



Introduction
The trends toward an increased aged population (the proportion of individuals aged 65 years and over) is a major public health problem, especially in China [1, 2]. Worldwide, the estimated number of elderly population was 962 million in 2017, and the growing rate was approximately 3% per year [3]. China has the largest elderly population in the world, with more than 225 million elderly people. The number of elderly people in China is projected to be 400 million by 2030 [4]. Ageing is a complex process characterized by progressive degradation of structural and functional integrity, during which the ability to maintain homeostasis is gradually lost, leading to the risk of impaired function and disease susceptibility [5–8]. Furthermore, ageing is a major risk factor for various chronic diseases [8]. However, there is great heterogeneity in health outcomes among elderly individuals of the same age group, suggesting that actual age is not an optimal indicator of the ageing progress [9].
Actual age correlates with the accumulation of biological changes, and individuals with the same actual age undergo these changes at different rates [10]. Biological age is used to measure damage accumulation with age at an individual level and can be quantified from the known biomarkers of ageing [11, 12]. To date, the ageing biomarkers include telomere length [13], DNA methylation [14–16], transcriptomic predictor [17, 18], plasma peptide [19], IgG N-glycosylation [20, 21], facial morphology [22], waist circumference density index [23], among others. Biological age determined by age-related DNA methylation has proven to be better than chronological age, as a predictor of 3-month outcomes after ischaemic stroke [24]. Biological age can issue a timely warning for health care and make people realize that his health is slipping away [12]. Therefore, the regular monitoring of the discrepancy between biological age and chronological age has potential positive impacts on the primary prevention and disease burden.
Biological ageing is associated with reduced reparative and regenerative potential of the body [25]. The ideal candidates to be studied for the purpose of predicting biological age must be representative of the level of homeostatic balance in the body. Plasma peptides, such as hormones, cytokines and growth factors, promote homeostasis in many biological processes [26]. Additionally, some plasma peptides have been found to be associated with age-related diseases, including Alzheimer's disease, hypertension, type 2 diabetes, and colorectal cancer [27–31]. Furthermore, our previous study shows that some peptides are highly correlated with chronological age in a Chinese population, such as fragment of apolipoprotein A-I, fibrinogen alpha, albumin and so on [19]. In particular, the levels of apolipoprotein A-I and fibrinogen alpha fragment gradually increased between 18 and 50 years of age, while albumin significantly degraded in middle-aged individuals. In the present study, we focused on building a biological age model with a set of specific plasma peptides from a Han Chinese population.
Results
Description of the subjects
This cross-sectional study included 1890 participants of Han Chinese descent. The summary of demographic variables was shown in Table 1. The median age was 34 years (P25 27 years, P75 45 years) in all subjects, 34 years (27 to 45 years) in male subjects, and 36 years (26 to 46 years) in female subjects (Table 1). All anthropometric variables, except for age and age group variables, were significantly different between male and female subjects (P < 0.001). Compared with female participants, the male subjects had greater height, weight, systolic blood pressure (SBP), diastolic blood pressure (DBP), and body mass index (BMI).
Table 1. Characteristics of the participants.
| Parameters | Total (n=1890) | Males (n=1136) | Females (n=754) | P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, year | 34 (27-45) | 34 (27-45) | 36 (26-46) | 0.512 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤ 39 | 1177 (62.28%) | 721 (63.47%) | 456 (60.48%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 40-59 | 593 (31.38%) | 323 (28.43%) | 270 (35.81%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 60 | 120 (6.35%) | 92 (8.10%) | 28 (3.71%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age group, % | 0.148 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤ 40 years old | 1225 (63.81%) | 751 (66.11%) | 474 (62.86%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| > 40 years old | 665 (35.19%) | 385 (33.89%) | 280 (37.14%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Height, cm | 169 (163-173) | 172 (169-176) | 162 (158-166) | < 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Weight, kg | 67 (58-76) | 73 (66-81) | 57 (52-63) | < 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, kg/m2 | 23.7 (21.2-25.9) | 24.6 (22.5-26.8) | 21.8 (19.9-24.1) | < 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP, mmHg | 120 (110-130) | 120 (112-130) | 114 (104-124) | < 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DBP, mmHg | 78 (70-82) | 80 (70-86) | 72 (66-80) | < 0.001* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *P < 0.05 indicating that the peptide was taken as a significant one. BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Model for predicted biological age
Among 84 detected peptides with masses in the range of 0.6-10.0 kDa, 13 identified peptides with amino acid sequences were used for subsequent analysis (Table 2). In particular, 11 peptides were selected for further analysis based on univariate linear regression (Table 3), except for fragment of complement C3 (m/z 1120.39) and complement C4-A (m/z 1052.53). As shown in Table 4, five plasma peptides, including fragments of apolipoprotein A-I (m/z 2883.99), fibrinogen alpha chain (m/z 3060.13), complement C3 (m/z 2190.59), complement C4-A (m/z 1898.21), and breast cancer type 2 susceptibility protein (m/z 1607.84), were identified by stepwise selection in a multivariate linear regression based on these 11 peptides and all demographic traits (BMI, SBP, DBP, age group). Finally, a biological age model was built based on the five identified plasma peptides and three demographic variables (Table 4). The estimated biological age can be calculated using the following equation (1).
