



Introduction
Frailty is characterized by a decline in physiological capacity across multiple systems, which leads to an increased vulnerability to stressors. It is highly prevalent in old age and is associated with a high risk of falls, disability, hospitalization, and mortality. This leads to a high burden of care and reduced quality of life [1–4]. As the aging population rapidly expands, the severity of frailty has gained increasing international attention. The Frailty index (FI), a relatively popular tool for measuring frailty, is a continuous measure calculated as the ratio of age-related health deficits to total deficits considered [5]. It has been previously validated in UK Biobank by Williams et al. [6]. It discriminates better at the low to middle end of the frailty continuum compared to the frailty phenotype, which is another measuring tool of frailty [7]. Several risk factors for frailty have been identified in previous studies, including smoking [8, 9], obesity [10–12], and sedentary behavior [13, 14], while alcohol [9, 15], birth weight [16], and physical activity [13, 14] have been identified as protective factors. However, most of the available evidence on frailty and these factors are from observational studies, which are vulnerable to potential confounders, reverse causality, and other biases that can undermine actual causation.
Mendelian randomization (MR) provides a novel analytic method that utilizes genetic variants of exposure as instrumental variables to estimate the causal association between exposure and health outcome [17]. Since genetic variants are randomly allocated and fixed at conception, MR studies can avoid reverse causality and are less vulnerable to confounders than conventional observational studies. Therefore, we applied two-sample MR to investigate the causal link between overall obesity (indicated by body mass index (BMI)), abdominal obesity (indicated by waist circumference), birth weight, and lifestyle factors (cigarette smoking, alcohol consumption, moderate-to-vigorous intensity physical activity (MVPA), and leisure screen time) and the risk of the frailty index (Figure 1).
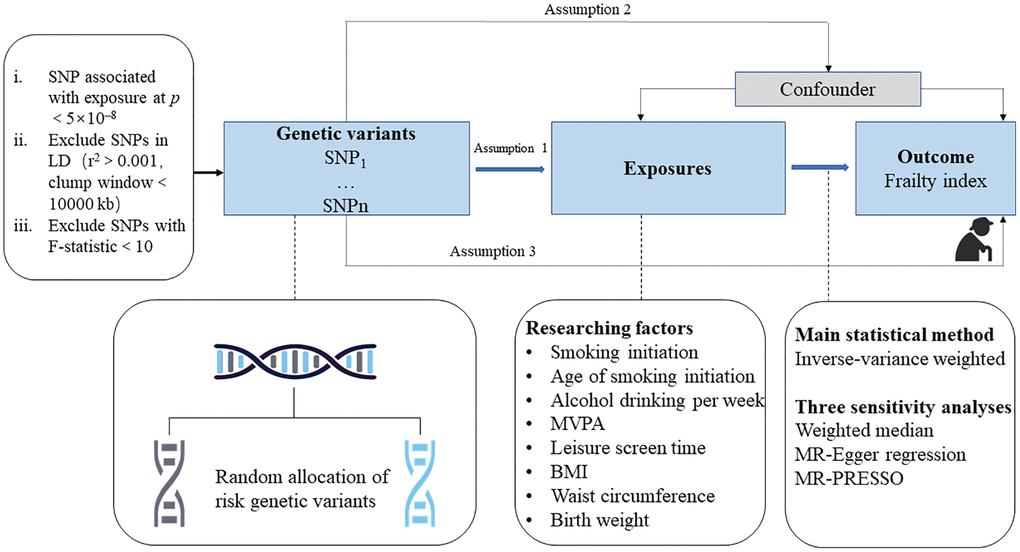
Figure 1. Study design overview. Abbreviations: SNP: single-nucleotide polymorphisms; LD: linkage disequilibrium; BMI: body mass index; MR-PRESSO: Mendelian randomization pleiotropy residual sum and outlier.
Results
According to the inverse-variance weighted (IVW) method, the principal statistical method, highly genetically predicted smoking initiation, longer leisure screen time, higher BMI and waist circumference were associated with an elevated risk of frailty (Figure 2). The β of the frailty index was 0.15 (95% confidence interval (CI), 0.10, 0.21; p = 3.88 × 10−9) for 1-standard deviation (SD) increase in the prevalence of smoking initiation, 0.19 (95% CI, 0.14, 0.24; p = 3.54 × 10−15) for 1-SD increase in leisure screen time, 0.13 (95% CI, 0.08, 0.18; p = 5.26 × 10−7) for 1-SD increase in BMI and 0.13 (95% CI, 0.06, 0.20; p = 1.80 × 10−4) for 1-SD increase in waist circumference. There was a suggestive association between genetically predicted higher birth weight (β for per 1-SD increase, −0.05, 95% CI, −0.10, −4.10 × 10−3; p = 0.03) and MVPA (β, −0.17, 95% CI, −0.32, −0.02; p = 0.03) with the risk of the frailty index. We observed no causal association between genetically predicted age of smoking initiation (β, −0.23, 95% CI, −0.53, 0.08; p = 0.14) and alcoholic drinks per week (β, 0.01, 95% CI, −0.09, 0.11; p = 0.89) with frailty index. In the three sensitivity analyses performed, the weighted median method and Mendelian randomization pleiotropy residual sum and outlier (MR-PRESSO) method remained completely consistent with the IVW method, with the MR-Egger regression method having a slightly different effect (Table 1).
