



Introduction
Rapid eye movement (REM) sleep behavior disorder (RBD) is a parasomnia characterized by the loss of normal skeletal muscle atonia during REM sleep and dream-enacting behaviors [1]. Its’ prevalence was estimated to be 1-2% in the general elderly populations [2, 3]. RBD can occur in association with (secondary RBD) or without (isolated RBD) a neurodegenerative disorder [1], and isolated RBD accounts for up to 60% at the diagnosis [4]. However, more than 80% of isolated RBD eventually developed a neurodegenerative disorder such as Parkinson’s disease (PD) and Lewy body disease (DLB) in 12-14 years [5, 6], which implies that a majority of isolated RBD may be a prodromal phase of α-synucleinopathies [1, 4].
A series of clinical trials found that the symptoms of RBD were improved by N-acetyl-5-methoxytryptamine (melatonin). In RBD patients, dream-enacting behaviors were reduced and REM sleep muscle atonia were restored by the administration of melatonin [7–11] but relapsed by discontinuation of melatonin [8]. Melatonin is a multifunctioning indoleamine produced by the pineal gland [12]. The pineal gland regulates sleep and circadian rhythm through the synthesis and secretion of melatonin [12, 13]. In humans, roughly 80% of the pineal gland is composed of melatonin-producing pinealocytes [13], and the volume of pineal gland (VPG) is proportional to the levels of melatonin in plasma, urine or saliva [14–16]. Although the pineal gland is reported to fully develop after the first year of life and does not change in size or weight later in life [12, 17, 18], recent studies have found that VPG could be changed by lifestyle such as coffee consumption or pathological conditions that may change melatonin production [19–21]. Given the effects of melatonin on RBD symptoms and the association of melatonin with VPG [14–16], we may assume that RBD patients may have smaller VPG than the individuals without RBD, and VPG may predict the future risk of RBD in the individuals without RBD. In this study, we investigated the association of VPG with current RBD symptoms cross-sectionally and with the future risk of RBD symptoms prospectively in cognitively normal (CN) elderly individuals without neurological or psychiatric disorders.
Results
The demographic and clinical characteristics of the participants are summarized in Table 1. The participants with probable RBD (pRBD) showed smaller volume of pineal parenchyma (VPP) and VPG than those without pRBD (p < 0.001).
Table 1. Demographic and clinical characteristics of the participants.
| Prevalent pRBD at baseline | Incident pRBD at 2-year follow-up | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Absent (n = 221) | Present (n = 24) | p | Absent (n = 142) | Present (n = 4) | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years, mean ± SD) | 71.79 ± 6.17 | 72.50 ± 6.16 | 0.594a | 70.70 ± 5.87 | 76.00 ± 7.96 | 0.080a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Women, n (%) | 114 (51.58) | 11 (45.83) | 0.592b | 72 (50.70) | 1 (25.00) | 0.311b | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education (years, mean ± SD) | 11.43 ± 4.93 | 10.42 ± 5.03 | 0.341a | 11.35 ± 5.11 | 13.75 ± 4.03 | 0.352a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Presence of cohabitants, n (%) | 191 (86.43) | 23 (95.83) | 0.188b | 124 (87.32) | 3 (75.00) | 0.470b | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcohol drinking (standard units/week, mean ± SD) | 3.03 ± 7.66 | 6.00 ± 11.17 | 0.215a | 3.67 ± 8.86 | 3.63 ± 5.71 | 0.992a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking (packs/day, mean ± SD) | 0.03 ± 0.18 | 0.02 ± 0.08 | 0.797a | 0.04 ± 0.21 | 0.00 ± 0.00 | 0.680a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| History of head injury, n (%) | 11 (4.98) | 1 (4.17) | 0.861b | 8 (5.63) | 0 (0.00) | 0.625b | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MMSE (points, mean ± SD) | 27.40 ± 2.06 | 27.17 ± 2.81 | 0.616a | 27.29 ± 2.11 | 27.00 ± 0.82 | 0.786a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GDS (points, mean ± SD) | 7.71 ± 5.63 | 9.93 ± 7.69 | 0.199a | 7.49 ± 5.68 | 12.00 ± 6.38 | 0.121a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CIRS (points, mean ± SD) | 5.62 ±2.83 | 6.33 ± 2.46 | 0.237a | 5.09 ± 2.64 | 6.50 ± 3.42 | 0.298a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| STOPBANG (points, mean ± SD) | 2.54 ± 0.94 | 2.96 ± 0.75 | 0.037a | 2.50 ± 0.95 | 3.25 ± 0.96 | 0.121a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RBDSQ (points, mean ± SD) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total score | 1.48 ± 1.26 | 5.79 ± 1.22 | < 0.001a | 1.37 ± 1.21 | 3.00 ± 1.16 | 0.009a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Item 6 score | 0.12 ± 0.37 | 1.17 ± 1.05 | < 0.001a | 0.10 ± 0.32 | 0.75 ± 0.96 | 0.267a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intracranial volume (cm3, mean ± SD) | 1565.40 ± 160.86 | 1553.13 ± 170.68 | 0.725a | 1576.95 ± 156.49 | 1530.15 ± 66.05 | 0.553a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VPP (mm3, mean ± SD) | 87.55 ± 30.04 | 58.42 ± 16.49 | < 0.001c | 90.13 ± 30.15 | 53.00 ± 20.07 | 0.016a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VPG (mm3, mean ± SD) | 95.18 ± 39.96 | 61.13 ± 18.30 | < 0.001c | 98.58 ± 42.12 | 56.25 ± 20.99 | 0.048a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: pRBD = probable REM sleep behavior disorder; SD = standard deviation; MMSE = Mini-Mental State Examination; GDS = Geriatric Depression Scale; CIRS = Cumulative Illness Rating Scale; RBDSQ = REM Sleep Behavior Disorder Screening Questionnaire; VPP = pineal parenchyma volume; VPG = pineal gland volume. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aIndependent sample t-test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bChi-square test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| cAnalysis of covariance adjusted for age, sex, years of education, intracranial volume, head injury, amount of smoking, and amount of alcohol drinking. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Both VPP and VPG were inversely associated with the REM Sleep Behavior Disorder Screening Questionnaire (RBDSQ) total score (RBDSQ-T) (standardized β = -0.352, p < 0.001 for VPP; standardized β = -0.301, p < 0.001 for VPG) and the item 6 score of the RBDSQ (RBDSQ-6) (standardized β = -0.239, p < 0.001 for VPP; standardized β = -0.198, p = 0.002 for VPG), indicating that the individuals with smaller VPP or VPG may have more RBD symptoms (Figure 1). There was no evidence of multicollinearity in all regression models with the maximum variance inflation factor being 2.05.
