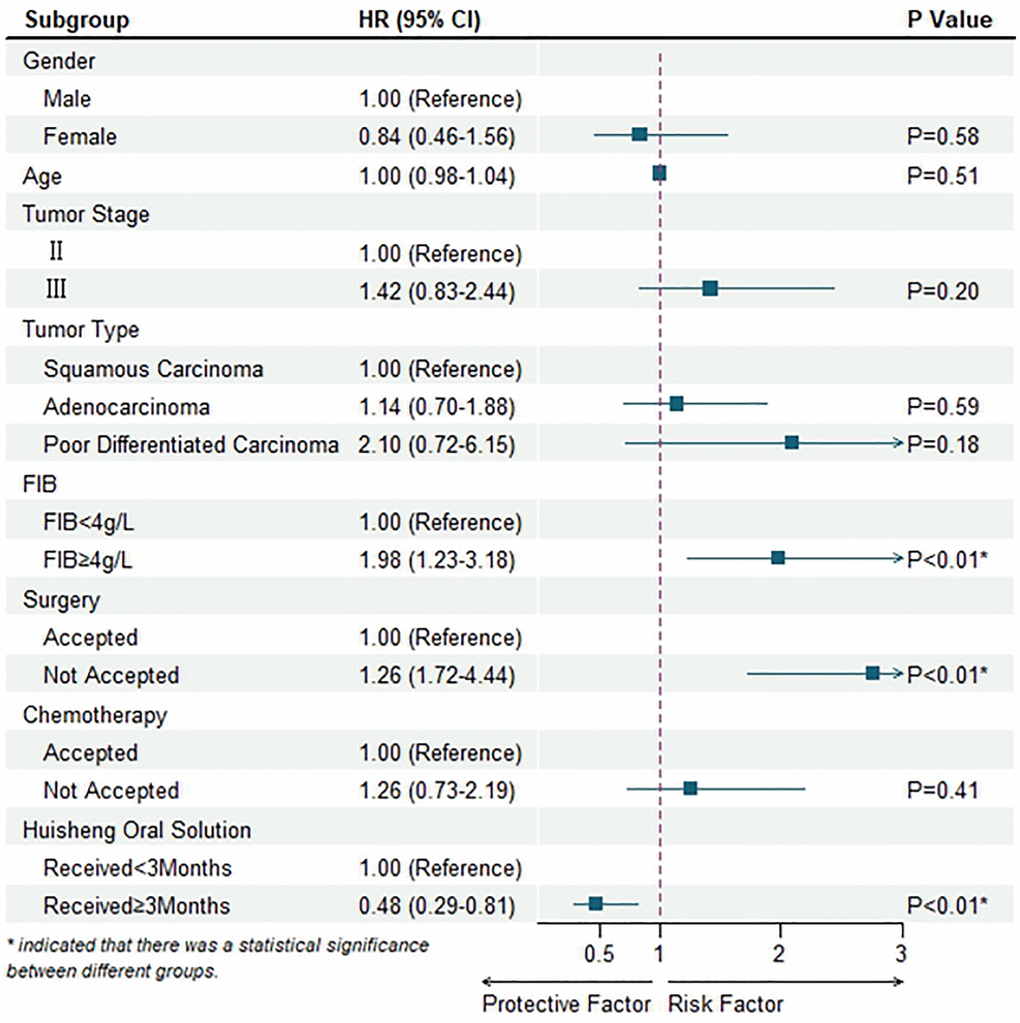
Figure 6. Multivariable Cox regression mode.
Table 4. Multivariable Cox regression model.
