



Introduction
It is estimated that familial susceptibility to breast cancer accounts for about 25% of all breast cancer cases [1]. The testing for germline mutations in high-penetrance breast cancer predisposition genes has become standard practice for breast cancer patients [2]. In clinical practice, BRCA1/2 are the most widely tested genes, particularly for breast cancer patients diagnosed at young age, with triple negative breast cancer (TNBC), or have a significant family history of breast, ovarian, or other related cancers [3]. Currently, existing recommendations for germline mutation testing of other high-penetrance genes including CDH1, TP53 and PTEN are based on specific clinical features [4]. Meanwhile, numerous studies have associated mutations in moderate-penetrance genes, including PALB2, ATM, CHEK2, BRIP1, with increased breast cancer risk of two to four-fold compared to the 10% risk of the general population [5]. Germline PALB2 mutations have been reported to play significant roles in hereditary breast cancer, with a five-fold or greater breast cancer risk for mutation carriers [6–8]. In addition, germline mutations in DNA damage repair genes such as ATM and CHEK2 are also associated with an increased risk of breast cancer [9, 10]. Despite mounting evidence suggesting the association of mutations in moderate-penetrance genes with increased breast cancer risk, the current guidelines still do not require the testing of these genes. Thus far, no consensus exists on the number and the specific genes needed to be sequenced and analyzed for the assessment of genetic cancer predisposition [11].
Although harboring germline mutations in either high- or moderate-penetrance genes will increase the predisposition to develop breast cancer, mutations in any one of these genes are rare and testing one gene at a time is both expensive and inefficient [12]. Recent advances in next-generation sequencing (NGS) have made multigene panels more affordable and allowed it to be increasingly used in cancer risk assessment in clinical practice [13, 14]. However, as compared to America and Europe, the use of multigene panel in cancer risk assessment of breast cancer patients is still relatively unpopular in Asia [15]. Expanded multigene panel testing can reveal incidental findings of germline variants in addition to the detection of somatic mutations in highly actionable genes [16]. The detection of likely pathogenic or pathogenic (LP/P) germline variants in low and moderate-risk genes as well as variants of uncertain significance (VUS) also challenges the established genetic counseling repertoire [17, 18]. Moreover, sequencing with multigene panels can identify significant gaps to further understand the relationship between genetics and tumor biology [19].
Numerous studies on germline mutation testing were focused on patients with family history of cancer [20, 21]. Current guidelines require only the patients with known family history to undergo genetic testing; however, not all patients with germline mutations have a known family history of tumors, which results in missing about 50% to 80% of individuals at risk [22, 23]. With growing evidence associating germline mutations with cancer predisposition as well as the availability of targeted therapies, the current view is that all patients newly diagnosed with cancer should be tested for germline mutations, which has the potential to reduce disease burden through secondary prevention and explore targeted therapies [24].
In order to promote the use of multigene panel testing of breast cancer patients, we need to understand the prevalence of germline mutations particularly in cancer predisposition genes beyond BRCA1/2 to identify the genes commonly mutated in our population. Moreover, the somatic mutation profiles of patients who harbor germline BRCA and non-BRCA mutations remain unexplored. In this study, we interrogated the germline and somatic mutational profile of 524 Chinese breast cancer patients with various stages unselected for predisposing factors, such as age at onset or family history, using a panel consisting of 520 cancer-related genes, including 62 cancer susceptibility genes (Supplementary Table 1). Our study aims to examine the prevalence of germline mutations in known breast cancer predisposition genes and other cancer-associated genes and to evaluate the clinical value of multigene panel testing of germline mutations in this population. We also assessed the relationship between clinicopathologic characteristics and germline mutation status and identified the somatic mutations among germline mutation carriers.
Results
Study population
A total of 524 breast cancer patients consented to NGS testing and were offered disclosure of germline results under a separate protocol. Clinical and pathologic features for study patients are provided in Table 1. The mean age at diagnosis was 49.2 years (range, 22 to 86 years). Except for 1 male, all the other 523 patients were females. Most of the patients were diagnosed at stage I (124 cases), II (231 cases) and III (102 cases), while the remaining 67 patients had stage IV. Majority of the patients (82.4%, 432/524) were diagnosed with invasive ductal cancer. Overall, 55 (32.0%) patients reported having a family history of breast or ovarian cancer and 55 (32.0%) patients reported having family history of other cancer. The remaining patients reported no family history of cancer.
Table 1. Clinicopathologic features of the study patients.
| Characteristics | No. | % |
| Age | ||
| ≤40 years | 96 | 18.32% |
| > 40 years | 428 | 81.68% |
| Menopausal status | ||
| Pre | 280 | 53.44% |
| Post | 231 | 44.08% |
| Unknown | 12 | 2.29% |
| Male | 1 | 0.19% |
| Family history of breast or ovarian cancer | ||
| Yes | 93 | 17.75% |
| No | 330 | 62.98% |
| Unknown | 101 | 19.27% |
| Tumor size | ||
| ≤2 cm | 199 | 37.98% |
| > 2 cm | 303 | 57.82% |
| Unknown | 22 | 4.20% |
| Lymph nodes status | ||
| Negative | 256 | 48.85% |
| Positive | 247 | 47.14% |
| Unknown | 21 | 4.01% |
| Grade | ||
| I | 23 | 4.39% |
| II | 234 | 44.66% |
| III | 234 | 44.66% |
| Unknown | 33 | 6.30% |
| Histology | ||
| DCIS | 14 | 2.67% |
| Infiltrating Ductal Carcinoma | 457 | 87.21% |
| Infiltrating Lobular | 10 | 1.91% |
| Carcinoma | ||
| Other, specify | 23 | 4.39% |
| Unknown | 20 | 3.82% |
| ER status | ||
| Negative | 139 | 26.53% |
| Positive | 363 | 69.27% |
| Unknown | 22 | 4.20% |
Frequency and characteristics of deleterious germline mutations
Paired white blood cell and tumor samples from 524 breast cancer patients were sequenced using a panel consisting of 520 cancer-related genes including 62 cancer susceptibility genes to interrogate the germline and somatic mutations, respectively.
Analysis revealed the detection of 76 likely pathogenic or pathogenic (LP/P) mutations in 15 cancer susceptibility genes from 58 patients (11.1%, 58/524) (Figure 1). Interestingly, 2 (0.38%) patients had more than one concurrent LP/P germline variants, with TP53 (c.919+1G>T) and PMS2 (p.R287fs) mutations detected in a patient with luminal B tumor, and BRCA2 (p.Q1129*) and FANCI (c.158-2A>G) mutations detected in a patient with luminal A tumor.
