



Introduction
Over the past decade, lung cancer has emerged as the predominant form of cancer detected globally and the primary reason for mortality. According to current statistics, there are approximately 20,000 lung cancer cases per year, with mortality of 17,600 cases annually [1, 2]. Non-small-cell lung cancer (NSCLC) represents approximately 85% of all lung cancer cases [2]. In NSCLC, lung adenocarcinoma (LUAD) and lung squamous cell carcinoma (LUSC) are the most common subtypes [3]. However, over the last 20–30 years, LUAD has replaced LUSC as the most common histological type [4]. Additionally, lymph node metastasis is more common in LUAD than LUSC [5]. Therefore, more advanced research is required to develop effective treatment strategies, including early diagnosis and treatment with reliable targets.
Secreted phosphoprotein 1 (SPP1), which encodes osteopontin (OPN), was initially named due to its discovery in bone tissue. OPN is widely expressed in various tissues and cell types [6], including bone, kidney, and lung [7]. It plays crucial functional and regulatory roles under physiological and pathological conditions [8, 9]. The SPP1 family exhibits specific binding capabilities and activates matrix metalloproteinases (MMPs) which are notable regulatory factors in tumors [10]. The secretion of this highly acidic phosphoprotein serves various purposes, such as promoting bone regeneration, facilitating angiogenesis, aiding in cell adhesion and migration, and contributing to inflammation [11]. In prostate [12], cervical [13, 14], breast [15], liver [16], and other cancers, SPP1 is substantially expressed and correlated with clinical stage and prognosis [17]. However, the utilization of SPP1 as a standalone prognostic indicator in LUAD remains unclear. Therefore, in this study, we aimed to investigate whether SPP1 has prognostic significance in this disease.
Given the identified role of SPP1 in other cancers and its demonstrated status as a biomarker for prognosis, this study sought to examine the expression of SPP1 in LUAD, determine its relationship with clinical manifestations and prognosis, and provide a novel reference for the diagnosis and prognosis of LUAD combining bioinformatics and molecular biology.
Results
Selection of DEGs associated with immune prognosis in NSCLC
In total, 5291 DEGs were identified, of which 241 were identified as being immune- or prognosis-related based on the ImmPort and TCGA database (Figure 1A). Out of the total, 47 genes were found to have a strong correlation with immune responses and prognosis, as determined by their |log2fc| (Supplementary Table 1), including SPP1 (p=0.037). Due to its involvement in diverse biological processes, SPP1 has been recognized as a significant contributor to numerous cancer types [18]. Consequently, SPP1 has been chosen for further comprehensive examination.
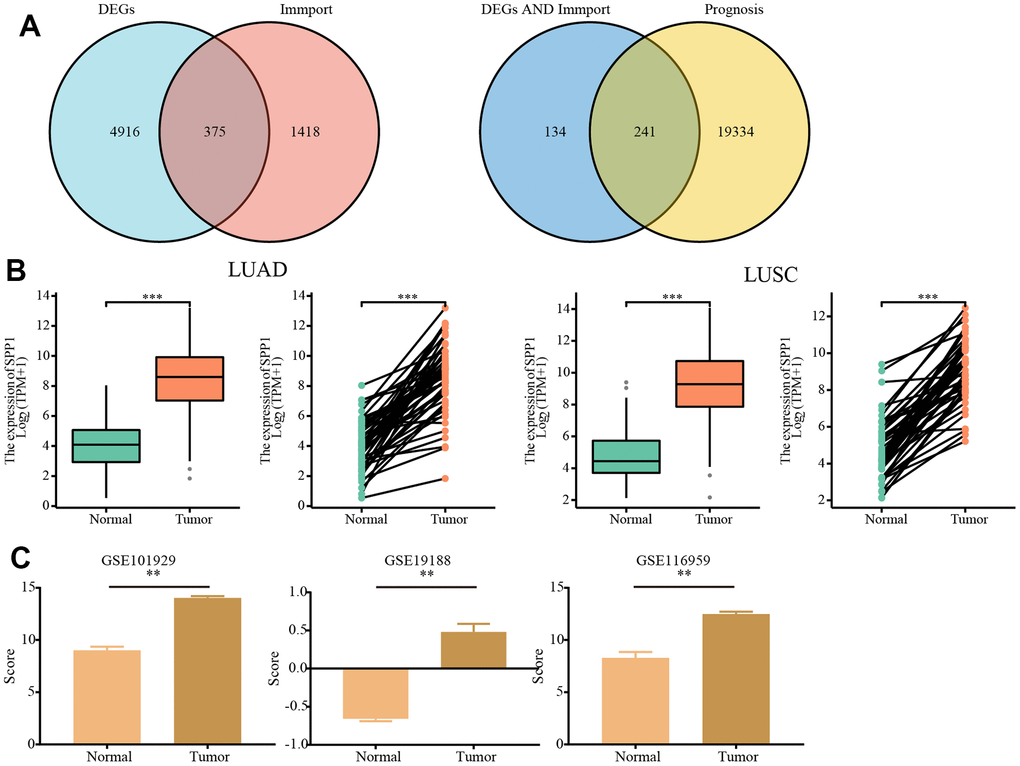
Figure 1. Analysis of the expression of SPP1 based on TCGA and GEO databases. (A) A Venn diagram of 241 immune- and prognosis-related differentially expressed genes. (B) According to the TCGA database differential expression of SPP1 in LUAD and LUSC versus normal tissues. (C) Differential expression of SPP1 based on GEO database GSE101929 (Normal=34, Tumor=32), GSE19188 (Normal=65, Tumor=91) and GSE116959 (Normal=11, Tumor=57). **p<0.01, ***p<0.001.
Unregulated expression of SPP1 in NSCLC
To clarify the expression pattern of SPP1 in NSCLC, the transcriptomic data from TCGA was examined to analyze the expression of SPP1 in normal, LUAD, and LUSC tissues. Figure 1B demonstrated a notable up-regulation of SPP1 in LUAD and LUSC tissues when compared with normal tissues (all p < 0.001). A similar analysis was conducted on the GSE101929, GSE19188, and GSE116959 datasets. The analysis of SPP1 expression in NSCLC, in comparison to normal tissues, also revealed a significant over-expression of SPP1 (all p < 0.01; Figure 1C). Hence, it could be concluded that SPP1 exhibited elevated levels of expression in NSCLC.
Clinicopathological features of SPP1 in NSCLC
The link between elevated SPP1 expression and NSCLC led to the use of KW analysis to investigate SPP1-related clinicopathological features in LUAD and LUSC. In Figure 2A, a strong association was found between SPP1 and the N stage of LUAD (p < 0.001), whereas no notable correlation was detected with other clinicopathological characteristics. Conversely, Figure 2B indicated no correlation between SPP1 and the clinicopathological features of LUSC.
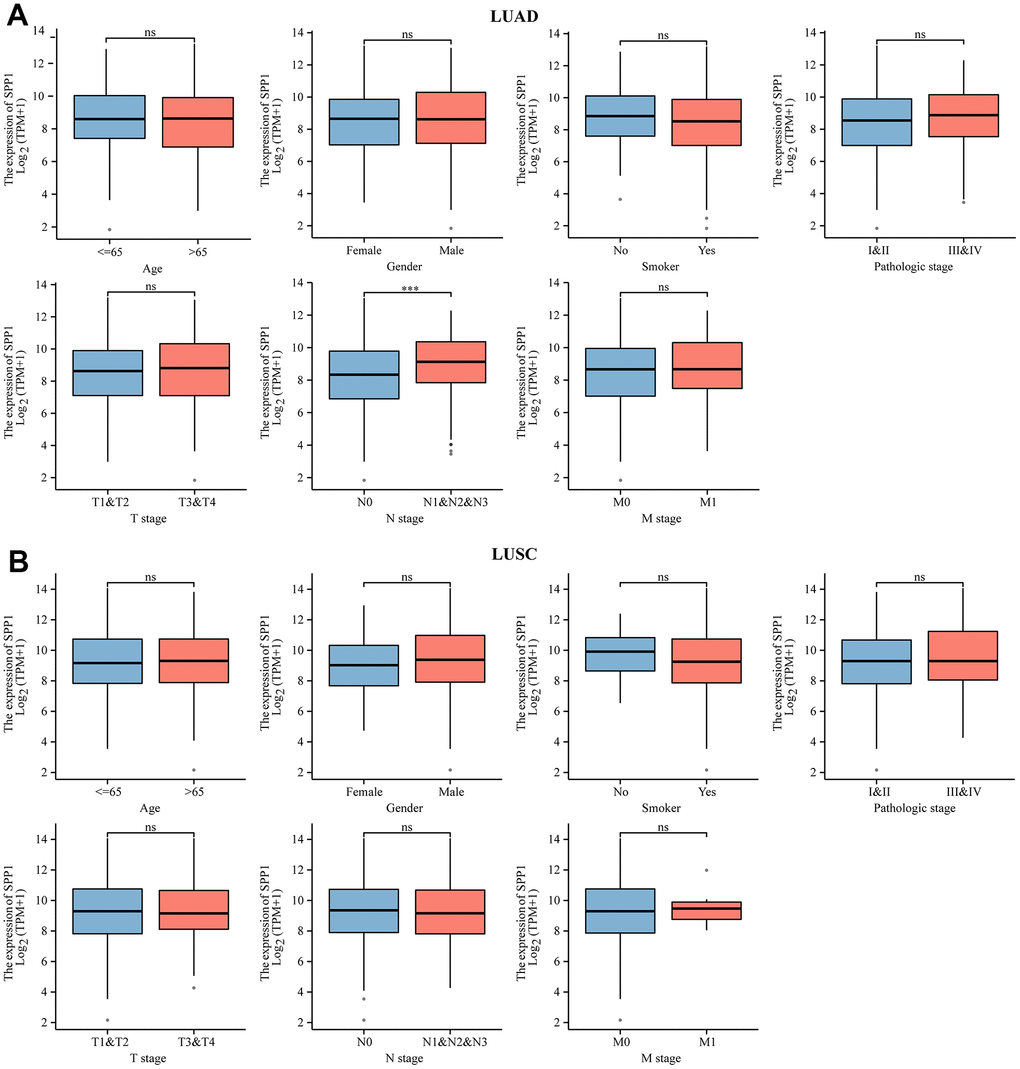
Figure 2. Association between clinical-pathological characteristics and SPP1 mRNA levels in NSCLC. Comparative analysis of SPP1 expression level of clinical-pathological characteristics in (A) LUAD and (B) LUSC. ns: no statistical significance, ***p<0.001.
