



Introduction
Clear cell renal cell carcinoma (ccRCC) is the most aggressive type of renal cell carcinoma (RCC) with a high degree of malignancy and mortality [1, 2]. The patients generally have a poor prognosis [3, 4], due to the absence of specific clinical symptoms in early stages of the disease, which causes delay in the diagnosis and treatment [5, 6]. The etiology of ccRCC is not well-understood [7], and the exploration of the molecular targets for diagnosis and treatment of ccRCC is important to fight this most prevalent cancer of the uro-genital system.
Proteomics is an integral part of systems biology that uses high-resolution protein separation and protein identification technologies to study life phenomena in an integrated, dynamic and quantitative manner [8, 9]. Proteomics and phosphoproteomics have been successfully used to decipher the hub targets of various diseases [10, 11]. PRIDE (Proteomics Identification archive database) has played an important role in this endeavor [12]. Protein phosphorylation plays crucial roles in many biological processes such as cell cycle, signal transduction, differentiation and development, metabolism, apoptosis and carcinogenesis. Hence, phosphoproteomics has always been on the forefront of biological research [13]. In our previous studies, we have used the sequencing techniques (including transcriptomics, proteomics and phosphoproteomics) to identify the core molecular players of ccRCC, and the results indicate that FCGR2A might be a hub gene involved in the development and progression of ccRCC [14].
The FCGR2A gene encodes a member of the immunoglobulin Fc receptor gene family [15]. Single nucleotide polymorphisms (SNPs) that can affect the expression levels and function of FCGR2A have been reported [16]. The FCGR2A SNPs have been found to be associated with a shorter allograft survival [17, 18] and increase the risk for a variety of diseases [19]. Studies have also indicated the role of FCGR2A in the activation of inflammatory cells involved in chronic allograft rejection [20]. Nevertheless, the relationship between FCGR2A expression and ccRCC development and progression remains unclear and the clinical significance of FCGR2A expression in ccRCC tumor tissues remain unknown.
Therefore, in this study we evaluated the expression of FCGR2A in ccRCC tissues, and investigated the clinical significance of FCGR2A expression in ccRCC patients.
Results
Expression of FCGR2A
There were no differences in the level of expression of FCGR2A between male and female patients (Figure 1A), patients <60 years and ≥60 years (Figure 1B), and the tumor size <3 cm and ≥3 cm (Figure 1C). Compared with the pathologic grade I, the expression of FCGR2A in the pathologic grade III tumors was higher (P<0.05). The expression of FCGR2A in the pathologic grade II tumors was lower than that of pathologic grade III tumors (Figure 1D). The expression of FCGR2A was higher in the Enneking stage III and IV tumors than in Enneking stage I tumors (Figure 1E).
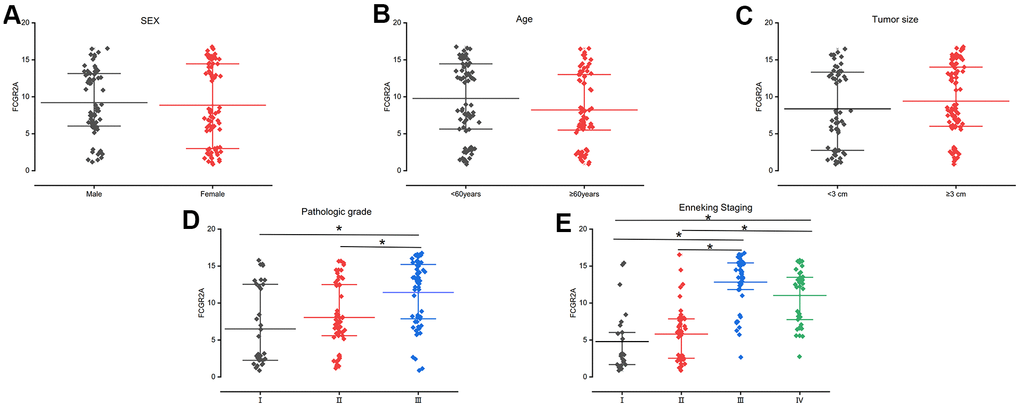
Figure 1. FCGR2A expression by different scatter plots in different groups. (A) Sex; (B) Age; (C) Tumor size; (D) Pathologic grade; (E) Enneking Staging. * represents that the P <0.05.
Associations between FCGR2A expression and demographic and clinical parameters
Pearson’s chi-squared test revealed that pathological grade of tumor (p<0.001), family history of ccRCC (p=0.001) and the Enneking stage of tumor (p<0.001) were significantly associated with FCGR2A expression. However, FCGR2A expression was not correlated with sex, age, and tumor size (p>0.05). (Table 1). Similarly, Spearman’s test showed that FCGR2A expression was significantly related to pathological grade of tumor (ρ = 0.406, p<0.001), family history of ccRCC (ρ = 1.000, p=0.001) and the Enneking stage of tumor (ρ =0.577, p<0.001). FCGR2A expression was not related with sex (ρ = -0.091, p = 0.266), age (ρ = -0.106, p = 0.193), and tumor size (ρ = 0.057, p = 0.484) (Table 2).
Table 1. Clinicopathological variables and the expression status of FCGR2A.
| FCGR2A | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| -/+(%) | ++(%) | +++(%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | Male | 66 | 10(6.6 %) | 25(16.6%) | 31(20.5%) | 0.136 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 85 | 24(15.9%) | 24(15.9%) | 37(24.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | <60years | 77 | 17(11.3 %) | 20(13.2%) | 40(26.5%) | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥60years | 74 | 17(11.3%) | 29(19.2%) | 28(18.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | <3 cm | 58 | 17(11.3 %) | 15(9.9%) | 26(17.2%) | 0.203 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥3 cm | 93 | 17(11.3%) | 34 (22.5%) | 42(27.8%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pathologic grade* | I | 35 | 19(12.6%) | 5 (3.3 %) | 11(7.3 %) | <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 59 | 11(7.3%) | 30(19.9%) | 18(11.9%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 57 | 4(2.6%) | 14(9.3%) | 39(25.8%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history of ccRCC* | No | 84 | 28(18.5 %) | 26(17.2 %) | 30(19.9%) | 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 67 | 6(4.0 %) | 23(15.2 %) | 38(25.2 %) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Enneking stage* | I | 25 | 15(9.9%) | 7(4.6 %) | 3(2.0%) | <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 44 | 17(11.3 %) | 22(14.6%) | 5(3.3 %) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 45 | 1(0.7 %) | 7(4.6 %) | 37(24.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 37 | 1(0.7 %) | 13(8.6 %) | 23(15.2 %) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pearson’s chi-squared test was used. *P<0.05. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. The corelationship between characteristics of patients and FCGR2A.