Table 2. Characteristics of identified plasma peptide in the participants.
| Peak | Amino acid sequence | Peak identity | Total (n=1890) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 2044.75 | K.VFDEFKPLVEEPQNLIK.Q | Albumin | 105.3 (40.0-160.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 2065.31 | D.APRIKKIVQKKLAGDESAD.- | Pro-Platelet basic protein | 35.3 (14.2-75.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 2487.01 | S.NSRDDGNSVFPAKASATGAGPAAAEK.R | Hyperpolarization-activated cyclic nucleotide-gated potassium channel 1 | 26.1 (16.7-42.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 3428.10 | K.YWSQQIEESTTVVTTQSAEVGAAETTLTELR.R | Keratin 18 | 60.4 (24.3-113.5) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 2883.99 | L.LPVLESFKVSFLSALEEYTKKLNTQ.- | Apolipoprotein A-I | 36.4 (19.5-59.2) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 1076.14 | E.GDFLAEGGGVR.G | Fibrinogen alpha chain | 30.2 (20.6-41.8) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 3060.13 | K.SSSYSKQ(+.98)FTSSTSYNRGDSTFESKSYK.M | Fibrinogen alpha chain | 73.6 (33.3-135.6) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 1120.39 | T.HRIHWESAS.L | Complement C3 | 18.5 (13.1-25.7) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 2190.59 | G.SPMYSIITPNILRLESEET.M | Complement C3 | 45.7 (26.2-80.4) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 1052.53 | K.SHALQLNNR.Q | Complement C4-A | 20.6 (13.7-29.9) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 1898.21 | S.STGRNGFKSHALQLNNR.Q | Complement C4-A | 24.3 (14.8-56.8) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 1607.84 | P.KC(+57.02)KEMQNSLN(+.98)NDK.N | Breast cancer type 2 susceptibility protein | 19.0 (9.97-38.8) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| m/z 2211.86 | V.YRLPPLRKGEVLPLPEAN(+.98)F.P | Histidine-rich glycoprotein | 38.1 (20.0-80.8) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data were presented as median together with interquartile range. Peptide content in human plasma is measured in intensity. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 3. Univariate linear regression analysis for each identified peptide.
| Variables | Coefficient | SE | P | 95% CI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Albumin (m/z 2044.75) | -0.005 | 0.002 | 0.012* | (-0.008, -0.001) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pro-Platelet basic protein (m/z 2065.31) | -0.008 | 0.005 | 0.100* | (-0.018, 0.002) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperpolarization-activated cyclic nucleotide-gated potassium channel 1 (m/z 2487.01) | 0.040 | 0.014 | 0.004* | (0.013, 0.067) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Keratin 18 (m/z 3428.10) | 0.014 | 0.005 | 0.002* | (0.005, 0.023) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Apolipoprotein A-I (m/z 2883.99) | 0.040 | 0.009 | < 0.001* | (0.023, 0.058) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrinogen alpha chain (m/z 1076.14) | -0.064 | 0.017 | < 0.001* | (-0.097, -0.030) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrinogen alpha chain (m/z 3060.13) | 0.009 | 0.003 | 0.002* | (0.003, 0.015) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Complement C3 (m/z 1120.39) | -0.048 | 0.029 | 0.100 | (-0.105, 0.009) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Complement C3 (m/z 2190.59) | 0.011 | 0.005 | 0.034* | (0.001, 0.022) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Complement C4-A (m/z 1052.53) | 0.002 | 0.023 | 0.921 | (-0.042, 0.046) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Complement C4-A (m/z 1898.21) | -0.007 | 0.004 | 0.074* | (-0.014, 0.001) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Breast cancer type 2 susceptibility protein (m/z 1607.84) | 0.015 | 0.009 | 0.072* | (-0.001, 0.032) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Histidine-rich glycoprotein (m/z 2211.86) | 0.007 | 0.004 | 0.090* | (-0.001, 0.016) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *P < 0.10 indicating that the peptide was taken as a significant one. The P value of pro-platelet basic protein (m/z 2065.31) was 0.0996 which rounded to three decimal places (0.100). Complement C3 (m/z 1120.39) and Complement C4-A (m/z 1052.53) were not selected for further multivariate linear regression analysis. SE: Standard error; 95% CI: 95% Confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 4. Multiple linear regression analysis for biological age.
