



Introduction
Parkinson's disease (PD) is a neurodegenerative disease characterized by resting tremors, bradykinesia, and rigidity [1]. The burden of disease to PD patients, their caregivers, and society is high. PD has been associated with an increase in disability-adjusted life years (one of the leading causes of years lived with disability [2]).
Intriguingly, studies have identified a relationship between cancer development following PD diagnosis. Several studies uncovered a positive relationship between PD and subsequent melanoma [3, 4], while some found a null relationship [5, 6]. Other studies also noted melanoma development after levodopa use, the standard PD pharmacological therapy [7].
Clearly, existing studies investigating the link between PD and subsequent melanoma have reached different conclusions. Furthermore, PD was associated with increased risks of breast [4], non-melanocytic [8], and brain cancer [9], but decreased prostate, bladder, and colorectal cancer risks [10]. Risk factors including gender, gene variants implicated in PD pathogenesis, and lifestyle habits like smoking, were also found to have effects on cancer risk following PD diagnosis, further adding to the debate.
Cancer is characterized by aberrant and uncontrolled proliferation [11], directly opposing PD pathogenesis. However, like PD, cancer is crippling due to the physical decline, high mortality, treatment effects, and psychological trauma involved [12]. This makes it more pertinent to interrogate the link between PD and subsequent cancer risk, to identify and treat both diseases early, and more importantly identify factors (such as gender, genetic predisposition, and lifestyle habits) that may influence the association between PD and cancer. Collectively, these efforts can reduce the overall disease burden associated with both pathologies.
To address these gaps in knowledge, we conduct a systematic review and meta-analysis (including case-control and cohort studies published between 1 January 2010 and 30 August 2020) to investigate the association of specific cancers with PD and the possible role of lifestyle, gender and genetic risk factors.
Results
Included studies
Fourteen studies were included in this meta-analysis, conducted in accordance with the Quality of Reporting of Meta-analyses (QUOROM) guidelines (Figure 1, Supplementary Table 1).
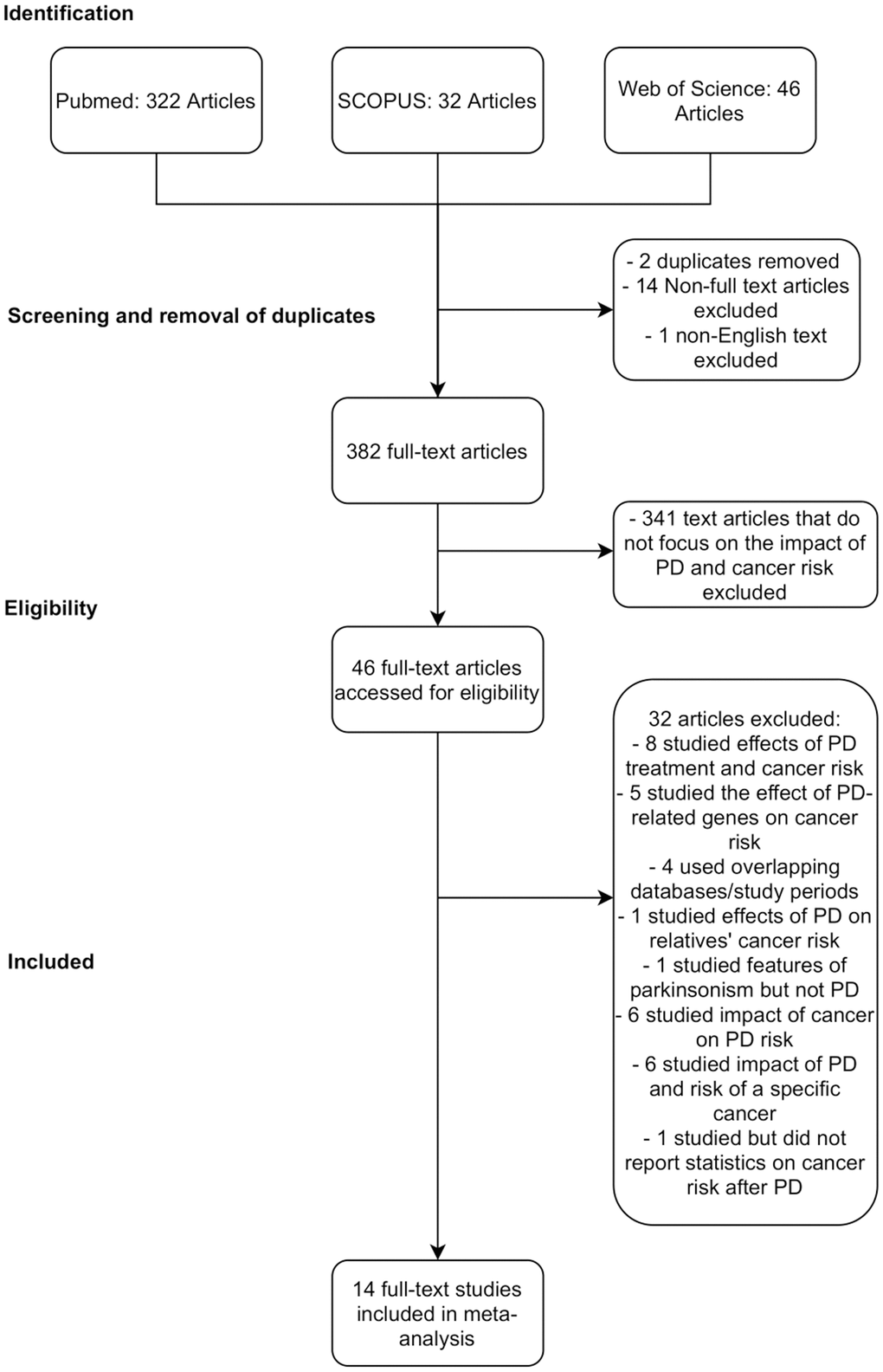
Figure 1. PRISMA chart detailing database search procedure and exclusion criteria.
The details of the 14 studies are provided in Table 1. Reasons for excluding studies investigating PD’s impact on subsequent cancer risk, despite meeting the eligibility criteria, are detailed in Supplementary Table 2.
Table 1. Characteristics of all studies included in the meta-analysis.
| No. | Author | Study design | Country | Sample size | Females (%) | Mean age (SD) | Adjustment | Cancer (s) reported | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | Lin, 2015 | Cohort | Taiwan | 62023 PD patients 124046 non-PD controls | 94458 (50.7%) | NR | Sex, age | Cancer in general, brain, melanoma, kidney, liver, uterus (women), oesophagus, skin, prostate (men), gallbladder, lymphoma/leukaemia, stomach, bladder, lung, pancreas, colorectal, cervical (women), breast (women), thyroid, ovary (women) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2 | Fois, 2010 | Cohort | UK | 4355 PD patients Compared to general population | 2205 (50.6%) | NR | Sex, age in 5y bands, time period (years), district of residence | Cancer in general, oral cavity, pharynx, lip, larynx, oesophageal, stomach, colon, rectum, pancreas, lung, breast, cervix, ovary, uterus, prostate, kidney, bladder, malignant melanoma, other skin cancer, malignant brain, bone, lymphoma, non-Hodgkin's lymphoma, multiple myeloma, leukaemia, lymphoid leukaemia, myeloid leukaemia, benign brain | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | Peretz, 2016 | Cohort | Israel | 7125 PD patients Compared to general population | 3297 (46.3%) | 71.1 (10.6) | Age, chronological year, sex | Cancer in general, breast (women), colon, CNS, kidney, leukaemia, lung, lymphoma, melanoma, ovary, pancreas, prostate (men), rectum, thyroid | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 | Park, 2019 | Cohort | South Korea | 52009 PD patients 260045 non-PD controls | 184776 (59.2%) | 71 (10) | Diabetes mellitus, hypertension, dyslipidaemia, income status | Cancer in general, oral cavity and pharyngeal, laryngeal, oesophageal, gastric, colorectal, liver, pancreatic, biliary, lung, renal, bladder, thyroid, leukaemia, lymphoma, multiple myeloma, skin, breast (women), uterine cervical (women), uterine corpus (women), ovarian (women), prostate (men), testicular (men) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 | Lo, 2010 | Cohort | USA | 692 PD patients 761 non-PD controls | 544 (37.4%) | 65.9 (12.1) | Age, sex, cigarette smoking (pack years), alcohol consumption (number of drinks per month), BMI, eye colour | Cancer in general, smoking-related cancer, non-smoking related cancer, lung, bladder, breast (women), prostate (men), colorectal, melanoma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 6 | Liat, 2014 | Cohort | UK | 219194 PD patients 9015614 non-PD controls | 43% | NR | NR | Cancer in general, bladder, bone, brain, breast (women), cervix (women), colon, upper GI, kidney, larynx, myeloid leukaemia, lymphoid leukaemia, liver, lung, Hodgkin's lymphoma, non-Hodgkin's lymphoma, malignant melanoma, multiple myeloma, nasopharynx, meninges, oesophageal, ovary (women), pancreas, prostate, rectum, salivary gland, non-melanoma skin cancer, stomach, testis (men), thyroid, uterus corpus (women) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7 | Rugbjerg, 2012 | Cohort | Denmark | 20343 PD patients Compared to general population | 9631 (47.3%) | 72.7 | NR | Cancer in general, malignant melanoma, non-melanoma skin, breast (women), larynx, lung, urinary bladder, ovary, fallopian tube and bread ligament (women), colorectal, prostate (men), non-Hodgkin lymphoma, corpus uteri (women), brain, multiple myeloma, lymphatic leukaemia, unspecified | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 8 | Wirdefeldt, 2014 | Cohort | Sweden | 11786 PD patients 58930 non-PD controls | 27906 (39.5%) | 62.5 (9.2) | Education level | Cancer in general, mouth, oesophageal, stomach, liver, pancreas, nose and nasal sinuses, larynx, trachea, bronchus, lung and pleura, cervix uteri (women), kidney and urinary organs, small intestine, peritoneum, mediastinum, breast (women), prostate (men), testis (men), malignant melanoma of skin, skin (excluding melanoma), endocrine glands, bone, connective tissue or muscle, nervous system, colon, rectum, anus, lymphoma, corpus uteri (women), ovary (women), male genital organs other than prostate and testis, thyroid gland, multiple myeloma, lymphatic leukaemia, unspecified | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9a | Becker, 2010 | Cohort | UK | 2993 PD patients 3003 non-PD controls | NR | NR | NR | Cancer in general, lung, larynx, pharynx, buccal cavity, stomach, urinary tract, oesophageal, pancreas, breast (women), colorectal, prostate (men), lymphoma/leukaemia, female reproductive organs, CNS, liver, gallbladder, thyroid gland, unspecified | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9b1 | Becker, 2010 | Case-control | UK | 1118 PD patients 1212 non-PD controls | NR | NR | NR | Cancer in general, lung, larynx, pharynx, buccal cavity, stomach, urinary tract, oesophageal, pancreas, breast (women), colorectal, prostate (men), lymphoma/leukaemia, female reproductive organs, CNS, liver, gallbladder, thyroid gland, unspecified | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 10 | Agalliu, 2019 | Case-control | Europe, Israel, USA | 712 PD patients 218 non-PD controls | 419 (45.1%) | 66.9 (10.9) | Age, sex, Ashkenazi Jews ethnicity (fixed effect) and study centre (random effect), smoking status, BMI | Cancer in general, skin cancer, melanoma, lung cancer, bladder cancer, breast (women), ovarian (women), prostate (men), colon, kidney/renal, haematologic/lymphoma, meningioma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 11 | Ruiz-Martínez, 2014 | Case-control | Spain | 637 PD patients 176 non-PD controls | 415 (51.0%) | 71.2 (12.0) | Age | Cancer in general, melanoma, lung, bladder, colon, kidney, breast (women), ovarian (women), prostate (men), hormonal, haematologic, meningioma, unspecified | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 12 | Freedman, 2015 | Case-control | USA | 6994 PD patients 972822 non-PD controls | 445388 (45.5%) | NR (Median age = 74 years) | Age, race, sex, number of doctors’ visits, cancer registry area and selection years | Cancer in general, oral cavity, oesophageal, stomach, colon, rectum, pancreas, larynx, lung and bronchus, melanoma, breast (women), cervix (women), uterus (women), ovary (women), prostate (men), urinary bladder, kidney/renal pelvis, thyroid, leukaemia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 13 | Tacik, 2016 | Case-control | USA | 971 PD patients 478 non-PD controls | 840 (58.0%) | NR (median age = 67 years) | Age and sex (except for sex-specific cancers - breast, prostate, ovarian, uterine, testicular) No adjustment - For cancers with <10 patients | Cancer in general, breast (women), colon, leukaemia, lymphoma, prostate (males), bladder, pancreatic, melanoma, nonmelanoma skin cancer, any skin cancer, ovarian (women), lung, brain, stomach, bile duct, uterine (women), oesophageal, liver, thyroid, bone, kidney, testicular (men) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 14 | Shalaby, 2016 | Case-control | USA | 108 PD patients 124 non-PD controls | 127 (54.7%) | 71.4 (7.94) |
| Cancer in general, basal cell, squamous integumentary, brain, squamous mesodermal, breast (women), lymphoma, lymphoma, myeloma, leukaemia, oral cavity/pharynx, uterine (women), ovarian (women), prostate (men), urinary/bladder, kidney, thyroid, gastric, colon, liver, pancreas, unspecified | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: PD: Parkinson’s Disease; NR: Not reported; BMI: Body mass index; GI: Gastrointestinal. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Subgroup analysis comparing cancer risk after PD diagnosis in LRRK2-G2019S mutation carriers and idiopathic PD patients included six studies. Three studies were included in the primary analysis [13–15] while three [16–18] were identified during the initial database search. The characteristics of these six studies are summarized in Supplementary Table 3.
Similarly, analysis comparing the cancer risk after PD diagnosis between female and male PD patients included four studies. Three studies [4, 19, 20] were included in the primary analysis, while one [6] was identified during the initial database search. The characteristics of the four studies are summarized in Supplementary Table 4.
General cancer risks and heterogeneity of studies
In this study, PD was associated with a reduced relative risk of subsequent cancer development (RR = 0.87, 95% CI = 0.81–0.93; data not shown). This association held true even after sensitivity analysis (RR = 0.87, 95% CI = 0.80–0.93; Figure 2). This is consistent with previous studies indicating an inverse relationship between PD and cancer.
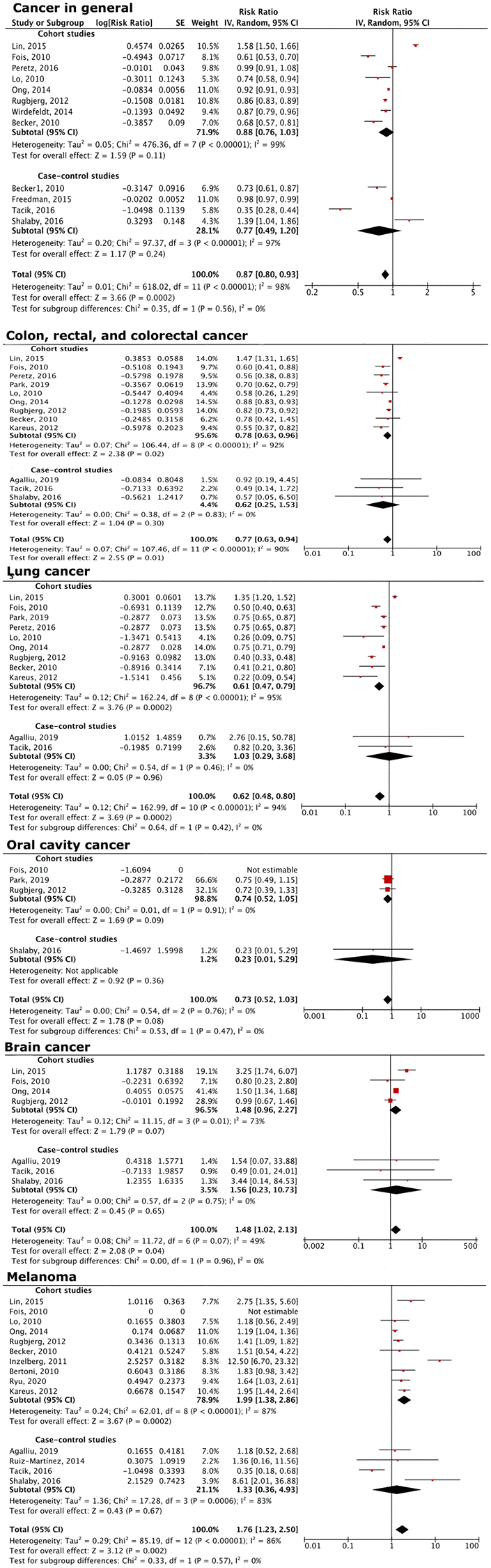
Figure 2. Forest plot of the association between PD and overall cancer risk, as well as that of specific cancers. PD patients had decreased overall cancer risks, and decreased risks of colon, rectal, colorectal, lung, oral cavity, brain cancers, and melanoma, compared to the general population.
Risk of specific cancers
Subgroup analysis revealed that PD is associated with a decrease in smoking-related cancers, including colon, rectal, and colorectal cancer (RR = 0.77, 95% CI = 0.63–0.94), lung cancer (RR = 0.62, 95% CI = 0.48–0.80), and oral cancers (RR = 0.73, 95% CI = 0.52–1.03; Figure 2), even though statistical significance was not reached for oral cancer.
The subgroup analysis also showed that PD was associated with an increased risk of brain cancers (RR = 1.48, 95% CI = 1.02–2.13) and melanoma (RR = 1.76, 95% CI = 1.23–2.50; Figure 2). These conclusions are consistent with earlier findings [9, 21, 22].