| Characteristics | FCGR2A | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ρ | p(spearman) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | -0.091 | 0.266 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | -0.106 | 0.193 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | 0.057 | 0.484 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pathologic grade* | 0.406 | <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history of ccRCC * | 1.000 | 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Enneking stage* | 0.577 | <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Spearman-rho test was used. *P<0.05. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
HRs of FCGR2A overexpression in ccRCC by univariate cox regression
Patients with family history of ccRCC had higher risk (HR=1.740, 95% CI, 1.197-2.530, p=0.004) of FCGR2A overexpression. Compared with type I pathological grade of tumor, the HR was 2.415 (95% CI, 1.347-4.331, p=0.003) for type II, and 5.475 (95% CI, 3.064-9.784, p<0.001) for type III grade tumors. The HR was 2.831 (95% CI, 1.437-5.574, p=0.003) for Enneking stage II, 14.555 (95% CI, 7.108-29.807, p<0.001) for Enneking stage III and 12.646 (95% CI, 5.950-26.876, p<0.001 for Enneking stage IV tumors. Compared with the ccRCC patients with low FCGR2A expression, those with high FCGR2A had poorer OS (HR=66.901, 95% CI, 28.251-159.428, p<0.001). There was no effect of sex, age and tumor size on the OS of ccRCC (P >0.05) (Table 3).
Table 3. Characteristics and their effect on OS based on univariate Cox proportional regression analysis.
| Characteristics | OS | p | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | Male | 66 | 1 | 0.193 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 85 | 0.782 | 0.540-1.133 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | <60years | 77 | 1 | 0.582 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥60years | 74 | 0.904 | 0.630-1.296 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | <3 cm | 58 | 1 | 0.981 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥3 cm | 93 | 1.004 | 0.695-1.452 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pathologic grade* | I | 35 | 1 | 0.003* <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 59 | 2.415 | 1.347-4.331 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 57 | 5.475 | 3.064-9.784 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history of ccRCC * | No | 84 | 1 | 0.004* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 67 | 1.740 | 1.197-2.530 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Enneking stage * | I | 25 | 1 | 0.003* <0.001* <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 44 | 2.831 | 1.437-5.574 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 45 | 14.555 | 7.108-29.807 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 37 | 12.646 | 5.950-26.876 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FCGR2A * | Low(-/+) | 34 | 1 | <0.001* <0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate(++) | 49 | 5.362 | 2.842-10.119 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High(+++) | 68 | 66.901 | 28.251-159.428 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OS, overall survival; HR, hazard ratio; 95% CI, 95% confidence interval. * P < 0.05. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Effect of demographic and clinical parameters on OS of ccRCC patients by multivariate Cox regression
ccRCC patients with high Enneking stage tumors (HR =1.995, 95% CI: 1.539-2.585, P <0.001) and overexpression of FCGR2A (HR = 7.612, 95% CI: 4.718-12.283, P <0.001) have poorer OS, whereas sex (HR = 0.925, 95% CI: 0.626-1.366, P = 0.694), age (HR = 0.937, 95% CI: 0.638-1.378, P = 0.742), tumor size (HR = 0.796, 95% CI: 0.536-1.183, P = 0.259), pathological grade of tumor (HR = 1.208, 95% CI: 0.902-1.618, P =0.205), family history of ccRCC (HR = 0.792, 95% CI: 0.515-1.218, P = 0.288) showed no significant effect on OS of ccRCC (Table 4).
Table 4. Characteristics and their effect on OS based on multivariate Cox regression analysis.
| Characteristics | OS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | p | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | 0.925 | 0.626-1.366 | 0.694 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 0.937 | 0.638-1.378 | 0.742 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size | 0.796 | 0.536-1.183 | 0.259 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pathologic grade | 1.208 | 0.902-1.618 | 0.205 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history of ccRCC | 0.792 | 0.515-1.218 | 0.288 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Enneking stage* | 1.995 | 1.539-2.585 | <0.001* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FCGR2A * | 7.612 | 4.718-12.283 | <0.001* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OS, overall survival; HR, hazard ratio; 95% CI, 95% confidence interval. *P < 0.05. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
ROC curve analysis
The area under the curve (AUC) for various ROC curves were calculated. The expression of FCGR2A could be used to predict the parameters associated with the disease with good sensitivity and specificity: tumor size (AUC = 0.57258, P=0.0472), pathological grade (AUC=0.73806, P=0.04145), family history (AUC= 0.62873, P=0.04596), Enneking stage (AUC= 0.64391, P= 0.06109), and survival time (AUC= 0.87944, P= 0.0278). Thus, FCGR2A expression can potentially be used as a diagnostic and prognostic marker for ccRCC (Figure 2).
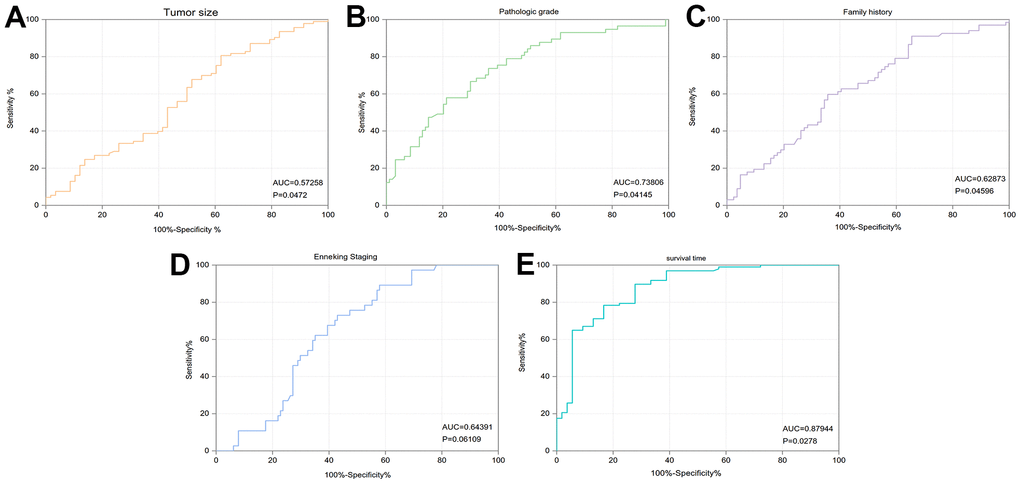
Figure 2. ROC curves to determine the effect of FCGR2A on diagnosing different traits of the ccRCC patients. (A) Tumor size. (B) Pathologic grade. (C) Family history. (D) Enneking Staging. (E) Survival time.