| Variables | Coefficient | SE | P | 95% CI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Constant | 13.3 | 1.73 | < 0.001* | (9.9, 16.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 0.122 | 0.054 | 0.025* | (0.016, 0.229) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP | 0.107 | 0.015 | < 0.001* | (0.079, 0.136) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age group | 21.0 | 0.387 | < 0.001* | (20.2, 21.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Apolipoprotein A-I (m/z 2883.99) | -0.014 | 0.006 | 0.035* | (-0.026, -0.001) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrinogen alpha chain (m/z 3060.13) | 0.004 | 0.002 | 0.050* | (3.69 × 10-6, 7.50 × 10-3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Complement C3 (m/z 2190.59) | 0.011 | 0.004 | 0.003* | (0.004, 0.019) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Complement C4-A (m/z 1898.21) | -0.005 | 0.003 | 0.053 | (-1.02 × 10-2, 5.50 × 10-5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Breast cancer type 2 susceptibility protein (m/z 1607.84) | 0.019 | 0.006 | 0.002* | (0.007, 0.031) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *P < 0.05 indicating that the peptide was taken as a significant one. The P value of fibrinogen alpha chain (m/z 3060.13) was 0.0498 which rounded to three decimal places (0.050). Adjusted R2 = 0.723. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI: Body mass index; SBP: Systolic blood pressure; SE: Standard error; 95% CI: 95% Confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Biological age = 13.3 + 0.122 × BMI + 0.107 × SBP + 21.0 × age group + (-0.014) × Apolipoprotein A-I fragment (m/z 2883.99) + 0.004 × Fibrinogen alpha chain fragment (m/z 3060.13) + 0.011 × Complement C3 fragment (m/z 2190.59) + (-0.005) × Complement C4-A fragment (m/z 1898.21) + 0.019 × Breast cancer type 2 susceptibility protein fragment (m/z 1607.84)(1)
All samples (from 1890 Chinese Han adults) were randomly divided into the training set (1500 samples) and validation set (390 samples). This model accounted for 72.3% of the variation in chronological age, with a correlation between the actual age and biological age of 0.851 (95% confidence interval (95% CI): 0.836-0.864) in the training set. Furthermore, in the validation set, the biological age was linearly correlated with the actual age (correlation coefficient (r) = 0.842, 95% CI: 0.810-0.869), and the normalized mean square error (NMSE) was 0.30. Visual analysis of the correlations between biological age and chronological age is presented in Figure 1. The predictive effect of the model is considered outstanding when the correlation curve is a straight line and its slope is equal to 1. The 95% CI of the fitted curve broadened with age, suggesting that the variation in biological age and heterogeneity among different individuals increased with actual age. Thus, plasma peptides can serve as potential biomarkers for predicting biological age, and their practical application warrants further research.
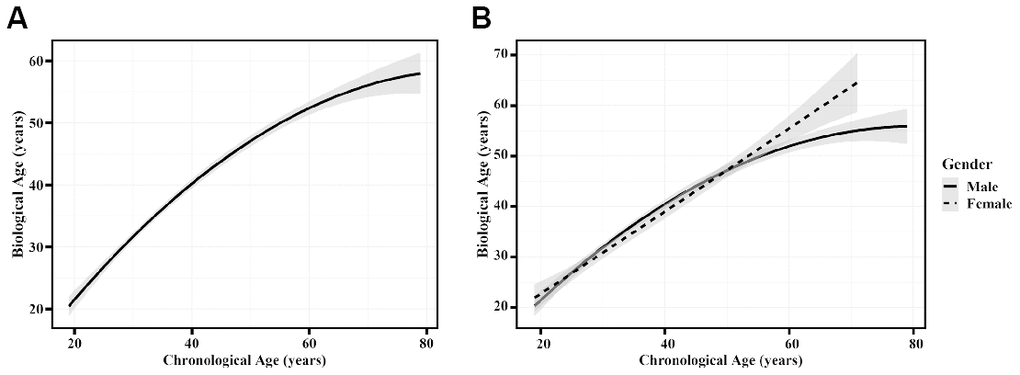
Figure 1. The correlation between chronological age and biological age. (A) The model performance based on the validation set. (B) The model performance presented by sex in the validation set. Dotted and solid curves were fitted to describe correlations between biological age and chronological age in females and males, respectively. The shade region was a pointwise 95% confidence interval.
Discussion
Biological age is a health indicator associated with chronological age, senescence and disease, and it can reflect dynamic and alterable health status better than chronological age [32]. In the present study, we built a biological age model correlated with actual age (r = 0.842, 95% CI: 0.810-0.869) in the validation set that explained 72.3% of the variation in chronological age, but its predictive ability still needs further verification. To the best of our knowledge, this study is the first attempt to build a biological age model based on plasma peptides in Han Chinese adults.
Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) is a key tool for peptide analysis of human body fluids, such as plasma, saliva and urine samples [26]. Based on this method, thirteen peptides were identified their amino acid sequences, and five of these peptides were used to construct a biological age model (fragment of apolipoprotein A-I (m/z 2883.99), fibrinogen alpha chain (m/z 3060.13), complement C3 (m/z 2190.59), complement C4-A (m/z 1898.21), and breast cancer type 2 susceptibility protein (m/z 1607.84)). Compared to our previous study, our study found four novel peptides associated with age [19]. The fragment of apolipoprotein A-I (m/z 2883.99) was found to be a biomarker of biological age in our previous study [19], which is consistent with our results. The level of plasma apolipoprotein A-I is associated with premature coronary artery disease [33] and clinical progression of Alzheimer's disease [34]. We previously found fibrinogen alpha chain (m/z 1076.14) fragment is related to ageing [19], whereas the other fragment of ageing-related fibrinogen alpha chain (m/z 3060.13) was used to build this biological age model in our study. Fibrinogen play an positive role in promoting blood haemostasis and leukocyte function regulation in inflammation [35]. However, elucidating the effect of the level of fibrinogen alpha chain fragment (m/z 3060.13) on ageing still requires further research. Complement C3 activates immune function through complement activation [36]. Furthermore, we also found that other peptides (fragment of complement C4-A (m/z 1898.21) and breast cancer type 2 susceptibility protein (m/z 1607.84)) can be used in predicting biological age, whereas their specific mechanisms in ageing remain to be elucidated.