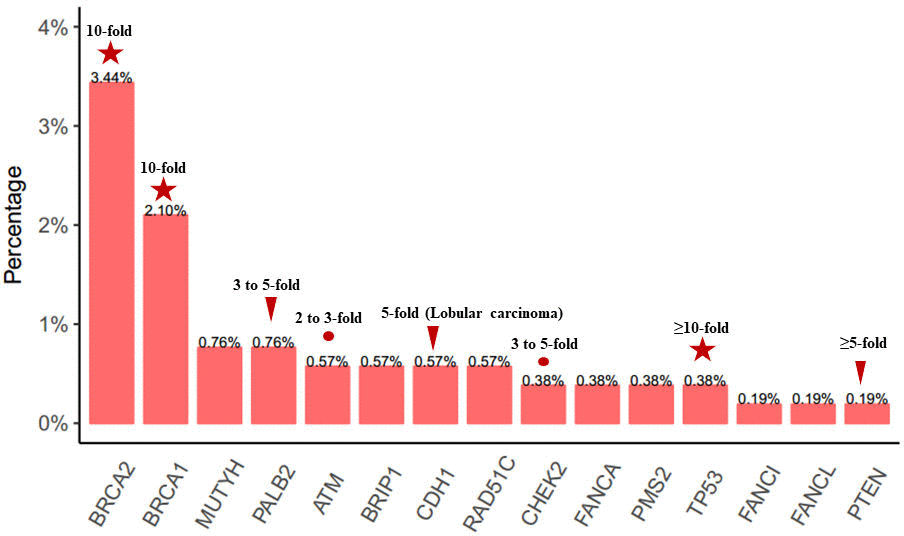
Figure 1. Frequency and distribution of LP/P germline variants. LP/P mutations identified in 62 cancer susceptibility genes in 524 unselected breast cancer patients. The multiples of genes associated with breast cancer risk are listed on the histogram.
Twenty-nine (5.53%, 29/524) patients carried germline BRCA1/2 mutation; including 11 (2.10%, 11/524) patients with BRCA1 and 18 (3.44%, 18/524) patients with BRCA2 mutations. As shown in Figure 2A–2B, BRCA1 T1691K (n = 2) and I1824fs (n = 2) and BRCA2 A938fs (n = 3) were the most frequent LP/P germline BRCA1/2 mutations in our cohort. In addition, 30 (5.72%) patients carried a total of 38 LP/P mutations in other cancer susceptibility genes beyond BRCA1/2. Mutations in genes beyond BRCA1/2 detected in the cohort included MUTYH (n = 4), PALB2 (n = 4), ATM (n = 3), BRIP1 (n = 3), CDH1 (n = 3), RAD51C (n = 3), CHEK2 (n = 2), FANCA (n = 2), PMS2 (n = 2), TP53 (n = 2), FANCI (n = 1), FANCL (n = 1) and PTEN (n = 1). Interestingly, among the 15 genes with germline mutations, 7 genes belong to Fanconi anaemia family of genes, including BRCA2, PALB2, BRIP1, RAD51C, FANCA, FANCI and FANCL, with 53.4% (31/58) of the patients carrying germline mutations in any of these genes. No LP/P germline mutations were found in the remaining 47 cancer susceptibility genes included in the panel. All the LP/P germline mutations detected in our cohort were listed in Table 2.
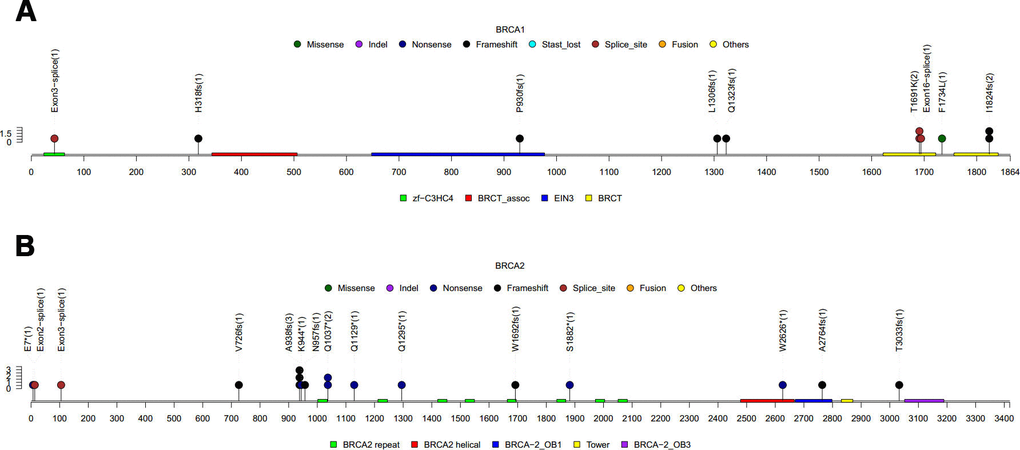
Figure 2. LP/P germline BRCA1/2 mutations detected in this cohort. (A) 11 LP/P mutations found in BRCA1. (B) 18 LP/P mutations found in BRCA2. Colored boxes depict the different functional domains along the gene. Small colored circles denote the type of mutation while the location of the circle specifies the mutation site. A patient is represented by a circle. The length of the lollipop represents the number of people of a specific variant.
Table 2. The list of likely pathogenic and pathogenic mutations detected in the cohort.
| Sample ID | Gene | Mutation type | Description | AF | Degrees | Public database or published paper |
| RS1829111TIS | ATM | frameshift variant | p.L2081fs | 78.90% | Likely pathogenic | N |
| RSI 829631HS | ATM | stop gained | p.Y155* | 43.90% | Likely pathogenic | N |
| RS1806623TIS | ATM | stop gained | p.E277* | 46.82% | Pathogenic | Y (clinvar) |
| RS1810742TIS | BRCA1 | splice region variant | p.T1691K | 57.66% | Likely pathogenic | Y (clinvar) |
| RSI 827051FFP | BRCA1 | splice region variant | p.T1691K | 72.22% | Likely pathogenic | Y (clinvar) |
| RS1828137FFP | BRCA1 | frameshift variant | p.H318fs | 60.59% | Likely pathogenic | Y (PMID: 28724667) |
| RS1834453TIS | BRCA1 | frameshift variant | p.I1824fs | 32.62% | Pathogenic | Y (PMID: 28724667) |
| RS1803594FFP | BRCA1 | splice region variant | c.5074+3A>G | 58.09% | Pathogenic | Y (clinvar) |
| RS1726576TIS | BRCAl | missense variant | P-F1734L | 80.27% | Likely pathogenic | Y (clinvar) |
| RS1725206FFP | BRCA1 | frameshift variant | p.I1824fs | 40.06% | Pathogenic | Y (PMID: 28724667) |
| RS1827494TIS | BRCAl | frameshift variant | p.P930fs | 61.94% | Likely pathogenic | Y (PMID: 28724667) |
| RS1829599FFP | BRCAl | frameshift variant | p.Q1323fs | 64.93% | Pathogenic | N |
| RSI 811823TIS | BRCAl | frameshift variant | p.L1306fs | 84.90% | Pathogenic | Y (PMID: 28724667) |
| RSI 804518FFP | BRCAl | splice donor variant | c.134+1G>T | 48.46% | Pathogenic | Y (clinvar) |
| RS1815241TIS | BRCA2 | frameshift variant | p.A938fs | 52.73% | Pathogenic | Y (clinvar) |
| RS1844984FFP | BRCA2 | splice acceptor variant | c.-39-l_-39del | 36.90% | Pathogenic | Y (clinvar) |
| RS1829456TIS | BRCA2 | stop gained | p.Q1295* | 55.38% | Pathogenic | Y (clinvar) |
| RS1803222TIS | BRCA2 | frameshift variant | p.A2764fs | 71.71% | Pathogenic | N |
| RS1821585FFP | BRCA2 | frameshift variant | p.V726fs | 51.09% | Likely pathogenic | N |
| RS1722724TIS | BRCA2 | stop gained | p.W2626* | 67.38% | Pathogenic | Y (clinvar) |
| RS1840694PLA | BRCA2 | stop gained | p.Q1037* | 49.37% | Pathogenic | Y (clinvar) |
| RSI 823761TIS | BRCA2 | stop gained | p.S1882* | 82.53% | Pathogenic | Y (clinvar) |
| RS1833574PLA | BRCA2 | stop gained | P-Q1037* | 48.98% | Pathogenic | Y (clinvar) |
| RS1841181FFP | BRCA2 | splice donor variant | c.316+lG>A | 59.00% | Pathogenic | Y (clinvar) |
| RS1723884TIS | BRCA2 | stop gained | p.K944* | 57.95% | Pathogenic | Y (clinvar) |
| RS1838903TIS | BRCA2 | frameshift variant | p.T3033fs | 57.11% | Pathogenic | Y (clinvar) |
| RS1826534FFP | BRCA2 | frameshift variant | p.N957fs | 57.89% | Pathogenic | N |
| RS1812099FFP | BRCA2 | stop gained | p.Ql 129* | 87.60% | Pathogenic | Y (clinvar) |
| RSI 800551FFP | BRCA2 | frameshift variant | p.A938fs | 54.00% | Pathogenic | Y (clinvar) |
| RS1813609FFP | BRCA2 | frameshift variant | p.W1692fs | 62.10% | Likely pathogenic | Y (PMID: 26689913, PMID: 25415331) |
| RS1801361TIS | BRCA2 | frameshift variant | p.A938fs | 56.82% | Pathogenic | Y (clinvar) |
| RS1813932FFP | BRCA2 | stop gained | p.E7* | 64.48% | Pathogenic | N |
| RS1840466TIS | BRIP1 | splice donor variant | c.627+lG>A | 64.39% | Pathogenic | Y (clinvar) |
| RS1809229FFP | BRIP1 | start lost | p.Ml? | 40.17% | Pathogenic | Y (clinvar) |
| RS1840704PLA | BRIP1 | stop gained | P-R798* | 48.41% | Pathogenic | Y (clinvar) |
| RS1828521TIS | CDH1 | missense variant | p.T340A | 45.90% | Likely pathogenic | Y (clinvar) |