Effect of tumor and patient characteristics on overall survival of ccRCC patients
There was no effect of sex (HR=0.782, P=0.18166), age (HR=0.904, P=0.57028), and tumor size (HR=1.004, P=0.57028) on OS of ccRCC. The higher the pathologic grade of the tumor, the worse was OS (HR=1.208, P<0.05 had poorer OS (HR=1.740, P<0.05). The higher the Enneking stage of tumor, the worse was OS (HR=1.995, P<0.05) (Figure 3).
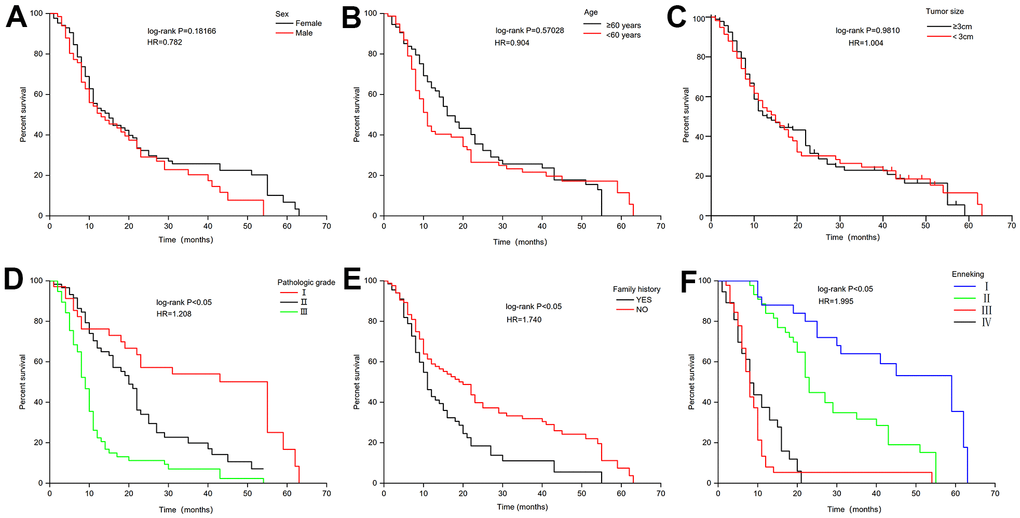
Figure 3. Effect of related characteristics on the overall survival of ccRCC. (A) Sex. (B) Age. (C) Tumor size. (D) Pathologic grade. (E) Family history. (F) Enneking Staging.
Patients with high expression of FCGR2A had poorer OS than patients with low expression of FCGR2A (HR=7.612, P<0.001) (Figure 4).
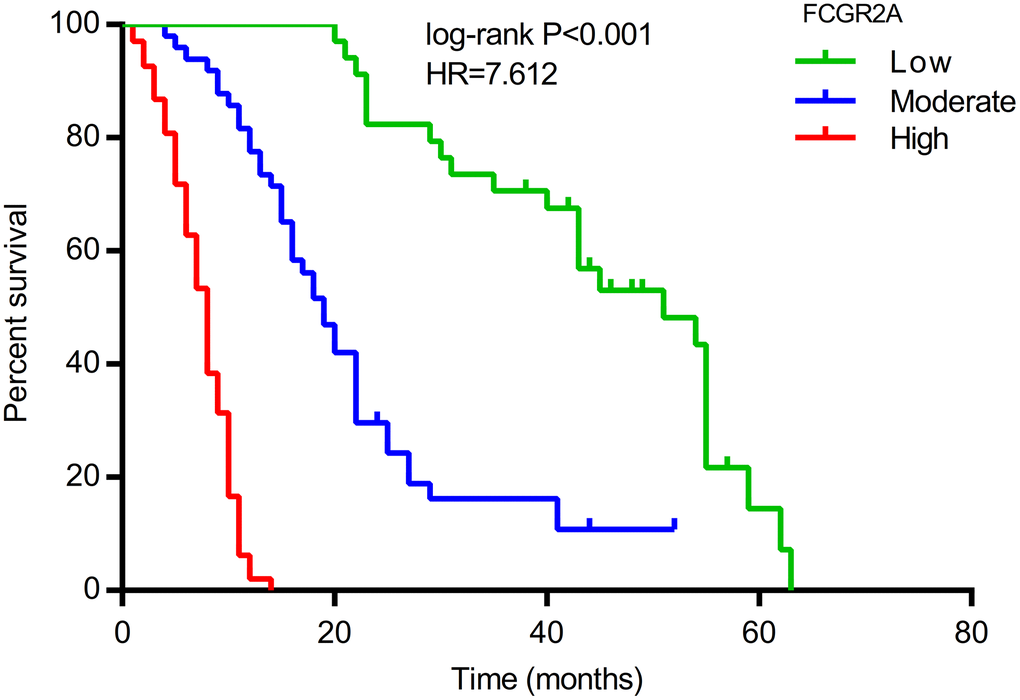
Figure 4. Effect of FCGR2A on the overall survival of ccRCC.
Pathological changes revealed by HE staining
The number of renal cells were lower in the control tissues as compared with ccRCC tissues (P<0.05). Changes in the cell morphology were noticed in ccRCC tissues and immature cells were more common in the tumor tissues (Figure 5).
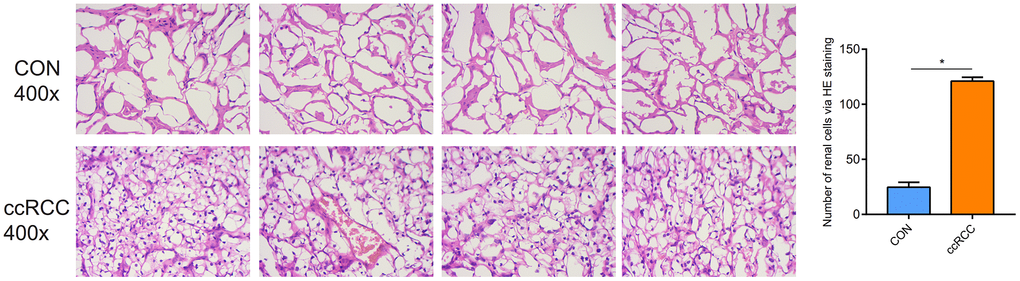
Figure 5. Pathological morphologic changes of ccRCC via the HE staining.