According to the findings of previous studies, this candidate biological age model had a better age correlation in the validation set (r = 0.842, 95% CI: 0.810-0.869) than telomere length (r = 0.695 (95% CI: 0.575-0.0.815), without validation) [13], transcriptomic predictor (r ranged from 0.348 to 0.744 in different independent cohorts) [17] and IgG Fc N-glycosylation (r = 0.59 for the Chinese population, and r = 0.84 for the European population) [20, 21], but a weaker correlation with DNA methylation age (r = 0.96) in their corresponding validation cohorts covering the entire adult life span and different ethnic populations [15]. Compared to the abovementioned micro biological age, the two macro biological ages also showed strong correlations with the actual age (r ranged from 0.85 to 0.86 for the three-dimensional facial image-based age predictor and r = 0.992 for the waist circumference density index) [22, 23]. Therefore, composite biomarker predictors may have potential for biological age assessment. In addition, our results were consistent with the large heterogeneity in health state of elderly individuals for the variation in biological age increased with chronological age (95% CI widen with age) [9]. We defined a "age group" variable, a binary variable grouped by 40 years old, based on complex changes of different peptides in different age groups (five age groups 18-29, 30-39, 40-49, 50-59, ≥ 60 years) [19]. The "age group" variable defined 40 years old as the demarcation point artificially based on the balance between these groups. Moreover, women older than 40 years of age will experience the transitional stage characterized by a transition from the reproductive to the non-reproductive stage [37]. Epidemiological studies showed a high prevalence of obesity [38], diabetes mellitus [39], and stroke [40] in adults older than 40 years.
There are several limitations of our study that should be acknowledged. First, due to the limitations of experimental conditions, there may be bias in the peptide analysis because we did not control for pH, removal of oxygen, storage under argon and enzyme inhibitors of all plasma samples, though we controlled for storage time and temperature [41]. Second, although MS-based peptide analysis has been widely used, the detection and identification process is complicated and time-consuming, and the pre-treatment of plasma has a great influence on peptide analysis [42]. Therefore, the pre-treatment of plasma samples and peptide analysis still requires methodological advancement. Finally, people aged 60 years or older comprised a relatively low proportion of the population (6.35%), which may lead to selection and information bias (Table 1). This biological age model needs to be explored in larger and more representative samples, including those of a non-Asian ethnicity, as our study only included Chinese Han adults.
Our finding has certain implications for ageing. This study is the first attempt to develop a biological age model based on plasma peptides in Han Chinese adults. Biological age based on plasma peptides may have the potential to indicate homeostasis abnormalities and the rate of ageing. Our study provided evidence for further research in peptide-based biological age. This evidence may help us to understand the underlying mechanisms of ageing through five age-related peptides.
In conclusion, our study suggested that plasma peptide profiles can be used to build a biological age model. This candidate model involving peptides and clinical traits was able to account for 72.3% of the variation in actual age, and this biological age correlated with chronological age (r = 0.842, 95% CI: 0.810-0.869) in the validation set. However, the practical applications of this model in primary prevention warrant further investigation.
Materials and Methods
Subjects
This cross-sectional study recruited 1927 participants of Han Chinese ancestry during regular health check-ups at Xuanwu Hospital, Capital Medical University, Beijing, China. Individuals who were 18 years old or older were eligible. In addition, subjects with a history of somatic or psychiatric abnormalities in their medical records and those who had used medication two weeks prior to the study were excluded. Subjects who had a history of cerebral infarction, cerebral haemorrhage, other cerebrovascular diseases, congenital heart disease, acute myocardial infarction, liver disease, renal failure, malignant tumour, chronic obstructive pulmonary disease, or rheumatoid arthritis were also excluded. In this study, 37 participants who had missing data for one or more clinical traits were subsequently excluded. Finally, a total of 1890 participants were included in the subsequent analysis. Further details of the study design, recruitment procedure, and physical examination were previously described [19].
Ethics approval
Written informed consent was obtained from each participant, and all procedures were implemented in accordance with the regulations of the ethics committee of Capital Medical University, Beijing, China.
Collection of plasma samples
The plasma samples for peptide analysis were collected according to a standard protocol. Fresh fasting blood samples were collected from the cubital vein into blood collection tubes (containing ethylenediaminetetraacetic acid). The plasma was separated by centrifugation at 3,000 rpm for 15 min and then stored at −80 °C until peptide analysis. The number of freeze-thaw cycles of all samples is basically the same during this process. After the plasma samples of all the participants were collected, peptide analysis was completed at the shortest possible time.
Magnetic bead-based sample preparation for peptide analysis
As in previous studies [27, 28, 43], all plasma samples were fractionated using weak cation exchange magnetic beads to gather and enrich the proteins or peptides, according to the instructions provided by the supplier (ClinProt™, Bruker Daltonics, Billerica, USA) [44, 45]. The samples were purified and isolated through three steps: binding, washing, and elution. The specific details of this process were published in a previous study [19]. Then, the resulting eluates were stored in a –20 °C freezer until further MS analysis.