| Variable | Hazard ratio (95% CI) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 1.00 (Reference) | P = 0.58 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 0.84 (0.46–1.56) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 1.00 (0.98–1.04) | P = 0.51 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 1.00 (Reference) | P = 0.20 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 1.42 (0.83–2.44) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor type | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Squamous carcinoma | 1.00 (Reference) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adenocarcinoma | 1.14 (0.70–1.88) | P = 0.59 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Poor differentiated carcinoma | 2.10 (0.72–6.15) | P = 0.18 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FIB | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FIB <4 g/L | 1.00 (Reference) | P < 0.01* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FIB ≥4 g/L | 1.98 (1.23–3.18) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Surgery | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Accepted | 1.00 (Reference) | P < 0.01* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not accepted | 2.76 (1.72–4.44) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chemotherapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Accepted | 1.00 (Reference) | P = 0.41 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not accepted | 1.26 (0.73–2.19) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Huisheng oral solution | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Received <3 months | 1.00 (Reference) | P < 0.01* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Received ≥3 months | 0.48 (0.29–0.81) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Indicated that there was a statistical significance between different groups. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Safety assessment
No adverse reactions related to HSOS were recorded in this study. All of the adverse reactions documented in the included medical records were evaluated as side effect of radiotherapy and chemotherapy by doctors in this research. HSOS has been prescribed for clinical use more than 20 years. A total of 46 cases of adverse reactions were found in the database of National Adverse Drug Reaction Monitoring System, which were all new and general adverse reactions [23, 24]. The national adverse drug reaction information and pharmacovigilance notice related to HSOS were not received, and no serious adverse reactions had been reported from clinical researches (Table 5).
Table 5. The summary of adverse reactions for HSOS from national adverse drug reaction monitoring system.
| No. | Adverse reaction | Occurred time | Prognosis | The reason of using HSOS | Remark |
| 1 | Diarrhea | 2011-11-17 | Improved | Lung cancer treatment | General adverse reaction |
| 2 | Fatigue, myalgia | 2011-3-26 | Improved | Esophageal cancer treatment | General adverse reaction |
| 3 | Dyspnea, chest tightness, insomnia | 2012-3-5 | Improved | Liver cancer treatment | General adverse reaction |
| 4 | Nausea, emsis | 2012-3-3 | Improved | Laryngopharynx cancer treatment | General adverse reaction |
| 5 | Fever | 2012-4-5 | Recovery | Cancer treatment | General adverse reaction |
| 6 | Nausea, diarrhea | 2012-11-1 | Recovery | Cancer treatment | General adverse reaction |
| 7 | Emesis | 2014-8-22 | Recovery | Eliminating disease, and removing blood stasis | General adverse reaction |
| 8 | Abdominalgia | 2014-9-4 | Recovery | Eliminating disease, and removing blood stasis | General adverse reaction |
| 9 | Rash, pruritus | 2014-7-20 | Recovery | Eliminating disease, and removing blood stasis | General adverse reaction |
| 10 | Emesis, nausea | 2014-7-16 | Improved | Lung cancer treatment | General adverse reaction |
| 11 | Waist soreness | 2014-7-28 | Unknown | Adjuvant therapy for cancer treatment | General adverse reaction |
| 12 | Dizziness | 2014-7-22 | Improved | Cancer treatment | General adverse reaction |
| 13 | Nausea, abdominalgia | 2014-10-10 | Improved | Cancer treatment | General adverse reaction |
| 14 | Rash, pruritus | 2014-9-21 | Recovery | Lung cancer treatment | General adverse reaction |
| 15 | Nausea, emesis | 2014-11-26 | Improved | Cancer treatment | General adverse reaction |
| 16 | Ulcer | 2014-8-6 | Recovery | Eliminating disease, and removing blood stasis | General adverse reaction |