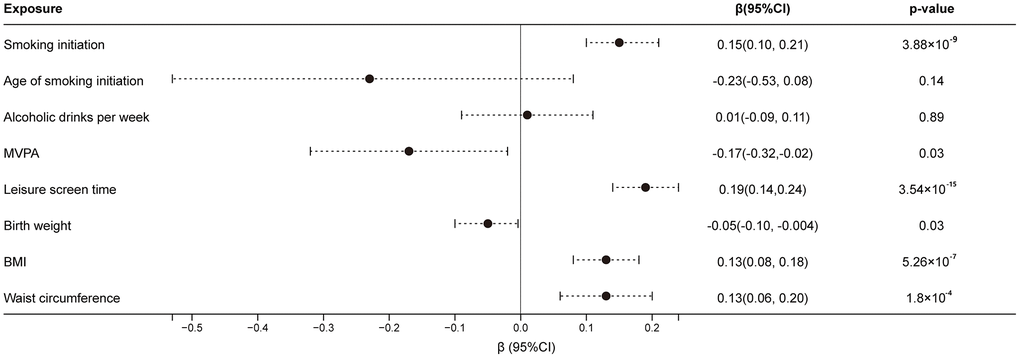
Figure 2. Associations of genetically predicted factors with the risk of frailty index. Estimates were obtained from the inverse-variance weighted method with random-effects. Abbreviations: CI: confidence interval; MVPA: moderate-to-vigorous intensity physical activity; BMI: body mass index.
Table 1. Association of genetically predicted risk factors with frailty index in MR sensitivity analysis.
| Risk factors | Cochrane’s Q | Ppleiotropya | Pdistortionb | MR-Egger | Weighted median | MR-PRESSO | Outliers | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β | 95% CI | p | β | 95% CI | p | β | 95% CI | p | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking initiation | 234.45 | 0.73 | 0.83 | 0.11 | −0.15, 0.37 | 0.42 | 0.13 | 0.07, 0.18 | 4.79 × 10−6 | 0.14 | 0.09, 0.20 | 2.06 × 10−7 | 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age of smoking initiation | 27.13 | 0.55 | 0.19 | 0.09 | −0.92, 1.11 | 0.87 | −0.08 | −0.30, 0.14 | 0.47 | −0.23 | −0.53, 0.08 | 0.19 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcoholic drinks per week | 74.60 | 0.69 | 0.02 | 0.03 | −0.14, 0.20 | 0.69 | 0.06 | −0.04, 0.16 | 0.27 | 3.53 × 10−3 | −0.10, 0.10 | 0.95 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MVPA | 17.76 | 0.97 | 0.92 | −0.15 | −0.87, 0.56 | 0.69 | −0.17 | −0.29, −0.04 | 8.26 × 10−3 | −0.17 | −0.26, −0.08 | 0.02 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leisure screen time | 135.00 | 0.77 | NA | 0.16 | −0.06, 0.38 | 0.15 | 0.15 | 0.09, 0.20 | 9.68 × 10−8 | 0.19 | 0.14, 0.24 | 4.96 × 10−11 | 0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Birth weight | 71.05 | 0.96 | 0.20 | −0.06 | −0.22, 0.11 | 0.51 | −0.04 | −0.09, 0.02 | 0.21 | −0.05 | −0.10, −0.01 | 0.03 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 153.86 | 0.21 | 0.90 | 0.04 | −0.11, 0.19 | 0.61 | 0.12 | 0.07, 0.17 | 6.54 × 10−6 | 0.12 | 0.07, 0.16 | 3.56 × 10−6 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist circumference | 111.35 | 0.80 | 0.35 | 0.10 | −0.15, 0.35 | 0.43 | 0.12 | 0.05, 0.18 | 3.49 × 10−4 | 0.12 | 0.06, 0.19 | 4.06 × 10−4 | 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: MVPA: moderate-to-vigorous intensity physical activity; BMI: body mass index; CI: confidence interval; NA: not available. Ppleiotropya is the p values for MR-Egger intercept test and p value < 0.05 indicates a significant horizontal pleiotropy. Pdistortionb is the p values obtained from MR-PRESSO distortion test and p value < 0.05 indicates a significant difference between estimates before and after outliers removal. Pdistortion for leisure screen time was not available because of no outliers detected. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The F statistics for instrumental variants are shown in Table 2. They were all over 10, indicating the strong instrument strength of the single-nucleotide polymorphisms (SNPs) used. Horizontal pleiotropy of all the SNPs was not detected in the MR-Egger analysis (all of the p-values for intercept >0.05). Zero to six outliers were observed in MR-PRESSO analysis; however, the association of each exposure (except alcoholic drinks per week) with the frailty index remained consistent after the removal of the related outliers, and no difference was observed in estimates before and after removing outliers (p for distortion test >0.05) (Table 1).
