



Introduction
Oral cavity cancer, one kind of head and neck cancer, is also one of the most aggressive malignant tumors in the world, with more than 350,000 new cases and over 170,000 deaths in 2018 [1]. The most common histological type of oral cavity cancer is oral squamous cell carcinoma (OSCC), which accounts for more than 90% of cases [2], and the estimated 5-year survival rate of OSCC patients is only 50% [3]. OSCC is the fourth most common cancer in the male population of Taiwan, and the buccal mucosa is the dominant subsite of OSCC due to high betel-quid-chewing rates [4]. Although the combined effects of genetic changes and multiple environmental risk factors were known to trigger OSCC, the causes of OSCC are very complex and a definitive tumorigenesis pathway is yet undefined. Thus, novel predictors for OSCC progression and prognosis, and targets for OSCC therapy still need to be discovered.
Cell proliferation is critical for tumor development and progression, and histamine is a major mediator of these biological processes in different types of cancers [5]. Histamine performs its functions via four histamine receptor subtypes, including histamine receptor H1~H4 (HRH1~HRH4) that belong to the family of G-protein-coupled receptors. Some studies indicated the relevance of histamine receptors to oral potentially malignant disorders (OPMDs) or OSCC. For example, HRH1 was reported to be expressed in OPMDs as well as the BICR56 and BICR3 OSCC cell lines. In OSCC patients, the high HRH1 level was correlated with poor disease-free survival, thus indicating the oncogenic role of HRH1 in OSCC [6, 7]. Parihar et al. indicated that HRH2 level was upregulated in tumor tissues compared to adjacent non-tumor tissues in in vivo oral cancer model. They further found that conjugation of histamine with chlorin p6 (Cp6) enhanced cellular uptake and photo toxicity of Cp6 for OSCC [8]. Moreover, HRH2 antagonist treatment in patients with head and neck squamous cell carcinomas (HNSCCs) had significantly better overall survival [9]. HRH4 is expressed by normal oral epithelial cells and is diminished in OSCC, and level of HRH4 was negatively correlated with the OSCC histopathological grade [10]. Taken together, downregulated levels of HRH4 together with upregulated levels of HRH1 and HRH2 may play critical roles in tumorigenesis of oral cancer.
Single nucleotide polymorphisms (SNPs) were identified within genes encoding HRHs, and their associations with several diseases including cancers were documented. For example, the GG genotype of rs2607474 (-1018-G/A) in HRH2 was found to be associated with atrophy of gastric mucosal and the subsequent development of gastric cancer [11]. Moreover, SNPs rs623590, rs11662595, and rs1421125 of HRH4 were significantly associated with the susceptibility and malignancy of breast cancer. Subjects harboring the rs623590 T allele and rs1421125 A allele respectively had a decreased and an increased risk of developing breast cancer. Furthermore, the haplotype of rs623590-rs11662595-rs1421125 (C-A-A) was found to correlate with risk of breast cancer [12]. Until now, HRH1 SNP rs346074 was reported to be associated with the treatment efficiency of psychiatric disorders such as bipolar I depression [13]. Moreover, HRH1 rs901865 SNP was shown to be associated with severe side effect after desloratadine treatment in patients with chronic spontaneous urticarial [14]. Furthermore, Klepstad et al. investigated the impact of HRH1 SNPs (rs2606731, rs346076, and rs901865) on opioid efficacy in cancer patients [15]. However, compared to the other HRH family members, the impacts of HRH1 SNPs in cancers have been less well investigated. We hypothesized that functional SNPs of HRH1 might influence the incidence or progression of OSCC. Therefore, we tried to identify the roles of HRH1 SNPs in the susceptibility and clinical features of OSCC from a Taiwanese population.
Results
General characteristics of study subjects
Table 1 summarizes the basic information including clinicopathological and lifestyle characteristics of all recruited participants. Age frequencies showed no obvious differences between the control and case groups. Compared to the control group, significantly higher frequencies (p<0.001) of alcohol consumption, betel-quid chewing, and cigarette smoking were observed in OSCC patients, and these lifestyle characteristics were consistent with Asian OSCC patients reported previously [16, 17], indicating that these lifestyle characteristics should be risk factors of OSCC. The majority of recruited OSCC patients had no lymph node (65.7%) or distal metastasis (99.2%) with moderately/poorly differentiated tumors (85.8%).
Table 1. Distributions of demographic characteristics of 1189 controls and 1184 male patients with oral cancer.
| Variable | Controls (N=1189) | Patients (N=1184) | p value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤55 | 605 (50.9%) | 591 (49.9%) | 0.638 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >55 | 584 (49.1%) | 593 (50.1%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Betel-quid chewing | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 993 (83.5%) | 311 (26.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 196 (16.5%) | 873 (73.7%) | <0.001* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cigarette smoking | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 560 (47.1%) | 188 (15.9%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 629 (52.9%) | 996 (84.1%) | <0.001* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcohol consumption | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 954 (80.2%) | 633 (53.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 235 (19.8%) | 551 (46.5%) | <0.001* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I+II | 558 (47.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III+IV | 626 (52.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor T status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1+T2 | 583 (49.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3+T4 | 601 (50.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lymph node status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | 778 (65.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1+N2+N3 | 406 (34.3%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M0 | 1174 (99.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M1 | 10 (0.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiation | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Well differentiated | 168 (14.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderately or poorly differentiated | 1016 (85.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The Mann-Whitney U-test or Fisher’s exact test was used to compare healthy controls and patients with oral cancer. * A p value of <0.05 was statistically significant. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Associations of HRH1 SNPs with OSCC susceptibility
Relationships of four loci of HRH1 with OSCC susceptibility are presented in Table 2. The four HRH1 polymorphisms in control group were consistent with Hardy-Weinberg equilibrium (HWE) (χ2 value=0.26, p=0.61 for rs346074 C>T, χ2 value=0.25, p=0.62 for rs346076 T>C, χ2 value=0.003, p=0.96 for rs901865 C>T, and χ2 value=0.10, p=0.75 for rs2606731 C>A). Multiple logistic regression models were used to estimate adjusted odds ratios (AORs) (with 95% confidence intervals (CIs)) after adjusting for other variables. We observed no associations between HRH1 SNPs and OSCC susceptibility in recruited Taiwanese population, as calculated either by a dominant model or a codominant model (Table 2).