Effect of SPP1 expression levels on prognosis in NSCLC
To examine the influence of SPP1 expression on the outlook of NSCLC, survival analysis curves were utilized to assess the overall survival (OS), disease-specific survival (DSS), and progression-free interval (PFI) of individuals diagnosed with LUAD and LUSC. Figure 3A illustrated that the OS of patients with LUAD was diminished in the presence of high expression of SPP1 (HR 1.37 (1.02–1.82), p=0.034). However, the association between SPP1 expression levels and DSS (HR 1.36 (0.94–1.96), p=0.104) and PFI (HR 1.22 (0.94–1.59), p=0.133) in patients with LUAD did not reach statistical significance. According to Figure 3B, there were no notable variances observed in the OS (HR 1.23 (0.94–1.61), p=0.133), DSS (HR 1.00 (0.66–1.53), p=0.995), or PFI (HR 1.07 (0.78–1.48), p=0.674) among LUSC individuals with elevated and reduced SPP1 levels. Consequently, it could be concluded that elevated SPP1 expression impacted the OS of patients with LUAD adversely, whereas the impact on the survival of patients with LUSC did not show statistical significance.
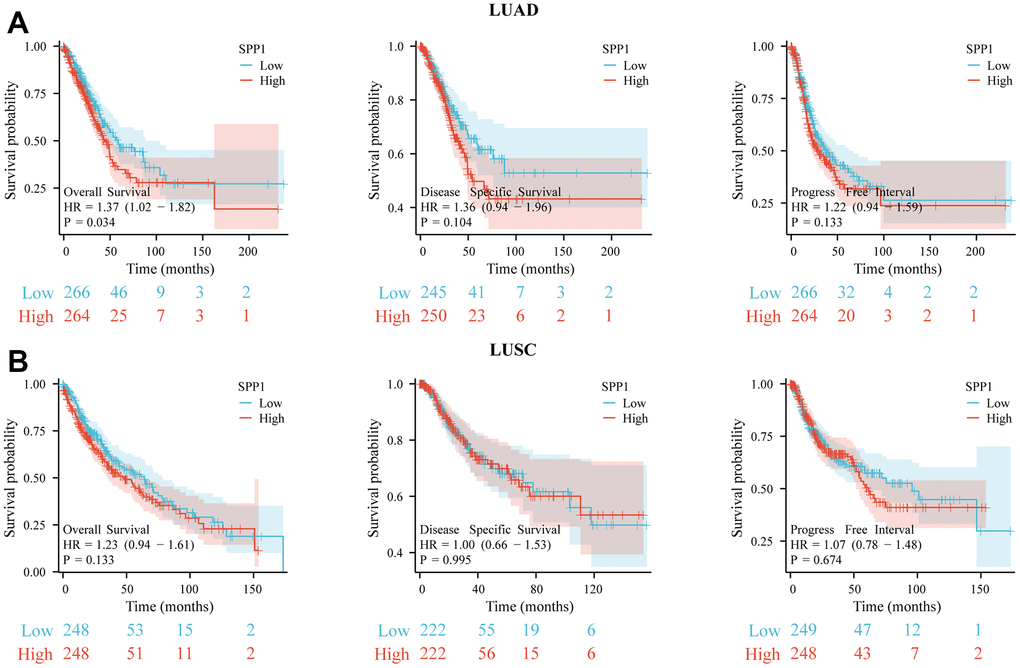
Figure 3. Survival analysis for different expression of SPP1. The prognostic impact of SPP1 on OS, DSS, and PFI in (A) LUAD and (B) LUSC. All gene sets were significantly enriched at nominal p-value <0.05.
Relationships between SPP1 expression and clinicopathological features of LUAD
As stated above, separate research on LUAD was initiated since the correlation of SPP1 with LUSC was not significant. Considering the clinical importance of SPP1 in LUAD, an examination of the detailed clinical attributes of patients with LUAD was initiated. Table 1 displayed a summary of clinicopathological features of 535 patients, encompassing age, gender, smoking habits, Tumor Node Metastasis (TNM) stage, pathological stage, tumor location, and primary effectiveness. Based on chi-square tests, SPP1 showed a significant correlation with N stage (p=0.002) and primary efficacy assessment (p=0.025), while no significant correlation was found with other clinicopathological factors. This suggested that SPP1 expression varied among the different LUAD N stages (N0, N1, N2 and N3). Patients with different efficacy evaluation outcomes also showed significantly different SPP1 expression levels.
Table 1. Relationship between SPP1 expression and clinicopathological features of LUAD in TCGA.
| Characteristics | Low SPP1 | High SPP1 | p-value |
| No. (%) | No. (%) | ||
| Age, n (%) | 0.791 | ||
| <=65 | 130 (25.2%) | 125 (24.2%) | |
| >65 | 129 (25%) | 132 (25.6%) | |
| Gender, n (%) | 0.968 | ||
| Female | 142 (26.5%) | 144 (26.9%) | |
| Male | 125 (23.4%) | 124 (23.2%) | |
| Smoker, n (%) | 0.159 | ||
| No | 31 (6%) | 44 (8.4%) | |
| Yes | 227 (43.6%) | 219 (42%) | |
| T stage, n (%) | 0.220 | ||
| T1 | 98 (18.4%) | 77 (14.5%) | |
| T2 | 133 (25%) | 156 (29.3%) | |
| T3 | 24 (4.5%) | 25 (4.7%) | |
| T4 | 10 (1.9%) | 9 (1.7%) | |
| N stage, n (%) | 0.002 | ||
| N0 | 192 (37%) | 156 (30.1%) | |
| N1 | 36 (6.9%) | 59 (11.4%) | |
| N2 | 30 (5.8%) | 44 (8.5%) | |
| N3 | 0 (0%) | 2 (0.4%) | |
| M stage, n (%) | 1.000 | ||
| M0 | 176 (45.6%) | 185 (47.9%) | |
| M1 | 12 (3.1%) | 13 (3.4%) | |
| Pathologic stage, n (%) | 0.200 | ||
| Stage I | 158 (30%) | 136 (25.8%) | |
| Stage II | 57 (10.8%) | 66 (12.5%) | |
| Stage III | 35 (6.6%) | 49 (9.3%) | |
| Stage IV | 13 (2.5%) | 13 (2.5%) | |
| Anatomic neoplasm subdivision, n (%) | 0.350 | ||
| Left | 96 (18.5%) | 109 (21%) | |
| Right | 162 (31.2%) | 153 (29.4%) | |
| Primary therapy outcome, n (%) | 0.025 | ||
| PD | 28 (6.3%) | 43 (9.6%) | |
| SD | 24 (5.4%) | 13 (2.9%) | |
| PR | 5 (1.1%) | 1 (0.2%) | |
| CR | 173 (38.8%) | 159 (35.7%) |
Association between SPP1 expression and clinical prognosis in LUAD
The KM approach was utilized to examine the association between different clinicopathological characteristics and SPP1 mRNA levels in LUAD, thereby evaluating its clinical prognostic significance. In elderly male patients aged 65 and above, as well as those with T stage T3, the research uncovered a noteworthy correlation between the expression of SPP1 mRNA and the clinical prognosis (Table 2). This finding indicated that T staging, specifically T stage T3, was affected by clinical factors, such as SPP1 mRNA expression, leading to variations in survival time among patients with LUAD and ultimately impacting clinical outcomes. Therefore, the objective was to investigate the prognostic impact of SPP1 on LUAD in more detail.
Table 2. Correlation of SPP1 expression and clinical prognosis in LUAD with different clinicopathological factors by KM.
| Clinicopathological characteristics | No. | Hazard ratio | p-value | |
| Age | ||||
| ≤65 | 255 | 1.18(0.77-1.81) | 0.437 | |
| >65 | 261 | 1.54(1.03-2.30) | 0.036 | |
| Gender | ||||
| Female | 286 | 1.62(1.08-2.42) | 0.02 | |
| Male | 249 | 1.12(0.74-1.69) | 0.601 | |
| Smoke | ||||
| No | 75 | 1.09 (0.49-2.40) | 0.834 | |
| Yes | 446 | 1.28 (0.93-1.77) | 0.127 | |
| T stage | ||||
| T1 | 175 | 1.32 (0.72-2.42) | 0.366 | |
| T2 | 289 | 0.97 (0.67-1.42) | 0.89 | |
| T3 | 49 | 2.61 (1.01-6.71) | 0.047 | |
| T4 | 19 | 1.45 (0.46-4.61) | 0.528 | |
| N stage | ||||
| N0 | 348 | 1.03(0.68-1.56) | 0.878 | |
| N1 | 95 | 0.71 (0.41-1.22) | 0.212 | |
| N2 | 74 | 1.78(0.95-3.34) | 0.073 | |
| N3 | 2 | --- | --- | |
| M stage | ||||
| M0 | 361 | 1.13 (0.81-1.59) | 0.472 | |
| M1 | 25 | 2.89 (0.90-9.32 | 0.076 | |
| Stage | ||||
| I | 294 | 1.00(0.63-1.61) | 0.992 | |
| II | 123 | 0.86(0.50-1.48) | 0.586 | |
| III | 84 | 1.78(0.99-3.22) | 0.054 | |
| IV | 26 | 2.48(0.84-7.36) | 0.102 | |
Prognostic analysis of LUAD clinical subgroups
Further analysis was conducted to examine the correlation between the OS of LUAD and SPP1 among different clinicopathological subgroups. Subgroup analysis showed that the higher expression of SPP1 in pathological stage III (HR 1.83 (1.02–3.30), p=0.044) and T stage T3 (HR 2.61 (1.01–6.71), p=0.047) patients was statistically correlated with worse OS, as shown in Figure 4A. Using the ROC curves analysis, the predictive accuracy of SPP1 for LUAD was evaluated in terms of 1-, 3-, and 5-year OS (Figure 4B). Area Under the Curve (AUC) > 0.5 suggested that SPP1 served as a reliable prognostic indicator for LUAD patients, predicting outcomes at 1-, 3-, and 5-year intervals. The AUC under the ROC curves were 0.542, 0.534, and 0.578 in several. The findings demonstrated that SPP1 exhibited slightly superior predictive capability for 1-, 3-, and 5-year survival compared to random prediction, thereby validating the accuracy of the diagnostic prediction. Therefore, the over-expression of SPP1 was considered a risk factor for worse prognosis.