The protein expression of FCGR2A in ccRCC tissues
The protein expression of FCGR2A in ccRCC tissues was higher than that in control tissues (P<0.05) in the Immunohistochemical staining. The yellow areas represent the expression of FCGR2A (Figure 6). Immunofluorescence staining also showed that the expression of FCGR2A in the control tissue was significantly lower than the ccRCC tissues (Figure 7).
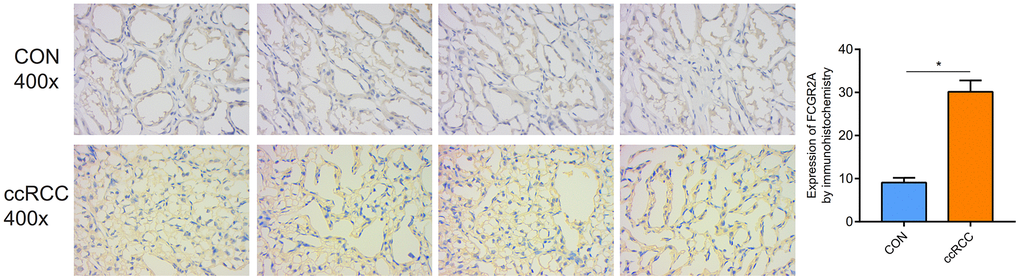
Figure 6. The protein expression of FCGR2A in the ccRCC and control tissues via immunohistochemical assay.
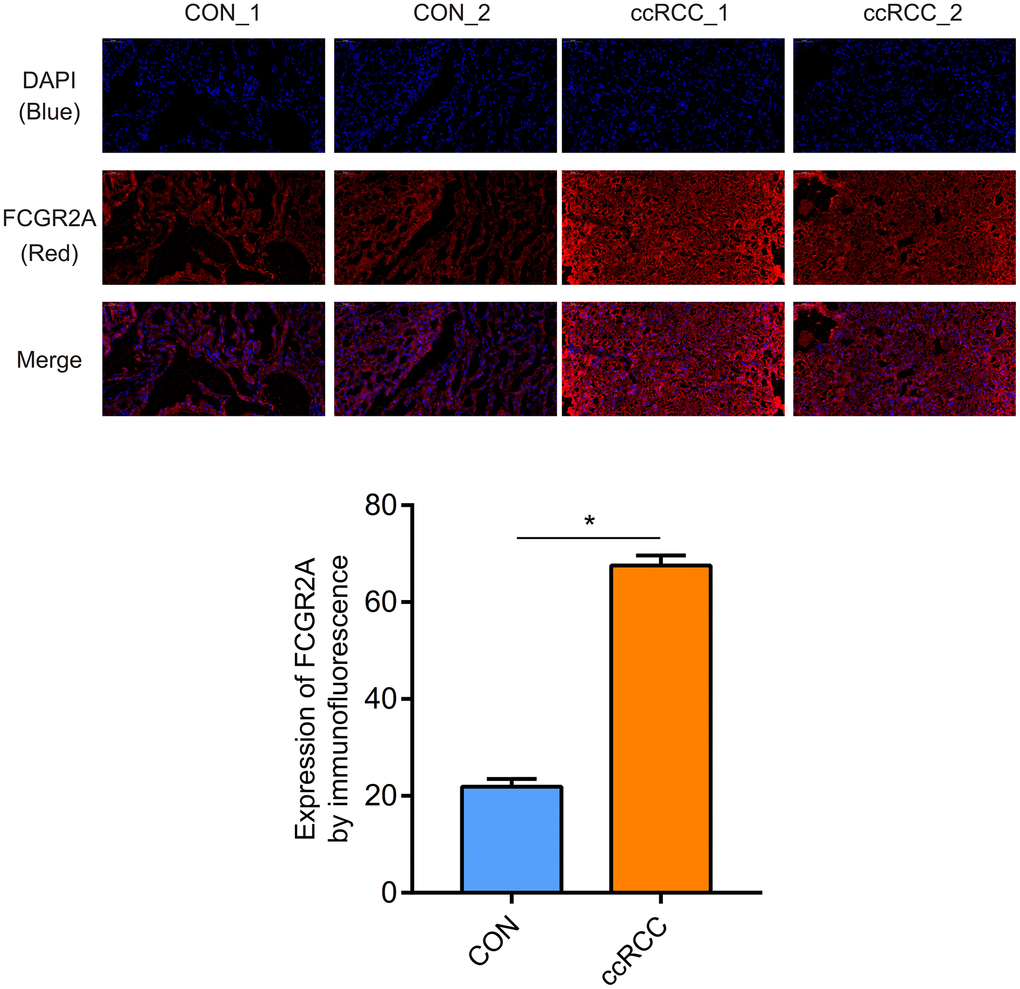
Figure 7. Verification of protein expression of FCGR2A by the immunofluorescence.
Correlation between the expression of FCGR2A and OS of ccRCC patients based on the BP neural network and SVM fitting
Fitting results of BP neural network showed that the R2 between FCGR2A expression and OS of ccRCC patients was 0.8429 (Figure 8A), SVM fitting results showed that the R2 between the FCGR2A expression and OS of ccRCC patients was 0.7669 (Figure 8B). The fitting data of the two prediction methods was more concentrated when OS was small, but the data was scattered when the survival time was large, indicating that the data prediction effect is better when the survival time is small. The R2 of BP neural network was significantly better than that of SVM, indicating that the prediction capability of BP was better than SVM. Also, the mean square error of SVM was 59.3845, compared with 40.0027 of BP.