Peptides profiling and processing of spectral data
Peptide profiling was performed by MALDI-TOF-MS [28, 43]. First, the eluted samples were diluted in a matrix solution of α-cyano-4-hydroxycinnamic acid and ethanol and acetone, which was prepared daily. Then, 1 μl of the diluted samples was pipetted onto a MALDI-TOF-MS target (AnchorChip™, Bruker Daltonics, Billerica, USA) and dried at room temperature before analysis. Finally, MALDI-TOF-MS measurements were performed using the Autoflex TOF instrument (Bruker Daltonics, Billerica, USA). Profile spectra were acquired from an average of 400 laser shots per sample, with the defined mass range of peak intensities (measured as m/z) of 600–10,000 Da.
Quality control was carried on before the MS analysis, with 11 peptides as external standards where the average molecular weight deviation was no more than 100 μg/g. After testing every 8 samples, each standard preparation was re-calibrated. Additionally, 13 reference samples were run as external standards. The system performance is considered acceptable when the coefficient of variability is less than 30%. All reference peptides and samples were prepared in the same matrix solution as above. All of the solutions and buffers were prepared using MS-grade reagents.
The MALDI mass spectra of peptides were analysed using ClinProTools (ClinProt software version 2.0, Bruker Daltonics, Billerica, USA) to subtract the baseline, normalize the spectra (using total ion current), and determine the peak m/z values and intensities in the mass range of 600–10,000 Da. In brief, local noise estimates were applied to estimate the background, then the background was subtracted from each spectrum. Peptide peaks with a signal-to-noise ratio higher than 5.0 were detected and defined. The cut-off value of the signal-to-noise ratio was set at 5.0 because this value was a good compromise between over detection and sensitivity. A mass shift of no more than 0.1% was determined for the spectra alignment. The peak area was used for quantitative standardization. To determine the peak m/z values or intensities in the target mass range, a ± 2 Da mass accuracy for each spectrum was tolerated [46]. To evaluate the experimental reproducibility, triplicate measurements were performed to examine the standard deviation on the same MALDI-TOF-MS instrument. In our study, the standard deviation was less than 10%, so the reproducibility for the MALDI-TOF MS instrument was considered acceptable.
Identification of the amino acid sequences of the peptides
The amino acid sequences of the peptides were identified using the nanoliquid chromatography–electrospray ionization–tandem mass spectrometry (nano-LC/ESI–MS/MS) system, which is comprised of an Aquity UPLC system (Waters, Milford, MA, USA) and an LTQ Obitrap XL mass spectrometer (Thermo Fisher Scientific, Bremen, Germany) equipped with a nano-ESI source. In brief, the peptide solution was loaded onto a symmetry C18 trap column (nanoACQUITY) (180 μm × 20 mm × 5 μm) and then analysed by symmetry C18 analytical column (nanoACQUITY, Waters, Milford, MA, USA) (75 μm × 150 mm × 3.5 μm). The mobile phases A, mobile phases B, flow rate and gradient elution were operated according to the published paper [19]. The running mode of the MS instrument was operated in a data-dependent model. The range of the full scan was 400–2,000 m/z with a mass resolution of 100,000 at m/z 400. The FDR cut-off value was set to 0.01 during the whole identification process. The eight strongest monoisotopic ions were the precursors for collision-induced dissociation. The MS/MS spectra were restricted to two consecutive scans per precursor ion followed by a 60-sec of dynamic exclusion.
To identify the peptides, the chromatograms were analysed using BioWorksBrowserTM 3.3.1 SP1 software (Thermo Fisher Scientific, Bremen, Germany). The resulting mass lists were located on the Sequest™ (IPI Human v3.45) database (Thermo Scientific, Waltham, MA, USA). Due to the generation of the peak list, the parent ion and fragment mass relative accuracy were set at 50 μg/g and 1 Da, respectively. MS/MS product-ion mass spectra were presented in Figure 2.
Figure 2. The total ion current chromatograms of secondary ion mass spectrometry.
Measurements
The dataset consisted of 7 main demographic variables: age (years), gender, height (cm), weight (kg), BMI (kg/m2), SBP (mmHg), DBP (mmHg). Considering that participants at different ages might have large variation in physiological functions [37–40], the constructed model included a “age group” variable defined by a binary indicator, where people aged 40 years and below were represented as 1, and people aged above 40 years were represented as 2. In addition, 84 peptides were detected, with masses in the range of 0.6-10.0 kDa. Among these peptides, 13 peptides were successfully identified as known amino acid sequences. These demographic variables above and the 13 identified peptides were used for subsequent analysis.
Statistical analysis
Continuous variables were expressed as median and interquartile ranges. Frequencies and percentages were used to express the categorical variables. Continuous variables in the two gender groups were compared using the Mann-Whitney U test. The χ2 test was used to compare proportions for categorical variables. Multivariate linear regression was used for the biological age model. The samples were randomly divided into the training set (1500 samples) and validation set (390 samples). The training set and the independent validation set were used for modelling and model validation, respectively. First, a univariate linear regression model was implemented for preliminary selection. If the peptide had a P value lower than the entering threshold (P < 0.10), then the peptide could be used for further variable screening. Second, all candidate peptides were entered in a multivariate linear regression with stepwise selection adjusting for all demographic variables. The direction argument and entering threshold of stepwise regression were set to “both” and “0.10”, respectively. The criteria for variable selection were based on the Akaike information criterion. Finally, variables identified by stepwise selection were used to build the final biological age mode. The performance of this biological age model was evaluated by the coefficient of determination (R2) and NMSE of prediction errors in the independent validation set. Except for variable screening of peptides in regression analysis, a two-tailed P-value < 0.05 was considered statistically significant. All statistical analyses were performed using R version 3.3.3 (R Foundation for Statistical Computing, Vienna, Austria).