Table 2. Detail information of corresponding studies.
| Exposure or outcome | Unit | Participants included in analysis | Adjustment | SNPs (selected instrumental variants) | F-statistic | PubMed ID | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking initiation | SD in prevalence of smoking initiation | 311,629 ever smokers and 321,173 never smokers of European-descent | Age, sex, and the first ten genetic principal components | 93 | 30–145 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age of smoking initiation | SD | 341,427 European-descent individuals | Age, sex, and the first ten genetic principal components | 7 | 31–53 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcoholic drinks per week | SD | 335,394 European-descent individuals | Age, sex, and the first ten genetic principal components | 35 | 30–927 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MVPA | Dichotomous outcome (defined as at least 30 min per week of MVPA yes/no) | 703,901 individuals (94.0% European, 2.1% African, 0.8% East Asian, 1.3% South Asian ancestries, and 1.9% Hispanic) | Age, sex and the first ten genetic principal components | 9 | 31–91 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leisure screen time | SD | 703,901 individuals (94.0% European, 2.1% African, 0.8% East Asian, 1.3% South Asian ancestries, and 1.9% Hispanic) | Age, sex and the first ten genetic principal components | 89 | 27–111 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Birth weight | SD | 143,677 European-descent individuals | Gestational age | 50 | 30–180 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | SD (>30 kg/m2) | 322,154 European-descent individuals | Age, age squared, sex, and the first four genetic principal components | 69 | 29–696 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist circumference | SD | 210,088 European-descent individuals | Age, age squared, and sex | 42 | 29–447 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Frailty index | SD | 164,610 UK Biobank participants and 84,819 TwinGene participants of European descent | Age, sex, and the first ten genetic principal components | − | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: SNPs: single-nucleotide polymorphisms; ID: identifier; SD: standard deviation; MVPA: moderate-to-vigorous intensity physical activity during leisure time; BMI: body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
This MR analysis revealed that smoking, longer leisure screen time, overall obesity, and abdominal obesity were causally associated with the risk of frailty. Additionally, it also suggested a possible causal link between higher birth weight, physical activity, and lower risk of frailty, but there was not enough evidence to support that alcohol consumption and age of smoking initiation were correlated with frailty.
Consistent with previous observations, this MR analysis indicated that smoking was associated with increased frailty regardless of the age at which smoking started. Similarly, the Rotterdam study with 11,539 participants reported that former and never smokers had lower FI scores than current smokers [18]. The Atlantic PATH cohort, comprising 9,133 participants aged 30–74 years, observed that current smokers of both genders under 60 years were more likely to have the highest level of frailty compared to never-smokers [9]. A possible mechanism for the smoking-related development of frailty could be smoking-induced DNA methylation [19].
Observational evidence on the association between alcohol consumption and frailty risk was not completely consistent. The Atlantic PATH cohort reported that female occasional alcohol drinkers were significantly less likely to be highly frail than non-drinkers, whereas, no significant association was found in the general population [9]. Another meta-analysis study suggested that heavier alcohol consumption was associated with lower incident frailty compared with no alcohol consumption [15]. This result was consistent with the result of the Rotterdam study showing that moderate or harmful alcohol intake was associated with less frailty than low alcohol intake [18]. This might be explained by the social benefits of drinking, such as enhancing positive situations and facilitating socializing with others, or by reversed causation, as those in poorer health were expected to stop their alcohol intake. Nevertheless, a study from Brazil did not find a significant association between alcohol consumption and frailty [20], which agreed with our MR results. Given the limited data and controversial results, more standardized studies are warranted.