Table 2. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) of oral cancer associated with histamine receptor H1 (HRH1) genotypic frequencies.
| Variable | Controls (N=1189) (%) | Patients (N=1184) (%) | AOR (95% CI) | p | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs346074 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 502 (42.2%) | 501 (42.3%) | 1.000 (reference) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CT | 535 (45.0%) | 536 (45.3%) | 1.061 (0.858~1.313) | 0.584 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | 152 (12.8%) | 147 (12.4%) | 0.959 (0.695~1.322) | 0.797 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CT+TT | 687 (57.8%) | 683 (57.7%) | 1.038 (0.849~1.270) | 0.716 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs346076 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | 471 (39.6%) | 470 (39.7%) | 1.000 (reference) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC | 561 (47.2%) | 555 (46.9%) | 1.043 (0.842~1.293) | 0.698 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 157 (13.2%) | 159 (13.4%) | 0.936 (0.682~1.284) | 0.680 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC+CC | 718 (60.4%) | 714 (60.3%) | 1.019 (0.831~1.249) | 0.858 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs901865 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 1038 (87.3%) | 1018 (86.0%) | 1.000 (reference) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CT | 146 (12.3%) | 156 (13.2%) | 1.340 (0.996~1.804) | 0.053 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | 5 (0.4%) | 10 (0.8%) | 1.242 (0.324~4.761) | 0.752 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CT+TT | 151 (12.7%) | 166 (14.0%) | 1.336 (0.998~1.789) | 0.051 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs2606731 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 582 (49.0%) | 592 (50.0%) | 1.000 (reference) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CA | 503 (42.3%) | 489 (41.3%) | 0.963 (0.781~1.186) | 0.721 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 104 (8.7%) | 103 (8.7%) | 0.817 (0.565~1.179) | 0.280 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CA+AA | 607 (51.0%) | 592 (50.0%) | 0.936 (0.767~1.142) | 0.514 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AORs with their 95% CIs were estimated by logistic regression models. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Associations between HRH1 genetic variants and clinicopathological characteristics in patients with OSCC
Next, we assessed whether HRH1 gene polymorphisms were connected to OSCC clinicopathologic features including the primary tumor size, clinical stage, histopathologic grade, and tumor metastatic statuses (Table 3). We observed that OSCC patients harboring one minor allele (CT or TT) of rs346074 showed a significantly lower risk to develop larger tumor sizes (>T2) (AOR: 0.790-fold; 95% CI: 0.626~0.997; p=0.048) compared to patients harboring the wild-type (WT) homozygotes (CC). OSCC patients with the CT or TT genotype of rs901865 also showed a lower risk of developing larger tumor sizes (AOR: 0.714-fold; 95% CI: 0.512~0.997; p=0.048). In addition to tumor size, no significant association was observed for histological grade, tumor metastasis, or clinical stage of OSCC.
Table 3. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) of clinical statuses associated with genotypic frequencies of histamine receptor H1 (HRH1) rs901865 and rs346074 in male oral cancer patients.
| Variable | rs901865 | rs346074 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC (N=1018) | CT+TT (N=166) | AOR (95% CI)a | p value | CC (N=501) | CT+TT (N=683) | AOR (95% CI) | p value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage I+II | 470 (46.2%) | 88 (53.0%) | 1.000 (reference) | 0.086 | 238 (47.5%) | 320 (46.8%) | 1.000 (reference) | 0.769 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage III+IV | 548 (53.8%) | 78 (47.0%) | 0.748 (0.537~1.042) | 263 (52.5%) | 363 (53.2%) | 1.035 (0.821~1.306) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤T2 | 490 (48.1%) | 93 (56.0%) | 1.000 (reference) | 0.048 | 231 (46.1%) | 352 (51.5%) | 1.000 (reference) | 0.048 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >T2 | 528 (51.9%) | 73 (44.0%) | 0.714 (0.512~0.997) | 270 (53.9%) | 331 (48.5%) | 0.790 (0.626~0.997) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lymph node metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 667 (65.5%) | 111 (66.9%) | 1.000 (reference) | 0.620 | 336 (67.1%) | 442 (64.7%) | 1.000 (reference) | 0.328 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 351 (34.5%) | 55 (33.1%) | 0.915 (0.644~1.300) | 165 (32.9%) | 241 (35.3%) | 1.130 (0.884~1.444) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M0 | 1009 (99.1%) | 165 (99.4%) | 1.000 (reference) | 0.639 | 497 (99.2%) | 677 (99.1%) | 1.000 (reference) | 0.836 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M1 | 9 (0.9%) | 1 (0.6%) | 0.607 (0.075~4.880) | 4 (0.8%) | 6 (0.9%) | 1.144 (0.320~4.092) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiated grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Well | 143 (14.0%) | 25 (15.1%) | 1.000 (reference) | 0.573 | 68 (13.6%) | 100 (14.6%) | 1.000 (reference) | 0.602 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderately or poorly | 875 (86.0%) | 141 (84.9%) | 0.875 (0.550~1.392) | 433 (86.4%) | 583 (85.4%) | 0.915 (0.655~1.277) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiate grade: grade I, well differentiated; grade II, moderately differentiated; grade III, poorly differentiated. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aThe AORs with their 95% CIs were estimated by multiple logistic regression models after controlling for age, betel-quid chewing, cigarette smoking, and alcohol consumption. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Combined and interactive effects of HRH1 SNPs and betel-quid chewing on OSCC progression
In East Asia, including Taiwan, betel-quid chewing is already known to be a dominant risk factor for OSCC and has been correlated with poor survival of OSCC patients [18–20]. Herein, we separated the recruited patients into subpopulation patients with and without betel-quid-chewing habits, and further investigated differences between HRH1 SNPs and the OSCC clinicopathological features in these two subpopulations. The significantly lower risk of developing an advanced clinical (III+IV) stage was observed in OSCC patients who chewed betel quid and also carried at least one polymorphic T allele of rs901865 (AOR: 0.614-fold; 95% CI: 0.408~0.924; p=0.020) (Table 4). In contrast, in subpopulation patients without the habit of betel-quid-chewing, the protective effect of rs901865 polymorphisms was not observed (Table 5). Taken together, our results indicated that a potential interaction between the existence of at least one minor allele of an HRH1 rs901865 SNP and betel-quid chewing was shown to be associate with OSCC progression.