| RS1829332TIS | CDHl | missense variant | P-T340A | 35.80% | Likely pathogenic | Y (clinvar) |
| RS1830223FFP | CDH1 | missense variant | p.T340A | 43.68% | Likely pathogenic | Y (clinvar) |
| RS1726142FFP | CHEK2 | stop gained | p.R95* | 73.50% | Pathogenic | Y (clinvar) |
| RSI 829637TIS | CHEK2 | missense variant | p.H371Y | 78.51% | Likely pathogenic | Y (clinvar) |
In addition to the LP/P variants, a total of 1,968 variants of uncertain clinical significance (VUS) in 62 cancer susceptibility genes were also detected in the cohort. At least one VUS was identified in 490 (93.5%) patients, with as many as three variants found per patient. Among them, 53 (10.8%) patients with a VUS also had an LP/P mutation. All the VUSs identified in our cohort are listed in Supplementary Table 2.
Germline mutations according to breast cancer molecular subtype
We also analyzed the distribution of LP/P germline mutations according to the molecular subtypes of the patients. The distribution and mutation detection rates of the germline mutations detected in our cohort according to their molecular breast cancer subtypes were summarized in Supplementary Tables 3 and 4, respectively.
According to the distribution, germline mutations in the 15 cancer susceptibility genes were found among patients with HR+/HER2- breast tumors (Supplementary Table 3). The overall LP/P germline mutation detection rates were 14.8% (9/61) for patients with triple-negative tumors, 8.5% (5/59) for patients with HER2-enriched tumors, 12.4% (33/267) for patients with HR+/HER2- tumors, 8.5% (7/82) for patients with HR+/HER2+ tumors and 7.3% (4/55) for patients with unknown molecular subtype (Supplementary Table 4). No statistical difference was found for the germline mutation rate according to the molecular subtypes (P=0.4).
Clinicopathological features of germline mutations carriers
Next, we further analyzed the clinicopathological characteristics of the LP/P germline mutation carriers to understand predisposing factors associated with the germline mutations. Breast cancer was diagnosed at a significantly younger age in germline mutation carriers as compared to non-carriers (median age: 45 vs 50 years, P=0.011, Table 3). Consistent with a younger age of onset, premenopausal women were more likely to carry LP/P germline mutations (P=0.013). Moreover, germline mutation carriers were more likely to have a family history of breast and/or ovarian cancer (P=0.001, Table 3). However, no further significant correlations were found between germline mutation status and other clinicopathologic factors, including tumor size (P=0.561), lymph node status (P=0.731), grade (P=0.420), histology (P=0.973), ER status (P=0.733), PR status (P=0.673), HER2 status (P=0.514) and a triple-negative phenotype (P=0.416). In addition, we found no significant correlation in the clinicopathological characteristics of patients carrying germline mutations in BRCA versus non-BRCA (data not shown).
Table 3. Clinicopathological characteristics between germline mutation carriers and non-carriers.
| Characteristics | Non-carriers | Germline mutation carriers | P-value | ||
| Age | 0.011* | ||||
| Median (range) | 50 (25-86) | 45 (22-72) | |||
| <40 years | 78 | 16.74% | 18 | 31.03% | |
| > 40 years | 388 | 83.26% | 40 | 68.97% | |
| Menopausal status | 0.013a* | ||||
| Pre | 238 | 51.07% | 42 | 72.41% | |
| Post | 216 | 46.35% | 15 | 25.86% | |
| Unknown | 11 | 2.36% | 1 | 1.72% | |
| Male | 1 | 0.21% | 0 | 0.00% | |
| Family history of breast or ovarian cancer | <0.001* | ||||
| Yes | 65 | 13.95% | 28 | 48.28% | |
| No | 311 | 66.74% | 19 | 32.76% | |
| Unknown | 90 | 19.31% | 11 | 18.97% | |
| Tumor size | 0.561a | ||||
| ≤2 cm | 179 | 38.41% | 20 | 34.48% | |
| > 2 cm | 266 | 57.08% | 37 | 63.79% | |
| Unknown | 21 | 4.51% | 1 | 1.72% | |
| Lymph nodes status | 0.731a | ||||
| Negative | 226 | 48.50% | 30 | 51.72% | |
| Positive | 220 | 47.21% | 27 | 46.55% | |
| Unknown | 20 | 4.29% | 1 | 1.72% | |
| Grade | 0.420a | ||||
| I | 21 | 4.51% | 2 | 3.45% | |
| II | 212 | 45.49% | 22 | 37.93% | |
| III | 202 | 43.35% | 32 | 55.17% | |
| Unknown | 31 | 6.65% | 2 | 3.45% | |
| Histology | 0.973a | ||||
| DCIS | 13 | 2.79% | 1 | 1.72% | |
| Infiltrating Ductal Carcinoma | 404 | 86.70% | 53 | 91.38% | |
| Infiltrating Lobular Carcinoma | 9 | 1.93% | 1 | 1.72% | |
| Other, specify | 21 | 4.51% | 2 | 3.45% | |
| Unknown | 19 | 4.08% | 1 | 1.72% | |
| ER status | 0.733a | ||||
| Negative | 124 | 26.61% | 15 | 25.86% | |
| Positive | 321 | 68.88% | 42 | 72.41% | |
| Unknown | 21 | 4.51% | 1 | 1.72% | |
Characteristics of somatic mutations in breast cancer patients with germline mutations
To understand the interplay between germline and somatic mutations in breast cancer patients, sequencing data derived from the paired tumor samples of the 524 breast cancer patients were analyzed. Genomic alterations with detection rate of more than 4% were shown in Figure 3. Interestingly, somatic TP53 mutations were detected in all (100%, 11/11) and a majority (67%, 2/3) of the patients with germline BRCA1 and CDH1 mutations, respectively. On the other hand, no somatic TP53 mutations were detected in all the patients with germline ATM (n=3) and TP53 (n=2). In addition, somatic mutations in PIK3CA were more frequent among patients with germline CDH1 (3/3). Furthermore, a patient with pathogenic germline PALB2 mutation (p.Q921fs) also had somatic PALB2 mutation (p.D525fs).