Acknowledgments
The authors appreciate Xingang Li and Isinta Elijah Maranga for their assistance in editing this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
This work was supported by grants from the National Natural Science Foundation of China (NSFC) (81673247, 81872682 and 81773527), the Joint Project of the NSFC and the Australian National Health and Medical Research Council (NHMRC) (NSFC 81561128020-NHMRC APP1112767).
References
- 1. Grover S. Aging population in Asia: are we preparing ourselves enough? Asian J Psychiatr. 2015; 13:1–2. https://doi.org/10.1016/j.ajp.2015.02.003 [PubMed]
- 2. Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, Wan X, Yu S, Jiang Y, Naghavi M, Vos T, Wang H, Lopez AD, Murray CJ. Rapid health transition in China, 1990-2010: findings from the global burden of disease study 2010. Lancet. 2013; 381:1987–2015. https://doi.org/10.1016/S0140-6736(13)61097-1 [PubMed]
- 3. United Nations DoEaSA, Population Division. . World Population Prospects: The 2017 Revision, Key Findings and Advance Tables. Working Paper No. ESA/P/WP/248. United Nations, New York, 2017. https://population.un.org/wpp/Publications/Files/WPP2017_KeyFindings.pdf.
- 4. Sun R, Cao H, Zhu X, Liu JP, Dong E. Current aging research in China. Protein Cell. 2015; 6:314–21. https://doi.org/10.1007/s13238-015-0145-5 [PubMed]
- 5. Childs BG, Durik M, Baker DJ, van Deursen JM. Cellular senescence in aging and age-related disease: from mechanisms to therapy. Nat Med. 2015; 21:1424–35. https://doi.org/10.1038/nm.4000 [PubMed]
- 6. Richardson AG, Schadt EE. The role of macromolecular damage in aging and age-related disease. J Gerontol A Biol Sci Med Sci. 2014 (Suppl 1); 69:S28–32. https://doi.org/10.1093/gerona/glu056 [PubMed]
- 7. Pawelec G, Goldeck D, Derhovanessian E. Inflammation, ageing and chronic disease. Curr Opin Immunol. 2014; 29:23–28. https://doi.org/10.1016/j.coi.2014.03.007 [PubMed]
- 8. North BJ, Sinclair DA. The intersection between aging and cardiovascular disease. Circ Res. 2012; 110:1097–108. https://doi.org/10.1161/CIRCRESAHA.111.246876 [PubMed]
- 9. Lowsky DJ, Olshansky SJ, Bhattacharya J, Goldman DP. Heterogeneity in healthy aging. J Gerontol A Biol Sci Med Sci. 2014; 69:640–49. https://doi.org/10.1093/gerona/glt162 [PubMed]
- 10. Levine ME. Modeling the rate of senescence: can estimated biological age predict mortality more accurately than chronological age? J Gerontol A Biol Sci Med Sci. 2013; 68:667–74. https://doi.org/10.1093/gerona/gls233 [PubMed]
- 11. Kirkwood TB. Alex comfort and the measure of aging. Exp Gerontol. 1998; 33:135–40. https://doi.org/10.1016/s0531-5565(97)00114-9 [PubMed]
- 12. Jylhävä J, Pedersen NL, Hägg S. Biological age predictors. EBioMedicine. 2017; 21:29–36. https://doi.org/10.1016/j.ebiom.2017.03.046 [PubMed]
- 13. Zhang WG, Zhu SY, Bai XJ, Zhao DL, Jian SM, Li J, Li ZX, Fu B, Cai GY, Sun XF, Chen XM. Select aging biomarkers based on telomere length and chronological age to build a biological age equation. Age (Dordr). 2014; 36:9639. https://doi.org/10.1007/s11357-014-9639-y [PubMed]
- 14. Hong SR, Jung SE, Lee EH, Shin KJ, Yang WI, Lee HY. DNA methylation-based age prediction from saliva: high age predictability by combination of 7 CpG markers. Forensic Sci Int Genet. 2017; 29:118–25. https://doi.org/10.1016/j.fsigen.2017.04.006 [PubMed]
- 15. Horvath S. DNA methylation age of human tissues and cell types. Genome Biol. 2013; 14:R115. https://doi.org/10.1186/gb-2013-14-10-r115 [PubMed]
- 16. Hannum G, Guinney J, Zhao L, Zhang L, Hughes G, Sadda S, Klotzle B, Bibikova M, Fan JB, Gao Y, Deconde R, Chen M, Rajapakse I, et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol Cell. 2013; 49:359–67. https://doi.org/10.1016/j.molcel.2012.10.016 [PubMed]
- 17. Peters MJ, Joehanes R, Pilling LC, Schurmann C, Conneely KN, Powell J, Reinmaa E, Sutphin GL, Zhernakova A, Schramm K, Wilson YA, Kobes S, Tukiainen T, et al, and NABEC/UKBEC Consortium. The transcriptional landscape of age in human peripheral blood. Nat Commun. 2015; 6:8570. https://doi.org/10.1038/ncomms9570 [PubMed]