Table 4. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) of clinical statuses associated with genotypic frequencies of histamine receptor H1 (HRH1) rs901865 in betel-quid chewers.
| Variable | Betel-quid chewers (N=873) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC (N=764) | CT+TT (N=109) | AOR (95% CI)a | p value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage I+II | 354 (46.3%) | 64 (58.7%) | 1.000 (reference) | 0.020 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage III+IV | 410 (53.7%) | 45 (41.3%) | 0.614 (0.408~0.924) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤T2 | 376 (49.2%) | 63 (57.8%) | 1.000 (reference) | 0.131 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >T2 | 388 (50.8%) | 46 (42.2%) | 0.730 (0.485~1.098) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lymph node metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 503 (65.8%) | 79 (72.5%) | 1.000 (reference) | 0.163 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 261 (34.2%) | 30 (27.5%) | 0.726 (0.463~1.139) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M0 | 757 (99.1%) | 109 (100.0%) | - | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M1 | 7 (0.9%) | 0 (0.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiated grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Well | 120 (15.7%) | 16 (14.7%) | 1.000 (reference) | 0.740 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderately or poorly | 644 (84.3%) | 93 (85.3%) | 1.101 (0.624~1.943) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiate grade: grade I, well differentiated; grade II, moderately differentiated; grade III, poorly differentiated. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aThe AORs with their 95% CIs were estimated by multiple logistic regression models after controlling for age, cigarette smoking, and alcohol consumption. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 5. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) of clinical statuses associated with genotypic frequencies of histamine receptor H1 (HRH1) rs901865 in non-betel-quid chewers.
| Variable | Non-betel-quid chewers (N=311) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC (N=254) | CT+TT (N=57) | AOR (95% CI)a | p value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage I+II | 116 (45.7%) | 24 (42.1%) | 1.000 (reference) | 0.582 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage III+IV | 138 (54.3%) | 33 (57.9%) | 1.179 (0.656~2.121) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤T2 | 114 (44.9%) | 30 (52.6%) | 1.000 (reference) | 0.249 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >T2 | 140 (55.1%) | 27 (47.4%) | 0.709 (0.396~1.272) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lymph node metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 164 (64.6%) | 32 (56.1%) | 1.000 (reference) | 0.189 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 90 (35.4%) | 25 (43.9%) | 1.485 (0.823~2.679) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metastasis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M0 | 252 (99.2%) | 56 (98.3%) | 1.000 (reference) | 0.412 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M1 | 2 (0.8%) | 1 (1.7%) | 2.798 (0.240~32.609) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiated grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Well | 23 (9.1%) | 9 (15.8%) | 1.000 (reference) | 0.151 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderately or poorly | 231 (90.9%) | 48 (84.2%) | 0.542 (0.235~1.251) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cell differentiate grade: grade I, well differentiated; grade II, moderately differentiated; grade III, poorly differentiated. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aThe AORs with their 95% CIs were estimated by multiple logistic regression models after controlling for age, cigarette smoking, and alcohol consumption. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Upregulation of HRH1 in OSCC tissues correlates with tumor progression and a poor prognosis
We further analyzed correlations of HRH1 expression levels and their clinical significance or survival rates in oral cancer, by examining cases of HNSCCs from The Cancer Genome Atlas (TCGA) dataset. We observed that HRH1 expression was prone to be upregulated in HNSCCs compared to noncancerous tissues (Figure 1A). To focus on OSCC, we analyzed dataset (GSE78060) from Gene Expression Omnibus (GEO) database and also found that HRH1 expression levels were significantly higher in OSCC tissues compared to normal tissues (Figure 1B). In the same GSE cohort, we observed that HRH1 transcripts were prone to be higher in OSCC patients with larger tumors (>T2 status) than in patients with smaller tumors (≤T2 status) (Figure 1C). Moreover, a Kaplan-Meier plot revealed that HNSCC patients from TCGA with HRH1high tumors had shorter overall and disease-specific survival times compared to those with HRH1low tumors (p=0.054 and 0.011; Figure 1D, left panel). Furthermore, 23 OSCC cases from the GEO database (GSE31056) were also analyzed, and shorter recurrence-free survival times was observed in patients harboring HRH1high tumors compared to those harboring HRH1low tumors (p=0.031; Figure 1D, right panel). Altogether, these data indicated that HRH1 SNPs might influence HRH1 expression and subsequently modulate OSCC progression and contribute to poor prognoses.
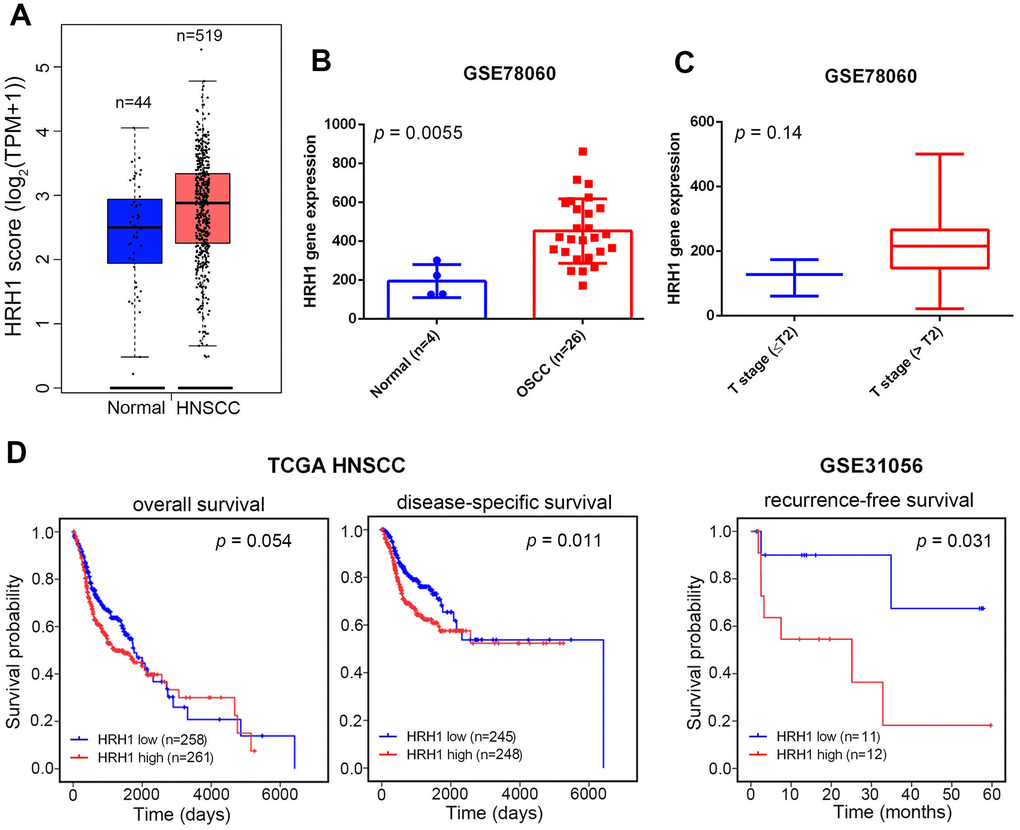
Figure 1. Clinical relevance of histamine receptor H1 (HRH1) levels in head and neck squamous cell carcinoma (HNSCC) or oral squamous cell carcinoma (OSCC) patients obtained from TCGA and GEO databases. (A, B) HRH1 expression was higher in HNSCC tissues (A) and OSCC tissues (B) than in normal tissues (database sources: TCGA and GSE78060). (C) HRH1 expression levels in OSCC from GSE78060 were compared according to the tumor size (T stages). (D) Kaplan-Meier curves for overall and disease-specific survival (left panel) and recurrence-free survival (right panel) of patients with HNSCC and OSCC, as categorized according to high or low expression of HRH1. The p value indicates a comparison between patients with HRH1high and HRH1low. (database sources: TCGA and GSE31056).