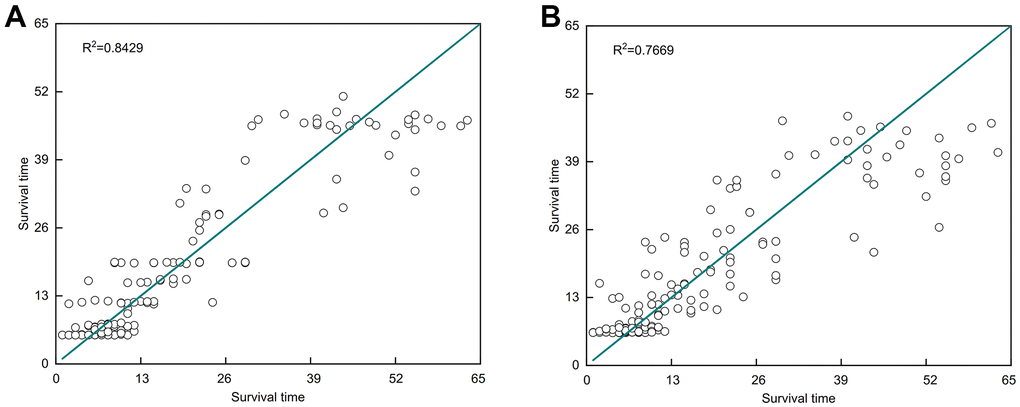
Figure 8. Strong correlation between the expression of FCGR2A and the survival time of ccRCC patients based on the BP neural network and support vector machine (SVM). (A) BP neural network. (B) SVM model.
Lower protein expression of FCGR2A in the ccRCC compared with control sample via western blotting
Through the western blotting assay, FCGR2A expression was lower in the ccRCC samples than control tissues. And the result was repeated three times, and the same trend was obtained. (P<0.05, Figure 9).
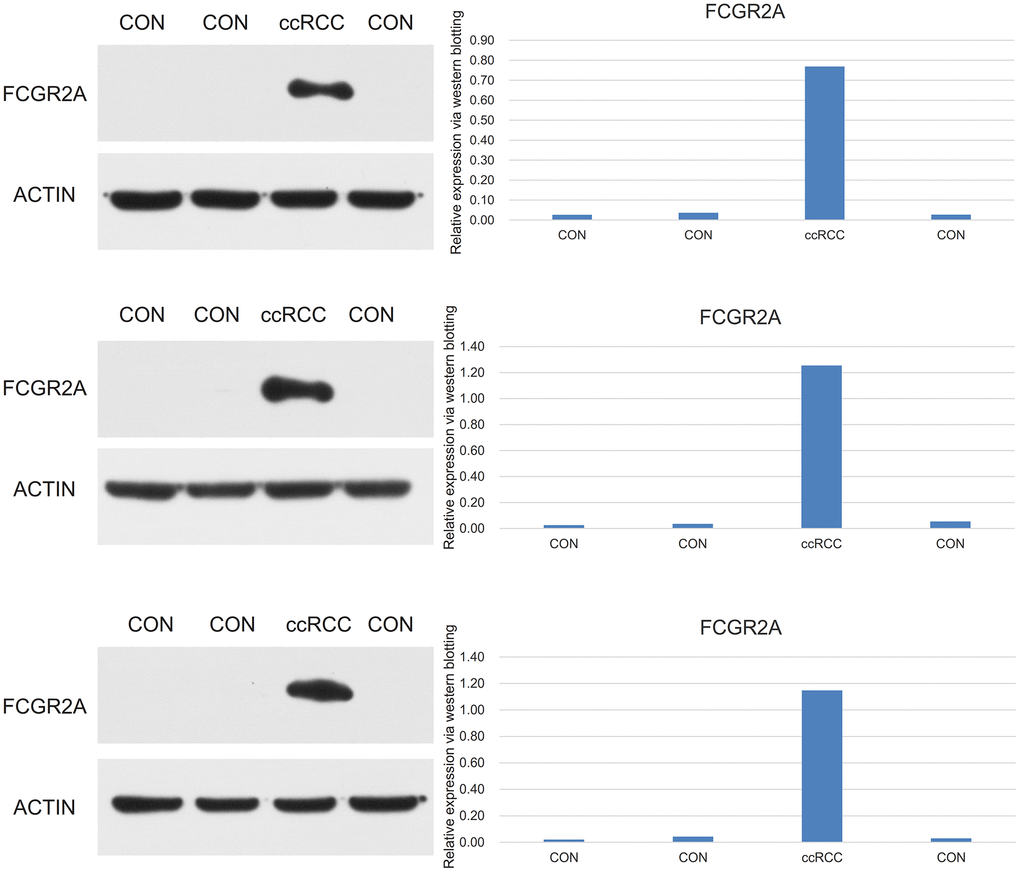
Figure 9. Lower protein expression of FCGR2A in the ccRCC compared with control sample via western blotting.
Discussion
Compared with normal renal tissue, FCGR2A was upregulated in patients with ccRCC. The patients with over expression of FCGR2A had poor OS. There was strong correlation between the expression of FCGR2A and OS of ccRCC patients based on the BP neural network and SVM.
Immunoglobulin IgGFc receptor (FcγRs) is a class of transmembrane glycoproteins that can specifically bind to IgGFc fragments and are expressed in a variety of immune cells [21]. The gene for FcγRIIa receptor (FCGR2A), which binds to the Fc fragment of IgG2 antibody is located on chromosome 1q23 [22]. FCGR2A is the only receptor of immunoglobulin G2 (IgG2) antibody, that is expressed in macrophages, lymphocytes and other innate immune cells, and regulates cell recognition, phagocytosis and cytotoxicity [23]. FcγRIIa is the most important immune-activating receptor in its family [24] which are expressed differently on immune cells and link the humoral and cell-mediated immune responses [25, 26]. After binding with IgG and cross-linking, activated FCGRs transmits signals within immune cells and activates the immune system [27–29]. FCGR2A was found to be associated with the clinical response in several clinical trials involving a variety of chimeric or humanized monoclonal antibodies targeting various cancers [30]. Researchers have demonstrated the correlation between FCGR2A genotypes and patients' response to immunotherapy [31, 32]. Therefore, we speculated that FCGR2A might participate in the development and progression of ccRCC by affecting immune function and inflammatory response, and might be used as a target for early diagnosis of ccRCC.
Previous studies have implicated FCGR2A in immune response to tumors. Since FCGR2A has a strong affinity for IgG2, it could play a role in antitumor defense. It could help in mounting immune response to tumors by causing antibody-dependent cell phagocytosis (ADCP) and facilitating antigen processing and presentation [33]. The involvement of FCGR2A in the immune response to ccRCC is indicated by a study that showed significant upregulation of various FCGR proteins, including FCGR2A in ccRCC tissues [34]. FCGRs may also play an in vivo antitumor role in ccRCC patients receiving high doses of IL2 [14]. These observations are consistent with our results of differential expression of FCGR2A in ccRCC tissues.