Increased cancer risks in LRRK2-G2019S PD patients
A comparison of subsequent cancer risk in LRRK2-G2019S PD and idiopathic PD patients revealed that LRRK2-G2019S PD patients had an increased risk of cancer in general (RR = 1.26, 95% CI = 1.09–1.46; Figure 3). This increase was particularly seen in brain (RR = 2.41, 95% CI = 1.06–5.50), breast (RR = 2.57, 95% CI = 1.19–5.58), colon (RR = 1.83, 95% CI = 1.13–2.99), and hematological cancers (RR = 2.05, 95% CI = 1.07–3.92; Figure 3).
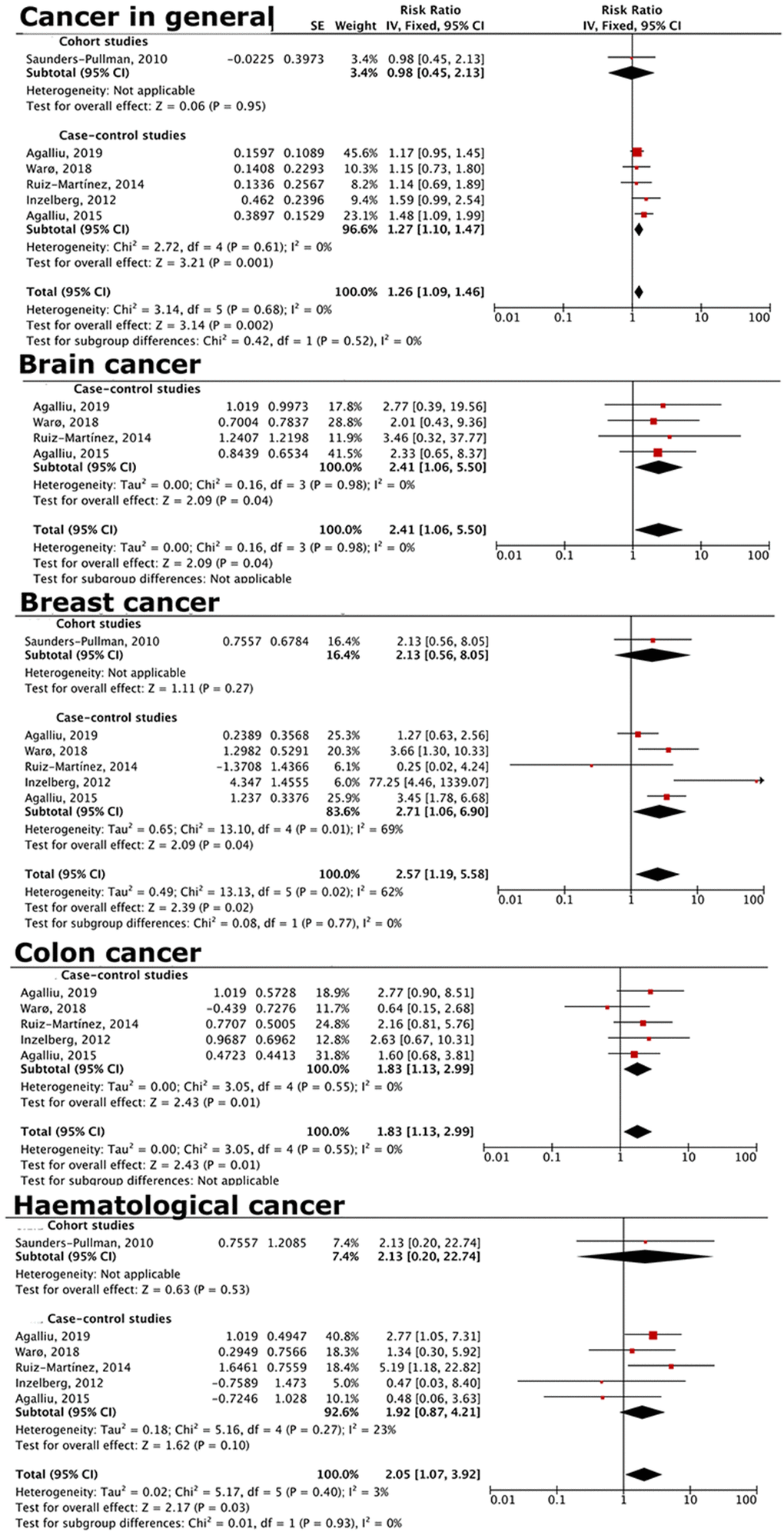
Figure 3. Forest plot comparing risks of cancer in general and specific cancers for LRRK2-PD vs. idiopathic PD patients. LRRK2-PD patients had higher risk of overall cancer, as well as brain, breast, colon, and hematological cancers.
Decreased cancer risks in female PD patients
Female PD patients have a decreased general cancer risk compared to male PD patients in this analysis (RR = 0.83, 95% CI = 0.69–0.98; Figure 4). In terms of specific cancers, there was a decreased risk of bladder (RR = 0.21, 95% CI = 0.14–0.32), colon (RR = 0.55, 95% CI = 0.36–0.83), hematological (RR = 0.52, 95% CI = 0.36–0.75), kidney (RR = 0.29, 95% CI = 0.24–0.35), liver (RR = 0.39, 95% CI = 0.31–0.49), lung (RR = 0.51, 95% CI = 0.30–0.84), rectal (RR = 0.37, 95% CI = 0.32–0.44), and stomach cancer (RR = 0.40, 95% CI = 0.22–0.70; Figure 4).
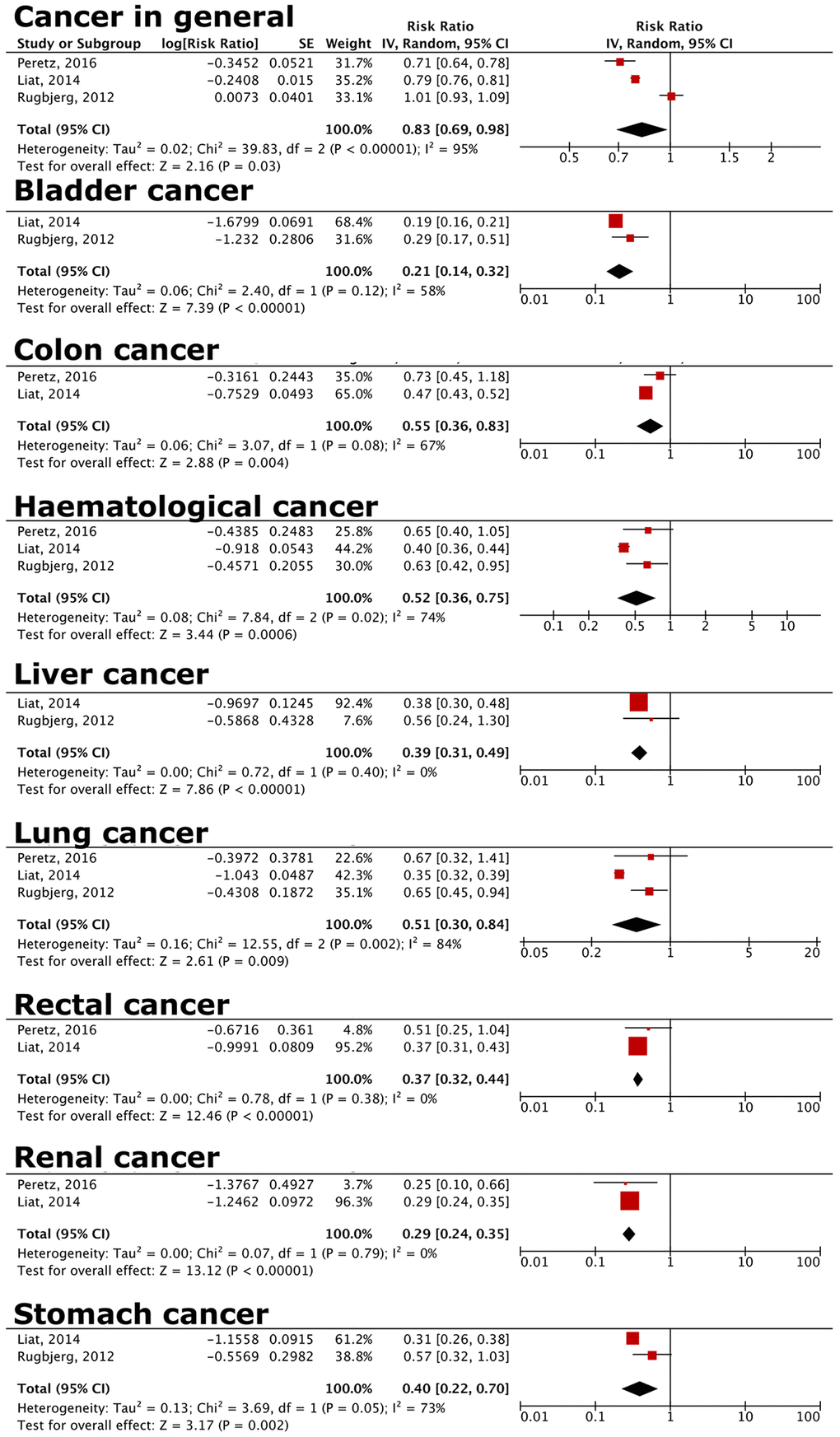
Figure 4. Forest plot comparing risks of cancer in general and specific cancers for female vs. male PD patients. Female PD patients have decreased risks of overall cancer, and bladder, colon, haematological, liver, lung, and rectal cancer compared to male PD patients. Details of specific cancers included in each cancer group are listed in Supplementary Table 6A–6C.