Genotype-based HRH1 expression analysis
To further investigate correlations of HRH1 rs901865 and rs346074 polymorphisms with HRH1 expression levels in OSCC, we examined rs901865 or rs346074 genotypes of five OSCC cell lines (SCC9, HSC-3, HSC-3M, SAS, and OECM1) and found that OECM1 cells carried the CT genotype of rs901865 and the TT genotype of rs346074 compared to HSC-3M, SAS, and HSC3 cells which carried the CC genotype of both SNPs (Figure 2, upper panel). Moreover, we detected HRH1 expression by two different antibodies using a Western blot analysis. Among these OSCC cell lines, we observed that OECM1 cells expressed lower HRH1 protein levels than SAS, HSC-3M, or HSC-3 cells (Figure 2, lower panel).
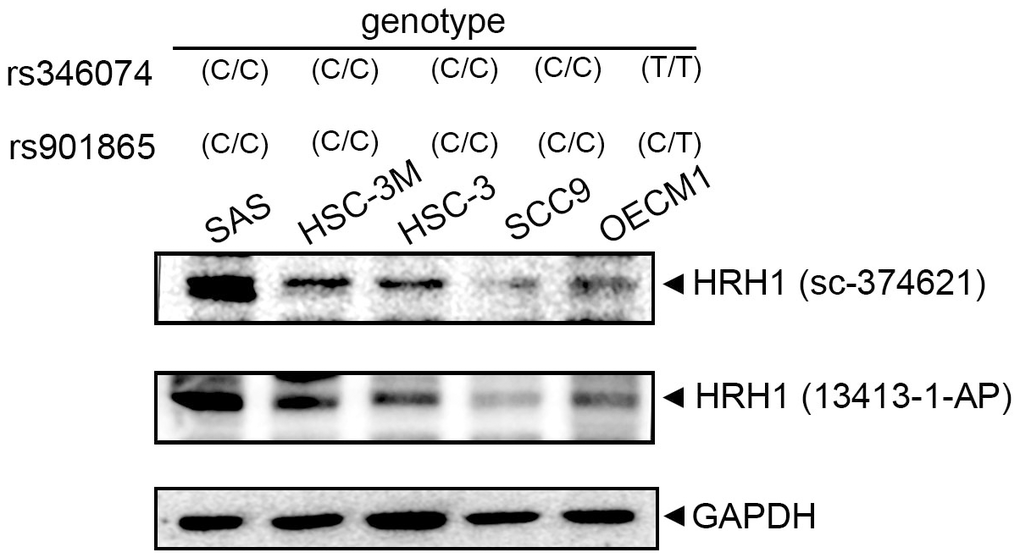
Figure 2. Correlations of histamine receptor H1 (HRH1) rs346074 and rs901865 genotypes with HRH1 protein levels in five oral squamous cell carcinoma (OSCC) cell lines. Upper panel, HRH1 rs346074 or rs901865 genotypes in OSCC cells (SAS, HSC-3M, HSC-3, SCC9, and OECM1) were detected by a TaqMan SNP Genotyping Assay. Lower panel, protein levels of HRH1 were detected by a Western blot analysis using two HRH1-specific antibodies.
Discussion
Histamine and its receptor, HRH1, are known to play important roles in many aspects of cancer development including cell proliferation [5, 21]. Recently, high expression levels of histamine or HRH1 were observed in different human cancers and were correlated with poor prognoses including in breast [22, 23], colon [24], and liver cancers [25, 26]. In the current study, we found that HRH1 was upregulated in OSCC and was correlated with larger tumor sizes and poor prognoses of OSCC patients, suggesting an oncogenic role of HRH1 in OSCC. Previous studies indicated that OSCC is a disease related to multiple gene mutations [27], and some of the gene polymorphisms were reported to be associated with OSCC risks and progression [28, 29]. Although previous reports indicated that HRH1 messenger (m)RNA expression was elevated in subjects with asthma and genetic variants of HRH1 contributed to the risk of allergic asthma [30, 31], knowledge of the clinical relevance of HRH1 SNPs in OSCC, which probably result in expression and functional changes of HRH1, is still lacking. Herein, we found for the first time that polymorphisms of the HRH1 gene play critical roles in influencing the clinicopathological characteristics of OSCC in a Taiwanese population.