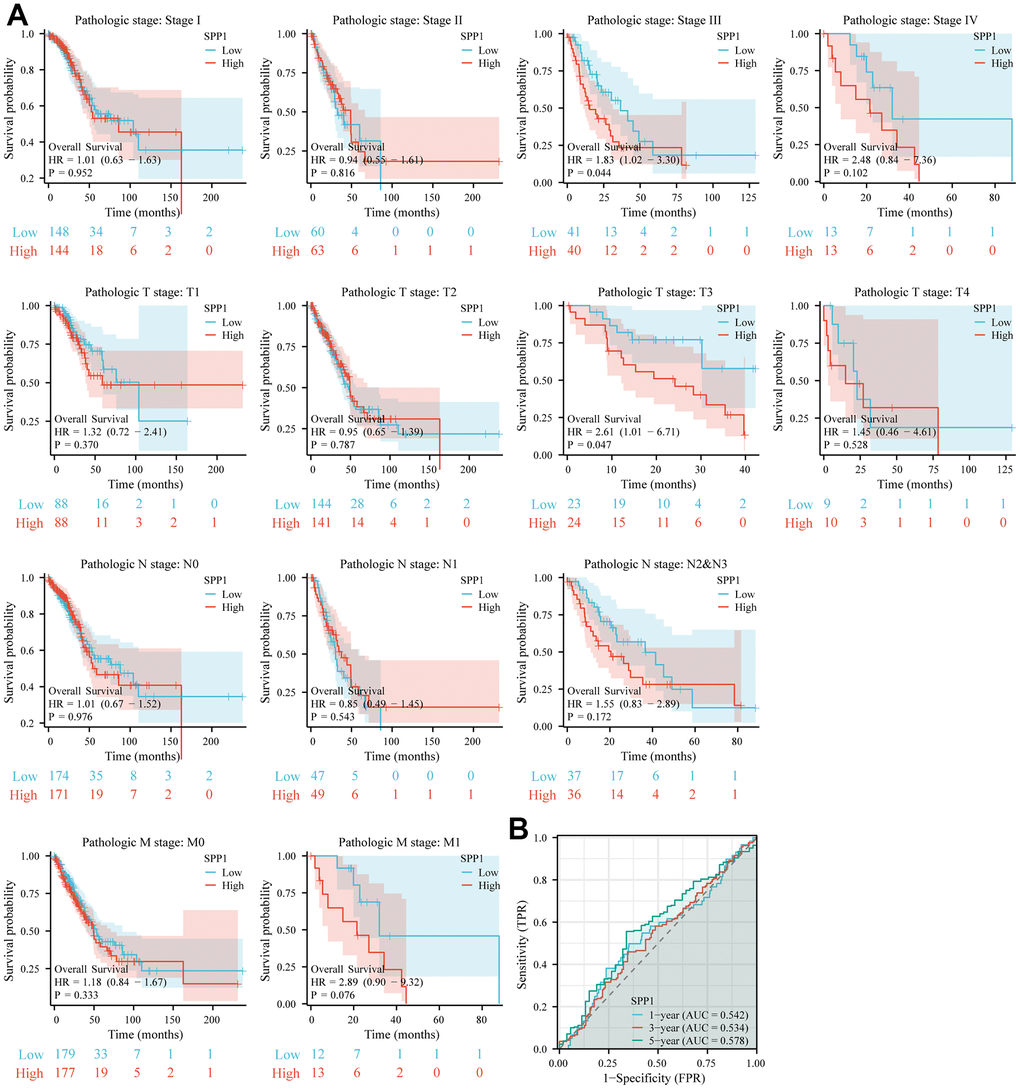
Figure 4. The predictive significance of SPP1 in various subcategories. (A) Significant association between elevated SPP1 expression and unfavorable overall survival was observed among different subgroups. (B) ROC curve of SPP1 expression at 1-, 3- and 5-year OS.
Connection between SPP1 expression and OS among LUAD patients by univariate and multivariate methods
Further analysis was prompted by the significant correlation between SPP1 and OS in LUAD patients, leading to the need for univariate and multivariate analysis. Through the analysis presented in Table 3, significant associations were observed between SPP1 and various stages of LUAD. During the univariate analysis, SPP1 showed connections with T3 and T4, N1, N2, and N3, M1, pathological III and IV stages, and high levels of SPP1 expression. Univariate analysis revealed a significant association between the individual predictors and the survival times of patients with LUAD. After accounting for the interplay between multiple predictors and survival times, the multivariate analysis indicated that the T3 and T4 stages and the N1, N2, and N3 stages were correlated with patient OS. The findings of this study highlight the possibility of enhancing precision and inclusiveness in prognostic prediction. Notably, clinicopathological stage and a high SPP1 expression level emerged as significant survival indicators and, following a comprehensive analysis of multiple factors, the latter portion of clinicopathological stage was identified as an independent prognostic factor for OS. The results provided a more accurate and thorough forecast, and comprehension of SPP1 as a standalone predictive element.
Table 3. Univariate and multivariate analysis of the correlation of SPP1 expression with OS among LUAD patients.
| Parameter | Total (No.) | Univariate analysis | Multivariate analysis | ||
| Hazard ratio (95% CI) | p-value | Hazard ratio (95% CI) | p-value | ||
| Age | |||||
| <=65 | 255 | ||||
| >65 | 261 | 1.223 (0.916-1.635) | 0.172 | 1.298 (0.911-1.849) | 0.149 |
| Gender | |||||
| Female | 280 | ||||
| Male | 246 | 1.070 (0.803-1.426) | 0.642 | 0.988 (0.693-1.408) | 0.946 |
| T stage | |||||
| T1&T2 | 457 | ||||
| T3&T4 | 66 | 2.317 (1.591-3.375) | <0.001 | 1.922 (1.197-3.089) | 0.007 |
| N stage | |||||
| N0 | 343 | ||||
| N1&N2&N3 | 167 | 2.601 (1.944-3.480) | <0.001 | 2.055 (1.353-3.120) | <0.001 |
| M stage | |||||
| M0 | 352 | ||||
| M1 | 25 | 2.136 (1.248-3.653) | 0.006 | 1.300 (0.671-2.520) | 0.437 |
| Pathologic stage | |||||
| I&II | 411 | ||||
| III&IV | 107 | 2.664 (1.960-3.621) | <0.001 | 1.380 (0.826-2.304) | 0.218 |
| Smoker | |||||
| No | 72 | ||||
| Yes | 440 | 0.894 (0.592-1.348) | 0.591 | 0.977 (0.584-1.636) | 0.930 |
| SPP1 | |||||
| Low | 264 | ||||
| High | 262 | 1.360 (1.019-1.814) | 0.037 | 1.213 (0.851-1.730) | 0.286 |
Roles of SPP1 in LUAD
To enhance comprehension of SPP1 manifestation and its fundamental mechanism in LUAD, single-cell analysis was conducted based on the CanerSEA database. The results indicated a negative correlation between SPP1 and various cellular processes, including cell metastasis, epithelial-mesenchymal transition, angiogenesis, DNA damage, cell quiescence, cancer cell invasion, and cell differentiation (Figure 5A). Analysis of the entire heatmap enabled the identification of distinct activity patterns exhibited by different cells or cell groups in diverse functional states (Figure 5B). This comprehensive understanding aided in discerning disparities in functional states within cells, the level of activation of specific genes or pathways, and the heterogeneity among cell groups. A metastatic analysis based on the EMTome database revealed an association between SPP1 and metastasis (Figure 5C). An analysis of GSEA on high SPP1 groups was conducted to identify SPP1-associated signaling pathways. By the HALLMARK pathway enrichment analysis, the highly expressed SPP1 phenotype was substantially enriched in 34 critical signaling pathways, one of which is EMT (Figure 5D). These results would help further explore the pathophysiological mechanisms of SPP1.
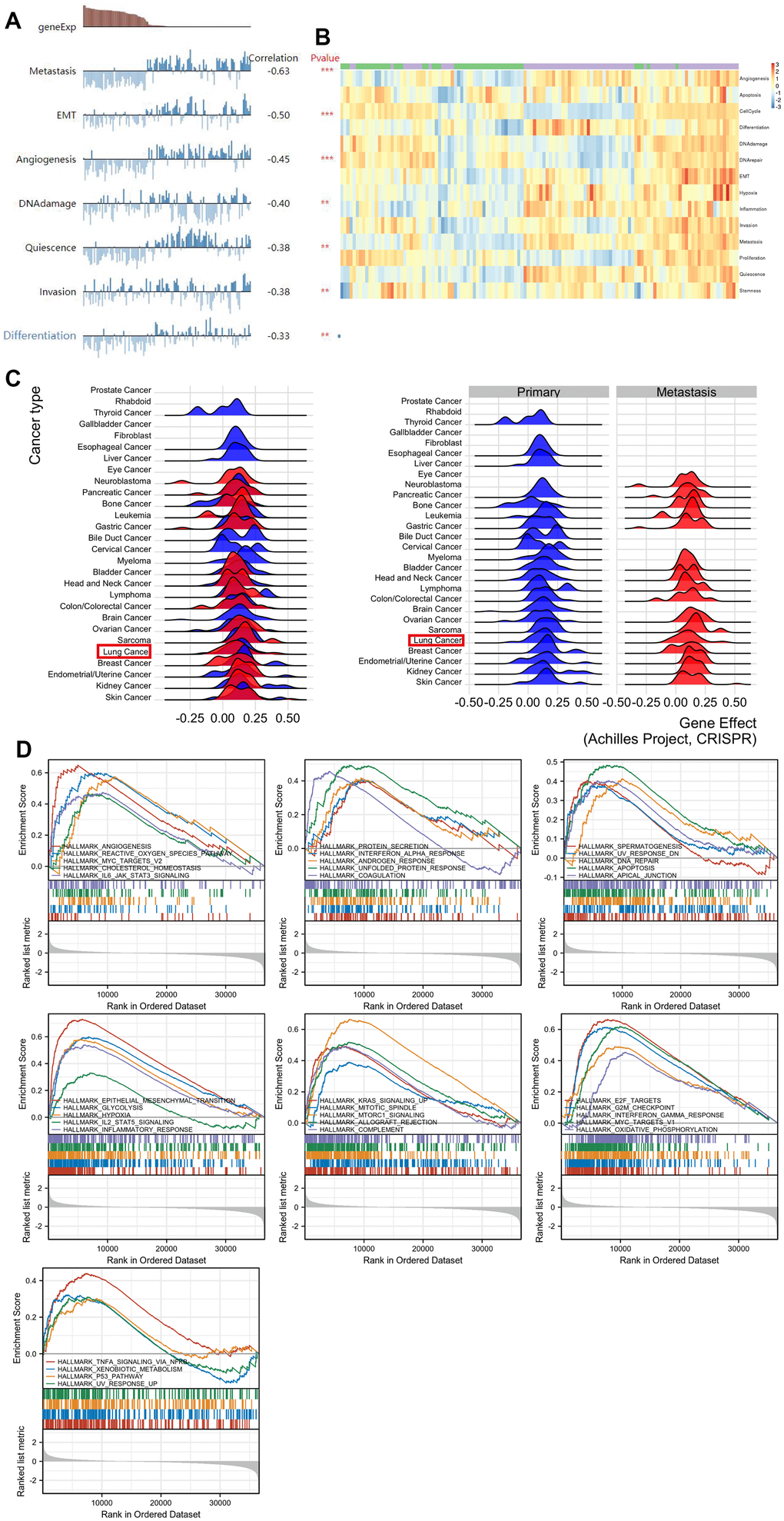
Figure 5. Comprehensive analysis of the functional role of SPP1 in LUAD. (A) Analysis of individual cells revealed multiple influence of SPP1, including cell metastasis, epithelial-to-mesenchymal transition, angiogenesis, DNA damage, cell dormancy, cancer cell invasion, and cellular differentiation. (B) Functional status profile showcasing the diverse activity of function states of LUAD cells. (C) Metastasis of lung cancer associated with SPP1 expression. (D) HALLMARK term analysis revealed in 34 positively correlated groups. **p<0.01, ***p<0.001.