| 17 | Rash | 2015-6-26 | Improved | Combined with other chemotherapy | General adverse reaction |
| 18 | Nausea, emesis | 2015-11-6 | Improved | Cancer treatment | General adverse reaction |
| 19 | Oral ulcer | 2015-9-18 | Recovery | Trachea, bronchus and lung cancer treatment | General adverse reaction |
| 20 | Nausea | 2015-4-20 | Improved | Gastric cancer treatment | General adverse reaction |
| 21 | Emesis | 2015-5-10 | Improved | Esophageal cancer treatment | General adverse reaction |
| 22 | Rash | 2015-11-26 | Recovery | Symptomatic treatment | General adverse reaction |
| 23 | Nausea, emesis | 2016-5-3 | Improved | Adjuvant therapy | General adverse reaction |
| 24 | Nausea | 2016-6-6 | Improved | Pneumonia treatment | General adverse reaction |
| 25 | Nausea | 2016-9-7 | Improved | Breast cancer treatment | General adverse reaction |
| 26 | Nausea | 2016-9-16 | Improved | Fibrosarcoma treatment | General adverse reaction |
| 27 | Diarrhea, abdominalgia | 2016-5-27 | Improved | Lung cancer | General adverse reaction |
| 28 | Severe pain | 2016-10-6 | Improved | Eliminating disease, and removing blood stasis | General adverse reaction |
| 29 | Dizziness, emesis | 2016-11-22 | Improved | Lung cancer treatment | General adverse reaction |
| 30 | Abdominal distension | 2016-11-27 | Improved | Cancer treatment | General adverse reaction |
| 31 | Dermatologic diseases | 2017-2-23 | Maintain | Cancer treatment | General adverse reaction |
| 32 | Diarrhea, abdominalgia, nausea, emesis | 2017-2-8 | Improved | Breast cancer treatment | General adverse reaction |
| 33 | Pruritus | 2017-12-3 | Improved | Cancer treatment | General adverse reaction |
| 34 | Diarrhea, dizziness | 2018-4-29 | Improved | Gastritis, bronchitis and lung cancer treatment | General adverse reaction |
| 35 | Papule, pruritus | 2018-8-7 | Improved | Lung cancer treatment | General adverse reaction |
| 36 | Rash | 2018-9-28 | Improved | Cancer treatment | General adverse reaction |
| 37 | Erythematous eruption | 2018-12-16 | Improved | Lung cancer treatment | General adverse reaction |
| 38 | Chill, Cyanosis | 2019-7-22 | Improved | Cancer treatment | General adverse reaction |
| 39 | Emesis, | 2019-12-25 | Improved | Cancer treatment | General adverse reaction |
| 40 | Rash, pruritus | 2020-5-8 | Improved | Cancer treatment | General adverse reaction |
| 41 | Skin allergy | 2020-6-25 | Recovery | Eliminating disease, and removing blood stasis | General adverse reaction |
| 42 | Eilema | 2020-8-13 | Recovery | Gastric cancer treatment | General adverse reaction |
| 43 | Dizziness, instability of gait | 2020-10-28 | Recovery | Lung cancer treatment | General adverse reaction |
| 44 | Abdominalgia | 2020-6-15 | Improved | Adjuvant therapy for cancer treatment | General adverse reaction |
| 45 | Nausea | 2021-1-3 | Recovery | Strengthen body | General adverse reaction |
| 46 | Diarrhea | 2021-1-22 | Improved | Rheumatoid arthritis treatment | General adverse reaction |
The names and traditional use of botanical compositions in HSOS
The botanical compositions and traditional use or pharmacological effect of HSOS were listed as follows (Table 6).
Table 6. The names and traditional use of botanical composition in Huisheng oral solution.
| No. | Accepted name | Chinese name | Latin name | Traditional use or pharmacological effect |
| 1 | Leonurus japonicus Houtt. | 益母草 | Leonuri Herba | Reduction of whole blood viscosity and platelets aggression (Liu XH et al., 2007) |
| 2 | Sparganium stoloniferum (Buch.-Ham. ex Graebn.) Buch.-Ham. ex Juz. | 三棱 | Sparganii Rhizoma | Anti-tumor and antithrombotic effects (Jia J et al., 2020) |
| 3 | Dalbergia odorifera T.C.Chen. | 降香 | Lignum Dalbergiae Odoriferae | Common use for promoting blood circulation, relieving pain and removing blood stasis (Yang ZH et al., 2013) |
| 4 | Alpinia officinarum Hance. | 高良姜 | Alpiniae Officinarum Rhizoma | Application to treating inflammation, pain, and stomach-ache (Abubakar IB et al., 2018) |
| 5 | Prunus armeniaca L. | 苦杏仁 | Armeniacae Semen Amarum | Application to treating dyschesia, constipation, abdominal fullness, fatigue and pale tongue (Gao L et al., 2014) |
| 6 | Foeniculum vulgare Mill. | 小茴香 | Foeniculi Fructus | Wide use as an antiemetic ameliorating stomach conditions or an analgesic (Lee JH et al., 2012) |
| 7 | Corydalis yanhusuo (Y.H.Chou and Chun C.Hsu) W.T.Wang ex Z.Y.Su and C.Y.Wu | 延胡索 | Corydalis Rhizoma | Antithrombotic, antimicrobial and anti-inflammation activity (Tian B et al., 2020) |