Our results indicate that FCGR2A might serve as an important core target for diagnosis of ccRCC and is closely related to the clinical characteristics of the tumor. In future, the role of FCGR2A in the development and progression of ccRCC can be explored further by siRNA based silencing of FCGR2A gene in vitro or in animal models. The molecule can also be used for the developments of kits for diagnosis of ccRCC.
In conclusion, FCGR2A is highly expressed in renal clear cell carcinoma, and when this molecule is highly expressed, the survival prognosis of renal carcinoma is poor. FCGR2A may be a potential target for the diagnosis and treatment of renal clear cell carcinoma.
Materials and Methods
Patients
A total of 151 ccRCC patients treated in the Fourth hospital of Hebei medical university hospital, Hubei province, China from March 2015 to June 2020 were recruited for the study. Inclusion criteria for the patients was: age 18-100 years old; ccRCC diagnosis with normal heart function; normal coagulation and fibrinolysis function. Exclusion criteria was: poor pulmonary, cardiac, and liver function and refusal to participate in the study.
Clinical characteristics
Clinical characteristics of ccRCC patients included sex, age (<60 years /≥60 years), tumor size (<3cm/≥3cm), pathologic grade (I/II/III), family history of ccRCC (Yes/No), and the Enneking stage (I/II/III/IV).
HE staining
The Paraffin embedded sections containing renal carcinoma and adjacent tissues were successively washed with solutions containing increasing concentrations of ethyl alcohol. The slices were then dehydrated in ethyl alcohol and treated with xylene. The nuclei were stained with hematoxylin and cytoplasm with eosin. The slides were mounted in the mounting medium and examined under the microscope.
Immunohistochemistry
Paraffin sections were dewaxed and incubated with 3% H2O2 for 5 min to eliminate the endogenous peroxidase activity. The sections were then rinsed with distilled water and soaked in PBS for 5 minutes and blocked with 5% goat serum for 10 minutes. Overnight incubation with an anti-FCGR2A primary antibody [FCGR2A monoclonal antibody (15625-1-AP, Proteintech Group, Inc, USA)] was performed at 4° C. The sections were rinsed with PBS and incubated with a biotin-labeled secondary antibody at 37° C for 30 min. Horseradish enzyme-labeled working solution was added drop wise to the sections and incubated for 5 min. The paraffin sections were washed three times, 5 min each, in PBS (pH 7.4) rotary shaker. After the slices were slightly dried, freshly prepared DAB color development solution was added drop wise and the color development time was controlled by observing the slides under the microscope. Nuclei were counterstained with hematoxylin.
Immunofluorescence staining of FCGR2A
Paraffin sections were dewaxed and rehydrated. After washing with PBS (pH7.4) three times. 5 min each, the sections were immersed in EDTA antigen retrieval buffer (pH 8.0) (Servicebio G1206, Wuhan, China) to retrieve the antigens. The sections were blocked with 3% BSA (Servicebio, G5001, Wuhan, China) in PBS (pH 7.4) for 30min and incubated overnight at 4° C with FCGR2A antibody (1:600, 15625-1-AP, Proteintech Group, Inc, USA). The sections were washed with PBS (pH 7.4) three times, 5 min each, and fluorescently-labeled secondary antibody (1:5000) was added. The slides were incubated in the secondary antibody for 50 min at RT in dark. After washing with PBS (pH 7.4) three times, 5 min each, the slides were incubated with DAPI solution (Servicebio, G1012, Wuhan, China) in dark for 10 min at RT to counterstain the nucleus. Spontaneous fluorescence was quenched with the spontaneous fluorescence quenching reagent (Servicebio, G1221, Wuhan, China) and the slides were sealed after adding the anti-fade mounting medium. Fluorescence microscope (Nikon NIKON ECLIPSE C1) was used to observe the slides. The nuclei were stained blue (excitation wavelength 330-380nm and emission 420nm) and the positive expression of FCGR2A exhibited red fluorescence.
RT-qPCR
T7 RNA polymerase, LA Taq polymerase, Ex Taq polymerase and DNA size markers were purchased from Takara (Tokyo, Japan). RNeasy Mini kit, and QLA quick Gel Extraction Kit were obtained from QIAGEN (Germany). The RT-PCR was performed on an ABI 7500 RT-PCR System (USA). RNA was extracted using RNeasy Mini Kit as per manufacturer’s instructions. The thermocycler was programmed as follows: 55° C (2min), 72° C (3min), 94° C (30s), 60° C (30s), and 72° C (30s). A total of 72 cycles of amplification was performed. The final extension was performed at 72° C for 10 min. The PCR products were separated on agarose gels and the PCR fragments were purified by QLA Quick Gel Extraction Kit. Relative expressions of the hub genes were calculated by the 2-ΔΔCt. GAPDH gene was used as an endogenous control. The following primer pairs were used for the amplification of FCGR2A gene: Forward: TCAGGGGGTGAGAGAAGAGACTAG; Reverse: CTAGTCTCTTCTCTCACCCCCTGAA.
Western blotting
Total protein was extracted from the tissue blocks frozen at -80° C. Tissue block was washed 3 times with pre-cooled PBS (pH 7.4) and homogenized in the lysis buffer. The lysate was incubated on ice for 30 min and centrifuged at 12000 x g for 10 min at 4° C. The supernatant was collected and protein concentration was estimated using Bradford’s reagent. The proteins were separated on a 10% SDS-PAGE gel and transferred on to a PVDF membrane using a semi-dry electroblotter. The membrane was blocked with 5% skimmed milk in PBS (pH 7.4) for 30 min and incubated overnight at 4° C with the primary antibody (anti-FCGR2A, 15625-1-AP, Proteintech, Wuhan, China). The blot was washed with PBS 3 times, 10 min each, and incubated with the secondary antibody for 1 h. After washing 3 times, 10 min each, with PBS (pH 7.4), the blot was placed in the chemiluminescence reagent and sealed in a transparent plastic wrap. The blot was exposed to the X-ray film in a cassette for 1-2 min and the film was developed. Alpha software (version: 12.3. USA) was used to analyze the image.