Effect of SPP1 on epithelial-mesenchymal transition (EMT) in LUAD
EMT is a crucial cellular process that was connected to SPP1 in the above-mentioned study [19, 20]. To gain further insights into the mechanistic actions of SPP1, an analysis was conducted on the effects of SPP1 as a marker on EMT (Figure 6). The activation of EMT, where epithelial cells experienced a transition and acquired mesenchymal properties, hence enhancing their motility and migratory potential, emerged as a crucial mechanism in the spread of cancer cells. Notably, Figure 6 demonstrated a correlation between the upregulation of SPP1 expression and the heightened expression of mesenchymal cell markers (N-cadherin, vimentin). At the same time, a number of transcription factor families, including SNAI1, SLUG, TWIST1, TWIST2, ZEB1, and ZEB2, controlled how the EMT process was modulated. Additionally, proteolytic digestion was made easier by the overexpression of matrix metalloproteinases (MMP2 and MMP9). The expression of MMP was regulated by the EMT-related signal transduction pathway (TGF-β). Collectively, these results implied that SPP1 may be involved in EMT pathways that were critical for the development of LUAD.
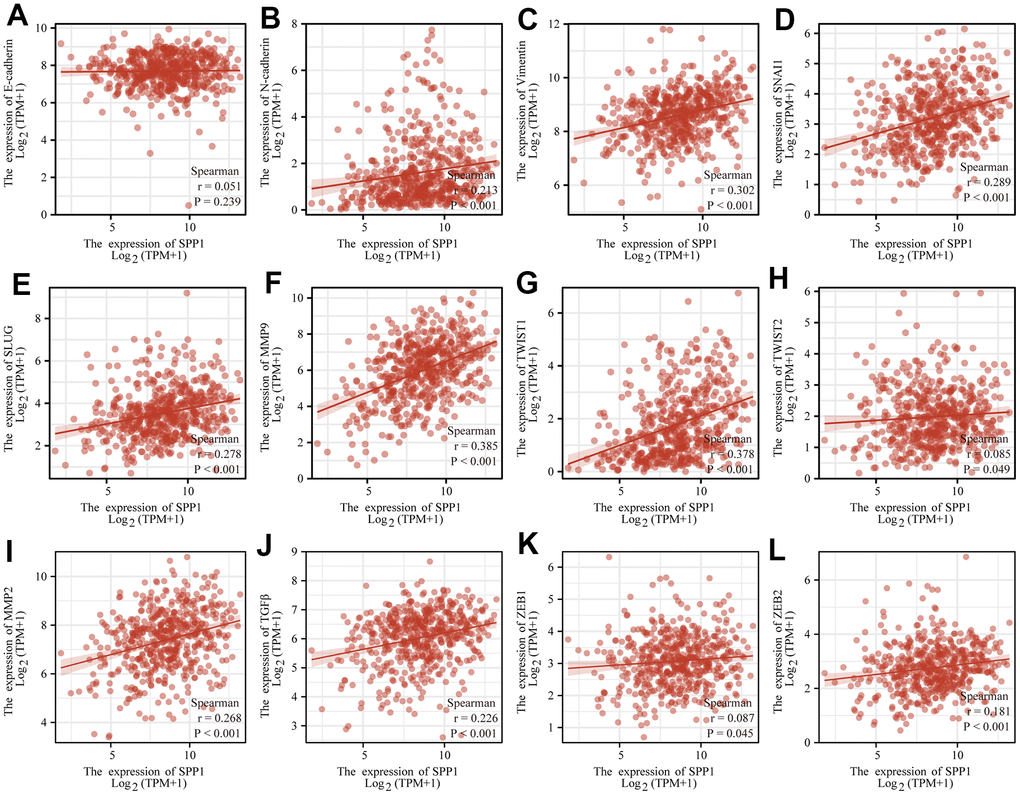
Figure 6. SPP1 expression correlated with EMT signatures in LUAD. SPP1 expression connected with (A) E-cadherin, (B) N-cadherin, (C) Vimentin, (D) SNAI1, (E) SLUG, (F) MMP9, (G) TWIST1, (H) TWIST2, (I) MMP2, (J) TGFβ, (K) ZEB1, and (L) ZEB2.
Detection of SPP1 infiltrating immune cells correlates with its expression
It is widely recognized that the immune system is crucial in the fight against cancer [21]. The role of SPP1 was investigated in the tumor microenvironment (TME) of LUAD by the EMTome database and CIBERSORT algorithm to analyze TCGA data and determine the landscape of immune cell infiltration in LUAD (Figure 7A, 7B). Subsequently, the specimens were categorized into two cohorts according to SPP1 manifestation, and the analysis of immune cells distribution between these cohorts was conducted. In Figure 7C, which represented the high SPP1 groups, a significant increase in the density of various immune cells was observed included M0, M1, and M2 macrophages, as well as resting memory CD4+ T cells and regulatory T cells (Tregs). The heat map analysis revealed a connection between 21 immune-infiltrating cells and tumor samples in the TCGA cohort, as indicated by the correlation observed (Figure 7D).
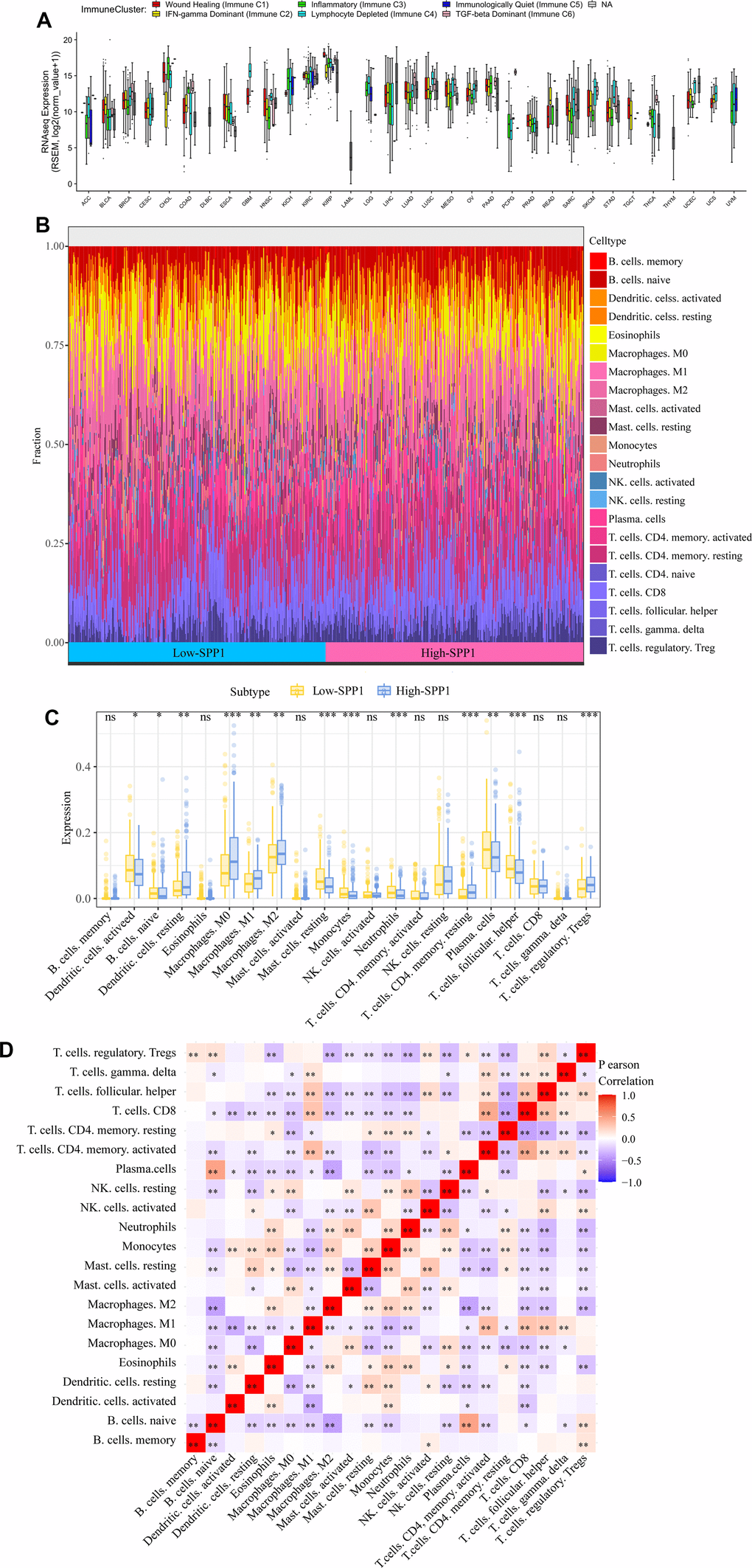
Figure 7. Impact of SPP1 on immune cell infiltration and distribution in LUAD. (A) Distinct immune clusters observed in different cancer types. (B) Immune landscape data of LUAD from different expression groups of SPP1. (C) Variations in the ratios of 21 different immune cell types between tumor samples with high and low SPP1 expression. (D) A heat map illustrated the spread of these immune-infiltrating cells within the tumor specimens. ns: no statistical significance, *p<0.05, **p<0.01, ***p<0.001.
It was found that SPP1 expression was correlated with 4 tumor-infiltrating immune cells by utilizing the TIMER database (Supplementary Figure 1A). We also identified relationships between SPP1 and the expression of 28 TILs in human cancers, with significant correlations with 23 of these immune cells. (Supplementary Figure 1B).
This discovery showed that SPP1 could play a special function in the immune cells’ invasion of LUAD.
Immune-inhibitory and immunostimulatory factors associated with SPP1 expression
Co-expression analysis was carried out utilizing TISIDB to learn more about the relationship between SPP1 and immunity. The use of immunomodulators in immunotherapies to target tumor cells and the TME around them has proven beneficial [22]. The goal was to determine how SPP1 expression and the expression of immunomodulators—which included both immunosuppressants and immunostimulants—related to one another.
Figure 8A visually depicted the association between SPP1 and the expression levels of 23 immunosuppressants in various human cancers, as obtained from the TISIDB database. There was a significant correlation between the expression of SPP1 and 11 immunosuppressants, including CD274 (rho=0.195, p=8.03e–06), CSF1R (rho=0.362, p=1.09e–17), HAVCR2 (rho=0.4, p<2.2e–16) and TGFBR1 (rho=0.239, p=3.98e–08). The expression of SPP1 could be regulated by immunosuppressive agents. Some immunosuppressants can inhibit SPP1 production or inhibit SPP1 expression in immune cells [23, 24].