- 18. Holly AC, Melzer D, Pilling LC, Henley W, Hernandez DG, Singleton AB, Bandinelli S, Guralnik JM, Ferrucci L, Harries LW. Towards a gene expression biomarker set for human biological age. Aging Cell. 2013; 12:324–26. https://doi.org/10.1111/acel.12044 [PubMed]
- 19. Lu J, Huang Y, Wang Y, Li Y, Zhang Y, Wu J, Zhao F, Meng S, Yu X, Ma Q, Song M, Chang N, Bittles AH, Wang W. Profiling plasma peptides for the identification of potential ageing biomarkers in chinese han adults. PLoS One. 2012; 7:e39726. https://doi.org/10.1371/journal.pone.0039726 [PubMed]
- 20. Yu X, Wang Y, Kristic J, Dong J, Chu X, Ge S, Wang H, Fang H, Gao Q, Liu D, Zhao Z, Peng H, Pucic Bakovic M, et al. Profiling IgG N-glycans as potential biomarker of chronological and biological ages: a community-based study in a han chinese population. Medicine (Baltimore). 2016; 95:e4112. https://doi.org/10.1097/MD.0000000000004112 [PubMed]
- 21. Krištić J, Vučković F, Menni C, Klarić L, Keser T, Beceheli I, Pučić-Baković M, Novokmet M, Mangino M, Thaqi K, Rudan P, Novokmet N, Sarac J, et al. Glycans are a novel biomarker of chronological and biological ages. J Gerontol A Biol Sci Med Sci. 2014; 69:779–89. https://doi.org/10.1093/gerona/glt190 [PubMed]
- 22. Chen W, Qian W, Wu G, Chen W, Xian B, Chen X, Cao Y, Green CD, Zhao F, Tang K, Han JD. Three-dimensional human facial morphologies as robust aging markers. Cell Res. 2015; 25:574–87. https://doi.org/10.1038/cr.2015.36 [PubMed]
- 23. Zhao X, Zhu S, Jia X, Yu L, Liu H. Constructing a waist circumference density index to predict biological age and evaluating the clinical significance of waist circumference density age. Exp Gerontol. 2013; 48:422–26. https://doi.org/10.1016/j.exger.2013.02.007 [PubMed]
- 24. Soriano-Tárraga C, Mola-Caminal M, Giralt-Steinhauer E, Ois A, Rodríguez-Campello A, Cuadrado-Godia E, Gómez-González A, Vivanco-Hidalgo RM, Fernández-Cadenas I, Cullell N, Roquer J, Jiménez-Conde J. Biological age is better than chronological as predictor of 3-month outcome in ischemic stroke. Neurology. 2017; 89:830–36. https://doi.org/10.1212/WNL.0000000000004261 [PubMed]
- 25. Khan SS, Singer BD, Vaughan DE. Molecular and physiological manifestations and measurement of aging in humans. Aging Cell. 2017; 16:624–33. https://doi.org/10.1111/acel.12601 [PubMed]
- 26. Mahboob S, Mohamedali A, Ahn SB, Schulz-Knappe P, Nice E, Baker MS. Is isolation of comprehensive human plasma peptidomes an achievable quest? J Proteomics. 2015; 127:300–09. https://doi.org/10.1016/j.jprot.2015.05.010 [PubMed]
- 27. Wang H, Luo C, Zhu S, Fang H, Gao Q, Ge S, Qu H, Ma Q, Ren H, Wang Y, Wang W. Serum peptidome profiling for the diagnosis of colorectal cancer: discovery and validation in two independent cohorts. Oncotarget. 2017; 8:59376–86. https://doi.org/10.18632/oncotarget.19587 [PubMed]
- 28. Meng Q, Ge S, Yan W, Li R, Dou J, Wang H, Wang B, Ma Q, Zhou Y, Song M, Yu X, Wang H, Yang X, et al. Screening for potential serum-based proteomic biomarkers for human type 2 diabetes mellitus using MALDI-TOF MS. Proteomics Clin Appl. 2017; 11:10.1002/prca.201600079. https://doi.org/10.1002/prca.201600079 [PubMed]
- 29. Li M, Wang J, Yang L, Gao P, Tian QB, Liu DW. eRF3b, a biomarker for hepatocellular carcinoma, influences cell cycle and phosphoralation status of 4E-BP1. PLoS One. 2014; 9:e86371. https://doi.org/10.1371/journal.pone.0086371 [PubMed]
- 30. Kostoeva AU, Mazur NA, Masenko VP, Sbrodova LV, Babaev FZ, Volkov VE, Pshenitsin AI, Khezheva FM, Shestakova NV. [N-terminal pro-brain natriuretic peptide and cardiac involvement in patients with hypertensive disease]. Kardiologiia. 2009; 49:33–38. [PubMed]
- 31. Koide S, Onishi H, Hashimoto H, Kai T, Yamagami S. Plasma neuropeptide Y is reduced in patients with alzheimer's disease. Neurosci Lett. 1995; 198:149–51. https://doi.org/10.1016/0304-3940(95)11973-z [PubMed]