Discussion
We showed that PD patients have decreased subsequent cancer risks (RR = 0.87, 95% CI = 0.81–0.93), with a reduced risk of colon, rectal, and colorectal cancer (RR = 0.77, 95% CI = 0.63–0.94), lung cancer (RR = 0.62, 95% CI = 0.48–0.80). There was an increased brain cancer (R = 1.48, 95% CI = 1.02–2.13) and melanoma risk (R = 1.76, 95% CI = 1.23–2.50). Compared to idiopathic PD, LRRK2-G2019S carrier patients had an increased risk of cancer in general (RR = 1.26, 95% CI = 1.09–1.46), especially for brain (RR = 2.41, 95% CI = 1.06–5.50), breast (RR = 2.57, 95% CI = 1.19–5.58), colon (RR = 1.83, 95% CI = 1.13–2.99), and hematological cancers (RR = 2.05, 95% CI = 1.07–3.92). Female PD patients have a decreased general cancer risk compared to male PD patients in this analysis (RR = 0.83, 95% CI = 0.69–0.98).
Several hypotheses could explain the above observations. These include opposing molecular pathways between PD and cancer, lifestyle changes in PD patients following PD diagnosis, and an increased rate of healthcare utilization and surveillance among PD patients compared to non-PD individuals.
Opposing molecular pathways of PD and cancer
PD involves degeneration of the dopamine producing cells of the substantia nigra, while cancer, with its proliferative nature [23], lies on the opposite end of the spectrum. Several PD-related genes have been found to possibly mediate the relationship between PD and subsequent cancer. These genes include LRRK2, PARK2, a tumor suppressor gene, PARK5, coding for the ubiquitin carboxyl-terminal hydrolase-L1 (UCH-L1) enzyme involved in ubiquitin-recycling, PARK7 (DJ-1), a strong anti-oxidant, and PARK6 (PINK1), a cell death and cell cycle regulator [23]. Oxidative damage, alterations in protein ubiquitination, and cell cycle dysregulation have been implicated in cancer pathogenesis [24]. Therefore, the PARK family proteins involved both in PD and regulation of replication stress can possibly mediate both pathologies.
Lifestyle changes in PD patients
Amongst PD patients, a ‘Parkinsonian personality’ characterized by low novelty seeking (NS) and high harm avoidance (HA) behavior, possible resulting from decreased dopaminergic stimulation, has been described [25]. NS behaviors include impulsivity, reward seeking, and exploration of novel experiences, while HA behaviors include pessimism, worry, and avoidance due to uncertainty [25]. While epidemiological research in this domain is lacking, PD patients may possibly be engaging in less risky lifestyle behaviors like smoking and adopting healthier habits of increased physical activity and eating balanced diets. These lifestyle attributes are related to a decreased cancer risk [26], contributing to lower cancer risks seen in our study.
Increased healthcare utilization and surveillance in PD patients
Tremors, rigidity, and bradykinesia significantly reduces one’s ability to perform daily activities [27]. PD patients also tend to have more comorbidities, including obesity, diabetes mellitus, and cardiac pathologies [27].
Furthermore, PD treatment with dopaminergic agonists may lead to complications such as cardiac fibrosis and arrhythmias [27]. The combination of PD-related symptoms, multiple comorbidities, on top of PD treatment effects has necessitated increased expenditure and healthcare utilization rates among PD patients in countries like Brazil [28] and the United States [29]. In the United States, states with higher PD prevalence have increased awareness and recognition of PD symptoms, further driving healthcare seeking behaviours [29] and comprehensive medical care involving not only neurologists, but also internal medicine physicians [27].
This possibly explains, at least partly, the decreased general cancer risk amongst PD patients, through earlier detection and management.
Risks of specific cancers following PD diagnosis
Brain cancers
Emerging research has pointed towards the neuroprotective effects of the gut microbiome through reducing proinflammatory cytokine production, inducing secretion of the anti-inflammatory interleukin IL-10, and promoting development of Treg cells that play a role in immunosuppression [31]. These effects are due to metabolites produced by the microbiota, especially short chain fatty acids (SCFAs) that have anti-inflammatory, neuroprotective, and anti-oxidant effects [32]. It is also postulated that these metabolites and the mediators induced as a result, could affect blood-brain barrier integrity, influencing susceptibility to neural insults [31].
Gut microbiome biodiversity alteration in PD patients, specifically in the abundance of bacteria in the phylae Firmicutes, Bacteroidetes, and Proteobacteria [33], have been reported. Decreased microbial biodiversity likely led to decreased SCFA production and therefore neuroprotective effects, possibly explaining the increased brain cancer risks.
Melanoma
Melanoma has consistently been reported to be more prevalent among PD patients. Several lines of evidence, from shared risk factors, common biochemical pathways, and genes, have been put forth to explain this relationship.
Ye et al. (2020) [34] outlined several overlapping characteristics between PD and melanoma: In terms of ethnicity, PD and melanoma were more common in Whites, with both rates increased in individuals with fair skin tones and red hair. In terms of lifestyle behaviors, decreased smoking rates in PD patients were correlated with increased melanoma risks, while coffee consumption was associated with both a decreased PD and melanoma risk.
Biochemically, the pigmentation pathway is shared for melanin production in the skin and neuromelanin in the brain from tyrosine [11]. Melanin in the skin protects cells against DNA damage induced by UV radiation, while neuromelanin is a crucial neuroprotective pigment in the dopaminergic neurons by sequestering reactive oxygen species and metal ions [11]. Alterations in this common pathway resulting in decreased melanin and neuromelanin production may therefore make skin cells more susceptible to genetic instability, and dopaminergic neurons more vulnerable to oxidative damage, possibly linking PD and melanoma.
Loss of heterozygosity of PARK2, LRRK2 mutations causing neuronal cell death and neurotoxicity, BRAF kinase alterations, and PARK7 oncogene activation with subsequent melanoma development are possible underpinning genetic pathophysiologiy [11, 34].
The combined effect of common risk factors, shared biochemical pathways, and overlapping genes provide strong evidence linking the positive correlation between PD and melanoma occurrence.
Cancer risks in LRRK2-G2019S PD carriers
LRRK2, a protein kinase gene, is most commonly implicated in familial PD [35]. LRRK2 promotes aggregation of α-synuclein into Lewy bodies and tau tangles [35]. In addition, these mutations also contribute to neurodegeneration in PD by driving cells towards a pro-inflammatory state, increasing oxidative stress, and disrupting mitochondrial functions and the autophagy-lysosomal system [35].
Inflammation, oxidative damage, mitochondrial dysfunction and disruption of the autophagy-lysosomal system are processes unique not only to PD development, but also cancer [36]. It is therefore unsurprising to find increased cancer risks amongst LRRK2-G2019S PD patients in our study, with LRRK2 promoting PD-associated neurodegeneration and cancer-related pathogenesis pathways. Interestingly, in addition to the expression of various LRRK2 mutations, namely R1441C, R1441G, R1441H, and G2019S in the brain [37], LRRK2 has been found in peripheral blood cells [38], gut [39], and in the lung and breast [40]. These expression patterns mirror our findings of increased brain, breast, colon, and hematological cancers, further strengthening the association between LRRK2 and cancer and increasing the value of targeting LRRK2 for therapeutic treatment of both PD and cancer.
LRRK2 has been identified to be a candidate prognostic biomarker for clear cell renal cell carcinoma [41]. Yang et al. [41] showed that there was up regulation (confirmed on immunohistochemical and protein studies) of LRRK2 expression that was associated with DNA methylation in this cancer. Interestingly, somatic LRRK2 truncating or deletion mutations have been identified in malignant mesothelioma and LRRK2 expression was absent or downregulated in primary tumor cell lines [42]. How this tumor suppressor change predispose to cancers still needs to be investigated. A specific LRRK2 rs10878441 CC genotype has been linked to a poorer prognosis in Chinese breast cancer patients [43]. High LRRK2 expression has also been associated with poorer survival in ovarian cancer [44]. It was also demonstrated that inhibiting LRRK2 promoted toxicity of PARP inhibitor by reducing homologous recombination-mediated DNA double strand break repair [44]. LRRK2 is also involved in the ATM-Mdm2-p53 pathway that regulates cell proliferation in response to DNA damage [45]. These clinical and experimental observations provide support linking LRRK2 to cancer.