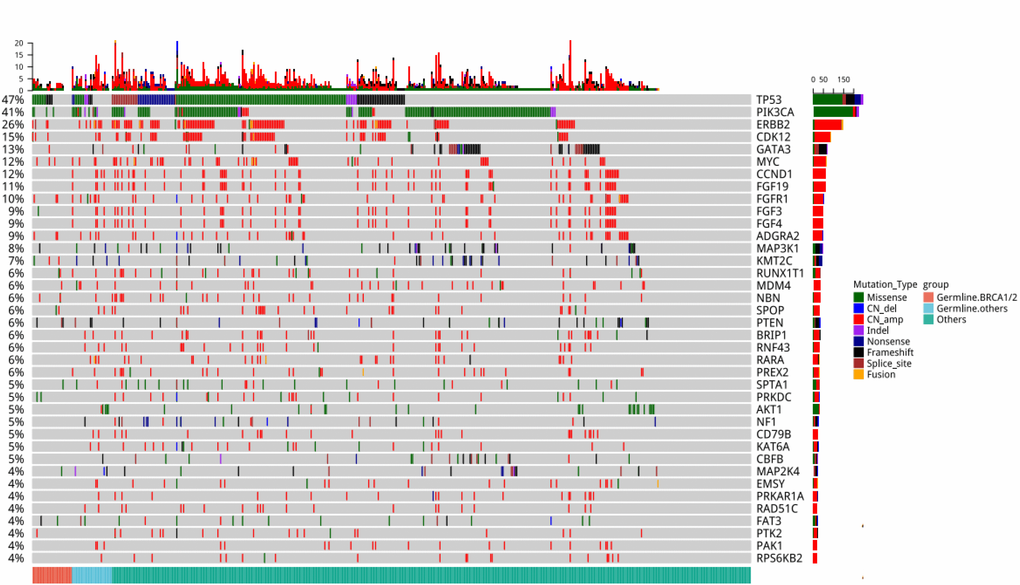
Figure 3. Comprehensive somatic mutation spectrum of the 524 patients. Each column represents a patient and each row represents a gene. The number on the left represents the percentage of patients with mutations in a specific gene. The top plot represents the overall number of mutations detected in a patient. Different colors denote different types of mutation. The annotation at the bottom, with each color representing each group, depicts the germline mutations carried by the patients.
Next, we divided the patients into three groups according to germline mutations: Germline-BRCA1/2, Germline-others (non-BRCA) and Others (non-carriers) (Figure 4A). There was no difference in the somatic mutation detection rate among the three groups (Figure 4B). Then, we analyzed the distribution of mutation types among the three groups (Figure 4C). Germline-BRCA1/2 group had significantly more missense mutations (P=0.02) and less copy number amplification (P=0.04) than the Germline-others group. Meanwhile, mutation types between Germline-others group and Others group were not statistically different (P>0.05). Moreover, the mutation rates of AKT1, CCND1, FGFR1, and PIK3CA were different among the three groups (Figure 4D and Supplementary Table 5). Mutations in AKT1 and CCND1 were not detected in the Germline-BRCA1/2 group. FGFR1 mutation rate was 24% in Germline-others group, 10% in Germline- BRCA1/2 group, and 9% in Others group. The PIK3CA mutation rate was significantly lower in Germline- BRCA1/2 group than the other two groups (Germline-BRCA1/2 vs Germline-others P=0.02; Germline-BRCA1/2 vs Others P=0.002). As shown in Figure 4E, PIK3CA H1047R was the hotspot mutation detected from all three groups. The Others group had significantly more missense PIK3CA mutations than the Germline-others group (P=0.02).