| 8 | Boswellia carteri Birdw. | 乳香 | Olibanum | Anti-inflammatory, anti-arthritic and anti-cancer effects (Choi OB et al., 2009) |
| 9 | Ferula sinkiangensis K.M.Shen. | 阿魏 | Ferulae Resina | Use as an antioxidant with chemo-preventive properties in cancer (Bagheri SM et al., 2016) |
| 10 | Rehmannia glutinosa (Gaertn.) DC. | 熟地黄 | Rehmannia glutinosa Libosch | Anti-inflammatory, anti-microbial, and anti-tumor effects (Bhattamisra SK et al., 2019) |
| 11 | Carthamus tinctorius L. | 红花 | Carthami Flos | Treating blood stasis and activating blood (Guo YF et al., 2014) |
| 12 | Angelica sinensis (Oliv.) Diels. | 当归 | Angelicae Sinensis Radix | Use of treating anemiafor invigorating blood circulation and modulating the balance of the immune system (Liu J et al., 2019) |
| 13 | Anemone raddeana Regel. | 两头尖 | Anemones Raddeanae Rhizoma | Application to conditions such as wind and cold symptoms, hand-foot disease and spasms, and joint pain and ulcer pain (Wang SS et al., 2020) |
| 14 | Cyperus rotundus L. | 香附 | Cyperi Rhizoma | The effect of activating blood circulation and dissipating blood stasis (Liu P et al., 2017) |
| 15 | Curcuma longa L. | 姜黄 | Curcumae Longae Rhizoma | Application to relieving stagnation and stasis, alleviating pain, and curing amenorrhea and wounds (Chen Z et al., 2017) |
| 16 | Rheum palmatum L. | 大黄 | Rhei Radix et Rhizoma | Use of treating liver diseases, constipation and inflammation (Pan TL et al., 2015) |
| 17 | Prunus persica (L.) Batsch | 桃仁 | Persicae Semen | Activating blood, removing stasis and loosing bowels to relieve constipation (Xi S et al., 2013) |
| 18 | Paeonia lactiflora Pall. | 白芍 | Paeoniae Radix Alba | Wide use of treating blood diseases, night sweating, contracture of the limbs, and headache (Tan YQ et al., 2020) |
| 19 | Cinnamomum cassia (L.) J.Presl | 肉桂 | Cinnamomi Cassiae Cortex | Anti-platelet aggregation and antioxidative, anti-diabetic, and anti-fungal activities (Zhou W et al., 2018) |
| 20 | Zanthoxylum bungeanum Maxim. | 花椒 | ZanthoxμLi Pericarpium | Anti-platelet aggregation, anti-inflammatory activity, antioxidant, and anti-cancer activity (Diao WR et al., 2013) |
| 21 | Caesalpinia sappan L. | 苏木 | Sappan Lignum | Promoting blood circulation, removing blood stasis, alleviating pain, and anti-tumor activity (Yang X et al., 2016) |
| 22 | Ligusticum chuanxiong Hort. | 川芎 | Chuanxiong Rhizoma | Anti-thrombotic, anti-inflammatory, anti-cancer, and anti-oxidant effects (Chen Z et al., 2018) |
| 23 | Panax ginseng C.A.Mey. | 人参 | Ginseng Radix et Rhizoma | Application to enhancing body immunity and preventing cancer (Yu S et al., 2020) |
| 24 | Commiphora myrrha (Nees) Engl. | 没药 | Myrrha | Antioxidant and anti-inflammatoryactivity (Ahmad A et al., 2015) |
| 25 | Perilla frutescens (L.) Britton | 紫苏子 | Perillae Fructus | Use of treating respiratory diseases, such as coughing and wheezing (Yim YK et al., 2010) |
| 26 | Syzygium aromaticum (L.) Merr. and L.M.Perry | 丁香 | Caryophylli Flos | Anti-microbial activity (Wong RW et al., 2010) Application to treating backache (Sun M et al., 2019) |
| 27 | Typha angustifolia L. | 蒲黄 | Typhae Pollen | Use of promoting blood circulation and removing stasis (Zeng H et al., 2016) |
| 28 | Euodia ruticarpa (A. Juss.) Benth. | 吴茱萸 | Evodiae Fructus | Analgesic, anti-emetic, anti-inflammatory and antidiarrheal effects (Cai Q et al., 2014) |
| 29 | Artemisia argyi H.Lév. and Vaniot | 艾叶 | Artemisiae Argyi Folium | Antibacterial, antiviral, anti-tumor and anti-inflammatory effects in relieving cough and asthma (Xiao-Yan L et al., 2020) |
Discussion
According to the results of this retrospective study and relevant literature, we made a preliminary hypothesis on the mechanism that HSOS could benefit patients with tumor by improving blood hypercoagulable state and tumor micro-environment of patients. However, there were many different theories about the mechanism of tumor recurrence and metastasis in TCM and Western Medicine. The theory of TCM held that recurrence and metastasis of the tumor were related to “Yuxie” and “Fudu”. The mechanism of the tumor recurrence was closely correlated to the existence of “Yuxie” and the weakness of “Zhengqi”, and the remaining tumor cells after surgery could become “Duxie” hidden in the body, waiting to be induced [15]. Thus, the main manifestation of this situation was recurrence of the tumor, which was difficulty to cure. The “seed and soil” theory held that recurrence and metastasis of the tumor was the result of interaction between tumor cells and their micro-environment [25]. The micro-environment where the tumor located was complicated, which included various types of cells and cytokines [26, 27]. Some of these cytokines could further induce the expression of vascular endothelial growth factor (VEGF), promote tumor angiogenesis, and eventually lead to tumor recurrence and metastasis.