Few studies are focusing on the effect of screen time on frailty. Nonetheless, enough evidence has proved that physical activity can help reduce frailty levels, while sedentary behaviors will accelerate the development of frailty [13, 21]. The underlined mechanism could be explained by the effects of physical exercise on anti-oxidative stress [22], anti-inflammation [23], and insulin resistance improvement [24]. As a type of sedentary behavior, longer screen time was significantly proved to be the obvious risk of frailty in our study, which verified the results of observational studies. However, the analysis of MR only pointed out that there was a suggestive association between MVPA and frailty index. This might be because the exposure used was a dichotomous variable, which hurt statistical power.
A growing body of evidence suggests a positive association between obesity and the risk of frailty. BMI, as a measure of overall obesity, also showed this association. A cohort study followed older adults (including 8,751 men and 3,033 women) for 26 years, finding that the risk of frailty increased with each additional year of obesity (BMI ≥30 kg/m2, adjusted OR 1.04 for men and 1.07 for women) [12]. Based on the 2001–2006 National Health and Nutrition Examination Survey (NHANES) cohorts and Survey of Health, Ageing and Retirement in Europe (SHARE), participants with a BMI level of ≥25 kg/m2 were found to have a higher level of frailty compared to those with a normal BMI [25]. Recent studies also obtained similar results using BMI ≥30 kg/m2 as a criterion [25, 26]. Waist circumference, as an indicator of abdominal obesity, is another appropriate way to evaluate obesity. In a meta-analysis of 12 observational studies comprising 37,985 older people, individuals with a BMI of ≥30 kg/m2 or a higher category of waist circumference were found to have a 40% or 57% higher risk of frailty, respectively, compared to those with normal values [10]. A cohort study also found that abdominal obesity was more closely associated with the incidence of frailty than overall obesity, and older adults with large waist circumferences are more likely to be frail [27]. Our data further confirmed this causal relationship. Several underlying mechanisms might explain the association between obesity and frailty. Obesity exacerbates the age-related decline in muscle mass, strength, cognitive impairment, and physical function [28–30], thus worsening health and well-being. It was also closely associated with metabolic disorders, inflammaging, insulin resistance, and oxidative stress [28, 31, 32], all of which have been proven risk factors for frailty [28, 31, 33, 34].
Previous review articles on the association between birth weight and frailty have found generally consistent evidence [16, 35, 36]. The Helsinki Birth cohort study, which included 1078 participants, observed that a 1 kg increase in birth weight was associated with a lower relative risk ratio (RRR) of frailty (RRR = 0.40), after adjusting for age and sex [16]. Recently, this cohort confirmed that for per 1 kg greater birth weight, the increase in FI levels per year was −0.087 percentage points slower [35]. Additionally, a longitudinal cohort study found that adults born with extremely low birth weight had reduced grip strength [36], which was a significant predictor of frailty. This finding is consistent with our MR results. Future well-designed studies are needed to explain the underlying mechanism.
As the progress of population aging accelerates, frailty is becoming a heavy burden in health and economy. From what we have found, it provided more sufficient evidence about different methods to decrease the risk of frailty. Reducing the number of smokers, shortening the leisure screen time and keeping a good shape will contribute to decrease the impact of frailty and improve living quality.
There are still several limitations that need to be considered when interpreting our results. The major issue for any MR analysis is the possible effect of horizontal pleiotropy, which means that the selected genetic instrumental variants influence the outcome not only via exposure but also via other potential confounders. However, in our analysis, it is unlikely that this limitation had a significant impact on our results. Firstly, all of the p-values for detecting pleiotropy from the MR-Egger intercept test had no statistical significance (p > 0.05). Secondly, the sensitivity analysis identified a few outliers by MR-PRESSO analysis, but the causal association remained consistent even after removing these outliers. Another limitation to consider is the partial overlap in the study population between the exposure and outcome, which may weaken the power of instrumental variants and bias causal estimates. Nevertheless, all the selected SNPs were at the high genome-wide significance level, and had F-statistic over 10, suggesting that the bias caused by partial overlap could be overlooked. Furthermore, our study was limited to individuals of European descent, which decreased the population structure bias. However, this confinement may limit the generalizability of our findings to other populations. Nevertheless, our findings were generally consistent with observational studies in patients of different descents, which strengthened the universality of the results. In our study, we used leisure screen time as a proxy for sedentary activity since the available genome-wide association studies (GWASs) data on sedentary activity mainly came from the UK Biobank, which had excessive overlaps with the outcome of the frailty index. We hope newer and more comprehensive GWAS studies will emerge to address this limitation in future studies.
Methods
Study design and data sources
As shown in Figure 1, the study design overview should satisfy three assumptions: (i) the SNPs used as genetic instrumental variables should be strongly associated with exposure; (ii) the selected SNPs should not be correlated with potential confounders; and (iii) the SNPs used should affect the outcome only through the exposure, not through other alternative pathways [17]. All data in this study are based on the publicly available summary-level database from large GWASs and consortia.