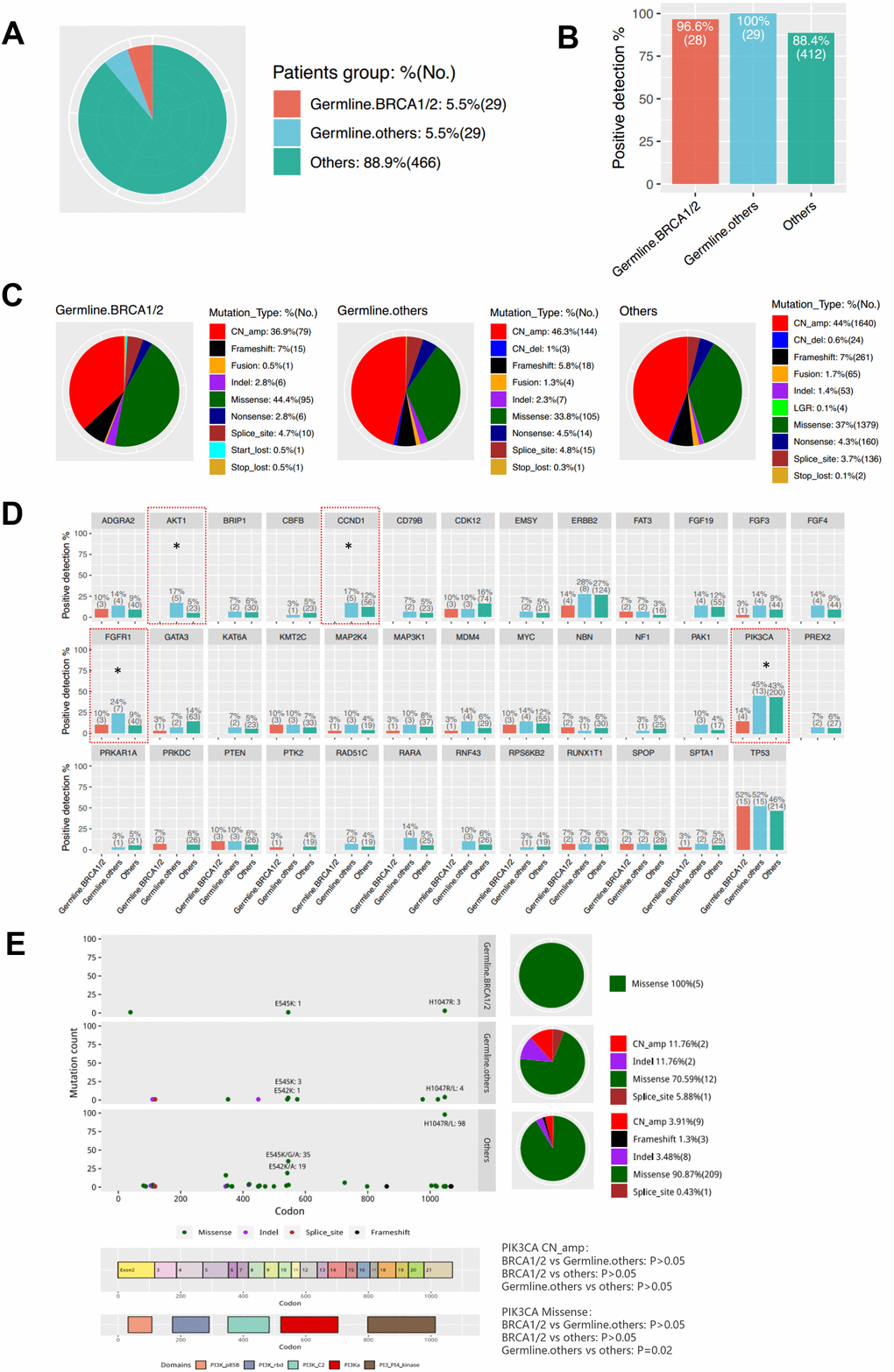
Figure 4. Characteristics of Somatic Mutations in Breast Cancer Patients with Germline Mutations. (A) Three groups according to germline mutations: Germline-BRCA1/2, Germline-others (non-BRCA) and Others (non-carriers). (B) Somatic mutation positive detection rate among the three groups. (C) The difference of the mutation type distribution among the three groups. (D) The difference of the mutation genes among the three groups. * P<0.05. (E). PIK3CA mutation spectrum in the three groups.
Discussion
In this study, we performed an NGS-based comprehensive analysis of germline mutations in 62 cancer susceptibility genes of 524 unselected Chinese patients with various stages of breast cancer. The inclusion of unselected breast cancer patients with various stages provided a more representative germline mutation landscape among these patients. To our knowledge, by simultaneously interrogating 62 cancer susceptibility genes, our study is the first to elucidate a more comprehensive germline mutation profile of unselected breast cancer patients in the Southern Chinese population.
Our study demonstrated the detection of a total of 76 LP/P germline mutations in 15 genes from 58 patients, revealing an overall germline mutation rate of 11.1%. In contrast, another study of a large cohort of unselected breast cancer patients from North China has revealed an LP/P germline mutation rate of 9.2% (743/8085) [25]. By identifying the 15 genes potentially associated with increased genetic cancer susceptibility in our population, we could advocate for the inclusion of these 15 genes in the routine diagnostic workup for the assessment of genetic cancer predisposition instead of just testing for only BRCA1/2 mutation status.
A number of studies have reported germline BRCA1/2 mutation rate of approximately 5% in unselected breast cancer patients regardless of ethnicity [25–30]. Interestingly, we found that Chinese breast cancer patients have more frequent mutations in BRCA2 than in BRCA1 which differ from those in Western breast cancer patients [2]. Meanwhile, most of the BRCA2 mutation carriers (77.8%) in our cohort are HR+/HER2-. Therefore, we should not overlook the clinical value of germline mutation test in both TNBC and non-TNBC patients in China. Our analysis also revealed a mutation rate of 5.72% (30/524) in other cancer predisposition genes beyond BRCA1/2. Although the frequency of mutations in each gene is much lower than BRCA1/2, the collective mutation rate is more than the mutation rate of BRCA1/2 in our cohort, providing important data for non-BRCA1/2 mutations in breast cancer patients in Southern Chinese population. In contrast, the recent survey by Sun et al. revealed a mutation rate of 2.9% (237/8085) and 1% (83/8085) in beyond BRCA1/2 genes and other cancer susceptibility genes, including mutations in PALB2 (n=56), TP53 (n=38), ATM (n=31), RAD51D (n=31), RECQL (n=30) and CHEK2 (n=27) among the most frequent [25]. Interestingly, germline mutation rate of members of the Fanconi anaemia family of genes (including BRCA2, PALB2, BRIP1, RAD51C, FANCA, FANCI and FANCL) was 53.4% (31/58) among the patients with germline mutations in our cohort. These data strongly support the inclusion of not only BRCA1/2, but also the Fanconi anaemia genes for the assessment of germline mutations in breast cancer patients. In addition to BRCA1/2, growing evidences implicate germline mutations in genes involved in homologous recombination repair pathway such as PALB2 in increased risk of breast and pancreatic cancer [6, 31] and improved sensitivity to therapeutic agents such as platinum-based chemotherapy and poly-ADP-ribose polymerase (PARP) inhibitors [32, 33]. A number of ongoing clinical trials are investigating the association of germline or somatic mutations in genes involved in homologous recombination repair including PALB2 and response to different therapeutic agents including chemotherapy in the adjuvant or neoadjuvant setting, PARP inhibitors or checkpoint inhibitors [33].
Among the 62 genes interrogated for germline mutation profiling, no LP/P germline mutations were detected in 47 genes from our cohort, indicating that LP/P germline mutations in these genes are rare in our population. In addition, with the comprehensive germline mutational profiling using 62 cancer susceptibility genes, VUS were detected in more than 90% of the patients. With the increase in the use of NGS in clinical practice, a growing number of VUS are being reported [34]. Further studies are required to understand the function of these variants and their association with the development of disease, particularly in this population.
Furthermore, our study has identified distinct somatic mutations among the carriers of germline mutations and non-carriers. We found that mutation type distribution was different among patients carrying germline mutations in BRCA1/2 than non-BRCA1/2. The mutation rates in AKT1, CCND1, FGFR1, and PIK3CA were different among the three groups. Interestingly, a patient with pathogenic germline PALB2 mutation (p.Q921fs) also had somatic PALB2 mutation (p.D525fs). The coexistence of LP/P germline and somatic mutations in this patient supports the “second-hit” hypothesis of breast cancer development [8].
There are two limitations in our study. First, all the 524 patients were from a single hospital with most of them from the Guangdong-Hong Kong-Macao Greater Bay Area. Second, no data for treatment responses and survival outcomes were available for analysis. Third, the sample size for certain molecular subtype was very limited. Larger nationwide multicenter studies should be conducted and long-term follow-up is needed to investigate the treatment and survival outcomes in germline mutation carriers.