Statistical methods
Pearson’s chi-squared test and Spearman’s Rho test were used to explore associations between the FCGR2A expression and demographic and clinical parameters of the patients. Hazard ratios (HRs) of FCGR2A overexpression for different clinical and demographics parameters of the patients were calculated by univariate Cox regression. Correlation between the various demographic and clinical parameters and overall survival (OS) of ccRCC patients was determined by multivariate Cox regression. Receiver operating characteristic (ROC) curves were constructed to explore the role of FCGR2A as a diagnostic marker for ccRCC. Correlation between the various demographic and clinical parameters and overall survival (OS) of ccRCC patients was also performed by the BP neural network and support vector machine (SVM). SPSS 24.0 (IBM Corp., USA), and Matlab (R2017a, MathWorks.Inc, USA) were used for statistical analysis. Statistical significance was achieved at P< 0.05.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the fourth hospital of Hebei medical university. Written informed consent was obtained from all patients.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
Feng Li performed the experiments, and was a major contributors in writing. Feng Li was also involved in the revision of the manuscript with critical inputs. Changjin Shi made substantial contributions to research conception and provided technical support. Yueyue Wei designed the draft of the research process., analyzed the data and submitted the manuscript for publication. All authors read and approved the final manuscript.
Acknowledgments
We are grateful to the director of Urology Department of the Fourth Hospital of Hebei Medical University for supporting this study.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This research was funded by the Key science and technology research program of scientific research fund of Hebei Provincial Health Commission (No. 20210874), and Youth Science and Technology Projects of Scientific Research Fund of Hebei Provincial Health Commission (No. 20190744).
References
- 1. Zhang G, Wu Y, Zhang J, Fang Z, Liu Z, Xu Z, Fan Y. Nomograms for predicting long-term overall survival and disease-specific survival of patients with clear cell renal cell carcinoma. Onco Targets Ther. 2018; 11:5535–44. https://doi.org/10.2147/OTT.S171881 [PubMed]
- 2. Xing T, He H. Epigenomics of clear cell renal cell carcinoma: mechanisms and potential use in molecular pathology. Chin J Cancer Res. 2016; 28:80–91. https://doi.org/10.3978/j.issn.1000-9604.2016.02.09 [PubMed]
- 3. Atkins MB, Tannir NM. Current and emerging therapies for first-line treatment of metastatic clear cell renal cell carcinoma. Cancer Treat Rev. 2018; 70:127–37. https://doi.org/10.1016/j.ctrv.2018.07.009 [PubMed]
- 4. Cao Q, Ruan H, Wang K, Song Z, Bao L, Xu T, Xiao H, Wang C, Cheng G, Tong J, Meng X, Liu D, Yang H, et al. Overexpression of PLIN2 is a prognostic marker and attenuates tumor progression in clear cell renal cell carcinoma. Int J Oncol. 2018; 53:137–47. https://doi.org/10.3892/ijo.2018.4384 [PubMed]
- 5. Zhao YH, Wang Z, Zhang N, Cui T, Zhang YH. Effect of ciRS-7 expression on clear cell renal cell carcinoma progression. Chin Med J (Engl). 2020; 133:2084–9. https://doi.org/10.1097/CM9.0000000000000867 [PubMed]
- 6. Zhang X, Xing ND, Lai CJ, Liu R, Jiao W, Wang J, Song J, Xu ZH. MicroRNA-375 Suppresses the Tumor Aggressive Phenotypes of Clear Cell Renal Cell Carcinomas through Regulating YWHAZ. Chin Med J (Engl). 2018; 131:1944–50. https://doi.org/10.4103/0366-6999.238153 [PubMed]
- 7. Jonasch E, Gao J, Rathmell WK. Renal cell carcinoma. BMJ. 2014; 349:g4797. https://doi.org/10.1136/bmj.g4797 [PubMed]
- 8. Muench DE, Olsson A, Ferchen K, Pham G, Serafin RA, Chutipongtanate S, Dwivedi P, Song B, Hay S, Chetal K, Trump-Durbin LR, Mookerjee-Basu J, Zhang K, et al. Mouse models of neutropenia reveal progenitor-stage-specific defects. Nature. 2020; 582:109–14. https://doi.org/10.1038/s41586-020-2227-7 [PubMed]
- 9. Dwivedi P, Chutipongtanate S, Muench DE, Azam M, Grimes HL, Greis KD. SWATH-Proteomics of Ibrutinib’s Action in Myeloid Leukemia Initiating Mutated G-CSFR Signaling. Proteomics Clin Appl. 2020; 14:e1900144. https://doi.org/10.1002/prca.201900144 [PubMed]
- 10. Dwivedi P, Greis KD. Granulocyte colony-stimulating factor receptor signaling in severe congenital neutropenia, chronic neutrophilic leukemia, and related malignancies. Exp Hematol. 2017; 46:9–20. https://doi.org/10.1016/j.exphem.2016.10.008 [PubMed]
- 11. Dwivedi P, Muench DE, Wagner M, Azam M, Grimes HL, Greis KD. Time resolved quantitative phospho-tyrosine analysis reveals Bruton’s Tyrosine kinase mediated signaling downstream of the mutated granulocyte-colony stimulating factor receptors. Leukemia. 2019; 33:75–87. https://doi.org/10.1038/s41375-018-0188-8 [PubMed]
- 12. Dwivedi P, Muench DE, Wagner M, Azam M, Grimes HL, Greis KD. Phospho serine and threonine analysis of normal and mutated granulocyte colony stimulating factor receptors. Sci Data. 2019; 6:21. https://doi.org/10.1038/s41597-019-0015-8 [PubMed]
- 13. Ochoa D, Jarnuczak AF, Viéitez C, Gehre M, Soucheray M, Mateus A, Kleefeldt AA, Hill A, Garcia-Alonso L, Stein F, Krogan NJ, Savitski MM, Swaney DL, et al. The functional landscape of the human phosphoproteome. Nat Biotechnol. 2020; 38:365–73. https://doi.org/10.1038/s41587-019-0344-3 [PubMed]