HSOS was an anti-tumor CPM with the effect of “eliminating disease”, “removing blood stasis”, and “strengthening body”. The previous study in vitro has shown that it could inhibit the proliferation of lung cancer cells and reduce the positive expression of CyclinD1 in lung adenocarcinoma cells. Some relevant experiments have also demonstrated that HSOS could improve tumor micro-environment and hypercoagulable state. Liu SQ and Wang W found that the FIB and D-dimer levels of SD rats treated with HSOS decreased significantly after 72 hours [19, 20]. Chen Z showed that the tumor micro-environment was considerably improved with the concentration of FIB, tissue factor, VEGF, and IL-6 decline after administration of HSOS [28]. Besides the effect on lung cancer, HSOS was also demonstrated that it could exert therapeutic effect on other types of tumor, such as ovarian, liver and esophageal cancer. Patients with different types of cancer mentioned above received HSOS combined with convention treatment (such as chemotherapy and radiotherapy) showed better outcomes than those who received convention treatment merely [29]. In this retrospective study, we found that survival benefits were highly associated with medium to long-term (more than 3 months) treatment of CPM/HSOS. The median survival time of patients who received HSOS intervention more than 3 months was longer than that of patients who received HSOS less than 3 months. Patients with elevated preoperative FIB level (more than 4 g/L) and those did not undergo surgery had a higher probability of cancer death, which was consistent with our previous study [30, 31]. Our previous study revealed that more than 3 months treatment of CPM/HSOS could improve 2-year survival rate of patients with stage II–III NSCLC, and preoperative FIB level more than 4 g/L was a risk factor for the prognosis [30]. The results did not change as follow-up time extended from 2 years to 4 years, and the hazard of death for patients with FIB more than 4 g/L was nearly 2 times than those with FIB less than 4 g/L, which to some extent strengthened the reliability of our study. Besides, we conducted further analysis involving patients with FIB ≥4 g/L, which could be regarded as a case that a patient was in hypercoagulable state, to compare outcomes for those who received HSOS more than 3 months and less than 3 months. However, the results showed that the difference of overall 4-year survival rate between FIB ≥4 g/L patients who received HSOS more than 3 months and less than 3 months was not statistically significant (P = 0.29), the median survival was longer for patients in hypercoagulable state and received HSOS more than 3 months compared to the contrast (31 months vs. 19 months), which to some extent demonstrated that HSOS could improve hypercoagulable state to prolong overall survival. There were also several shortcomings in our research: Firstly, this retrospective study was based on medical records from Hospital Information System and telephone visit, therefore, data missing and confounding bias were inevitable. Secondly, owing to the nature of retrospective design, it was difficult for us to verify the actual medical condition of each patient or to figure out the reasons why patients dropout, which might affect the results of the study. Thirdly, since many different types of medicine simultaneously or successively prescribed to the patients in actual treatment process, we could not distinguish the effect of each CPM in the combined treatment, especially in the case of short cumulative treatment duration (less than 3 months, Cumulative treatment duration ≥3 months was set as the effective exposure dose for our survival analysis [14, 15], but only to make a preliminary assessment on its curative effect. The missing value of coagulation indicators after the long-term intervention of HSOS also impeded our exploration on their relationship [32, 33]. Therefore, a prospective clinical research would be anticipated to investigate whether patients could benefit from adequate CPM intervention in the future.