Conclusions
Our findings have potential clinical implications. Firstly, our study is the most comprehensive germline mutation study in unselected breast cancer patients in Southern China interrogating all breast or ovarian cancer-related genes listed in the US genetic guidelines. Secondly, our findings may be useful for selecting the subset of breast cancer patients to receive multigene panel testing. The inclusion of the 15 most common cancer susceptibility genes in cancer genetic predisposition screening is clinically relevant for the Chinese population. Thirdly, we explored the important difference of somatic mutation profiles among BRCA, non-BRCA germline mutations carriers and non-carriers. It provided a basis for better understanding of the tumor characteristics of patients with LP/P germline mutations.
Materials and Methods
Patient selection
This study was approved by the institutional review board of the Guangdong Provincial People's Hospital, and all participants provided written informed consent. From March 1, 2016 through December 31, 2018, a total of 524 breast cancer patients (AJCC stage Tis to IV) seen at the Department of Breast Cancer in Guangdong Provincial People's Hospital were offered germline sequencing. The disclosure of results was in accordance to an institutional protocol of matched tumor-germline DNA sequencing. Patients were unselected for age or personal and family history of cancers. Clinical and family history data were obtained from medical records. American Society of Clinical Oncology (ASCO) /College of American Pathologists (CAP) guidelines were used to define estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) positivity. All breast cancers samples were reviewed by breast pathologists. Genetic test results from this analysis were considered research and were not used for clinical decision making.
Preparation of plasma and tissue samples
Plasma was separated from blood samples collected in EDTA-treated tubes by centrifugation (1,500 x g, 4°C, 10 min). Plasma fractions were transferred into fresh tubes, centrifuged (16,000 x g, 4°C, 10 min) to remove cell debris, aliquoted into fresh tubes, and stored at -80°C until DNA extraction. Breast cancer tissue samples were obtained by biopsy and processed into FFPE cell blocks.
DNA extraction
Cell-free DNA (cfDNA) and genomic DNA were isolated from plasma and tissue samples using a QIAamp Circulating Nucleic Acid kit or QIAamp DNA FFPE tissue kit, respectively, according to the manufacturer’s standard protocol (Qiagen, Hilden, Germany). Quantification of DNA obtained from plasma and tissue samples was performed using the Qubit dsDNA assay (Life Technologies, Carlsbad, CA, USA).
NGS library preparation, sequencing and data analysis
DNA was subjected to end repair, phosphorylation and adaptor ligation. Fragments of size 200–400bp were selected by AMPure beads (Agencourt AMPure XP Kit), followed by hybridization with capture probe baits, hybrid selection with magnetic beads and PCR amplification. A bioanalyzer high-sensitivity DNA assay was subsequently performed to assess the quality and size of the fragments. Indexed paired samples were sequenced on Nextseq500 sequencer (Illumina, Inc., USA) with paired-end reads in a Clinical Laboratory Improvement Amendments (CLIA)/CAP-certified laboratory using a panel consisting of 520 cancer-related genes, spanning 1.64 megabases of the human genome (OncoScreen Plus panel, Burning Rock Biotech, Guangzhou, China) [35]. The panel was designed to capture whole exons of 312 genes and critical exons, introns and promoter regions of the remaining 208 genes. The panel also includes 62 cancer susceptibility genes for profiling the germline variants (Supplementary Table 1). The 62 cancer susceptibility genes included in our study was based on the ACMG version 2.0 [36], National Comprehensive Cancer Network (NCCN) Guidelines Genetic/Familial High-Risk Assessment: Breast and Ovarian, Version 2.2017 [37] and Genomics guidelines [38–40]. Sequencing data were analyzed using the Burrows-Wheeler Aligner followed by Genome Analysis Toolkit with an established somatic and germline variant calling pipeline.
Identification and classification of germline variants
The reported mutations were further confirmed with dbSNP and ClinVar databases. Additionally, other databases such as BRCA Exchange, and Breast Cancer Information Core [41] were searched along with publications archived in PubMed to confirm the assigned class of the mutation, the level of clinical and functional evidence of the mutation and identify novel mutations. Intervar [16], the computational tool for semi-automated variant interpretation, was used to aggregate the variant annotations from multiple databases, prediction tools and publications at a single site. In the absence of clinical data and in vitro functional assay, in silico predictions using algorithms that assess phylogenetic conservation and the likelihood of severe physiochemical alterations in the protein structure or function were utilized as prediction tools. All genetic annotations and nomenclature were based on GRCh37/hg19 build. The variants were classified according to the American Society of Medical Genetics and Genomics (ACMG) recommendations for standards of interpretation and reporting of sequence variations. The variants were organized into five classes as follows: pathogenic (Class 5), likely pathogenic (Class 4), variants of uncertain significance (Class 3,) likely benign (Class 2) and benign (Class 1) [36]. Without departing from the scope of this study, only pathogenic and likely pathogenic (LP/P) mutations were further analyzed.
Statistical methods
Patient characteristics and sequencing results were summarized with descriptive statistics, including medians, means, and standard deviations for continuous data. Demographic, clinical, and pathologic characteristics were compared using the Chi-square test or Fisher’s exact test (categorical variables), as applicable. P<0.05 was considered statistically significant.
Ethics approval
Primary tumor biopsies were obtained using an Institutional Review Board approved protocol, and this study had been approved by the Ethics Committee of Guangdong Provincial People's Hospital. All patients provided written informed consent for translational research.
Author Contributions
NL, BC and GZ designed the study. BC, GZ, XL, GW, CR, KL, YW, HM, LW, MJ, CL, LG, JL, GW, YL, YZ participated in sample collection, sample processing, clinical information collection and data analysis. BC, XL, CR, JL and GZ analyzed and interpreted data. BC, NL and AL participated in manuscript writing. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare that they have no conflicts of interests.
Funding
This work was supported by funds from Natural Science Foundation of Guangdong Province (2016A030313768, Ning Liao) and Research Funds from Guangzhou Municipal Science and Technology Project (201707010418, Ning Liao); High-level Hospital Construction Project (DFJH201921, Bo Chen); the National Natural Science Foundation of China (81902828, Bo Chen); the Fundamental Research Funds for the Central Universities (y2syD2192230, Bo Chen); and Medical Scientific Research Foundation of Guangdong Province (B2019039, Bo Chen). The funding body has no roles in the design of the study and collection, analysis and interpretation of data and in writing the manuscript.