Our present data indicated that patients with a mutant base T of rs346074 or rs901865 had a significantly reduced risk of developing larger tumor sizes (>T2) under a dominant model (CT+TT). Previous in vitro and in vivo investigations showed that agonists of HRH1 such as histamine significantly induced progression (growth and metastasis) of liver cancer via HRH1 which was highly expressed in liver cancer tissues [25]. Previous studies indicated that some SNPs of HRHs were shown to influence their mRNA expression levels. For example, the SNPs ss142022671 and ss142022677 of HRH4 were respectively reported to increase the HRH4 mRNA level and protein stability [32]. Actually, Li et al. indicated that Chinese patients with chronic spontaneous urticaria who harbor the HRH1 rs901865 CC polymorphism were associated with severe sedation side effects caused by desloratadine treatment. They claimed that patients harboring rs901865 CC genotype had high levels of HRH1 transcripts, which triggered serious sedation side effects [14]. In the same race, Chu also indicated that patients harboring the CC genotype of rs901865 exhibited the increased response of H1-antihistamines treatment in patients with allergic rhinitis [33]. In contrast, in African American populations with asthma, no difference in HRH1 mRNA expression was detected relative to the rs901865 genotype [34], suggesting that the HRH1 rs901865 polymorphism contributing to HRH1 gene expressions might be diverse in different races. In addition to rs901865, the rs346074 SNP located on transcription factor binding sites of the HRH1 gene may affect transcription rates [35], but the impact of rs346074 SNPs on HRH1 mRNA expression should be further investigated. Actually, our present study further examined the genotypes of rs901865 and rs346074 in five OSCC cell lines (SCC9, HSC-3, HSC-3M, SAS, and OECM1) and found that OECM1 cells carrying the rs901865 CT genotype and the rs346074 TT genotype expressed lower HRH1 protein levels compared to SAS, HSC-3, and HSC-3M cells carrying the CC genotype of both SNPs, suggesting that the T allele of rs901865 or rs346074 may produce a decrease in HRH1 levels in OSCC and subsequently cause smaller tumor sizes in OSCC patients carrying one minor allele of rs901865 or rs346074.
Because betel-quid chewing increased the risk of OPMDs and OSCC [36, 37], herein, we explored the combined effect of HRH1 SNPs and betel-quid chewing on OSCC progression. We observed that patients with one T allele of HRH1 rs901865 had a lower risk to develop an advanced clinical stage in the subpopulation of betel-quid chewers, and this phenomenon was not observed in the subpopulation who did not chew areca nut. Previous studies showed that betel-quid chewing can induce histamine release and further cause gastric hemorrhaging and mucosal ulceration in rats. Activation of HRH1 is involved in aggravating histamine-induced gastric mucosal ulceration in betel-quid-fed rats, and this phenomenon was ameliorated by treatment with the antihistamine, ketotifen [38]. We suggest that betel-quid chewing might induce upregulation of histamine in OSCC patients with a betel-quid-chewing habit and promote OSCC progression via HRH1, and the protective effect observed in OSCC patients carrying the CT/TT genotypes of HRH1 rs901865 might be due to lower expression levels of HRH1 in this subgroup.
Histamine and its receptors play critical roles in several cancer-associated processes in tumor microenvironment, where mast cells (MCs) is a major source of histamine. Previous reports indicated that numbers of MCs are higher among OPMDs and OSCC compared to normal oral mucosa [39]. The MCs mainly located at the lamina propria surrounding the tumor invasive front of OSCC. Increased MCs were also observed in hotspot microvascular density areas, suggesting MC numbers may correlate with angiogenesis [40–42]. Based on the previous studies, the upregulated levels of HRH1/HRH2 and tumor-associated MCs may play crucial roles in promoting tumorigenesis and progression of OSCC [7]. Therefore, the correlation among HRH1 SNPs, MCs infiltration, and OSCC progression will be further investigated in our future work.
Nevertheless, this study still has some limitations that need to be discussed. First, all of the subjects included in this study were Taiwanese (of Chinese ethnicity), so it is unclear whether these results can be observed in other races. Therefore, further investigations of these SNPs in different racial OSCC populations are necessary to confirm our results. Second, the sample size was not large enough, which might cause statistical impacts on the accuracy of the results. Third, the functional impacts of HRH1 SNPs on OSCC is still unclear. Moreover, we should simultaneously collect DNA and mRNA from the same samples to check the influences of HRH1 SNPs on HRH1 expression in future. Last, this study just focused on the association of HRH1 SNPs with OSCC, and the impacts of other genetic variations within the histamine pathway including those of L-histidine decarboxylase, histamine N-methyltransferase, and diamine oxidase on OSCC need to be further investigated.
In summary, our study first pointed out the diverse allelic effects of HRH1 SNPs (rs901865 and 346074) which affect the clinicopathologic features of OSCC. Moreover, the combined effect of rs901865 SNPs with betel-quid chewing was found to causally influence the development of OSCC. Our preliminary analysis indicated that the T allele of rs901865 or rs346074 may cause a decrease in HRH1 levels in OSCC cells. At present, a large proportion of OSCC patients still will develop advanced disease eventually, and the reliable tools are lacking to predict who those patients are. Our present results provide novel information for detecting high-risk populations for OSCC and formulating individualized preventive measures.
Materials and Methods
Study population selection
Between 2010 and 2021, a total of 1184 male patients diagnosed with OSCC were randomly collected from a patient database of Chung Shan Medical University Hospital (Taichung, Taiwan). In addition, 1189 anonymized healthy male controls without a history of oral precancerous disease or other cancers were randomly selected from the Taiwan Biobank Project. All study populations were Han Chinese and lived in the same geographic area. Medical information and demographic data, including age, gender, primary tumor size, the tumor, node, metastasis (TNM) clinical staging, lymph node and distal metastasis, and histologic grade, were all obtained from medical records. The protocol of this case-control study was approved by the Ethics Committee of Chung Shan Medical University Hospital (no. CS1-21151).
OSCC cell lines and culture
The human SAS, HSC-3, HSC-3M, and SCC9 OSCC cell lines were purchased from the Japanese Collection of Research Bioresources Cell Bank (JCRB, Osaka, Japan) or the American Type Culture Collection (ATCC, Manassas, VA, USA). All four of these OSCC cell lines were cultured in Dulbecco’s modified Eagle medium/nutrient mixture F-12 (DMEM/F12; Life Technologies, Grand Island, NY, USA) containing 10% fetal bovine serum (FBS) (Gibco, Grand Island, NY, USA). The OECM1 OSCC cell line derived from surgical resection of a primary tumor from a male Taiwanese patient [43] was maintained in RPMI-1640 medium (Life Technologies) with 10% FBS. All cells were maintained in an incubator (37° C, 5% CO2 and 95% air atmosphere).