Decreased cancer risk in female PD patients
The protective role of estrogen has been well documented in dopaminergic neurons [46], adipose tissues, skeletal muscles, macrophages, and immune cells [47]. Estrogen is neuroprotective, reducing the oxidative damage from dopamine, iron, and calcium [46] that contribute to PD development. In other non-neuronal cells, estrogen modulates fuel metabolism, specifically of lipids, amino acids, and glucose [47], which are commonly dysregulated in cancer cells [36]. This can possibly explain why females with higher lifetime estrogen exposures, and women who have used estrogen therapy have decreased PD [46], as well as cancer risks found in our analysis.
LRRK2 and estrogen have opposing effects on similar domains of inflammation, oxidative stress, and metabolism, with the former toxic and the latter protective in neurons and non-neuronal cells. It may therefore be reasonable to postulate that LRRK2 mutation effects may override the protection afforded by estrogen in female carriers, resulting in more severe PD symptoms and increased cancer risks.
Implications of study
The identification of potential healthier lifestyle choices and more frequent healthcare monitoring provides increased impetus to encourage PD patients to adopt lifestyle changes and follow-up adherence to reduce both PD progression and cancer development. Furthermore, the involvement of PARK family genes in PD and cancer pathogenesis opens a new therapeutic angle through targeted downregulation of these genes to reduce risk of contracting either or both pathologies.
While general cancer risk in PD patients was decreased, increased risks of brain cancers and melanoma were found. This prompts a need for more frequent screening for early signs and symptoms of these neoplasms. The gut-brain microbiome’s effects and decreased gut biodiversity in PD patients suggest that diet regulation and probiotics to promote improved gut health may be a preventive measure against brain cancers. The common pathway involved in melanin and neuromelanin production, implicated in both melanoma and PD, indicates a possible treatment strategy focused on altering the enzyme kinetics as a means of reducing melanoma risks.
The opposing effects of LRRK2 and estrogen on PD and cancer development highlight the potential utility of estrogen replacement to slow PD progression and severity, as well as cancer development in PD patients. This is supported by a prior study [48] indicating that estrogen has beneficial effects on neurons in the nigrostriatum. While further analysis is required to determine the contribution of gender and estrogen effects on the increased cancer risks in LRRK2-PD patients, our findings suggest the potential utility of hormonal therapy as a dual preventive measure for PD and cancer.
Comparison to previous meta-analysis
Two other meta-analyses investigating the relationship between PD and subsequent cancer development were conducted in 2010 [49], 2019 [50] respectively. However, our study has several strengths.
First, we uniformly extracted unadjusted RRs from the included studies, or manually calculated it from the data provided in the papers or by the authors. In contrast, Bajaj et al. (2010) [49] and Zhang and Liu (2019) [50] extracted and treated adjusted and unadjusted ORs, RRs, SIRs, and HRs equally, under the assumption that PD and cancer are rare conditions. However, with increased prevalence of both diseases [51, 52], it is incorrect to make the assumption, and hence only RRs would reflect the true risk of developing cancer after PD. Additionally, since different studies adjusted their results based on different factors, the actual PD effect on subsequent cancer risk can only be compared equally using unadjusted RRs, as in this case.
Second, we provided a concise account of cancer risks in specific PD populations, comparing between male and female patients and between LRRK2-PD and idiopathic PD patients. Although the negative association between PD and subsequent cancer development found in this study was similar to that of previous meta-analysis [49, 50] additional analyses conducted showed that the decreased risks were more significant in female and idiopathic PD patients.
Identification of specific at-risk subgroups can facilitate management strategies encompassing increased screening and surveillance, lifestyle changes, and hormonal replacement as promising therapeutic options. This study therefore provides a holistic review of not just the relationship shared between PD and cancer, but the multiple factors and probable treatment options for PD patients.
Study limitations
First, the effects of comorbidities and level of tobacco use could not be analyzed as the information were unavailable. Second, as the included studies were mostly conducted in Western populations, the generalizability of the current findings to an Asian population is unclear.
In conclusion, we demonstrated that PD patients have a reduced risk of colon, rectal, colorectal cancer and lung cancers and an increased risk of brain cancer and melanoma. LRRK2-G2019S carriers have an increased cancer risk, in particular for brain, breast, colon and blood cancers and female gender was associated with a reduced risk of bladder colon, hematological, kidney, liver, lung, rectal, and stomach cancer.
Future gene-environmental and lifestyle prospective studies will be able to identify factors that may modulate the association between PD and cancer. Functional studies in experimental models to elucidate the pathophysiology of PD and cancer contributed by kinase functions and targets of LRRK2 in the cell cycle may facilitate identification of therapeutic targets.
Methods
Search strategy
Database search was conducted on PubMed, Web of Science, and SCOPUS to identify published articles between 1 January 2010-30 August 2020 investigating the incidence and prevalence of cancer following PD diagnosis. “Parkinson disease”, “Neoplasm”, “Cancer”, and “Epidemiological studies” were entered as search topics or medical subject headings and connected with Boolean operators. Where applicable, filters were applied to limit studies to those conducted in humans, in English, and were in full text. The search strategy is detailed in Supplementary Methods.
Searches were performed for each database and were updated until 1 June 2021.Titles and abstracts were screened independently by two reviewers (J.Y.S.L and J.H.N) against a set of pre-defined eligibility criteria. Potentially eligible studies were selected for full-text analysis. Additional relevant studies were identified by manually examining the references provided in the published studies identified initially during the database search.
Eligibility criteria
Studies eligible for inclusion in the primary analysis investigated the impact of PD on subsequent cancer development. Data were reviewed to ensure that subjects recruited in the studies were cancer-free before PD diagnosis, regardless of subsequent cancer development. This was done through appraising the study cohorts employed between two independent reviewers. Studies investigating cancer’s effect on subsequent PD development, and on cancer risk in relatives of PD patients were not considered. Resolution of disagreements were by consensus after discussion.
Of the studies identified through the initial database search, eight investigated the effect of pharmaceutical PD treatment on cancer risk [17, 53–59], five looked at the impact of genetic variants, such as LRRK2 on cancer development [13, 16–18, 60] and six investigated PD’s effect on the development of specific cancers [3, 22, 56, 58, 61, 62]. Another study [63] investigated PD’s impact on subsequent cancer development but did not report the outcome statistics, and was excluded from primary analysis. While these studies were not included in the primary analysis, they were included in subgroup analyses to determine the effect of gender, PD treatment, PD-related genetic variants, or PD’s effect on specific cancers.
Studies meeting the eligibility criteria were then analyzed in detail to ensure that there were no overlapping study cohorts. Four Taiwanese [6, 9, 64, 65] and two Israeli studies [19, 66] utilized the same study cohort in their respective countries. The study that employed the most study subjects and tracked the development of the most cancers in each of the two countries was ultimately chosen.
Exclusion criteria
This analysis excluded papers that were non-English and conducted in non-human subjects. Non-original research papers, laboratory-based, and epidemiological studies with no clinical characteristics reported were also not considered. Case series and case reports were excluded according to recommendations by the Cochrane Statistical Methods Group and in accordance with methodologies of previously published meta-analyses [67].
Data extraction
Information from the studies were extracted by two independent reviewers (J.Y.S.L and J.H.N). These included the number of subjects recruited, demographic details inclusive of the mean age, gender distribution, and country where the study was conducted. Information pertaining to the study included the study design, the adjustment applied to the outcome variables (risk ratio; RR, hazard ratio; HR, odds ratio; OR, and standardised incidence rate; SIR).
Outcome
Overall and specific cancer risk analyzed by each study and the number of subjects who developed each kind of cancer were extracted. We used the unadjusted RR as the common outcome measurement for comparison between all studies. If only adjusted RRs or adjusted or unadjusted ORs were reported, unadjusted RR values were manually calculated.
Unadjusted HRs and SIRs were considered interchangeable with the unadjusted RR [68]. If studies reported only adjusted HRs, effort was invested to contact the authors to obtain the unadjusted values. For conversion of adjusted RRs and adjusted ORs to unadjusted RRs, and for ACR computation, we contacted the authors of the studies to determine if the number of cases of subsequent cancer in PD patients and control subjects were reported.
Of the fourteen papers, three provided adjusted HRs [64, 69, 70], two provided unadjusted SIRs [4, 19], one provided unadjusted ORs [15], three provided adjusted RRs [20, 71, 72], while five provided adjusted ORs [14, 73–76]. Of the studies reporting adjusted RRs and adjusted ORs, only one author [14] was able to supplement with unadjusted ORs. Other authors were unable to assist in our analysis due to a lack of access or unavailability of study data.
Assessment of study quality
The risk of bias (RoB) analysis was conducted using the Newcastle-Ottawa Scale (NOS). NOS scores were subsequently converted to Agency for Healthcare Research and Quality (AHRQ) ratings to classify the studies as of ‘Good’, ‘Fair’ or ‘Poor’ quality. The RoB and AHQR framework used for study assessment in this meta-analysis are detailed in Supplementary Methods. Two reviewers (J.Y.S.L and J.H.N) assessed the quality of all included studies and discussed discrepancies until consensus was reached. The risk of bias analysis for cohort and case-control studies are detailed in Supplementary Table 5A and 5B respectively.