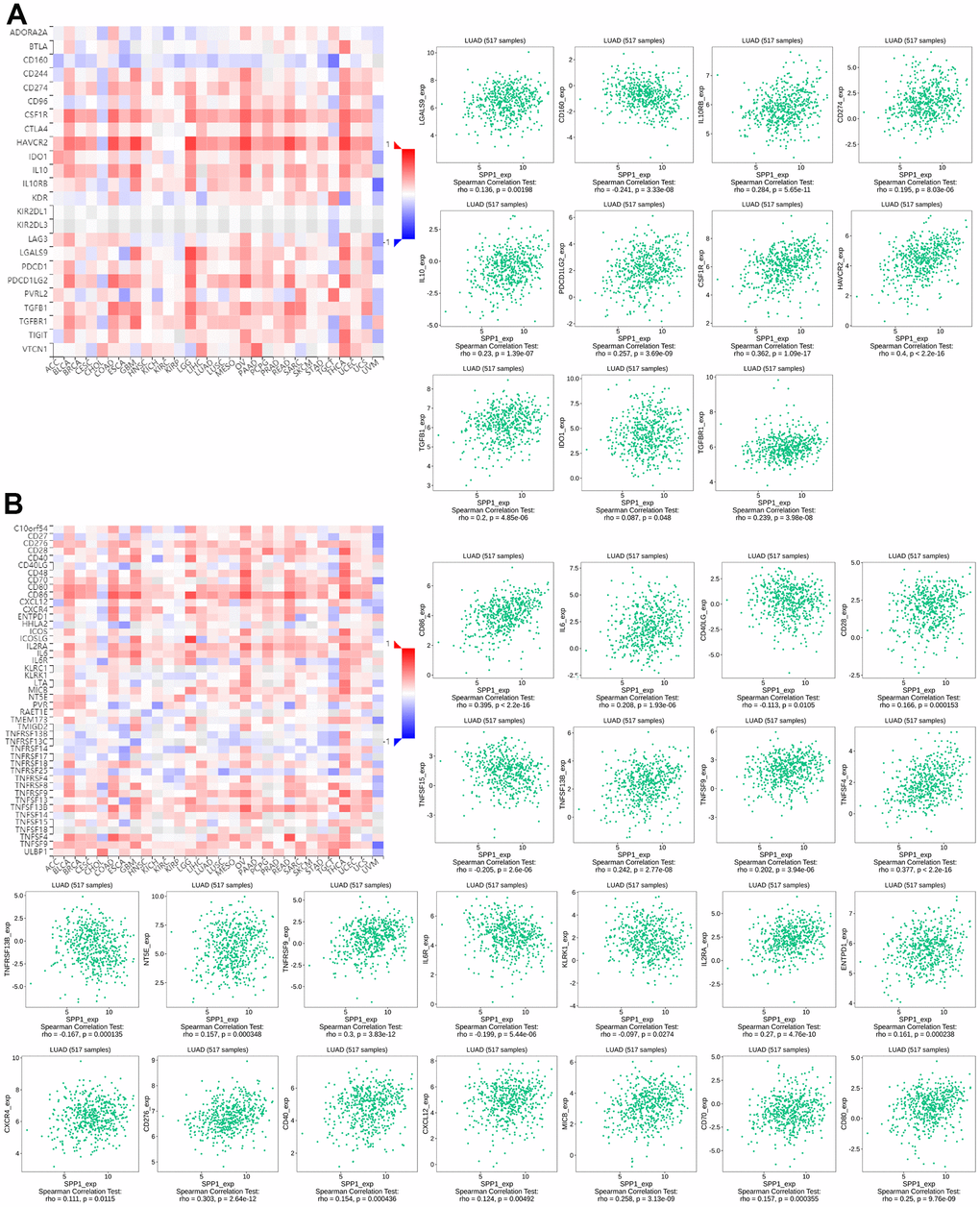
Figure 8. Correlation between the levels of immune infiltration and SPP1 expression. (A) Relationship between 23 immunosuppressants and SPP1 expression in LUAD. (B) Correlation between 46 immune enhancers and SPP1 expression in LUAD.
The relationship between SPP1 and the expression of 46 immune enhancers in human cancers from the TISIDB database was depicted in Figure 8B. A strong association was observed between SPP1 expression and 22 of these enhancers, including TNFSF15 (rho=–0.205, p=2.6e–06) and IL6R (rho=–0.199, p=5.44e–06). Therefore, it was inferred that SPP1 could serve as a target of immunostimulants or mediate the effects of immunostimulants.
The findings suggested that SPP1 may have a function in modifying immunological responses by being engaged in the regulation of these immune modulators.
Correlation analysis on LUAD to examine the relationship between SPP1 and associated genes and markers of immune cells
To better understand the connection between SPP1 expression and immune cell infiltration in LUAD, Table 4 displayed the results of the correlation between SPP1 expression and a number of markers related to immune infiltration. SPP1 expression was correlated with the majority of immunological marker sets of monocytes, tumor-associated macrophage (TAM), M1 macrophage, M2 macrophage, Dendritic cell and Tregs in LUAD. Additionally, SPP1 copy number alterations were examined in tumors with varying invasion levels. Notably, the arm-level deletion copy number variant of SPP1 exhibited a significant association with CD4+ T cells, macrophages, and dendritic cells infiltration in LUAD (Supplementary Figure 2). Consequently, SPP1 may modulate immune cell function through its ability to regulate marker gene expression.
Table 4. Correlation analysis between SPP1 and relate genes and markers of immune cells in LUAD by TIMER.
| Gene markers | None | p-value | Purity | p-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Correlation | Correlation | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD8+ T cell | CD8A | 0 | 0.9920 | -0.059 | 0.1940 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD8B | -0.012 | 0.7830 | -0.055 | 0.2190 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T cell (general) | CD3D | 0.044 | 0.3140 | -0.017 | 0.7080 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD3E | -0.021 | 0.6410 | -0.1 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD2 | 0.032 | 0.4670 | -0.035 | 0.4350 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| B cell | CD19 | -0.045 | 0.3090 | -0.113 | * | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD79A | 0.033 | 0.4530 | -0.021 | 0.6490 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Monocyte | CD86 | 0.405 | *** | 0.411 | *** | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD115 (CSF1R) | 0.376 | *** | 0.37 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TAM | CCL2 | 0.346 | *** | 0.334 | *** | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD68 | 0.319 | *** | 0.313 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IL10 | 0.25 | *** | 0.237 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M1 macrophage | INOS (NOS2) | 0.005 | 0.9140 | -0.033 | 0.4630 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IRF5 | 0.194 | *** | 0.176 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| COX2 (PTGS2) | 0.117 | * | 0.11 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M2 macrophage | CD163 | 0.316 | *** | 0.308 | *** | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VSIG4 | 0.379 | *** | 0.374 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MS4A4A | 0.331 | *** | 0.332 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Neutrophils | CD66b (CEACAM8) | -0.016 | 0.7090 | -0.032 | 0.4720 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD11B (ITGAM) | 0.358 | *** | 0.352 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CCR7 | -0.056 | 0.2020 | -0.134 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Natural killer cell | KIR2DL1 | -0.063 | 0.1540 | -0.095 | * | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| KIR2DL3 | -0.031 | 0.4780 | -0.06 | 0.1810 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| KIR2DL4 | 0.095 | * | 0.068 | 0.1300 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| KIR3DL1 | -0.07 | 0.1130 | -0.107 | 0.0174 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| KIR3DL2 | 0.005 | 0.9140 | -0.018 | 0.6880 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| KIR3DL3 | 0.044 | 0.3240 | 0.022 | 0.6310 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| KIR2DS4 | -0.049 | 0.2710 | -0.081 | 0.0710 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dendritic cell | HLA-DPB1 | 0.094 | * | 0.055 | 0.2200 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HLA-DQB1 | 0.099 | * | 0.067 | 0.1370 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HLA-DRA | 0.192 | *** | 0.169 | ** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HLA-DPA1 | 0.152 | ** | 0.117 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BDCA-1 (CD1C) | 0.052 | 0.2360 | 0.03 | 0.5120 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BDCA-4 (NRP1) | 0.16 | ** | 0.139 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CD11c (ITGAX) | 0.209 | *** | 0.237 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Th1 | T-bet (TBX21) | -0.075 | 0.0911 | -0.142 | * | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| STAT4 | 0.09 | * | 0.04 | 0.3750 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| STAT1 | 0.158 | ** | 0.127 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IFN-g (IFNG) | 0.062 | 0.1620 | 0.021 | 0.6350 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TNF-a (TNF) | 0.173 | *** | 0.151 | ** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Th2 | GATA3 | 0.051 | 0.2450 | -0.006 | 0.8960 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| STAT6 | -0.173 | *** | -0.168 | ** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| STAT5A | 0.076 | 0.0864 | 0.036 | 0.4220 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IL-13 | -0.044 | 0.317 | -0.074 | 0.0989 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tfh | BCL6 | 0.016 | 0.7210 | 0.001 | 0.9850 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IL21 | 0.042 | 0.3440 | 0.01 | 0.8270 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Th17 | STAT3 | 0.011 | 0.8030 | 0.004 | 0.9220 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IL17A | -0.021 | 0.6390 | -0.047 | 0.2940 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treg | FOXP3 | 0.146 | ** | 0.097 | * | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CCR8 | 0.164 | ** | 0.13 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| STAT5B | -0.062 | 0.1630 | -0.074 | 0.0998 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TGF-β(TGFB1) | 0.208 | *** | 0.179 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T cell exhaustion | PD-1(PDCD1) | 0.067 | 0.1290 | 0.016 | 0.7240 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTLA4 | 0.074 | 0.0937 | 0.019 | 0.6800 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TIM-3(HAVCR2) | 0.406 | *** | 0.407 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GZMB | 0.127 | * | 0.09 | * | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LAG3 | 0.052 | 0.2430 | 0.006 | 0.8960 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PDL1(CD274) | 0.216 | *** | 0.186 | *** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *p<0.05, **p<0.01, ***p<0.001. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Correlation between SPP1 expression and drug sensitivity
Drug resistance has long been recognized as a major obstacle in LAUD management. To enhance the clinical efficacy of different treatments, it is imperative to subject different chemotherapy drugs to sensitivity analysis. In this study, we analyzed the sensitivity of 367 drugs in the GDSC database. Specifically, 510 samples in the TCGA-LUAD dataset were categorized into the high and low expression groups based on the expression levels of the SPP1 gene, and subsequently, IC50 values were calculated. Remarkably, we observed that the IC50 values of 127 drugs exhibited significant disparities between the high and low SPP1 expression groups, including notable drugs, such as gemcitabine and cisplatin (Figure 9). Spearman correlation analysis also showed a significant negative correlation between SPP1 expression level and the two drugs, gemcitabine and cisplatin. This finding suggested that tumors with elevated SPP1 expression levels show heightened sensitivity to gemcitabine and cisplatin, rendering them more likely to respond favorably to these treatments compared with counterparts with low SPP1 expression levels. Moreover, these findings provided valuable insights for tailoring personalized treatments for individual patients with LUAD. However, further research is required to validate these observations and elucidate the underlying associated mechanisms.