Genetic instrument selection
Genetic instrumental variants associated with smoking initiation [37], age of smoking initiation [37], alcoholic drinks per week [37], MVPA [38], leisure screen time [38], birth weight [39], BMI [40], and waist circumference [40] at the genome-wide significance level (p < 5 × 10–8) were obtained from corresponding GWASs (Table 2). The analysis of MVPA and leisure screen time was partially derived from multiple descents; therefore, we removed rs2173650, rs12981974, rs142601240 and rs9903845, retaining only the relative SNPs from European descents. We estimated the linkage disequilibrium (LD) among the SNPs by using the 1000 Genomes European panel as a reference population [41]. We excluded SNPs in LD (r2 > 0.001 and clump window < 10000 kb) and retained the SNPs with the strongest correlation to the exposure. The final SNP information is given in Supplementary Tables 1–8. We used F-statistics to evaluate the instrument strength of the relationship between each genetic instrumental variant and exposure. Generally, F <10 indicates weak instrument strength [42].
Data sources for frailty index
Summary-level data on the associations of exposure-related SNPs with FI were obtained from a GWAS meta-analysis in European descent UK Biobank participants (n = 164,610, 60–70 years) and Swedish TwinGene participants (n = 10,616, 41–87 years) [43], which were available at Trait: Frailty index - IEU OpenGWAS project (mrcieu.ac.uk). FI was presented as the proportion of the sum of all deficits, which were based on 49 or 44 self-reported items on symptoms, disabilities, and diagnosed diseases for UK Biobank and TwinGene, respectively (see Supplementary Table 9 for details of the 49 items and the proportion of individuals scoring one for each item) [43]. The GWAS analysis was adjusted for age, sex, and the first ten principal components.
Statistical analysis
We applied the random-effects IVW model as our primary statistical method, which gave the most precise estimate. However, the IVW model is susceptible to pleiotropy or invalid instrument bias if any of the assumptions are violated. To enhance the robustness of our results and test for pleiotropy, we performed three sensitivity analyses: the weighted median method, MR-Egger regression, and MR-PRESSO. The weighted median method can yield consistent estimates even when up to 50% of SNPs are invalid instrumental variables [44]. MR-Egger regression can adjust for pleiotropy but has low power. We used the p value of the MR-Egger intercept to detect horizontal pleiotropy [45]. The MR-PRESSO method can detect outliers and provide an estimate after the removal of outliers. The embedded distortion test is used to detect significant differences in the causal estimates before and after outlier removal [46]. Cochrane’s Q statistic was estimated to assess the heterogeneity of SNPs used for each exposure. To adjust for multiple testing, we applied a Bonferroni-corrected, two-sided significance level of 6.25 × 10−3 (0.05 divided by 8 risk exposures). We considered associations with p-value < 6.25 × 10−3 as significant, and associations with a p-value ≥ 6.25 × 10−3 and ≤ 0.05 as suggestive. We conducted all analyses using the TwoSampleMR package (version 0.5.6) in R (version 4.3.0).
Supplementary Materials
Author Contributions
Yingzhen Gu as the first author performed the statistical analysis and wrote the manuscript. Naqiang Lv organized the study and supervised all work. Zuozhi Li collected the data and revised the manuscript. Aiming Dang interpreted the results. Wei Zhang, Jinxing Liu, Xiaorong Han, and Yifan Li were responsible for the construction of tables and figures. All authors read and approved the final manuscript.
Acknowledgments
This research was conducted based on the public database. The authors gratefully thank the UK Biobank participants and investigators for making this study available.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement
All MR analyses were conducted in a two-sample approach using publicly available summary statistics, and thus no additional ethical approval or informed consent would be required.
Funding
This work was supported by the Key Projects of the National Health Commission of China (2020-ZD13) and National Key Research and Development Program (2022YFC3602400, 2022YFC3602405).