- 14. Li F, Jin Y, Pei X, Guo P, Dong K, Wang H, Chen Y, Guo P, Meng LB, Wang Z. Bioinformatics analysis and verification of gene targets for renal clear cell carcinoma. Comput Biol Chem. 2021; 92:107453. https://doi.org/10.1016/j.compbiolchem.2021.107453 [PubMed]
- 15. Márquez Pete N, Maldonado Montoro MDM, Pérez Ramírez C, Martínez Martínez F, Martínez de la Plata JE, Daddaoua A, Jiménez Morales A. Influence of the FCGR2A rs1801274 and FCGR3A rs396991 Polymorphisms on Response to Abatacept in Patients with Rheumatoid Arthritis. J Pers Med. 2021; 11:573. https://doi.org/10.3390/jpm11060573 [PubMed]
- 16. Paul P, Pedini P, Lyonnet L, Di Cristofaro J, Loundou A, Pelardy M, Basire A, Dignat-George F, Chiaroni J, Thomas P, Reynaud-Gaubert M, Picard C. FCGR3A and FCGR2A Genotypes Differentially Impact Allograft Rejection and Patients’ Survival After Lung Transplant. Front Immunol. 2019; 10:1208. https://doi.org/10.3389/fimmu.2019.01208 [PubMed]
- 17. Yuan FF, Watson N, Sullivan JS, Biffin S, Moses J, Geczy AF, Chapman JR. Association of Fc gamma receptor IIA polymorphisms with acute renal-allograft rejection. Transplantation. 2004; 78:766–9. https://doi.org/10.1097/01.tp.0000132560.77496.cb [PubMed]
- 18. Arnold ML, Fuernrohr BG, Weiß KM, Harre U, Wiesener MS, Spriewald BM. Association of a coding polymorphism in Fc gamma receptor 2A and graft survival in re-transplant candidates. Hum Immunol. 2015; 76:759–64. https://doi.org/10.1016/j.humimm.2015.09.034 [PubMed]
- 19. Zhang C, Wang W, Zhang H, Wei L, Guo S. Association of FCGR2A rs1801274 polymorphism with susceptibility to autoimmune diseases: A meta-analysis. Oncotarget. 2016; 7:39436–43. https://doi.org/10.18632/oncotarget.9831 [PubMed]
- 20. Fildes JE, Yonan N, Tunstall K, Walker AH, Griffiths-Davies L, Bishop P, Leonard CT. Natural killer cells in peripheral blood and lung tissue are associated with chronic rejection after lung transplantation. J Heart Lung Transplant. 2008; 27:203–7. https://doi.org/10.1016/j.healun.2007.11.571 [PubMed]
- 21. Takai T. Roles of Fc receptors in autoimmunity. Nat Rev Immunol. 2002; 2:580–92. https://doi.org/10.1038/nri856 [PubMed]
- 22. Bruhns P, Iannascoli B, England P, Mancardi DA, Fernandez N, Jorieux S, Daëron M. Specificity and affinity of human Fcgamma receptors and their polymorphic variants for human IgG subclasses. Blood. 2009; 113:3716–25. https://doi.org/10.1182/blood-2008-09-179754 [PubMed]
- 23. Munde EO, Okeyo WA, Raballah E, Anyona SB, Were T, Ong’echa JM, Perkins DJ, Ouma C. Association between Fcγ receptor IIA, IIIA and IIIB genetic polymorphisms and susceptibility to severe malaria anemia in children in western Kenya. BMC Infect Dis. 2017; 17:289. https://doi.org/10.1186/s12879-017-2390-0 [PubMed]
- 24. Vogelpoel LT, Baeten DL, de Jong EC, den Dunnen J. Control of cytokine production by human fc gamma receptors: implications for pathogen defense and autoimmunity. Front Immunol. 2015; 6:79. https://doi.org/10.3389/fimmu.2015.00079 [PubMed]
- 25. Nimmerjahn F, Ravetch JV. Analyzing antibody-Fc-receptor interactions. Methods Mol Biol. 2008; 415:151–62. https://doi.org/10.1007/978-1-59745-570-1_9 [PubMed]
- 26. Nimmerjahn F, Ravetch JV. Fcgamma receptors as regulators of immune responses. Nat Rev Immunol. 2008; 8:34–47. https://doi.org/10.1038/nri2206 [PubMed]
- 27. Bakema JE, van Egmond M. Fc receptor-dependent mechanisms of monoclonal antibody therapy of cancer. Curr Top Microbiol Immunol. 2014; 382:373–92. https://doi.org/10.1007/978-3-319-07911-0_17 [PubMed]
- 28. Platzer B, Stout M, Fiebiger E. Antigen cross-presentation of immune complexes. Front Immunol. 2014; 5:140. https://doi.org/10.3389/fimmu.2014.00140 [PubMed]
- 29. Harbers SO, Crocker A, Catalano G, D’Agati V, Jung S, Desai DD, Clynes R. Antibody-enhanced cross-presentation of self antigen breaks T cell tolerance. J Clin Invest. 2007; 117:1361–9. https://doi.org/10.1172/JCI29470 [PubMed]
- 30. Weng WK, Levy R. Two immunoglobulin G fragment C receptor polymorphisms independently predict response to rituximab in patients with follicular lymphoma. J Clin Oncol. 2003; 21:3940–7. https://doi.org/10.1200/JCO.2003.05.013 [PubMed]
- 31. Kjersem JB, Skovlund E, Ikdahl T, Guren T, Kersten C, Dalsgaard AM, Yilmaz MK, Fokstuen T, Tveit KM, Kure EH. FCGR2A and FCGR3A polymorphisms and clinical outcome in metastatic colorectal cancer patients treated with first-line 5-fluorouracil/folinic acid and oxaliplatin +/- cetuximab. BMC Cancer. 2014; 14:340. https://doi.org/10.1186/1471-2407-14-340 [PubMed]
- 32. Weng WK, Weng WK, Levy R. Immunoglobulin G Fc receptor polymorphisms do not correlate with response to chemotherapy or clinical course in patients with follicular lymphoma. Leuk Lymphoma. 2009; 50:1494–500. https://doi.org/10.1080/10428190903128660 [PubMed]
- 33. Lejeune J, Piègu B, Gouilleux-Gruart V, Ohresser M, Watier H, Thibault G. FCGR2C genotyping by pyrosequencing reveals linkage disequilibrium with FCGR3A V158F and FCGR2A H131R polymorphisms in a Caucasian population. MAbs. 2012; 4:784–7. https://doi.org/10.4161/mabs.22287 [PubMed]
- 34. Nie W, Yao Y, Luo B, Zhu J, Li S, Yang X, Luo T, Liu W, Yan S. Systematic Analysis of the Expression and Prognosis of Fcγ Receptors in Clear Cell Renal Cell Carcinoma. Front Oncol. 2022; 12:755936. https://doi.org/10.3389/fonc.2022.755936 [PubMed]