References
- 1. Balmaña J, Díez O, Castiglione M, Group EG, and ESMO Guidelines Working Group. BRCA in breast cancer: ESMO clinical recommendations. Ann Oncol. 2009 (Suppl 4); 20:19–20. https://doi.org/10.1093/annonc/mdp116 [PubMed]
- 2. Tung N, Lin NU, Kidd J, Allen BA, Singh N, Wenstrup RJ, Hartman AR, Winer EP, Garber JE. Frequency of Germline Mutations in 25 Cancer Susceptibility Genes in a Sequential Series of Patients With Breast Cancer. J Clin Oncol. 2016; 34:1460–68. https://doi.org/10.1200/JCO.2015.65.0747 [PubMed]
- 3. Khatcheressian JL, Wolff AC, Smith TJ, Grunfeld E, Muss HB, Vogel VG, Halberg F, Somerfield MR, Davidson NE, and American Society of Clinical Oncology. American Society of Clinical Oncology 2006 update of the breast cancer follow-up and management guidelines in the adjuvant setting. J Clin Oncol. 2006; 24:5091–97. https://doi.org/10.1200/JCO.2006.08.8575 [PubMed]
- 4. Han MR, Zheng W, Cai Q, Gao YT, Zheng Y, Bolla MK, Michailidou K, Dennis J, Wang Q, Dunning AM, Brennan P, Chen ST, Choi JY, et al. Evaluating genetic variants associated with breast cancer risk in high and moderate-penetrance genes in Asians. Carcinogenesis. 2017; 38:511–18. https://doi.org/10.1093/carcin/bgx010 [PubMed]
- 5. Hollestelle A, Wasielewski M, Martens JW, Schutte M. Discovering moderate-risk breast cancer susceptibility genes. Curr Opin Genet Dev. 2010; 20:268–76. https://doi.org/10.1016/j.gde.2010.02.009 [PubMed]
- 6. Rahman N, Seal S, Thompson D, Kelly P, Renwick A, Elliott A, Reid S, Spanova K, Barfoot R, Chagtai T, Jayatilake H, McGuffog L, Hanks S, et al, and Breast Cancer Susceptibility Collaboration (UK). PALB2, which encodes a BRCA2-interacting protein, is a breast cancer susceptibility gene. Nat Genet. 2007; 39:165–67. https://doi.org/10.1038/ng1959 [PubMed]
- 7. Zhang K, Zhou J, Zhu X, Luo M, Xu C, Yu J, Deng M, Zheng S, Chen Y. Germline mutations of PALB2 gene in a sequential series of Chinese patients with breast cancer. Breast Cancer Res Treat. 2017; 166:865–73. https://doi.org/10.1007/s10549-017-4425-z [PubMed]
- 8. Lee JE, Li N, Rowley SM, Cheasley D, Zethoven M, McInerny S, Gorringe KL, James PA, Campbell IG. Molecular analysis of PALB2-associated breast cancers. J Pathol. 2018; 245:53–60. https://doi.org/10.1002/path.5055 [PubMed]
- 9. Reiner AS, Sisti J, John EM, Lynch CF, Brooks JD, Mellemkjær L, Boice JD, Knight JA, Concannon P, Capanu M, Tischkowitz M, Robson M, Liang X, et al, and WECARE Study Collaborative Group. Breast Cancer Family History and Contralateral Breast Cancer Risk in Young Women: An Update From the Women’s Environmental Cancer and Radiation Epidemiology Study. J Clin Oncol. 2018; 36:1513–20. https://doi.org/10.1200/JCO.2017.77.3424 [PubMed]
- 10. Fan Z, Ouyang T, Li J, Wang T, Fan Z, Fan T, Lin B, Xu Y, Xie Y. Identification and analysis of CHEK2 germline mutations in Chinese BRCA1/2-negative breast cancer patients. Breast Cancer Res Treat. 2018; 169:59–67. https://doi.org/10.1007/s10549-018-4673-6 [PubMed]
- 11. Taylor A, Brady AF, Frayling IM, Hanson H, Tischkowitz M, Turnbull C, Side L, and UK Cancer Genetics Group (UK-CGG). Consensus for genes to be included on cancer panel tests offered by UK genetics services: guidelines of the UK Cancer Genetics Group. J Med Genet. 2018; 55:372–77. https://doi.org/10.1136/jmedgenet-2017-105188 [PubMed]
- 12. Mandelker D, Zhang L, Kemel Y, Stadler ZK, Joseph V, Zehir A, Pradhan N, Arnold A, Walsh MF, Li Y, Balakrishnan AR, Syed A, Prasad M, et al. Mutation Detection in Patients With Advanced Cancer by Universal Sequencing of Cancer-Related Genes in Tumor and Normal DNA vs Guideline-Based Germline Testing. JAMA. 2017; 318:825–35. https://doi.org/10.1001/jama.2017.11137 [PubMed]
- 13. Slavin TP, Niell-Swiller M, Solomon I, Nehoray B, Rybak C, Blazer KR, Weitzel JN. Clinical Application of Multigene Panels: Challenges of Next-Generation Counseling and Cancer Risk Management. Front Oncol. 2015; 5:208. https://doi.org/10.3389/fonc.2015.00208 [PubMed]
- 14. Bonnet-Serrano F, Bertherat J. Genetics of tumors of the adrenal cortex. Endocr Relat Cancer. 2018; 25:R131–52. https://doi.org/10.1530/ERC-17-0361 [PubMed]
- 15. Li JY, Jing R, Wei H, Wang M, Xiaowei Q, Liu H, Jian L, Ou JH, Jiang WH, Tian FG, Sheng Y, Li HY, Xu H, et al. Germline mutations in 40 cancer susceptibility genes among Chinese patients with high hereditary risk breast cancer. Int J Cancer. 2019; 144:281–89. https://doi.org/10.1002/ijc.31601 [PubMed]
- 16. Kurian AW, Li Y, Hamilton AS, Ward KC, Hawley ST, Morrow M, McLeod MC, Jagsi R, Katz SJ. Gaps in Incorporating Germline Genetic Testing Into Treatment Decision-Making for Early-Stage Breast Cancer. J Clin Oncol. 2017; 35:2232–39. https://doi.org/10.1200/JCO.2016.71.6480 [PubMed]
- 17. Park KS, Cho EY, Nam SJ, Ki CS, Kim JW. Comparative analysis of BRCA1 and BRCA2 variants of uncertain significance in patients with breast cancer: a multifactorial probability-based model versus ACMG standards and guidelines for interpreting sequence variants. Genet Med. 2016; 18:1250–57. https://doi.org/10.1038/gim.2016.39 [PubMed]
- 18. Cobain EF, Milliron KJ, Merajver SD. Updates on breast cancer genetics: clinical implications of detecting syndromes of inherited increased susceptibility to breast cancer. Semin Oncol. 2016; 43:528–35. https://doi.org/10.1053/j.seminoncol.2016.10.001 [PubMed]
- 19. Zhang G, Wang Y, Chen B, Guo L, Cao L, Ren C, Wen L, Li K, Jia M, Li C, Mok H, Chen X, Wei G, et al. Characterization of frequently mutated cancer genes in Chinese breast tumors: a comparison of Chinese and TCGA cohorts. Ann Transl Med. 2019; 7:179. https://doi.org/10.21037/atm.2019.04.23 [PubMed]
- 20. Wang J, Li W, Shi Y, Huang Y, Sun T, Tang L, Lu Q, Lei Q, Liao N, Jin F, Li H, Huang T, Qian J, et al. Germline mutation landscape of Chinese patients with familial breast/ovarian cancer in a panel of 22 susceptibility genes. Cancer Med. 2019; 8:2074–84. https://doi.org/10.1002/cam4.2093 [PubMed]