References
- 1. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA, and Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001; 56:M146–56. https://doi.org/10.1093/gerona/56.3.m146 [PubMed]
- 2. Hoogendijk EO, Muntinga ME, van Leeuwen KM, van der Horst HE, Deeg DJ, Frijters DH, Hermsen LA, Jansen AP, Nijpels G, van Hout HP. Self-perceived met and unmet care needs of frail older adults in primary care. Arch Gerontol Geriatr. 2014; 58:37–42. https://doi.org/10.1016/j.archger.2013.09.001 [PubMed]
- 3. Kojima G, Iliffe S, Jivraj S, Walters K. Association between frailty and quality of life among community-dwelling older people: a systematic review and meta-analysis. J Epidemiol Community Health. 2016; 70:716–21. https://doi.org/10.1136/jech-2015-206717 [PubMed]
- 4. Hanlon P, Nicholl BI, Jani BD, Lee D, McQueenie R, Mair FS. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Health. 2018; 3:e323–32. https://doi.org/10.1016/S2468-2667(18)30091-4 [PubMed]
- 5. Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. ScientificWorldJournal. 2001; 1:323–36. https://doi.org/10.1100/tsw.2001.58 [PubMed]
- 6. Williams DM, Jylhävä J, Pedersen NL, Hägg S. A Frailty Index for UK Biobank Participants. J Gerontol A Biol Sci Med Sci. 2019; 74:582–7. https://doi.org/10.1093/gerona/gly094 [PubMed]
- 7. Blodgett J, Theou O, Kirkland S, Andreou P, Rockwood K. Frailty in NHANES: Comparing the frailty index and phenotype. Arch Gerontol Geriatr. 2015; 60:464–70. https://doi.org/10.1016/j.archger.2015.01.016 [PubMed]
- 8. Ramsay SE, Arianayagam DS, Whincup PH, Lennon LT, Cryer J, Papacosta AO, Iliffe S, Wannamethee SG. Cardiovascular risk profile and frailty in a population-based study of older British men. Heart. 2015; 101:616–22. https://doi.org/10.1136/heartjnl-2014-306472 [PubMed]
- 9. DeClercq V, Duhamel TA, Theou O, Kehler S. Association between lifestyle behaviors and frailty in Atlantic Canadian males and females. Arch Gerontol Geriatr. 2020; 91:104207. https://doi.org/10.1016/j.archger.2020.104207 [PubMed]
- 10. Yuan L, Chang M, Wang J. Abdominal obesity, body mass index and the risk of frailty in community-dwelling older adults: a systematic review and meta-analysis. Age Ageing. 2021; 50:1118–28. https://doi.org/10.1093/ageing/afab039 [PubMed]
- 11. Porter Starr KN, McDonald SR, Bales CW. Obesity and physical frailty in older adults: a scoping review of lifestyle intervention trials. J Am Med Dir Assoc. 2014; 15:240–50. https://doi.org/10.1016/j.jamda.2013.11.008 [PubMed]
- 12. Landré B, Czernichow S, Goldberg M, Zins M, Ankri J, Herr M. Association Between Life-Course Obesity and Frailty in Older Adults: Findings in the GAZEL Cohort. Obesity (Silver Spring). 2020; 28:388–96. https://doi.org/10.1002/oby.22682 [PubMed]
- 13. da Silva VD, Tribess S, Meneguci J, Sasaki JE, Garcia-Meneguci CA, Carneiro JAO, Virtuoso JS
Jr . Association between frailty and the combination of physical activity level and sedentary behavior in older adults. BMC Public Health. 2019; 19:709. https://doi.org/10.1186/s12889-019-7062-0 [PubMed] - 14. Blodgett J, Theou O, Kirkland S, Andreou P, Rockwood K. The association between sedentary behaviour, moderate-vigorous physical activity and frailty in NHANES cohorts. Maturitas. 2015; 80:187–91. https://doi.org/10.1016/j.maturitas.2014.11.010 [PubMed]
- 15. Kojima G, Liljas A, Iliffe S, Jivraj S, Walters K. A systematic review and meta-analysis of prospective associations between alcohol consumption and incident frailty. Age Ageing. 2018; 47:26–34. https://doi.org/10.1093/ageing/afx086 [PubMed]
- 16. Haapanen MJ, Perälä MM, Salonen MK, Kajantie E, Simonen M, Pohjolainen P, Eriksson JG, von Bonsdorff MB. Early life determinants of frailty in old age: the Helsinki Birth Cohort Study. Age Ageing. 2018; 47:569–75. https://doi.org/10.1093/ageing/afy052 [PubMed]
- 17. Grover S. Mendelian Randomization: Methods for Using Genetic Variants in Causal Estimation. S. Burgess and S. G. Thompson (2015). London, UK: Chapman & Hall/CRC Press. 224 pages, ISBN: 9781466573178. Biom J. 2017; 59:1086–87. https://doi.org/10.1002/bimj.201700051