Subgroup analyses
Besides analyzing the relationship between PD and the risk of subsequent cancer in general, and that of specific cancers through the primary and subgroup analysis, secondary analyses were conducted. These subgroup analyses investigated the effect of genetic variants implicated in PD development, PD treatment, and gender on subsequent cancer development. Studies included in these subgroup analyses were identified during the database search but did not meet the inclusion criteria for primary analysis. We conducted subgroup analyses using these studies since both cancer and PD are multifactorial. Similar variables were extracted for the secondary analyses as for the primary analyses. Details and results of the studies included are provided in the subsequent sections.
Statistical analysis
Review Manager (Review Manager (RevMan) [Computer program]. Version 5.4. The Cochrane Collaboration, 2020) was used for data analysis in the present study. Type I error was fixed at 5% and 95% confidence intervals were reported for all calculations.
Heterogeneity between studies
Heterogeneity between the studies was evaluated using the Q test and I2. P values for the I2 statistics were computed by chi-square distribution of Cochran Q test. Random effect models were used to pool the results and to allow for differences in the treatment effect from study to study (sampling variability across studies). Subgroup analyses on PD’s effect on subsequent development of specific cancers were conducted to assess the heterogeneity source.
Sensitivity analysis
Sensitivity analysis was conducted to assess the robustness of the present study. The meta-analysis was conducted twice, once with all studies included, and once after excluding studies rated ‘Poor’ by AHRQ standards for sensitivity analysis.
Publication bias
Publication bias of the included studies was assessed using the funnel plot (Supplementary Figure 1A–1C).
Author Contributions
Joon Yan Selene Lee extracted and analysed the relevant data and contributed substantially to the drafting of the manuscript. Eng King Tan provided clinical expertise and advice and was involved in editing the manuscript. Seyed Ehsan Saffari contributed to the statistical analysis of the extracted data. Jing Han Ng was involved in the review of the manuscript. All authors confirm the final version of the manuscript and contributed to the write-up.
Acknowledgments
We thank the National Medical Research Council for support (STaR and PD LCG 0002 grants) and Dr Agalliu of Albert Einstein College of Medicine, NY, USA, for providing relevant data included in this meta-analysis.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Funding
This work was supported by the National Medical Research Council.
References
- 1. Jankovic J, Tan EK. Parkinson's disease: etiopathogenesis and treatment. J Neurol Neurosurg Psychiatry. 2020; 91:795–808. https://doi.org/10.1136/jnnp-2019-322338 [PubMed]
- 2. Epidemiology & Disease Control Division, Ministry of Health, Singapore, and Institute for Health Metrics and Evaluation. The Burden of Disease in Singapore, 1990–2017: An overview of the Global Burden of Disease Study 2017 results. Seattle, WA: IHME. 2019. https://www.moh.gov.sg/docs/librariesprovider5/default-document-library/gbd_2017_singapore_reportce6bb0b3ad1a49c19ee6ebadc1273b18.pdf.
- 3. Constantinescu R, Romer M, Kieburtz K, and DATATOP Investigators of the Parkinson Study Group. Malignant melanoma in early Parkinson's disease: the DATATOP trial. Mov Disord. 2007; 22:720–2. https://doi.org/10.1002/mds.21273 [PubMed]
- 4. Rugbjerg K, Friis S, Lassen CF, Ritz B, Olsen JH. Malignant melanoma, breast cancer and other cancers in patients with Parkinson's disease. Int J Cancer. 2012; 131:1904–11. https://doi.org/10.1002/ijc.27443 [PubMed]
- 5. Fiala KH, Whetteckey J, Manyam BV. Malignant melanoma and levodopa in Parkinson's disease: causality or coincidence? Parkinsonism Relat Disord. 2003; 9:321–7. https://doi.org/10.1016/s1353-8020(03)00040-3 [PubMed]
- 6. Sun LM, Liang JA, Chang SN, Sung FC, Muo CH, Kao CH. Analysis of Parkinson's disease and subsequent cancer risk in Taiwan: a nationwide population-based cohort study. Neuroepidemiology. 2011; 37:114–9. https://doi.org/10.1159/000331489 [PubMed]
- 7. Sandyk R. Accelerated growth of malignant melanoma by levodopa in Parkinson's disease and role of the pineal gland. Int J Neurosci. 1992; 63:137–40. https://doi.org/10.3109/00207459208986663 [PubMed]
- 8. Olsen JH, Friis S, Frederiksen K. Malignant melanoma and other types of cancer preceding Parkinson disease. Epidemiology. 2006; 17:582–7. https://doi.org/10.1097/01.ede.0000229445.90471.5e [PubMed]
- 9. Tang CF, Lu MK, Muo CH, Tsai CH, Kao CH. Increased risk of brain tumor in patients with Parkinson's disease: a nationwide cohort study in Taiwan. Acta Neurol Scand. 2016; 134:148–53. https://doi.org/10.1111/ane.12524 [PubMed]
- 10. Driver JA, Logroscino G, Buring JE, Gaziano JM, Kurth T. A prospective cohort study of cancer incidence following the diagnosis of Parkinson's disease. Cancer Epidemiol Biomarkers Prev. 2007; 16:1260–5. https://doi.org/10.1158/1055-9965.epi-07-0038 [PubMed]
- 11. Bose A, Petsko GA, Eliezer D. Parkinson's Disease and Melanoma: Co-Occurrence and Mechanisms. J Parkinsons Dis. 2018; 8:385–98. https://doi.org/10.3233/JPD-171263 [PubMed]
- 12. Gieseler F, Gaertner L, Thaden E, Theobald W. Cancer Diagnosis: A Trauma for Patients and Doctors Alike. Oncologist. 2018; 23:752–4. https://doi.org/10.1634/theoncologist.2017-0478 [PubMed]
- 13. Saunders-Pullman R, Barrett MJ, Stanley KM, Luciano MS, Shanker V, Severt L, Hunt A, Raymond D, Ozelius LJ, Bressman SB. LRRK2 G2019S mutations are associated with an increased cancer risk in Parkinson disease. Mov Disord. 2010; 25:2536–41. https://doi.org/10.1002/mds.23314 [PubMed]
- 14. Agalliu I, Ortega RA, Luciano MS, Mirelman A, Pont-Sunyer C, Brockmann K, Vilas D, Tolosa E, Berg D, Warø B, Glickman A, Raymond D, Inzelberg R, et al. Cancer outcomes among Parkinson's disease patients with leucine rich repeat kinase 2 mutations, idiopathic Parkinson's disease patients, and nonaffected controls. Mov Disord. 2019; 34:1392–8. https://doi.org/10.1002/mds.27807 [PubMed]
- 15. Ruiz-Martínez J, de la Riva P, Rodríguez-Oroz MC, Mondragón Rezola E, Bergareche A, Gorostidi A, Gago B, Estanga A, Larrañaga N, Sarasqueta C, López de Munain A, Martí Massó JF. Prevalence of cancer in Parkinson's disease related to R1441G and G2019S mutations in LRRK2. Mov Disord. 2014; 29:750–5. https://doi.org/10.1002/mds.25778 [PubMed]
- 16. Agalliu I, San Luciano M, Mirelman A, Giladi N, Waro B, Aasly J, Inzelberg R, Hassin-Baer S, Friedman E, Ruiz-Martinez J, Marti-Masso JF, Orr-Urtreger A, Bressman S, Saunders-Pullman R. Higher frequency of certain cancers in LRRK2 G2019S mutation carriers with Parkinson disease: a pooled analysis. JAMA Neurol. 2015; 72:58–65. https://doi.org/10.1001/jamaneurol.2014.1973 [PubMed]
- 17. Inzelberg R, Cohen OS, Aharon-Peretz J, Schlesinger I, Gershoni-Baruch R, Djaldetti R, Nitsan Z, Ephraty L, Tunkel O, Kozlova E, Inzelberg L, Kaplan N, Fixler Mehr T, et al. The LRRK2 G2019S mutation is associated with Parkinson disease and concomitant non-skin cancers. Neurology. 2012; 78:781–6. https://doi.org/10.1212/WNL.0b013e318249f673 [PubMed]