DNA extraction and SNP genotyping for allelic frequencies of the HRH1 gene
Genomic DNA was isolated from peripheral blood leukocytes of all participants or OSCC cell lines using a Genomic DNA Extraction kit (Qiagen, Valencia, CA, USA) according to the manufacturer’s instructions. The DNA concentration was detected with a Nanodrop-2000 spectrophotometer (ThermoFisher Scientific, Waltham, MA, USA) and stored at -20° C before genotyping. Allelic discrimination of the four HRH1 SNPs including rs346074 (assay ID: C__26855885_10), rs346076 (assay ID: C__11984711_10), rs901865 (assay ID: C__25471612_10), and rs2606731 (assay ID: C__15902251_10), was determined by the TaqMan SNP Genotyping Assay which utilized the ABI StepOnePlus™ Real-Time PCR System (Applied Biosystems, Foster City, CA, USA) and ABI StepOnePlus™ Software (version 2.3) used to analyze the final data.
In silico expression analyses of the human HRH1 gene
The Gene Expression Profiling Interactive Analysis (GEPIA) (http://gepia.cancer-pku.cn/index.html) online database [44] is a communal network server that includes a transcriptome sequencing dataset of 9736 tumors together with 8587 adjacent normal tissues from Genotype-Tissue Expression (GTEx) and The Cancer Genome Atlas (TCGA) datasets. Herein, we compared the expression of HRH1 between HNSCC and normal tissues. Moreover, transcriptomic data of normal and OSCC tissues from an Asian population was also analyzed using the GSE78060 dataset from the GEO database (https://www.ncbi.nlm.nih.gov/geo/). The prognostic significance of HRH1 in HNSCC and OSCC was determined using a Kaplan-Meier analysis of TCGA and GEO databases, respectively.
Total protein extraction and Western blot analysis
Total cell lysate extraction was carried out and protein contents were determined as previously described [45]. A Western blot analysis was performed with primary antibodies for HRH1(sc-374621, Santa Cruz Biotechnology, Heidelberg, Germany; 13413-1-AP, Proteintech Group, Chicago, IL, USA) or GAPDH (#2118, Cell Signaling Technology, Danvers, MA, USA).
Statistical analysis
Differences in demographic parameters between OSCC patients and cancer-free controls were analyzed using the Fisher’s exact test and Mann-Whitney U-test. Using multiple logistic regression models after controlling for covariates, the AORs with their 95% CIs for the association between genotype frequencies and the OSCC risk or clinical pathological characteristics of OSCC were calculated. Statistical analysis of our data used the SAS software program (version 9.1, 2005; SAS Institute, Cary, NC, USA). A p value of <0.05 was considered significant.
Author Contributions
Y-FD, S-FY, and M-HC contributed to the concept and design, drafted the manuscript, and critically revised the manuscript; S-FY, W-KC, C-WL, and L-CC contributed to the concept, performed the experiments, and analyzed the data. Y-CY, M-HC, and J-SC performed the in silico data exploration, integration, and analysis. Y-FD and S-FY prepared all the figures and tables. All authors read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Funding
This study was supported by the TMU Research Center of Cancer Translational Medicine from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan (to M.-H. Chien) and by grant no. 110-phd-03 from Taipei Medical University-Wan Fang Hospital (to Y.-F. Ding).
References
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. https://doi.org/10.3322/caac.21492 [PubMed]
- 2. Thompson L. World Health Organization classification of tumours: pathology and genetics of head and neck tumours. Ear Nose Throat J. 2006; 85:74. [PubMed]
- 3. Argiris A, Karamouzis MV, Raben D, Ferris RL. Head and neck cancer. Lancet. 2008; 371:1695–709. https://doi.org/10.1016/S0140-6736(08)60728-X [PubMed]
- 4. Lin NC, Hsien SI, Hsu JT, Chen MYC. Impact on patients with oral squamous cell carcinoma in different anatomical subsites: a single-center study in Taiwan. Sci Rep. 2021; 11:15446. https://doi.org/10.1038/s41598-021-95007-5 [PubMed]
- 5. Massari NA, Nicoud MB, Medina VA. Histamine receptors and cancer pharmacology: an update. Br J Pharmacol. 2020; 177:516–38. https://doi.org/10.1111/bph.14535 [PubMed]
- 6. Grimm M, Krimmel M, Alexander D, Munz A, Kluba S, Keutel C, Hoffmann J, Polligkeit J, Reinert S, Hoefert S. Prognostic value of histamine H1 receptor expression in oral squamous cell carcinoma. Clin Oral Investig. 2013; 17:949–55. https://doi.org/10.1007/s00784-012-0784-3 [PubMed]
- 7. Salem A, Salo T. Nothing to sneeze at: Histamine and histamine receptors in oral carcinogenesis. Oral Dis. 2021; 27:1090–6. https://doi.org/10.1111/odi.13411 [PubMed]
- 8. Parihar A, Dube A, Gupta PK. Photodynamic treatment of oral squamous cell carcinoma in hamster cheek pouch model using chlorin p6-histamine conjugate. Photodiagnosis Photodyn Ther. 2013; 10:79–86. https://doi.org/10.1016/j.pdpdt.2012.05.005 [PubMed]
- 9. Papagerakis S, Bellile E, Peterson LA, Pliakas M, Balaskas K, Selman S, Hanauer D, Taylor JM, Duffy S, Wolf G. Proton pump inhibitors and histamine 2 blockers are associated with improved overall survival in patients with head and neck squamous carcinoma. Cancer Prev Res (Phila). 2014; 7:1258–69. https://doi.org/10.1158/1940-6207.CAPR-14-0002 [PubMed]