- 18. Brinkman S, Voortman T, Kiefte-de Jong JC, van Rooij FJA, Ikram MA, Rivadeneira F, Franco OH, Schoufour JD. The association between lifestyle and overall health, using the frailty index. Arch Gerontol Geriatr. 2018; 76:85–91. https://doi.org/10.1016/j.archger.2018.02.006 [PubMed]
- 19. Gao X, Zhang Y, Saum KU, Schöttker B, Breitling LP, Brenner H. Tobacco smoking and smoking-related DNA methylation are associated with the development of frailty among older adults. Epigenetics. 2017; 12:149–56. https://doi.org/10.1080/15592294.2016.1271855 [PubMed]
- 20. Santiago LM, Gobbens RJJ, Mattos IE, Ferreira DB. A comparison between physical and biopsychosocial measures of frailty: Prevalence and associated factors in Brazilian older adults. Arch Gerontol Geriatr. 2019; 81:111–8. https://doi.org/10.1016/j.archger.2018.12.003 [PubMed]
- 21. Angulo J, El Assar M, Álvarez-Bustos A, Rodríguez-Mañas L. Physical activity and exercise: Strategies to manage frailty. Redox Biol. 2020; 35:101513. https://doi.org/10.1016/j.redox.2020.101513 [PubMed]
- 22. Mota MP, Dos Santos ZA, Soares JFP, de Fátima Pereira A, João PV, O'Neil Gaivão I, Oliveira MM. Intervention with a combined physical exercise training to reduce oxidative stress of women over 40 years of age. Exp Gerontol. 2019; 123:1–9. https://doi.org/10.1016/j.exger.2019.05.002 [PubMed]
- 23. Monteiro-Junior RS, de Tarso Maciel-Pinheiro P, da Matta Mello Portugal E, da Silva Figueiredo LF, Terra R, Carneiro LSF, Rodrigues VD, Nascimento OJM, Deslandes AC, Laks J. Effect of Exercise on Inflammatory Profile of Older Persons: Systematic Review and Meta-Analyses. J Phys Act Health. 2018; 15:64–71. https://doi.org/10.1123/jpah.2016-0735 [PubMed]
- 24. Ha MS, Son WM. Combined exercise is a modality for improving insulin resistance and aging-related hormone biomarkers in elderly Korean women. Exp Gerontol. 2018; 114:13–8. https://doi.org/10.1016/j.exger.2018.10.012 [PubMed]
- 25. Jayanama K, Theou O, Godin J, Mayo A, Cahill L, Rockwood K. Relationship of body mass index with frailty and all-cause mortality among middle-aged and older adults. BMC Med. 2022; 20:404. https://doi.org/10.1186/s12916-022-02596-7 [PubMed]
- 26. Ting MJM, Hyde Z, Flicker L, Almeida OP, Golledge J, Hankey GJ, Yeap BB. Associations between diabetes, body mass index and frailty: The Western Australian Health In Men Study. Maturitas. 2022; 161:58–64. https://doi.org/10.1016/j.maturitas.2022.02.008 [PubMed]
- 27. Liao Q, Zheng Z, Xiu S, Chan P. Waist circumference is a better predictor of risk for frailty than BMI in the community-dwelling elderly in Beijing. Aging Clin Exp Res. 2018; 30:1319–25. https://doi.org/10.1007/s40520-018-0933-x [PubMed]
- 28. Kalinkovich A, Livshits G. Sarcopenic obesity or obese sarcopenia: A cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res Rev. 2017; 35:200–21. https://doi.org/10.1016/j.arr.2016.09.008 [PubMed]
- 29. Tomlinson DJ, Erskine RM, Morse CI, Winwood K, Onambélé-Pearson G. The impact of obesity on skeletal muscle strength and structure through adolescence to old age. Biogerontology. 2016; 17:467–83. https://doi.org/10.1007/s10522-015-9626-4 [PubMed]
- 30. Miller AA, Spencer SJ. Obesity and neuroinflammation: a pathway to cognitive impairment. Brain Behav Immun. 2014; 42:10–21. https://doi.org/10.1016/j.bbi.2014.04.001 [PubMed]
- 31. Ferrucci L, Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol. 2018; 15:505–22. https://doi.org/10.1038/s41569-018-0064-2 [PubMed]
- 32. Ahmed B, Sultana R, Greene MW. Adipose tissue and insulin resistance in obese. Biomed Pharmacother. 2021; 137:111315. https://doi.org/10.1016/j.biopha.2021.111315 [PubMed]