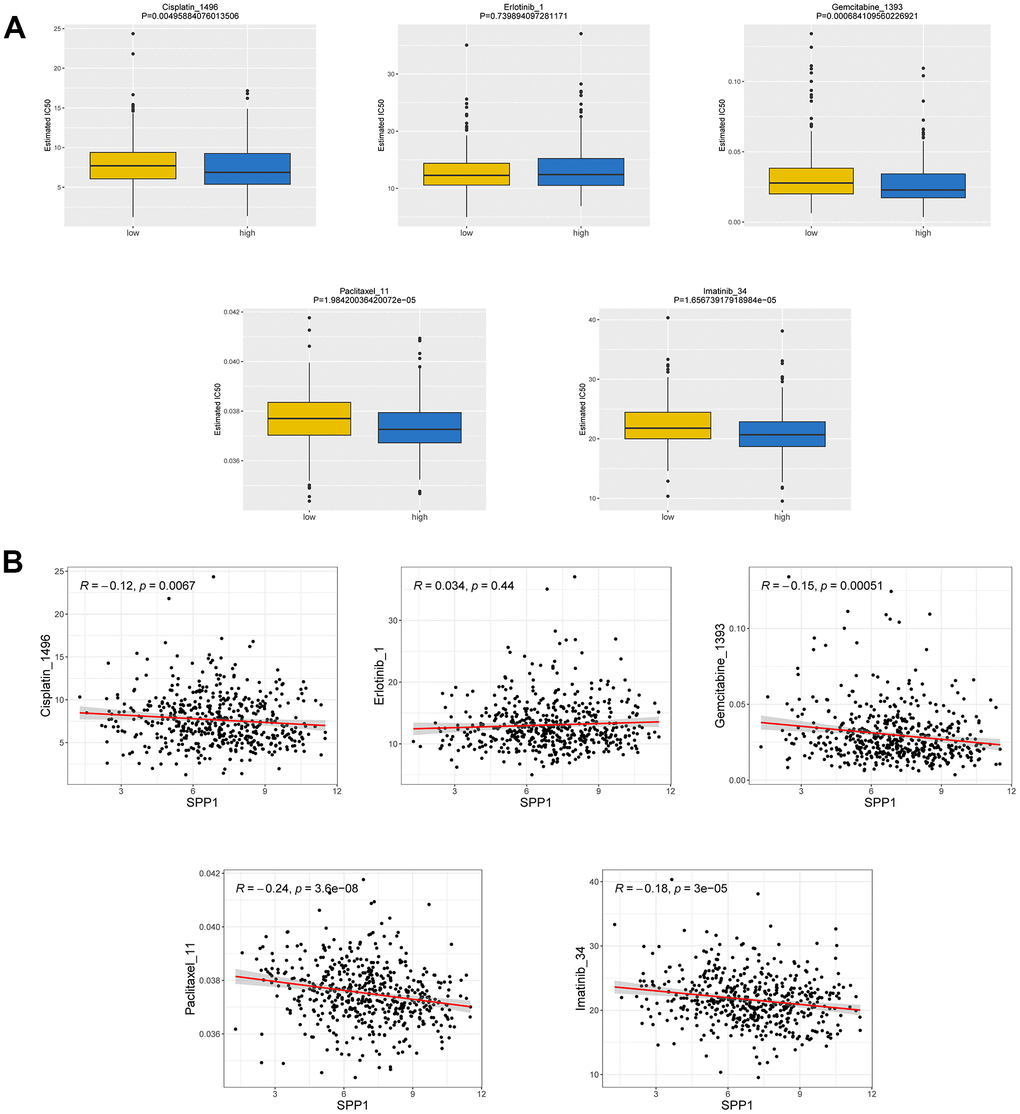
Figure 9. Correlation between drug susceptibility and SPP1 expression. (A) IC50 difference between groups with high and low expression of the SPP1. (B) Relationship between IC50 and SPP1.
Discussion
LUAD is a common cancer type distinguished by a substantial frequency and elevated fatality rate [25, 26]. In the treatment of LUAD, radiotherapy and chemotherapy remain the primary therapeutic modalities for patients with advanced and end-stage disease, whereas radical surgery is preferred for patients in early stages [27]. Therefore, it is crucial to investigate effective molecular targets to improve treatment results [28]. Such advancements will bring us closer to overcoming the formidable challenges associated with cancer. Nevertheless, the use of pharmaceutical interventions is considerably constrained by the presence of adenocarcinoma mutations and drug resistance, which impedes their widespread application [29, 30]. Therefore, it is crucial to identify new predictive biomarkers that can explore the underlying mechanisms of LUAD and support the advancement of therapeutic treatments.
SPP1 gene refers to the gene encoding Osteopontin-1. OPN, which is secreted by tumor cells, osteoclasts, immune cells, and other cells, being a constituent of the extracellular matrix [31]. SPP1 glycoprotein is involved in a variety of important physiological and pathological processes outside the cell, including cell migration, recruitment of inflammatory cells and tumor metastasis [32]. SPP1 is extensively found in various human tissues and organs, highly expressed in numerous tumors, and linked to unfavorable prognosis [33]. It is secreted by diverse cancer cell types, playing a role in the initiation, advancement, spread, infiltration, and resistance to radiotherapy of tumors [27, 34]. Nevertheless, the precise workings of SPP1 in LUAD are still not fully understood.
The major goal of this study was to investigate the role of SPP1 in LUAD prognosis and immune response. SPP1 was identified as one of the DEGs showing a strong correlation with immune responses and prognosis in NSCLC. Analysis of data from the TCGA databases revealed that NSCLC samples exhibited elevated levels of SPP1 expression compared with normal tissues. These results were further validated using the GEO database. We also observed that elevated SPP1 expression levels were significantly associated with clinicopathological features and unfavorable survival outcomes in patients with LUAD, whereas no such correlation was observed in patients with LUSC. Therefore, considering that the correlation between SPP1 and LUSC was not significant, our subsequent analyses involved only LUAD. Furthermore, the detailed analysis of the relationship between SPP1 expression and the clinical attributes of patients with LUAD showed a significant correlation between SPP1 expression level and N stage and primary efficacy assessment, whereas no significant correlation was observed for other clinicopathological factors. For older male patients (aged ≥65 years) and those with disease at the T3 stage, our analysis showed a significant correlation between SPP1 mRNA expression level and the clinical prognosis. Therefore, we further investigated the prognostic impact of SPP1 on LUAD. The prognostic analysis of clinical subgroups in LUAD showed that the higher SPP1 expression level in patients with pathological stage III and T stage T3 of the disease was significantly associated with a worse OS. The ROC curves obtained in this regard showed that SPP1 exhibited slightly superior predictive capability for 1-, 3-, and 5-year survival compared with random prediction, thereby validating the accuracy of the SPP1 expression-based diagnostic prediction in LAUD. Moreover, both univariate and multivariate analyses provided additional evidence supporting SPP1 expression as a significant predictor of survival, consistent with findings from previous studies [35]. Numerous research has shown a robust association between the manifestation of SPP1 and tumor cells evolutionary progression, along with the microenvironment reprogramming [36–39]. Furthermore, it has been noted that the existence of molecular diversity within tumors is vital in the emergence of resistance to treatment and substantially affects the prognosis of patients. Notably, both experimental and human invasive lung cancers have exhibited an overexpression of SPP1, which has been associated with unfavorable survival outcomes [40, 41]. As a result, the increased expression of SPP1 is commonly considered as a biomarker, suggesting an unfavorable prognosis in individuals diagnosed with LUAD.
Since SPP1 showed association with OS in patients with LUAD, we performed further analyses, which revealed significant associations between SPP1 expression level and various stages of LUAD. To elucidate the molecular mechanisms of SPP1 in LUAD, CancerSEA and GSEA analyses were performed. Furthermore, we comprehensively analyzed the functional role of SPP1 in LUAD. The results obtained showed a negative correlation between SPP1 expression levels and various cellular processes, including metastasis, EMT, angiogenesis, DNA damage, cancer cell invasion, and cell differentiation. Therefore, our findings enhance comprehension regarding the role of SPP1 and its fundamental mechanism in LUAD cells. Based on the EMTome database, a metastatic analysis revealed an association between SPP1 and metastasis in lung cancer. According to gene enrichment analysis, SPP1 is associated with 34 pathways, one of which is EMT. These results would help further explore the pathophysiological mechanisms of SPP1. Additionally, the upregulation of SPP1 was involved in EMT pathways that were critical for the development of LUAD, including the heightened expression of mesenchymal cell markers (N-cadherin, vimentin), a number of transcription factor families (SNAI1, SLUG, TWIST1, TWIST2, ZEB1, and ZEB2) which controlled how the EMT process was modulated, the overexpression of matrix metalloproteinases (MMP2 and MMP9) and the EMT-related signal transduction pathway (TGF-β). Subsequently, the correlation was examined between the expression of SPP1 and the infiltration of immune cells in LUAD.
This study found that a close association was observed between SPP1 and immunomodulatory factors. Research has demonstrated that the host immune system can be regulated by SPP1 in mouse macrophages and natural killer cells [42, 43]. A variation in the plasma level of OPN expressed by SPP1 could impose an influence on cancer metastasis, which had a chemotactic effect on numerous immune cells and affected cell-mediated immunity [44]. In LUAD, the involvement of SPP1 included the increase of PD-L1 levels, which subsequently affected the polarization of macrophages and aided in evading the immune system [45, 46]. Together, these findings suggested a potential involvement of SPP1 in immunity. The analysis showed that immune cells that infiltrate tumors and TILs were associated with SPP1 expression levels in LUAD. High levels of SPP1 upregulated the immunosuppressive expression of LGALS9, IL10RB, CD274, IL10, PDCD1LG2, CSF1R, HAVCR2, TGFB1, IDO1, and TGFBR1. Simultaneously, SPP1 downregulated CD40LG, TNFSF15, TNFRSF13B, IL6R, KLRK1, and other immune stimulants, indicating that SPP1 played a role in the evasion of tumor immunity by controlling the immunosuppressive surroundings. These findings highlighted the possible function of SPP1 in the TME of LUAD.
Furthermore, the expression of SPP1 exhibited correlations with various factors, including tumor purity, macrophages, neutrophils, and DCs. Notably, SPP1 expression was related to a number of markers related to immune infiltration and the arm-level deletion copy number variant of SPP1 exhibited a significant association with CD4+ T cells, macrophages, and dendritic cells infiltration in LUAD. Previous research has also demonstrated the significance of SPP1 as a chemokine in recruiting macrophages to glioblastomas, facilitating communication between tumor cells and the innate immune system, and potentially serving as a therapeutic target [47]. Furthermore, the tumor immune microenvironment was affected by SPP1 as it increases the PD-L3 expression via the PI1K/AKT, JAK, and TGF-β signaling pathways [48]. Other studies have also provided a comprehensive analysis of the interplay between SPP1 and its receptor, CD47, elucidating their inhibitory effects on angiogenesis through the antagonism of nitric oxide signaling in endothelial and vascular smooth muscle cells [49]. These studies supported the findings of this study related to the role of SPP1 in the immune system of patients with LUAD.
In summary, we have demonstrated that SPP1 is a valuable prognostic marker for LUAD which may prove beneficial for improved disease prediction and immunotherapy. However, the specific mechanism of action awaits verification, and further experimental studies, as well as clinical trials will be necessary.