- 21. Thompson ER, Rowley SM, Li N, McInerny S, Devereux L, Wong-Brown MW, Trainer AH, Mitchell G, Scott RJ, James PA, Campbell IG. Panel Testing for Familial Breast Cancer: Calibrating the Tension Between Research and Clinical Care. J Clin Oncol. 2016; 34:1455–59. https://doi.org/10.1200/JCO.2015.63.7454 [PubMed]
- 22. Childers CP, Childers KK, Maggard-Gibbons M, Macinko J. National Estimates of Genetic Testing in Women With a History of Breast or Ovarian Cancer. J Clin Oncol. 2017; 35:3800–06. https://doi.org/10.1200/JCO.2017.73.6314 [PubMed]
- 23. Gabai-Kapara E, Lahad A, Kaufman B, Friedman E, Segev S, Renbaum P, Beeri R, Gal M, Grinshpun-Cohen J, Djemal K, Mandell JB, Lee MK, Beller U, et al. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc Natl Acad Sci USA. 2014; 111:14205–10. https://doi.org/10.1073/pnas.1415979111 [PubMed]
- 24. Kurian AW, Ward KC, Hamilton AS, Deapen DM, Abrahamse P, Bondarenko I, Li Y, Hawley ST, Morrow M, Jagsi R, Katz SJ. Uptake, Results, and Outcomes of Germline Multiple-Gene Sequencing After Diagnosis of Breast Cancer. JAMA Oncol. 2018; 4:1066–72. https://doi.org/10.1001/jamaoncol.2018.0644 [PubMed]
- 25. Sun J, Meng H, Yao L, Lv M, Bai J, Zhang J, Wang L, Ouyang T, Li J, Wang T, Fan Z, Fan T, Lin B, Xie Y. Germline Mutations in Cancer Susceptibility Genes in a Large Series of Unselected Breast Cancer Patients. Clin Cancer Res. 2017; 23:6113–19. https://doi.org/10.1158/1078-0432.CCR-16-3227 [PubMed]
- 26. Koumpis C, Dimitrakakis C, Antsaklis A, Royer R, Zhang S, Narod SA, Kotsopoulos J. Prevalence of BRCA1 and BRCA2 mutations in unselected breast cancer patients from Greece. Hered Cancer Clin Pract. 2011; 9:10. https://doi.org/10.1186/1897-4287-9-10 [PubMed]
- 27. Cancer Genome Atlas N, and Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012; 490:61–70. https://doi.org/10.1038/nature11412 [PubMed]
- 28. Abugattas J, Llacuachaqui M, Allende YS, Velásquez AA, Velarde R, Cotrina J, Garcés M, León M, Calderón G, de la Cruz M, Mora P, Royer R, Herzog J, et al. Prevalence of BRCA1 and BRCA2 mutations in unselected breast cancer patients from Peru. Clin Genet. 2015; 88:371–75. https://doi.org/10.1111/cge.12505 [PubMed]
- 29. Wen WX, Allen J, Lai KN, Mariapun S, Hasan SN, Ng PS, Lee DS, Lee SY, Yoon SY, Lim J, Lau SY, Decker B, Pooley K, et al. Inherited mutations in BRCA1 and BRCA2 in an unselected multiethnic cohort of Asian patients with breast cancer and healthy controls from Malaysia. J Med Genet. 2018; 55:97–103. https://doi.org/10.1136/jmedgenet-2017-104947 [PubMed]
- 30. Li J, Wen WX, Eklund M, Kvist A, Eriksson M, Christensen HN, Torstensson A, Bajalica-Lagercrantz S, Dunning AM, Decker B, Allen J, Luccarini C, Pooley K, et al. Prevalence of BRCA1 and BRCA2 pathogenic variants in a large, unselected breast cancer cohort. Int J Cancer. 2019; 144:1195–204. https://doi.org/10.1002/ijc.31841 [PubMed]
- 31. Tischkowitz M, Xia B. PALB2/FANCN: recombining cancer and Fanconi anemia. Cancer Res. 2010; 70:7353–59. https://doi.org/10.1158/0008-5472.CAN-10-1012 [PubMed]
- 32. Villarroel MC, Rajeshkumar NV, Garrido-Laguna I, De Jesus-Acosta A, Jones S, Maitra A, Hruban RH, Eshleman JR, Klein A, Laheru D, Donehower R, Hidalgo M. Personalizing cancer treatment in the age of global genomic analyses: PALB2 gene mutations and the response to DNA damaging agents in pancreatic cancer. Mol Cancer Ther. 2011; 10:3–8. https://doi.org/10.1158/1535-7163.MCT-10-0893 [PubMed]
- 33. Isaac D, Karapetyan L, Tamkus D. Association of Germline PALB2 Mutation and Response to Platinum-Based Chemotherapy in Metastatic Breast Cancer: A Case Series. JCO Precis Oncol. 2018; 1–5. https://doi.org/10.1200/PO.17.00258
- 34. Hoffman-Andrews L. The known unknown: the challenges of genetic variants of uncertain significance in clinical practice. J Law Biosci. 2018; 4:648–57. https://doi.org/10.1093/jlb/lsx038 [PubMed]
- 35. Chen B, Zhang G, Wei G, Wang Y, Guo L, Lin J, Li K, Mok H, Cao L, Ren C, Wen L, Jia M, Li C, et al. Heterogeneity of genomic profile in patients with HER2-positive breast cancer. Endocrine-related cancer. 2020; 3:153–162. https://doi.org/10.1530/ERC-19-0414 [PubMed]
- 36. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, Grody WW, Hegde M, Lyon E, Spector E, Voelkerding K, Rehm HL; ACMG Laboratory Quality Assurance Committee. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015; 17:405–24. https://doi.org/10.1038/gim.2015.30 [PubMed]
- 37. Daly MB, Pilarski R, Berry M, Buys SS, Farmer M, Friedman S, Garber JE, Kauff ND, Khan S, Klein C, Kohlmann W, Kurian A, Litton JK, et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast and Ovarian, Version 2.2017. J Natl Compr Canc Netw. 2017; 15:9–20. https://doi.org/10.6004/jnccn.2017.0003 [PubMed]
- 38. Rahman N. Realizing the promise of cancer predisposition genes. Nature. 2014; 505:302–08. https://doi.org/10.1038/nature12981 [PubMed]
- 39. Cheng DT, Prasad M, Chekaluk Y, Benayed R, Sadowska J, Zehir A, Syed A, Wang YE, Somar J, Li Y, Yelskaya Z, Wong D, Robson ME, et al. Comprehensive detection of germline variants by MSK-IMPACT, a clinical diagnostic platform for solid tumor molecular oncology and concurrent cancer predisposition testing. BMC Med Genomics. 2017; 10:33. https://doi.org/10.1186/s12920-017-0271-4 [PubMed]
- 40. Gupta S, Provenzale D, Regenbogen SE, Hampel H, Slavin TP
Jr , Hall MJ, Llor X, Chung DC, Ahnen DJ, Bray T, Cooper G, Early DS, Ford JM, et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Colorectal, Version 3.2017. J Natl Compr Canc Netw. 2017; 15:1465–75. https://doi.org/10.6004/jnccn.2017.0176 [PubMed] - 41. Szabo C, Masiello A, Ryan JF, Brody LC. The breast cancer information core: database design, structure, and scope. Hum Mutat. 2000; 16:123–31. https://doi.org/10.1002/1098-1004(200008)16:2<123::AID-HUMU4>3.0.CO;2-Y [PubMed]