Finally, due to the complex compositions of TCM, it was challenging for the existing science and technology to clarify the mechanism and mutual relationships between different Chinese medicine components. Therefore, it is better to take the TCM formula that has been widely used in clinical practice for verification, and then infer the mechanism after obtaining reliable and scientific data to develop its application in other disease fields instead of analyzing mechanism directly.
Author Contributions
GF and JD contributed the conception and the design of the study. BH searched the database, and set criteria for inclusion and data extraction, and CZ completed the statistical analysis. KJ and FL wrote the first draft of the manuscript and completed the final version. SX wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Conflicts of Interest
Authors Jun Du, Fang Li, and Chenxu Zhang were employed by the company Chengdu Diao Pharmaceutical Group Co., Ltd. The remaining authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical Statement and Consent
The study was reviewed and approved by the Ethics Committee of Sichuan Provincial People’s Hospital (Number: 2019-205). Written informed consent for participation was acquired.
Funding
This study was supported by Science and Technology Department of Sichuan Province, China (Grant Number: 2019ZYZF0114).
References
- 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71:209–49. https://doi.org/10.3322/caac.21660 [PubMed]
- 2. Yu N, Xiong Y, Wang C. Bu-Zhong-Yi-Qi Decoction, the Water Extract of Chinese Traditional Herbal Medicine, Enhances Cisplatin Cytotoxicity in A549/DDP Cells through Induction of Apoptosis and Autophagy. Biomed Res Int. 2017; 2017:3692797. https://doi.org/10.1155/2017/3692797 [PubMed]
- 3. Sugimura H, Nichols FC, Yang P, Allen MS, Cassivi SD, Deschamps C, Williams BA, Pairolero PC. Survival after recurrent nonsmall-cell lung cancer after complete pulmonary resection. Ann Thorac Surg. 2007; 83:409–17. https://doi.org/10.1016/j.athoracsur.2006.08.046 [PubMed]
- 4. Berghmans T, Paesmans M, Sculier JP. Prognostic factors in stage III non-small cell lung cancer: a review of conventional, metabolic and new biological variables. Ther Adv Med Oncol. 2011; 3:127–38. https://doi.org/10.1177/1758834011401951 [PubMed]
- 5. Ohtaki Y, Shimizu K, Kaira K, Nagashima T, Obayashi K, Nakazawa S, Kakegawa S, Igai H, Kamiyoshihara M, Nishiyama M, Takeyoshi I. Risk factors associated with recurrence of surgically resected node-positive non-small cell lung cancer. Surg Today. 2016; 46:1196–208. https://doi.org/10.1007/s00595-015-1301-5 [PubMed]
- 6. Nierodzik ML, Karpatkin S. Thrombin induces tumor growth, metastasis, and angiogenesis: Evidence for a thrombin-regulated dormant tumor phenotype. Cancer Cell. 2006; 10:355–62. https://doi.org/10.1016/j.ccr.2006.10.002 [PubMed]
- 7. Farge D, Durant C, Villiers S, Long A, Mahr A, Marty M, Debourdeau P, and Groupe Francophone Thrombose et Cancer (GFTC). Lessons from French National Guidelines on the treatment of venous thrombosis and central venous catheter thrombosis in cancer patients. Thromb Res. 2010 (Suppl 2); 125:S108–16. https://doi.org/10.1016/S0049-3848(10)70027-X [PubMed]
- 8. Choi PJ, Jeong SS, Yoon SS. Prediction and prognostic factors of post-recurrence survival in recurred patients with early-stage NSCLC who underwent complete resection. J Thorac Dis. 2016; 8:152–60. https://doi.org/10.3978/j.issn.2072-1439.2016.01.10 [PubMed]