This study offered a thorough examination of the predictive and immune relationship between SPP1 and LUAD. Consequently, these findings have significant implications for the TME. Specifically, this investigation systematically investigates the impact of SPP1 on tumor progression, prognosis, and immune in individuals diagnosed with LUAD. The findings of this research indicate that the increase in SPP1 is involved in immune transmission and is strongly linked to an adverse prognosis in patients with LUAD. Thus, SPP1 emerges as a promising biomarker for prognosticating human LUAD and represents a novel therapeutic target.
Materials and Methods
Screening of differentially expressed genes (DEGs)
A total of 5291 DEGs were screened using transcriptome data from NSCLC (LUAD and LUSC) cells or tissues and normal tissue samples extracted from The Cancer Genome Atlas (TCGA) (https://portal.gdc.cancer.gov/). The statistical thresholds for DEG analysis were as follows: |log (fold change) | > 2 and adjusted p-value < 0.01. Additionally, duplicate gene names were eliminated. Therefore, 2483 immune-related genes were identified using the Immunology Database and Analysis Portal (ImmPort) database. Eventually, 1793 genes were retained for the study after excluding genes with identical symbol names. Subsequently, we investigated the overlap between DEGs and immune-associated genes in ImmPort. The selected genes continued to be screened for genes associated with prognosis in the TCGA database to get overlapping genes. The results were shown as Venn diagrams.
Data acquisition and analysis
In TCGA database, transcriptome RNA-Seq data and related clinical data were gathered. Depending on pathological traits, the patient cohort was divided into two groups, LUAD (n=598) and LUSC (n=551). Additionally, we retrieved independent datasets (GSE101929, n=66; GSE19188, n=156; GSE116959, n=68) from the Gene Expression Omnibus (GEO) database (https://www.ncbi.nlm.nih.gov/geo/) to obtain three separate groups of tumor and control samples from NSCLC patients. To investigate the impact of SPP1 on the pathological stage and patient outcomes, a subgroup analysis was conducted.
Analysis of receiver operating characteristic (ROC) curve
Using the pROC package in the R programming language, the true and false positive rates data points were obtained, the ROC curve was constructed, and the area of the curve was computed. In the two-dimensional ROC curve, the ordinate and abscissa represented the true positive and true negative rates, respectively.
Evaluation of logistic regression via univariate and multivariate methods
To assess if SPP1 could serve as a standalone prognostic indicator in LUAD, univariate and multivariate analyses were used, considering the impact of SPP1 and clinicopathological characteristics of LUAD. Subsequently, the survival time was assessed using COX regression analysis to determine the impact of various factors and provide the corresponding hazard ratio (HR), while taking into account other potential factors. First, single factor analysis was conducted to assess the extent of the influence of different SPP1 expression levels on independent variables. Thereafter, we assessed how multiple factors, including SPP1 expression, affected LUAD prognosis.
Analysis of individual cells
CancerSEA (http://biocc.hrbmu.edu.cn/CancerSEA/), an online database and tool, facilitates the integrated analysis and interpretation of single-cell transcriptome data to uncover expression patterns of the SPP1 gene and the underlying biological mechanisms in LUAD.
Assessment of cancer metastasis
EMTome database (http://ec2-3-231-76-84.compute-1.amazonaws.com/emtome/) was used for the analysis of SPP1 in lung cancer metastasis. To pinpoint crucial pathways connected to tumor metastasis, Gene Set Enrichment Analysis (GSEA) of gene set relevant to metastasis was carried out. A special GSEA-based enrichment analysis approach called Hallmark pathway enrichment analysis was applied.
Analysis with the CIBERSORT algorithm
The immune landscape was examined using the CIBERSORT method, and the relationship between SPP1 expression and immunological performance was assessed. This relationship level was inferred from a large number of tumor transcriptomes of patients with LUAD and immune cell subtypes.
Timer database analysis
TIMER (https://cistrome.shinyapps.io/timer/), a network server, was used to analyze the relationship between SPP1 expression and the presence of several immune cells in patients with LUAD, including B lymphocytes, CD8+T lymphocytes, CD4+T lymphocytes, dendritic cells (DCs), macrophages, and neutrophils. We also discovered the connection between SPP1 overexpression and tumor purity using TIMER’s "Relevant" module and the tumor purity correction section.
TISIDB database analysis
The TISIDB portal website (http://cis.hku.hk/TISIDB/index.php) was utilized to assess tumor-immune interactions and evaluate the relevance of SPP1 expression to immunosuppression and immune activation. Moreover, TISIDB was utilized as a valuable resource to explore potential connections between SPP1 expression and the presence of tumor-infiltrating lymphocytes (TILs) in diverse human cancers. Gene expression profiles were employed to conduct gene set variation analysis, enabling the evaluation of TILs proportions. Spearman test was then used to measure the connection between SPP1 expression and TILs levels.
Drug sensitivity analysis
The TCGA-LUAD dataset from the Genomics of Drug Sensitivity in Cancer (GDSC) [50] (https://www.cancerrxgene.org/) database, containing data regarding 510 samples and 367 drugs, was employed for sensitivity analysis. The IC50 values of the 367 drugs were compared between the high and low SPP1 expression groups using the oncoPredict package in R by performing a Wilcoxon rank sum test. Furthermore, Spearman correlation analysis was used to examine the association between the different variables.
Analysis of data using statistical methods
For comparing two groups, statistical methods, such as t-test and Wilcoxon test, were utilized, while Kruskal-Wallis test was used for comparing several groups. To investigate the survival analysis of the patients, univariate and multivariate logistic regression analyses, as well as Kaplan-Meier (KM) curves that showed the survival analysis curves, were employed. Continuous variables according to whether they had a linear relationship, Spearman’s or Pearson’s correlation coefficients were used to assess the relationship between SPP1 expression and immune infiltration. All data analyses were performed in R (version 4.0.3) and statistical significance was defined as a p-value of 0.05 or less.
Author Contributions
Binbin Li wrote the original draft; Xue Li and Qingfeng Yang checked the data, figures and tables; Yiyang Jiang downloaded and analyzed the raw data from TCGA and GEO databases; Qianwen Zhang reviewed the relevant literature; Jingtao Zhang contributed to analyze the data; Wenqiang Cui prepared the figures and tables; and Fei Xu designed the study and made revisions.
Conflicts of Interest
All authors declared that they had no conflicts of interest.
Funding
The present study was supported by the Shandong Province Taishan Scholar Project (grant no. tsqn 202306393 and 202211355) and the China Postdoctoral Science Foundation (grant no. 2021T140427 and 2021M691986).
References
- 1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023; 73:17–48. https://doi.org/10.3322/caac.21763 [PubMed]
- 2. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021; 398:535–54. https://doi.org/10.1016/S0140-6736(21)00312-3 [PubMed]
- 3. Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018; 553:446–54. https://doi.org/10.1038/nature25183 [PubMed]
- 4. Ruiz-Cordero R, Devine WP. Targeted Therapy and Checkpoint Immunotherapy in Lung Cancer. Surg Pathol Clin. 2020; 13:17–33. https://doi.org/10.1016/j.path.2019.11.002 [PubMed]
- 5. Deng HY, Zeng M, Li G, Alai G, Luo J, Liu LX, Zhou Q, Lin YD. Lung Adenocarcinoma has a Higher Risk of Lymph Node Metastasis than Squamous Cell Carcinoma: A Propensity Score-Matched Analysis. World J Surg. 2019; 43:955–62. https://doi.org/10.1007/s00268-018-4848-7 [PubMed]
- 6. Kidess E, Giesecke Y, Eichhorn I, Mohr R, Jann H, Fischer C, Wiedenmann B, Roderburg C, Tacke F, Sigal M. Osteopontin is a prognostic circulating biomarker in patients with neuroendocrine neoplasms. J Cancer Res Clin Oncol. 2023; 149:10925–33. https://doi.org/10.1007/s00432-023-04979-6 [PubMed]
- 7. Tang Z, Xia Z, Wang X, Liu Y. The critical role of osteopontin (OPN) in fibrotic diseases. Cytokine Growth Factor Rev. 2023; 74:86–99. https://doi.org/10.1016/j.cytogfr.2023.08.007 [PubMed]
- 8. Chunder R, Schropp V, Marzin M, Amor S, Kuerten S. A Dual Role of Osteopontin in Modifying B Cell Responses. Biomedicines. 2023; 11:1969. https://doi.org/10.3390/biomedicines11071969 [PubMed]
- 9. Robinson JA, Mahmud FJ, Greif E, Toribio M, Zanni MV, Brown AM, Burdo TH. Osteopontin Is an Integral Mediator of Cardiac Interstitial Fibrosis in Models of Human Immunodeficiency Virus Infection. J Infect Dis. 2023; 228:122–32. https://doi.org/10.1093/infdis/jiad149 [PubMed]
- 10. Fedarko NS, Jain A, Karadag A, Fisher LW. Three small integrin binding ligand N-linked glycoproteins (SIBLINGs) bind and activate specific matrix metalloproteinases. FASEB J. 2004; 18:734–6. https://doi.org/10.1096/fj.03-0966fje [PubMed]
- 11. Liu Y, Ye G, Dong B, Huang L, Zhang C, Sheng Y, Wu B, Han L, Wu C, Qi Y. A pan-cancer analysis of the oncogenic role of secreted phosphoprotein 1 (SPP1) in human cancers. Ann Transl Med. 2022; 10:279. https://doi.org/10.21037/atm-22-829 [PubMed]