- 18. Warø BJ, Aasly JO. Exploring cancer in LRRK2 mutation carriers and idiopathic Parkinson's disease. Brain Behav. 2017; 8:e00858. https://doi.org/10.1002/brb3.858 [PubMed]
- 19. Peretz C, Gurel R, Rozani V, Gurevich T, El-Ad B, Tsamir J, Giladi N. Cancer incidence among Parkinson's disease patients in a 10-yrs time-window around disease onset: A large-scale cohort study. Parkinsonism Relat Disord. 2016; 28:68–72. https://doi.org/10.1016/j.parkreldis.2016.04.028 [PubMed]
- 20. Ong EL, Goldacre R, Goldacre M. Differential risks of cancer types in people with Parkinson's disease: a national record-linkage study. Eur J Cancer. 2014; 50:2456–62. https://doi.org/10.1016/j.ejca.2014.06.018 [PubMed]
- 21. Ritz B, Ascherio A, Checkoway H, Marder KS, Nelson LM, Rocca WA, Ross GW, Strickland D, Van Den Eeden SK, Gorell J. Pooled analysis of tobacco use and risk of Parkinson disease. Arch Neurol. 2007; 64:990–7. https://doi.org/10.1001/archneur.64.7.990 [PubMed]
- 22. Inzelberg R, Rabey JM, Melamed E, Djaldetti R, Reches A, Badarny S, Hassin-Baer S, Cohen O, Trau H, Aharon-Peretz J, Milo R, Schwartz M, Huberman M, et al. High prevalence of malignant melanoma in Israeli patients with Parkinson's disease. J Neural Transm (Vienna). 2011; 118:1199–207. https://doi.org/10.1007/s00702-011-0580-2 [PubMed]
- 23. D'Amelio M, Ragonese P, Sconzo G, Aridon P, Savettieri G. Parkinson's disease and cancer: insights for pathogenesis from epidemiology. Ann N Y Acad Sci. 2009; 1155:324–34. https://doi.org/10.1111/j.1749-6632.2008.03681.x [PubMed]
- 24. Gaillard H, García-Muse T, Aguilera A. Replication stress and cancer. Nat Rev Cancer. 2015; 15:276–89. https://doi.org/10.1038/nrc3916 [PubMed]
- 25. Poletti M, Bonuccelli U. Personality traits in patients with Parkinson's disease: assessment and clinical implications. J Neurol. 2012; 259:1029–38. https://doi.org/10.1007/s00415-011-6302-8 [PubMed]
- 26. LoConte NK, Gershenwald JE, Thomson CA, Crane TE, Harmon GE, Rechis R. Lifestyle Modifications and Policy Implications for Primary and Secondary Cancer Prevention: Diet, Exercise, Sun Safety, and Alcohol Reduction. Am Soc Clin Oncol Educ Book. 2018; 38:88–100. https://doi.org/10.1200/EDBK_200093 [PubMed]
- 27. Csoti I, Jost WH, Reichmann H. Parkinson's disease between internal medicine and neurology. J Neural Transm (Vienna). 2016; 123:3–17. https://doi.org/10.1007/s00702-015-1443-z [PubMed]
- 28. Bovolenta TM, de Azevedo Silva SM, Arb Saba R, Borges V, Ferraz HB, Felicio AC. Systematic Review and Critical Analysis of Cost Studies Associated with Parkinson's Disease. Parkinsons Dis. 2017; 2017:3410946. https://doi.org/10.1155/2017/3410946 [PubMed]
- 29. Mantri S, Fullard ME, Beck J, Willis AW. State-level prevalence, health service use, and spending vary widely among Medicare beneficiaries with Parkinson disease. NPJ Parkinsons Dis. 2019; 5:1. https://doi.org/10.1038/s41531-019-0074-8 [PubMed]
- 30. Gallo V, Vineis P, Cancellieri M, Chiodini P, Barker RA, Brayne C, Pearce N, Vermeulen R, Panico S, Bueno-de-Mesquita B, Vanacore N, Forsgren L, Ramat S, et al. Exploring causality of the association between smoking and Parkinson's disease. Int J Epidemiol. 2019; 48:912–25. https://doi.org/10.1093/ije/dyy230 [PubMed]
- 31. Mehrian-Shai R, Reichardt JKV, Harris CC, Toren A. The Gut-Brain Axis, Paving the Way to Brain Cancer. Trends Cancer. 2019; 5:200–7. https://doi.org/10.1016/j.trecan.2019.02.008 [PubMed]
- 32. Bullich C, Keshavarzian A, Garssen J, Kraneveld A, Perez-Pardo P. Gut Vibes in Parkinson's Disease: The Microbiota-Gut-Brain Axis. Mov Disord Clin Pract. 2019; 6:639–51. https://doi.org/10.1002/mdc3.12840 [PubMed]
- 33. Boulos C, Yaghi N, El Hayeck R, Heraoui GN, Fakhoury-Sayegh N. Nutritional Risk Factors, Microbiota and Parkinson's Disease: What Is the Current Evidence? Nutrients. 2019; 11:1896. https://doi.org/10.3390/nu11081896 [PubMed]
- 34. Ye Q, Wen Y, Al-Kuwari N, Chen X. Association Between Parkinson's Disease and Melanoma: Putting the Pieces Together. Front Aging Neurosci. 2020; 12:60. https://doi.org/10.3389/fnagi.2020.00060 [PubMed]
- 35. Li JQ, Tan L, Yu JT. The role of the LRRK2 gene in Parkinsonism. Mol Neurodegener. 2014; 9:47. https://doi.org/10.1186/1750-1326-9-47 [PubMed]
- 36. Giampazolias E, Tait SW. Mitochondria and the hallmarks of cancer. FEBS J. 2016; 283:803–14. https://doi.org/10.1111/febs.13603 [PubMed]
- 37. Manzoni C. The LRRK2-macroautophagy axis and its relevance to Parkinson's disease. Biochem Soc Trans. 2017; 45:155–62. https://doi.org/10.1042/BST20160265 [PubMed]
- 38. Padmanabhan S, Lanz TA, Gorman D, Wolfe M, Joyce A, Cabrera C, Lawrence-Henderson R, Levers N, Joshi N, Ma TC, Liong C, Narayan S, Alcalay RN, et al. An Assessment of LRRK2 Serine 935 Phosphorylation in Human Peripheral Blood Mononuclear Cells in Idiopathic Parkinson's Disease and G2019S LRRK2 Cohorts. J Parkinsons Dis. 2020; 10:623–9. https://doi.org/10.3233/JPD-191786 [PubMed]
- 39. Maekawa T, Shimayama H, Tsushima H, Kawakami F, Kawashima R, Kubo M, Ichikawa T. LRRK2: An Emerging New Molecule in the Enteric Neuronal System That Quantitatively Regulates Neuronal Peptides and IgA in the Gut. Dig Dis Sci. 2017; 62:903–12. https://doi.org/10.1007/s10620-017-4476-3 [PubMed]
- 40. Jung K, Choi JS, Koo BM, Kim YJ, Song JY, Sung M, Chang ES, Noh KW, An S, Lee MS, Song K, Lee H, Kim RN, et al. TM4SF4 and LRRK2 Are Potential Therapeutic Targets in Lung and Breast Cancers through Outlier Analysis. Cancer Res Treat. 2021; 53:9–24. https://doi.org/10.4143/crt.2020.434 [PubMed]
- 41. Yang C, Pang J, Xu J, Pan H, Li Y, Zhang H, Liu H, Xiao SY. LRRK2 is a candidate prognostic biomarker for clear cell renal cell carcinoma. Cancer Cell Int. 2021; 21:343. https://doi.org/10.1186/s12935-021-02047-y [PubMed]
- 42. Cheung M, Kadariya Y, Sementino E, Hall MJ, Cozzi I, Ascoli V, Ohar JA, Testa JR. Novel LRRK2 mutations and other rare, non-BAP1-related candidate tumor predisposition gene variants in high-risk cancer families with mesothelioma and other tumors. Hum Mol Genet. 2021; 30:1750–61. https://doi.org/10.1093/hmg/ddab138 [PubMed]
- 43. Zhang L, Han L, Huang Y, Feng Z, Wang X, Li H, Song F, Liu L, Li J, Zheng H, Wang P, Song F, Chen K. SNPs within microRNA binding sites and the prognosis of breast cancer. Aging (Albany NY). 2021; 13:7465–80. https://doi.org/10.18632/aging.202612 [PubMed]
- 44. Chen L, Hou J, Zeng X, Guo Q, Deng M, Kloeber JA, Tu X, Zhao F, Wu Z, Huang J, Luo K, Kim W, Lou Z. LRRK2 inhibition potentiates PARP inhibitor cytotoxicity through inhibiting homologous recombination-mediated DNA double strand break repair. Clin Transl Med. 2021; 11:e341. https://doi.org/10.1002/ctm2.341 [PubMed]
- 45. Chen Z, Cao Z, Zhang W, Gu M, Zhou ZD, Li B, Li J, Tan EK, Zeng L. LRRK2 interacts with ATM and regulates Mdm2-p53 cell proliferation axis in response to genotoxic stress. Hum Mol Genet. 2017; 26:4494–505. https://doi.org/10.1093/hmg/ddx337 [PubMed]