- 10. Salem A, Almahmoudi R, Listyarifah D, Siponen M, Maaninka K, Al-Samadi A, Salo T, Eklund KK. Histamine H4 receptor signalling in tongue cancer and its potential role in oral carcinogenesis - a short report. Cell Oncol (Dordr). 2017; 40:621–30. https://doi.org/10.1007/s13402-017-0336-6 [PubMed]
- 11. Arisawa T, Tahara T, Ozaki K, Matsue Y, Minato T, Yamada H, Nomura T, Hayashi R, Matsunaga K, Fukumura A, Nakamura M, Toshikuni N, Shiroeda H, Shibata T. Association between common genetic variant of HRH2 and gastric cancer risk. Int J Oncol. 2012; 41:497–503. https://doi.org/10.3892/ijo.2012.1482 [PubMed]
- 12. He GH, Lu J, Shi PP, Xia W, Yin SJ, Jin TB, Chen DD, Xu GL. Polymorphisms of human histamine receptor H4 gene are associated with breast cancer in Chinese Han population. Gene. 2013; 519:260–5. https://doi.org/10.1016/j.gene.2013.02.020 [PubMed]
- 13. Perlis RH, Adams DH, Fijal B, Sutton VK, Farmen M, Breier A, Houston JP. Genetic association study of treatment response with olanzapine/fluoxetine combination or lamotrigine in bipolar I depression. J Clin Psychiatry. 2010; 71:599–605. https://doi.org/10.4088/JCP.08m04632gre [PubMed]
- 14. Li J, Chen W, Peng C, Zhu W, Liu Z, Zhang W, Su J, Li J, Chen X. Human H1 receptor (HRH1) gene polymorphism is associated with the severity of side effects after desloratadine treatment in Chinese patients with chronic spontaneous uticaria. Pharmacogenomics J. 2020; 20:87–93. https://doi.org/10.1038/s41397-019-0094-0 [PubMed]
- 15. Klepstad P, Fladvad T, Skorpen F, Bjordal K, Caraceni A, Dale O, Davies A, Kloke M, Lundström S, Maltoni M, Radbruch L, Sabatowski R, Sigurdardottir V, et al, and European Palliative Care Research Collaborative (EPCRC), and the European Association for Palliative Care Research Network. Influence from genetic variability on opioid use for cancer pain: a European genetic association study of 2294 cancer pain patients. Pain. 2011; 152:1139–45. https://doi.org/10.1016/j.pain.2011.01.040 [PubMed]
- 16. Goud EVSS, Malleedi S, Ramanathan A, Wong GR, Hwei Ern BT, Yean GY, Ann HH, Syan TY, Zain RM. Association of Interleukin-10 Genotypes and Oral Cancer Susceptibility in Selected Malaysian Population: A Case- Control Study. Asian Pac J Cancer Prev. 2019; 20:935–41. https://doi.org/10.31557/APJCP.2019.20.3.935 [PubMed]
- 17. Senghore T, Chien HT, Wang WC, Chen YX, Young CK, Huang SF, Yeh CC. Polymorphisms in ERCC5 rs17655 and ERCC1 rs735482 Genes Associated with the Survival of Male Patients with Postoperative Oral Squamous Cell Carcinoma Treated with Adjuvant Concurrent Chemoradiotherapy. J Clin Med. 2019; 8:33. https://doi.org/10.3390/jcm8010033 [PubMed]
- 18. Lee YA, Li S, Chen Y, Li Q, Chen CJ, Hsu WL, Lou PJ, Zhu C, Pan J, Shen H, Ma H, Cai L, He B, et al. Tobacco smoking, alcohol drinking, betel quid chewing, and the risk of head and neck cancer in an East Asian population. Head Neck. 2019; 41:92–102. https://doi.org/10.1002/hed.25383 [PubMed]
- 19. Yang J, Wang ZY, Huang L, Yu TL, Wan SQ, Song J, Zhang BL, Hu M. Do betel quid and areca nut chewing deteriorate prognosis of oral cancer? A systematic review, meta-analysis, and research agenda. Oral Dis. 2021; 27:1366–75. https://doi.org/10.1111/odi.13456 [PubMed]
- 20. Jeng JH, Chang MC, Hahn LJ. Role of areca nut in betel quid-associated chemical carcinogenesis: current awareness and future perspectives. Oral Oncol. 2001; 37:477–92. https://doi.org/10.1016/s1368-8375(01)00003-3 [PubMed]
- 21. Bijman JT, Wagener DJ, Graafsma SJ, Wessels JM, Van den Broek P. Modulation of proliferation of a human head and neck squamous carcinoma cell line (HN-1) by catecholamines and histamine. Anticancer Res. 1987; 7:147–50. [PubMed]
- 22. Fernández-Nogueira P, Noguera-Castells A, Fuster G, Recalde-Percaz L, Moragas N, López-Plana A, Enreig E, Jauregui P, Carbó N, Almendro V, Gascón P, Bragado P, Mancino M. Histamine receptor 1 inhibition enhances antitumor therapeutic responses through extracellular signal-regulated kinase (ERK) activation in breast cancer. Cancer Lett. 2018; 424:70–83. https://doi.org/10.1016/j.canlet.2018.03.014 [PubMed]
- 23. Sieja K, Stanosz S, von Mach-Szczypiński J, Olewniczak S, Stanosz M. Concentration of histamine in serum and tissues of the primary ductal breast cancers in women. Breast. 2005; 14:236–41. https://doi.org/10.1016/j.breast.2004.06.012 [PubMed]
- 24. Shi Z, Fultz RS, Engevik MA, Gao C, Hall A, Major A, Mori-Akiyama Y, Versalovic J. Distinct roles of histamine H1- and H2-receptor signaling pathways in inflammation-associated colonic tumorigenesis. Am J Physiol Gastrointest Liver Physiol. 2019; 316:G205–16. https://doi.org/10.1152/ajpgi.00212.2018 [PubMed]
- 25. Zhao J, Hou Y, Yin C, Hu J, Gao T, Huang X, Zhang X, Xing J, An J, Wan S, Li J. Upregulation of histamine receptor H1 promotes tumor progression and contributes to poor prognosis in hepatocellular carcinoma. Oncogene. 2020; 39:1724–38. https://doi.org/10.1038/s41388-019-1093-y [PubMed]
- 26. Francis H, DeMorrow S, Venter J, Onori P, White M, Gaudio E, Francis T, Greene JF