- 9. Lin Y, Liu Z, Qiu Y, Zhang J, Wu H, Liang R, Chen G, Qin G, Li Y, Zou D. Clinical significance of plasma D-dimer and fibrinogen in digestive cancer: A systematic review and meta-analysis. Eur J Surg Oncol. 2018; 44:1494–503. https://doi.org/10.1016/j.ejso.2018.07.052 [PubMed]
- 10. Hou C, Jiang F, Ma H, Zhu Q, Wang Z, Zhao B, Xue T, Tan S, Yang R, Qian Y, Luo X, Zhao M, Xu X, et al. Prognostic role of preoperative platelet, fibrinogen, and D-dimer levels in patients with non-small cell lung cancer: A multicenter prospective study. Thorac Cancer. 2019; 10:304–11. https://doi.org/10.1111/1759-7714.12956 [PubMed]
- 11. Wang S, Long S, Wu W. Application of Traditional Chinese Medicines as Personalized Therapy in Human Cancers. Am J Chin Med. 2018; 46:953–70. https://doi.org/10.1142/S0192415X18500507 [PubMed]
- 12. Han Y, Wang H, Xu W, Cao B, Han L, Jia L, Xu Y, Zhang Q, Wang X, Zhang G, Yu M, Yang G. Chinese herbal medicine as maintenance therapy for improving the quality of life for advanced non-small cell lung cancer patients. Complement Ther Med. 2016; 24:81–9. https://doi.org/10.1016/j.ctim.2015.12.008 [PubMed]
- 13. Wang XM, Yu RC, Wang YT. [Study on advanced non-small cell lung cancer patients with Qi deficiency and blood stasis syndrome]. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1994; 14:724–6. [PubMed]
- 14. Xu Y, Mao JJ, Sun L, Yang L, Li J, Hao Y, Li H, Hou W, Chu Y, Bai Y, Jia X, Wang J, Shen L, et al. Association Between Use of Traditional Chinese Medicine Herbal Therapy and Survival Outcomes in Patients With Stage II and III Colorectal Cancer: A Multicenter Prospective Cohort Study. J Natl Cancer Inst Monogr. 2017; 2017:lgx015. https://doi.org/10.1093/jncimonographs/lgx015 [PubMed]
- 15. Wang XQ, Zhang Y, Hou W, Wang YT, Zheng JB, Li J, Lin LZ, Jiang YL, Wang SY, Xie Y, Zhang HL, Shu QJ, Li P, et al. Association between Chinese Medicine Therapy and Survival Outcomes in Postoperative Patients with NSCLC: A Multicenter, Prospective, Cohort Study. Chin J Integr Med. 2019; 25:812–9. https://doi.org/10.1007/s11655-019-3168-6 [PubMed]
- 16. Guo YF, Shen D, Yang HJ. [Analysis on composition regularity of carthami flos-containing traditional Chinese medicines]. Zhongguo Zhong Yao Za Zhi. 2014; 39:2144–8. [PubMed]
- 17. Yu S, Wang S, Huang S, Wang W, Wei Z, Ding Y, Wang A, Huang S, Chen W, Lu Y. Radix et Rhizoma Ginseng chemoprevents both initiation and promotion of cutaneous carcinoma by enhancing cell-mediated immunity and maintaining redox homeostasis. J Ginseng Res. 2020; 44:580–92. https://doi.org/10.1016/j.jgr.2019.05.004 [PubMed]
- 18. Chen Z, Zhang C, Gao F, Fu Q, Fu C, He Y, Zhang J. A systematic review on the rhizome of Ligusticum chuanxiong Hort. (Chuanxiong). Food Chem Toxicol. 2018; 119:309–25. https://doi.org/10.1016/j.fct.2018.02.050 [PubMed]
- 19. Wang W, Wang H, Wang CM, Gou S, Chen ZH, Guo J. Treatment with Huisheng oral solution inhibits the development of pulmonary thromboembolism and metastasis in mice with Lewis lung carcinoma. Oncol Lett. 2014; 7:87–94. https://doi.org/10.3892/ol.2013.1661 [PubMed]
- 20. Liu SQ, Guo JY, Du J, Deng Q, He ZJ, Lin HY, Lei SH. Anticoagulant effect of Huisheng Oral Solution in a rat model of thrombosis. Indian J Pharmacol. 2013; 45:359–64. https://doi.org/10.4103/0253-7613.115018 [PubMed]