- 33. Arauna D, García F, Rodríguez-Mañas L, Marrugat J, Sáez C, Alarcón M, Wehinger S, Espinosa-Parrilla Y, Palomo I, Fuentes E. Older adults with frailty syndrome present an altered platelet function and an increased level of circulating oxidative stress and mitochondrial dysfunction biomarker GDF-15. Free Radic Biol Med. 2020; 149:64–71. https://doi.org/10.1016/j.freeradbiomed.2020.01.007 [PubMed]
- 34. Clegg A, Hassan-Smith Z. Frailty and the endocrine system. Lancet Diabetes Endocrinol. 2018; 6:743–52. https://doi.org/10.1016/S2213-8587(18)30110-4 [PubMed]
- 35. Haapanen MJ, Jylhävä J, Kortelainen L, Mikkola TM, Salonen M, Wasenius NS, Kajantie E, Eriksson JG, von Bonsdorff MB. Early-Life Factors as Predictors of Age-Associated Deficit Accumulation Across 17 Years From Midlife Into Old Age. J Gerontol A Biol Sci Med Sci. 2022; 77:2281–7. https://doi.org/10.1093/gerona/glac007 [PubMed]
- 36. Morrison KM, Gunn E, Guay S, Obeid J, Schmidt LA, Saigal S. Grip strength is lower in adults born with extremely low birth weight compared to term-born controls. Pediatr Res. 2021; 89:996–1003. https://doi.org/10.1038/s41390-020-1012-5 [PubMed]
- 37. Liu M, Jiang Y, Wedow R, Li Y, Brazel DM, Chen F, Datta G, Davila-Velderrain J, McGuire D, Tian C, Zhan X, Choquet H, Docherty AR, et al, and 23andMe Research Team, and HUNT All-In Psychiatry. Association studies of up to 1.2 million individuals yield new insights into the genetic etiology of tobacco and alcohol use. Nat Genet. 2019; 51:237–44. https://doi.org/10.1038/s41588-018-0307-5 [PubMed]
- 38. Wang Z, Emmerich A, Pillon NJ, Moore T, Hemerich D, Cornelis MC, Mazzaferro E, Broos S, Ahluwalia TS, Bartz TM, Bentley AR, Bielak LF, Chong M, et al, and Lifelines Cohort Study. Genome-wide association analyses of physical activity and sedentary behavior provide insights into underlying mechanisms and roles in disease prevention. Nat Genet. 2022; 54:1332–44. https://doi.org/10.1038/s41588-022-01165-1 [PubMed]
- 39. Horikoshi M, Beaumont RN, Day FR, Warrington NM, Kooijman MN, Fernandez-Tajes J, Feenstra B, van Zuydam NR, Gaulton KJ, Grarup N, Bradfield JP, Strachan DP, Li-Gao R, et al, and CHARGE Consortium Hematology Working Group, and Early Growth Genetics (EGG) Consortium. Genome-wide associations for birth weight and correlations with adult disease. Nature. 2016; 538:248–52. https://doi.org/10.1038/nature19806 [PubMed]
- 40. Locke AE, Kahali B, Berndt SI, Justice AE, Pers TH, Day FR, Powell C, Vedantam S, Buchkovich ML, Yang J, Croteau-Chonka DC, Esko T, Fall T, et al, and LifeLines Cohort Study, and ADIPOGen Consortium, and AGEN-BMI Working Group, and CARDIOGRAMplusC4D Consortium, and CKDGen Consortium, and GLGC, and ICBP, and MAGIC Investigators, and MuTHER Consortium, and MIGen Consortium, and PAGE Consortium, and ReproGen Consortium, and GENIE Consortium, and International Endogene Consortium. Genetic studies of body mass index yield new insights for obesity biology. Nature. 2015; 518:197–206. https://doi.org/10.1038/nature14177 [PubMed]
- 41. Clarke L, Zheng-Bradley X, Smith R, Kulesha E, Xiao C, Toneva I, Vaughan B, Preuss D, Leinonen R, Shumway M, Sherry S, Flicek P, and 1000 Genomes Project Consortium. The 1000 Genomes Project: data management and community access. Nat Methods. 2012; 9:459–62. https://doi.org/10.1038/nmeth.1974 [PubMed]
- 42. Burgess S, Thompson SG, and CRP CHD Genetics Collaboration. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011; 40:755–64. https://doi.org/10.1093/ije/dyr036 [PubMed]
- 43. Atkins JL, Jylhävä J, Pedersen NL, Magnusson PK, Lu Y, Wang Y, Hägg S, Melzer D, Williams DM, Pilling LC. A genome-wide association study of the frailty index highlights brain pathways in ageing. Aging Cell. 2021; 20:e13459. https://doi.org/10.1111/acel.13459 [PubMed]
- 44. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet Epidemiol. 2016; 40:304–14. https://doi.org/10.1002/gepi.21965 [PubMed]
- 45. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015; 44:512–25. https://doi.org/10.1093/ije/dyv080 [PubMed]
- 46. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018; 50:693–8. https://doi.org/10.1038/s41588-018-0099-7 [PubMed]