- 46. Cerri S, Mus L, Blandini F. Parkinson's Disease in Women and Men: What's the Difference? J Parkinsons Dis. 2019; 9:501–15. https://doi.org/10.3233/JPD-191683 [PubMed]
- 47. Mauvais-Jarvis F, Clegg DJ, Hevener AL. The role of estrogens in control of energy balance and glucose homeostasis. Endocr Rev. 2013; 34:309–38. https://doi.org/10.1210/er.2012-1055 [PubMed]
- 48. Lee YH, Cha J, Chung SJ, Yoo HS, Sohn YH, Ye BS, Lee PH. Beneficial effect of estrogen on nigrostriatal dopaminergic neurons in drug-naïve postmenopausal Parkinson's disease. Sci Rep. 2019; 9:10531. https://doi.org/10.1038/s41598-019-47026-6 [PubMed]
- 49. Bajaj A, Driver JA, Schernhammer ES. Parkinson's disease and cancer risk: a systematic review and meta-analysis. Cancer Causes Control. 2010; 21:697–707. https://doi.org/10.1007/s10552-009-9497-6 [PubMed]
- 50. Zhang P, Liu B. Association between Parkinson's Disease and Risk of Cancer: A PRISMA-compliant Meta-analysis. ACS Chem Neurosci. 2019; 10:4430–9. https://doi.org/10.1021/acschemneuro.9b00498 [PubMed]
- 51. GBD 2016 Parkinson's Disease Collaborators. Global, regional, and national burden of Parkinson's disease, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018; 17:939–53. https://doi.org/10.1016/S1474-4422(18)30295-3 [PubMed]
- 52. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. https://doi.org/10.3322/caac.21492 [PubMed]
- 53. Schwid SR, Bausch J, Oakes D, Schuchter L, Tanner C, Forrest M, Lang AE, Shoulson I, Shoulson I, Hyson C, Oakes D, Flagg E, Rudolph A, et al, and PSG PRECEPT Investigators. Cancer incidence in a trial of an antiapoptotic agent for Parkinson's disease. Mov Disord. 2010; 25:1801–8. https://doi.org/10.1002/mds.23006 [PubMed]
- 54. Wang V, Chao TH, Hsieh CC, Lin CC, Kao CH. Cancer risks among the users of ergot-derived dopamine agonists for Parkinson's disease, a nationwide population-based survey. Parkinsonism Relat Disord. 2015; 21:18–22. https://doi.org/10.1016/j.parkreldis.2014.10.015 [PubMed]
- 55. Korhonen P, Kuoppamäki M, Prami T, Hoti F, Christopher S, Ellmén J, Aho V, Vahteristo M, Pukkala E, Haukka J. Entacapone and prostate cancer risk in patients with Parkinson's disease. Mov Disord. 2015; 30:724–8. https://doi.org/10.1002/mds.26140 [PubMed]
- 56. Bertoni JM, Arlette JP, Fernandez HH, Fitzer-Attas C, Frei K, Hassan MN, Isaacson SH, Lew MF, Molho E, Ondo WG, Phillips TJ, Singer C, Sutton JP, Wolf JE
Jr , and North American Parkinson's and Melanoma Survey Investigators. Increased melanoma risk in Parkinson disease: a prospective clinicopathological study. Arch Neurol. 2010; 67:347–52. https://doi.org/10.1001/archneurol.2010.1 [PubMed] - 57. Constantinescu R, Elm J, Auinger P, Sharma S, Augustine EF, Khadim L, Kieburtz K, and NET-PD Investigators. Malignant melanoma in early-treated Parkinson's disease: the NET-PD trial. Mov Disord. 2014; 29:263–5. https://doi.org/10.1002/mds.25734 [PubMed]
- 58. Boursi B, Mamtani R, Haynes K, Yang YX. Parkinson's disease and colorectal cancer risk-A nested case control study. Cancer Epidemiol. 2016; 43:9–14. https://doi.org/10.1016/j.canep.2016.05.007 [PubMed]
- 59. Major JM, Dong D, Cunningham F, By K, Hur K, Shih DC, Jiang R, Podskalny GD, Wei X, Pinheiro S, Bird ST, Keeton S, Graham DJ. Entacapone and prostate cancer in Parkinson's disease patients: A large Veterans Affairs healthcare system study. Parkinsonism Relat Disord. 2018; 53:46–52. https://doi.org/10.1016/j.parkreldis.2018.04.035 [PubMed]
- 60. Allegra R, Tunesi S, Cilia R, Pezzoli G, Goldwurm S. LRRK2-G2019S mutation is not associated with an increased cancer risk: a kin-cohort study. Mov Disord. 2014; 29:1325–6. https://doi.org/10.1002/mds.25969 [PubMed]
- 61. Ryu HJ, Park JH, Choi M, Jung JH, Han K, Kwon DY, Kim DH, Park YG. Parkinson's disease and skin cancer risk: a nationwide population-based cohort study in Korea. J Eur Acad Dermatol Venereol. 2020; 34:2775–80. https://doi.org/10.1111/jdv.16462 [PubMed]
- 62. Jespersen CG, Nørgaard M, Borre M. Parkinson's disease and risk of prostate cancer: A Danish population-based case-control study, 1995-2010. Cancer Epidemiol. 2016; 45:157–61. https://doi.org/10.1016/j.canep.2016.11.002 [PubMed]
- 63. Kareus SA, Figueroa KP, Cannon-Albright LA, Pulst SM. Shared predispositions of parkinsonism and cancer: a population-based pedigree-linked study. Arch Neurol. 2012; 69:1572–7. https://doi.org/10.1001/archneurol.2012.2261 [PubMed]
- 64. Lin PY, Chang SN, Hsiao TH, Huang BT, Lin CH, Yang PC. Association Between Parkinson Disease and Risk of Cancer in Taiwan. JAMA Oncol. 2015; 1:633–40. https://doi.org/10.1001/jamaoncol.2015.1752 [PubMed]
- 65. Liao KF, Lin CL, Lai SW, Chen WC. Parkinson’s disease and risk of pancreatic cancer: a population-based case-control study in Taiwan. Neurol Asia. 2015; 20:251–5.
- 66. Lerman S, Amichai B, Weinstein G, Shalev V, Chodick G. Parkinson's Disease, Melanoma, and Keratinocyte Carcinoma: A Population-Based Study. Neuroepidemiology. 2018; 50:168–73. https://doi.org/10.1159/000487855 [PubMed]
- 67. Peryer G, Golder S, Junqueira DR, Vohra S, Loke YK. Chapter 19: Adverse effects. Cochrane Training. 2021. https://training.cochrane.org/handbook/current/chapter-19.
- 68. Higgins JPT, Li T, Deeks JJ. Chapter 6: Choosing effect measures and computing estimates of effect. Cochrane Training. 2021. https://training.cochrane.org/ handbook/current/chapter-06.
- 69. Park JH, Kim DH, Park YG, Kwon DY, Choi M, Jung JH, Han K. Cancer risk in patients with Parkinson's disease in South Korea: A nationwide, population-based cohort study. Eur J Cancer. 2019; 117:5–13. https://doi.org/10.1016/j.ejca.2019.04.033 [PubMed]
- 70. Wirdefeldt K, Weibull CE, Chen H, Kamel F, Lundholm C, Fang F, Ye W. Parkinson's disease and cancer: A register-based family study. Am J Epidemiol. 2014; 179:85–94. https://doi.org/10.1093/aje/kwt232 [PubMed]
- 71. Fois AF, Wotton CJ, Yeates D, Turner MR, Goldacre MJ. Cancer in patients with motor neuron disease, multiple sclerosis and Parkinson's disease: record linkage studies. J Neurol Neurosurg Psychiatry. 2010; 81:215–21. https://doi.org/10.1136/jnnp.2009.175463 [PubMed]
- 72. Lo RY, Tanner CM, Van Den Eeden SK, Albers KB, Leimpeter AD, Nelson LM. Comorbid cancer in Parkinson's disease. Mov Disord. 2010; 25:1809–17. https://doi.org/10.1002/mds.23246 [PubMed]
- 73. Freedman DM, Wu J, Chen H, Kuncl RW, Enewold LR, Engels EA, Freedman ND, Pfeiffer RM. Associations between cancer and Alzheimer's disease in a U.S. Medicare population. Cancer Med. 2016; 5:2965–76. https://doi.org/10.1002/cam4.850 [PubMed]
- 74. Tacik P, Curry S, Fujioka S, Strongosky A, Uitti RJ, van Gerpen JA, Diehl NN, Heckman MG, Wszolek ZK. Cancer in Parkinson's disease. Parkinsonism Relat Disord. 2016; 31:28–33. https://doi.org/10.1016/j.parkreldis.2016.06.014 [PubMed]
- 75. Shalaby SY, Louis ED. Statin Use and Its Association with Essential Tremor and Parkinson's Disease. Neuroepidemiology. 2016; 47:11–7. https://doi.org/10.1159/000446655 [PubMed]
- 76. Becker C, Brobert GP, Johansson S, Jick SS, Meier CR. Cancer risk in association with Parkinson disease: a population-based study. Parkinsonism Relat Disord. 2010; 16:186–90. https://doi.org/10.1016/j.parkreldis.2009.11.005 [PubMed]