- 21. Chen Z, Sun D, Bi X, Zeng X, Luo W, Cai D, Zeng Q, Xu A. Pharmacokinetic based study on "lagged stimulation" of Curcumae Longae Rhizoma - Piper nigrum couplet in their main active components' metabolism using UPLC-MS-MS. Phytomedicine. 2017; 27:15–22. https://doi.org/10.1016/j.phymed.2017.01.012 [PubMed]
- 22. Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman J, Chirieac LR, D'Amico TA, DeCamp MM, Dilling TJ, Dobelbower M, Doebele RC, Govindan R, Gubens MA, et al. Non-Small Cell Lung Cancer, Version 5.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017; 15:504–35. https://doi.org/10.6004/jnccn.2017.0050 [PubMed]
- 23. Ahmad A, Raish M, Ganaie MA, Ahmad SR, Mohsin K, Al-Jenoobi FI, Al-Mohizea AM, Alkharfy KM. Hepatoprotective effect of Commiphora myrrha against d-GalN/LPS-induced hepatic injury in a rat model through attenuation of pro inflammatory cytokines and related genes. Pharm Biol. 2015; 53:1759–67. https://doi.org/10.3109/13880209.2015.1005754 [PubMed]
- 24. Lee JH, Lee DU, Kim YS, Kim HP. 5-Lipoxygenase Inhibition of the Fructus of Foeniculum vulgare and Its Constituents. Biomol Ther (Seoul). 2012; 20:113–7. https://doi.org/10.4062/biomolther.2012.20.1.113 [PubMed]
- 25. Fidler IJ, Poste G. The "seed and soil" hypothesis revisited. Lancet Oncol. 2008; 9:808. https://doi.org/10.1016/S1470-2045(08)70201-8 [PubMed]
- 26. Cedervall J, Hamidi A, Olsson AK. Platelets, NETs and cancer. Thromb Res. 2018 (Suppl 1); 164:S148–52. https://doi.org/10.1016/j.thromres.2018.01.049 [PubMed]
- 27. Wu T, Dai Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017; 387:61–8. https://doi.org/10.1016/j.canlet.2016.01.043 [PubMed]
- 28. Chen Z, Liu M, Xie K, Chen H, Wang J, Liu X. Huisheng Oral Solution exerts anti-tumor effects by downregulating tissue factor and inhibiting the expression of metastasis-related factors, CD44, MMP2, and VEGF. Transl Cancer Res. 2019; 8:2602–12. https://doi.org/10.21037/tcr.2019.10.25 [PubMed]
- 29. Chen J. Huisheng oral liquid combined with TACE for treatment of primary hepatic carcinoma: Meta-analysis. Chin J Interv Imaging Ther. 2019; 12:545–9.
- 30. Wang L, Jia K, Li F, Zhang C, Feng G, Du J. Comparison of Improvement in 2-Year Survival Rate of Patients with Stage II-III Non-Small Cell Lung Cancer Treated with Different Durations of Chinese Patent Medicine: A Retrospective Cohort Study. Front Pharmacol. 2021; 12:719802. https://doi.org/10.3389/fphar.2021.719802 [PubMed]
- 31. Yang X, Zhang H, Kong F, Wang G, Gu Q, Zhao Z, Li T, Ren M, Li Z, Guo Y. Effect of Huisheng oral solution on coagulation function in perioperative period in patients with primary lung cancer. J Thorac Dis. 2017; 9:1891–902. https://doi.org/10.21037/jtd.2017.06.64 [PubMed]
- 32. Choi OB, Park JH, Lee YJ, Lee CK, Won KJ, Kim J, Lee HM, Kim B. Olibanum extract inhibits vascular smooth muscle cell migration and proliferation in response to platelet-derived growth factor. Korean J Physiol Pharmacol. 2009; 13:107–13. https://doi.org/10.4196/kjpp.2009.13.2.107 [PubMed]
- 33. Jia J, Li X, Ren X, Liu X, Wang Y, Dong Y, Wang X, Sun S, Xu X, Li X, Song R, Ma J, Yu A, et al. Sparganii Rhizoma: A review of traditional clinical application, processing, phytochemistry, pharmacology, and toxicity. J Ethnopharmacol. 2021; 268:113571. https://doi.org/10.1016/j.jep.2020.113571 [PubMed]