Jr , Tran S, Meininger CJ, Alpini G. Inhibition of histidine decarboxylase ablates the autocrine tumorigenic effects of histamine in human cholangiocarcinoma. Gut. 2012; 61:753–64. https://doi.org/10.1136/gutjnl-2011-300007 [PubMed] - 27. Nakagaki T, Tamura M, Kobashi K, Koyama R, Fukushima H, Ohashi T, Idogawa M, Ogi K, Hiratsuka H, Tokino T, Sasaki Y. Profiling cancer-related gene mutations in oral squamous cell carcinoma from Japanese patients by targeted amplicon sequencing. Oncotarget. 2017; 8:59113–22. https://doi.org/10.18632/oncotarget.19262 [PubMed]
- 28. Lin T, Zhang B, He H. Identification of genes correlated with oral squamous cell carcinoma. J Cancer Res Ther. 2018 (Supplement); 14:S675–9. https://doi.org/10.4103/0973-1482.202893 [PubMed]
- 29. Ding YF, Wen YC, Chuang CY, Lin CW, Yang YC, Liu YF, Chang WM, Chang LC, Yang SF, Chien MH. Combined Impacts of Genetic Variants of Long Non-Coding RNA MALAT1 and the Environmental Carcinogen on the Susceptibility to and Progression of Oral Squamous Cell Carcinoma. Front Oncol. 2021; 11:684941. https://doi.org/10.3389/fonc.2021.684941 [PubMed]
- 30. Anvari S, Vyhlidal CA, Dai H, Jones BL. Genetic Variation along the Histamine Pathway in Children with Allergic versus Nonallergic Asthma. Am J Respir Cell Mol Biol. 2015; 53:802–9. https://doi.org/10.1165/rcmb.2014-0493OC [PubMed]
- 31. Vyhlidal CA, Riffel AK, Dai H, Rosenwasser LJ, Jones BL. Detecting gene expression in buccal mucosa in subjects with asthma versus subjects without asthma. Pediatr Allergy Immunol. 2013; 24:138–43. https://doi.org/10.1111/pai.12042 [PubMed]
- 32. Yu B, Shao Y, Zhang J, Dong XL, Liu WL, Yang H, Liu L, Li MH, Yue CF, Fang ZY, Zhang C, Hu XP, Chen BC, et al. Polymorphisms in human histamine receptor H4 gene are associated with atopic dermatitis. Br J Dermatol. 2010; 162:1038–43. https://doi.org/10.1111/j.1365-2133.2010.09675.x [PubMed]
- 33. Chu JT. Histamine H1 receptor gene polymorphism acts as a biological indicator of the prediction of therapeutic efficacy in patients with allergic rhinitis in the Chinese Han population. J Cell Biochem. 2019; 120:164–70. https://doi.org/10.1002/jcb.27278 [PubMed]
- 34. Raje N, Vyhlidal CA, Dai H, Jones BL. Genetic variation within the histamine pathway among patients with asthma--a pilot study. J Asthma. 2015; 52:353–62. https://doi.org/10.3109/02770903.2014.973501 [PubMed]
- 35. Vehof J, Risselada AJ, Al Hadithy AF, Burger H, Snieder H, Wilffert B, Arends J, Wunderink L, Knegtering H, Wiersma D, Cohen D, Mulder H, Bruggeman R. Association of genetic variants of the histamine H1 and muscarinic M3 receptors with BMI and HbA1c values in patients on antipsychotic medication. Psychopharmacology (Berl). 2011; 216:257–65. https://doi.org/10.1007/s00213-011-2211-x [PubMed]
- 36. Wang TH, Hsia SM, Shih YH, Shieh TM. Association of Smoking, Alcohol Use, and Betel Quid Chewing with Epigenetic Aberrations in Cancers. Int J Mol Sci. 2017; 18:1210. https://doi.org/10.3390/ijms18061210 [PubMed]
- 37. Cheng RH, Wang YP, Chang JY, Pan YH, Chang MC, Jeng JH. Genetic Susceptibility and Protein Expression of Extracellular Matrix Turnover-Related Genes in Oral Submucous Fibrosis. Int J Mol Sci. 2020; 21:8104. https://doi.org/10.3390/ijms21218104 [PubMed]
- 38. Hung CR, Chen HM. Role of histamine and acid back-diffusion in modulation of gastric microvascular permeability and haemorrhagic ulcers in betel-quid-fed rats. Inflammopharmacology. 2004; 12:277–87. https://doi.org/10.1163/1568560042342310 [PubMed]
- 39. Shrestha A, Keshwar S, Raut T. Evaluation of Mast Cells in Oral Potentially Malignant Disorders and Oral Squamous Cell Carcinoma. Int J Dent. 2021; 2021:5609563. https://doi.org/10.1155/2021/5609563 [PubMed]
- 40. Laishram D, Rao K, Devi HSU, Priya NS, Smitha T, Sheethal HS. Mast cells and angiogenesis in malignant and premalignant oral lesions: An immunohistochemical study. J Oral Maxillofac Pathol. 2017; 21:229–38. https://doi.org/10.4103/jomfp.JOMFP_111_15 [PubMed]
- 41. Singh S, Gupta V, Vij R, Aggarwal R, Sharma B, Nagpal M. Evaluation of mast cells in oral premalignant and malignant lesions: A histochemical study. Natl J Maxillofac Surg. 2018; 9:184–90. https://doi.org/10.4103/njms.NJMS_49_17 [PubMed]
- 42. Michailidou EZ, Markopoulos AK, Antoniades DZ. Mast cells and angiogenesis in oral malignant and premalignant lesions. Open Dent J. 2008; 2:126–32. https://doi.org/10.2174/1874210600802010126 [PubMed]
- 43. Yang CY, Meng CL. Regulation of PG synthase by EGF and PDGF in human oral, breast, stomach, and fibrosarcoma cancer cell lines. J Dent Res. 1994; 73:1407–15. https://doi.org/10.1177/00220345940730080301 [PubMed]
- 44. Tang Z, Li C, Kang B, Gao G, Li C, Zhang Z. GEPIA: a web server for cancer and normal gene expression profiling and interactive analyses. Nucleic Acids Res. 2017; 45:W98–102. https://doi.org/10.1093/nar/gkx247 [PubMed]
- 45. Tseng TH, Chien MH, Lin WL, Wen YC, Chow JM, Chen CK, Kuo TC, Lee WJ. Inhibition of MDA-MB-231 breast cancer cell proliferation and tumor growth by apigenin through induction of G2/M arrest and histone H3 acetylation-mediated p21WAF1/CIP1 expression. Environ Toxicol. 2017; 32:434–44. https://doi.org/10.1002/tox.22247 [PubMed]