- 12. Pang X, Zhang J, He X, Gu Y, Qian BZ, Xie R, Yu W, Zhang X, Li T, Shi X, Zhou Y, Cui Y. SPP1 Promotes Enzalutamide Resistance and Epithelial-Mesenchymal-Transition Activation in Castration-Resistant Prostate Cancer via PI3K/AKT and ERK1/2 Pathways. Oxid Med Cell Longev. 2021; 2021:5806602. https://doi.org/10.1155/2021/5806602 [PubMed]
- 13. Chen X, Xiong D, Ye L, Yang H, Mei S, Wu J, Chen S, Mi R. SPP1 inhibition improves the cisplatin chemo-sensitivity of cervical cancer cell lines. Cancer Chemother Pharmacol. 2019; 83:603–13. https://doi.org/10.1007/s00280-018-3759-5 [PubMed]
- 14. Zhao K, Ma Z, Zhang W. Comprehensive Analysis to Identify SPP1 as a Prognostic Biomarker in Cervical Cancer. Front Genet. 2022; 12:732822. https://doi.org/10.3389/fgene.2021.732822 [PubMed]
- 15. Göthlin Eremo A, Lagergren K, Othman L, Montgomery S, Andersson G, Tina E. Evaluation of SPP1/osteopontin expression as predictor of recurrence in tamoxifen treated breast cancer. Sci Rep. 2020; 10:1451. https://doi.org/10.1038/s41598-020-58323-w [PubMed]
- 16. Wang J, Hao F, Fei X, Chen Y. SPP1 functions as an enhancer of cell growth in hepatocellular carcinoma targeted by miR-181c. Am J Transl Res. 2019; 11:6924–37. [PubMed]
- 17. Matsubara E, Yano H, Pan C, Komohara Y, Fujiwara Y, Zhao S, Shinchi Y, Kurotaki D, Suzuki M. The Significance of SPP1 in Lung Cancers and Its Impact as a Marker for Protumor Tumor-Associated Macrophages. Cancers (Basel). 2023; 15:2250. https://doi.org/10.3390/cancers15082250 [PubMed]
- 18. Yim A, Smith C, Brown AM. Osteopontin/secreted phosphoprotein-1 harnesses glial-, immune-, and neuronal cell ligand-receptor interactions to sense and regulate acute and chronic neuroinflammation. Immunol Rev. 2022; 311:224–33. https://doi.org/10.1111/imr.13081 [PubMed]
- 19. Kalluri R, Weinberg RA. The basics of epithelial-mesenchymal transition. J Clin Invest. 2009; 119:1420–8. https://doi.org/10.1172/JCI39104 [PubMed]
- 20. Yang J, Antin P, Berx G, Blanpain C, Brabletz T, Bronner M, Campbell K, Cano A, Casanova J, Christofori G, Dedhar S, Derynck R, Ford HL, et al, and EMT International Association (TEMTIA). Guidelines and definitions for research on epithelial-mesenchymal transition. Nat Rev Mol Cell Biol. 2020; 21:341–52. https://doi.org/10.1038/s41580-020-0237-9 [PubMed]
- 21. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010; 140:883–99. https://doi.org/10.1016/j.cell.2010.01.025 [PubMed]
- 22. Tang H, Qiao J, Fu YX. Immunotherapy and tumor microenvironment. Cancer Lett. 2016; 370:85–90. https://doi.org/10.1016/j.canlet.2015.10.009 [PubMed]
- 23. Darvin P, Toor SM, Sasidharan Nair V, Elkord E. Immune checkpoint inhibitors: recent progress and potential biomarkers. Exp Mol Med. 2018; 50:1–11. https://doi.org/10.1038/s12276-018-0191-1 [PubMed]
- 24. Cheng M, Liang G, Yin Z, Lin X, Sun Q, Liu Y. Immunosuppressive role of SPP1-CD44 in the tumor microenvironment of intrahepatic cholangiocarcinoma assessed by single-cell RNA sequencing. J Cancer Res Clin Oncol. 2023; 149:5497–512. https://doi.org/10.1007/s00432-022-04498-w [PubMed]
- 25. Brody H. Lung cancer. Nature. 2020; 587:S7. https://doi.org/10.1038/d41586-020-03152-0 [PubMed]
- 26. Chen P, Quan Z, Song X, Gao Z, Yuan K. MDFI is a novel biomarker for poor prognosis in LUAD. Front Oncol. 2022; 12:1005962. https://doi.org/10.3389/fonc.2022.1005962 [PubMed]
- 27. Shen XY, Liu XP, Song CK, Wang YJ, Li S, Hu WD. Genome-wide analysis reveals alcohol dehydrogenase 1C and secreted phosphoprotein 1 for prognostic biomarkers in lung adenocarcinoma. J Cell Physiol. 2019; 234:22311–20. https://doi.org/10.1002/jcp.28797 [PubMed]
- 28. Chen J, Fu Y, Hu J, He J. Hypoxia-related gene signature for predicting LUAD patients’ prognosis and immune microenvironment. Cytokine. 2022; 152:155820. https://doi.org/10.1016/j.cyto.2022.155820 [PubMed]
- 29. Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, Garg K, Austin JH, Asamura H, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; 6:244–85. https://doi.org/10.1097/JTO.0b013e318206a221 [PubMed]
- 30. Matsubara E, Komohara Y, Esumi S, Shinchi Y, Ishizuka S, Mito R, Pan C, Yano H, Kobayashi D, Fujiwara Y, Ikeda K, Sakagami T, Suzuki M. SPP1 Derived from Macrophages Is Associated with a Worse Clinical Course and Chemo-Resistance in Lung Adenocarcinoma. Cancers (Basel). 2022; 14:4374. https://doi.org/10.3390/cancers14184374 [PubMed]
- 31. Cao DX, Li ZJ, Jiang XO, Lum YL, Khin E, Lee NP, Wu GH, Luk JM. Osteopontin as potential biomarker and therapeutic target in gastric and liver cancers. World J Gastroenterol. 2012; 18:3923–30. https://doi.org/10.3748/wjg.v18.i30.3923 [PubMed]
- 32. O’Regan A. The role of osteopontin in lung disease. Cytokine Growth Factor Rev. 2003; 14:479–88. https://doi.org/10.1016/s1359-6101(03)00055-8 [PubMed]
- 33. Zeng B, Zhou M, Wu H, Xiong Z. SPP1 promotes ovarian cancer progression via Integrin β1/FAK/AKT signaling pathway. Onco Targets Ther. 2018; 11:1333–43. https://doi.org/10.2147/OTT.S154215 [PubMed]
- 34. Rabjerg M, Bjerregaard H, Halekoh U, Jensen BL, Walter S, Marcussen N. Molecular characterization of clear cell renal cell carcinoma identifies CSNK2A1, SPP1 and DEFB1 as promising novel prognostic markers. APMIS. 2016; 124:372–83. https://doi.org/10.1111/apm.12519 [PubMed]
- 35. Yi X, Luo L, Zhu Y, Deng H, Liao H, Shen Y, Zheng Y. SPP1 facilitates cell migration and invasion by targeting COL11A1 in lung adenocarcinoma. Cancer Cell Int. 2022; 22:324. https://doi.org/10.1186/s12935-022-02749-x [PubMed]
- 36. Ma L, Wang L, Ching-Wen C, Heinrich S, Dominguez D, Forgues M, Candia J, Hernandez MO, Kelly M, Zhao Y, Tran B, Hernandez JM, Davis JL, et al. Single-cell atlas of tumor clonal evolution in liver cancer. Cold Spring Harbor Laboratory Press. 2020. https://doi.org/10.1101/2020.08.18.254748
- 37. Rittling SR, Chambers AF. Role of osteopontin in tumour progression. Br J Cancer. 2004; 90:1877–81. https://doi.org/10.1038/sj.bjc.6601839 [PubMed]
- 38. Hoeft K, Schaefer GJL, Kim H, Schumacher D, Bleckwehl T, Long Q, Klinkhammer BM, Peisker F, Koch L, Nagai J, Halder M, Ziegler S, Liehn E, et al. Platelet-instructed SPP1+ macrophages drive myofibroblast activation in fibrosis in a CXCL4-dependent manner. Cell Rep. 2023; 42:112131. https://doi.org/10.1016/j.celrep.2023.112131 [PubMed]
- 39. Morse C, Tabib T, Sembrat J, Buschur KL, Bittar HT, Valenzi E, Jiang Y, Kass DJ, Gibson K, Chen W, Mora A, Benos PV, Rojas M, Lafyatis R. Proliferating SPP1/MERTK-expressing macrophages in idiopathic pulmonary fibrosis. Eur Respir J. 2019; 54:1802441. https://doi.org/10.1183/13993003.02441-2018 [PubMed]
- 40. Giopanou I, Kanellakis NI, Giannou AD, Lilis I, Marazioti A, Spella M, Papaleonidopoulos V, Simoes DCM, Zazara DE, Agalioti T, Moschos C, Magkouta S, Kalomenidis I, et al. Osteopontin drives KRAS-mutant lung adenocarcinoma. Carcinogenesis. 2020; 41:1134–44. https://doi.org/10.1093/carcin/bgz190 [PubMed]
- 41. Tang H, Chen J, Han X, Feng Y, Wang F. Upregulation of SPP1 Is a Marker for Poor Lung Cancer Prognosis and Contributes to Cancer Progression and Cisplatin Resistance. Front Cell Dev Biol. 2021; 9:646390. https://doi.org/10.3389/fcell.2021.646390 [PubMed]
- 42. Dong B, Wu C, Huang L, Qi Y. Macrophage-Related SPP1 as a Potential Biomarker for Early Lymph Node Metastasis in Lung Adenocarcinoma. Front Cell Dev Biol. 2021; 9:739358. https://doi.org/10.3389/fcell.2021.739358 [PubMed]
- 43. Rabinowich H, Lin WC, Amoscato A, Herberman RB, Whiteside TL. Expression of vitronectin receptor on human NK cells and its role in protein phosphorylation, cytokine production, and cell proliferation. J Immunol. 1995; 154:1124–35. https://doi.org/10.4049/jimmunol.154.3.1124 [PubMed]
- 44. Wang KX, Denhardt DT. Osteopontin: role in immune regulation and stress responses. Cytokine Growth Factor Rev. 2008; 19:333–45. https://doi.org/10.1016/j.cytogfr.2008.08.001 [PubMed]
- 45. Zhang Y, Du W, Chen Z, Xiang C. Upregulation of PD-L1 by SPP1 mediates macrophage polarization and facilitates immune escape in lung adenocarcinoma. Exp Cell Res. 2017; 359:449–57. https://doi.org/10.1016/j.yexcr.2017.08.028 [PubMed]
- 46. Xu C, Sun L, Jiang C, Zhou H, Gu L, Liu Y, Xu Q. SPP1, analyzed by bioinformatics methods, promotes the metastasis in colorectal cancer by activating EMT pathway. Biomed Pharmacother. 2017; 91:1167–77. https://doi.org/10.1016/j.biopha.2017.05.056 [PubMed]
- 47. Wei J, Marisetty A, Schrand B, Gabrusiewicz K, Hashimoto Y, Ott M, Grami Z, Kong LY, Ling X, Caruso H, Zhou S, Wang YA, Fuller GN, et al. Osteopontin mediates glioblastoma-associated macrophage infiltration and is a potential therapeutic target. J Clin Invest. 2019; 129:137–49. https://doi.org/10.1172/JCI121266 [PubMed]
- 48. Wang Y, Zheng K, Chen X, Chen R, Zou Y. Bioinformatics analysis identifies COL1A1, THBS2 and SPP1 as potential predictors of patient prognosis and immunotherapy response in gastric cancer. Biosci Rep. 2021; 41:BSR20202564. https://doi.org/10.1042/BSR20202564 [PubMed]
- 49. Bornstein P. Thrombospondins function as regulators of angiogenesis. J Cell Commun Signal. 2009; 3:189–200. https://doi.org/10.1007/s12079-009-0060-8 [PubMed]
- 50. Yang W, Soares J, Greninger P, Edelman EJ, Lightfoot H, Forbes S, Bindal N, Beare D, Smith JA, Thompson IR, Ramaswamy S, Futreal PA, Haber DA, et al. Genomics of Drug Sensitivity in Cancer (GDSC): a resource for therapeutic biomarker discovery in cancer cells. Nucleic Acids Res. 2013; 41:D955–61. https://doi.org/10.1093/nar/gks1111 [PubMed]