- 32. Johnson TE. Recent results: biomarkers of aging. Exp Gerontol. 2006; 41:1243–46. https://doi.org/10.1016/j.exger.2006.09.006 [PubMed]
- 33. Genest JJ
Jr , Bard JM, Fruchart JC, Ordovas JM, Wilson PF, Schaefer EJ. Plasma apolipoprotein a-I, a-II, B, E and C-III containing particles in men with premature coronary artery disease. Atherosclerosis. 1991; 90:149–57. https://doi.org/10.1016/0021-9150(91)90109-g [PubMed] - 34. Slot RE, Van Harten AC, Kester MI, Jongbloed W, Bouwman FH, Teunissen CE, Scheltens P, Veerhuis R, van der Flier WM. Apolipoprotein A1 in cerebrospinal fluid and plasma and progression to alzheimer's disease in non-demented elderly. J Alzheimers Dis. 2017; 56:687–97. https://doi.org/10.3233/JAD-151068 [PubMed]
- 35. Vitorino de Almeida V, Silva-Herdade A, Calado A, Rosário HS, Saldanha C. Fibrinogen modulates leukocyte recruitment in vivo during the acute inflammatory response. Clin Hemorheol Microcirc. 2015; 59:97–106. https://doi.org/10.3233/CH-121660 [PubMed]
- 36. Ricklin D, Reis ES, Mastellos DC, Gros P, Lambris JD. Complement component C3 - the “swiss army knife” of innate immunity and host defense. Immunol Rev. 2016; 274:33–58. https://doi.org/10.1111/imr.12500 [PubMed]
- 37. Legorreta D, Montaño JA, Hernández I, Salinas C, Hernández-Bueno JA, and AMEC Research Committee. Age at menopause, motives for consultation and symptoms reported by 40-59-year-old mexican women. Climacteric. 2013; 16:417–25. https://doi.org/10.3109/13697137.2012.696288 [PubMed]
- 38. Oliveira GF, Oliveira TR, Ikejiri AT, Galvao TF, Silva MT, Pereira MG. Prevalence of obesity and overweight in an indigenous population in central Brazil: a population-based cross-sectional study. Obes Facts. 2015; 8:302–10. https://doi.org/10.1159/000441240 [PubMed]
- 39. Najafipour H, Sanjari M, Shokoohi M, Haghdoost AA, Afshari M, Shadkam M, Etemad K, Mirzazade A. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes and its predictors in general population aged 15 to 75 years: a community-based study (KERCADRS) in southeastern Iran. J Diabetes. 2015; 7:613–21. https://doi.org/10.1111/1753-0407.12195 [PubMed]
- 40. Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, Wang L, Jiang Y, Li Y, Wang Y, Chen Z, Wu S, Zhang Y, et al, and NESS-China Investigators. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017; 135:759–71. https://doi.org/10.1161/CIRCULATIONAHA.116.025250 [PubMed]
- 41. Tammen H, Schulte I, Hess R, Menzel C, Kellmann M, Schulz-Knappe P. Prerequisites for peptidomic analysis of blood samples: I. Evaluation of blood specimen qualities and determination of technical performance characteristics. Comb Chem High Throughput Screen. 2005; 8:725–33. https://doi.org/10.2174/138620705774962508 [PubMed]
- 42. Schrader M. Origins, technological development, and applications of peptidomics. Methods Mol Biol. 2018; 1719:3–39. https://doi.org/10.1007/978-1-4939-7537-2_1 [PubMed]
- 43. Cao F, Li X, Yang Y, Fang H, Qu H, Chang N, Ma Q, Cao W, Zhou J, Wang W. Toward candidate proteomic biomarkers in clinical monitoring of acute promyelocytic leukemia treatment with arsenic trioxide. OMICS. 2019; 23:119–30. https://doi.org/10.1089/omi.2018.0178 [PubMed]
- 44. Ketterlinus R, Hsieh SY, Teng SH, Lee H, Pusch W. Fishing for biomarkers: analyzing mass spectrometry data with the new ClinProTools software. Biotechniques. 2005; Suppl:37–40. https://doi.org/10.2144/05386su07 [PubMed]
- 45. Huang Z, Shi Y, Cai B, Wang L, Wu Y, Ying B, Qin L, Hu C, Li Y. MALDI-TOF MS combined with magnetic beads for detecting serum protein biomarkers and establishment of boosting decision tree model for diagnosis of systemic lupus erythematosus. Rheumatology (Oxford). 2009; 48:626–31. https://doi.org/10.1093/rheumatology/kep058 [PubMed]
- 46. Chang JT, Chen LC, Wei SY, Chen YJ, Wang HM, Liao CT, Chen IH, Cheng AJ. Increase diagnostic efficacy by combined use of fingerprint markers in mass spectrometry—plasma peptidomes from nasopharyngeal cancer patients for example. Clin Biochem. 2006; 39:1144–51. https://doi.org/10.1016/j.clinbiochem.2006.08.010 [PubMed]