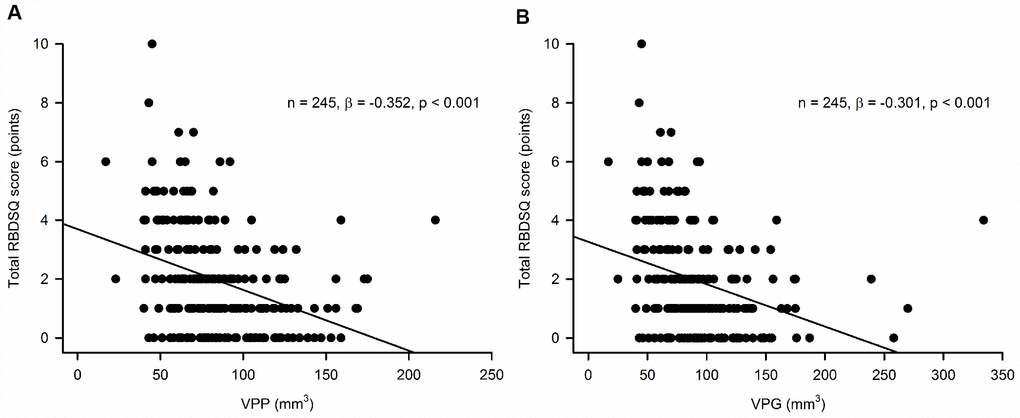
Figure 1. Association of (A) pineal parenchyma volume (VPP, mm3) and (B) pineal gland volume (VPG, mm3) with the REM Sleep Behavior Disorder Screening Questionnaire (RBDSQ) total scorea.aMultiple linear regression model adjusted for age, sex, years of education, intracranial volume, head injury, amount of smoking, and amount of alcohol drinking.
Baseline VPP and VPG were inversely associated with the risk of prevalent pRBD at the baseline evaluation (odds ratio [OR] = 0.939, 95% CI = 0.912 - 0.966, p < 0.001 for VPP; OR = 0.947, 95% CI = 0.924 - 0.972, p < 0.001 for VPG), indicating that the individuals with larger VPP and VPG may have a lower risk of prevalent pRBD (Table 2). The baseline VPP and VPG were also inversely associated with the risk of incident pRBD at the 2-year follow-up evaluation (OR = 0.890, 95% CI = 0.798 - 0.993, p = 0.036 for VPP; OR = 0.912, 95% CI = 0.832 - 0.999, p = 0.047 for VPG), indicating that the individuals with larger VPP and VPG may have a lower risk of future pRBD (Table 2).
Table 2. Association of the baseline pineal parenchyma volume and pineal gland volume with the prevalent and incident probable REM sleep behavior disorder.
| Total, n | pRBD, n | OR (95% CI)a | pa | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| For prevalent pRBD | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VPP (mm3) | 245 | 24 | 0.939 (0.912 - 0.966) | < 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VPG (mm3) | 245 | 24 | 0.947 (0.924 - 0.972) | < 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| For incident pRBD | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VPP (mm3) | 146b | 4 | 0.890 (0.798 - 0.993) | 0.036 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VPG (mm3) | 146b | 4 | 0.912 (0.832 - 0.999) | 0.047 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: pRBD = probable REM sleep behavior disorder; VPP = pineal parenchyma volume; VPG = pineal gland volume; OR = odds ratio; CI = confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aBinary logistic regression analyses adjusting age, sex, years of education, intracranial volume, head injury, amount of smoking, and amount of alcohol drinking at the baseline evaluation as covariates. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bThe number of participants who did not have probable RBD at the baseline evaluation and completed the 2-year follow-up evaluation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The diagnostic accuracies of the baseline VPP and VPG for prevalent pRBD at the baseline evaluation were good; area under the receiver operator characteristic curve (AUC) was 0.82 (95% CI = 0.762 - 0.863, p < 0.0001) for VPP and 0.81 (95% CI = 0.749 - 0.852, p < 0.0001) for VPG (Figure 2). The optimal cutoff values of the baseline VPP and VPG for classifying pRBD were 70 mm3 (sensitivity = 87.50%; specificity = 70.59%) and 77 mm3 (sensitivity = 83.33%; specificity = 64.25%), respectively. The predictive accuracies of baseline VPP and VPG for incident pRBD at the 2-year follow-up evaluation were also good; AUC was 0.89 (95% CI = 0.821 - 0.932, p < 0.0001) for VPP and 0.87 (95% CI = 0.799 - 0.916, p < 0.0001) for VPG (Figure 2). The optimal cutoff values of the baseline VPP and VPG for predicting incident pRBD at 2-year follow-up evaluation were 65 mm3 (sensitivity = 100.00%; specificity = 83.10%) and 69 mm3 (sensitivity = 100.00%; specificity = 78.87%), respectively.
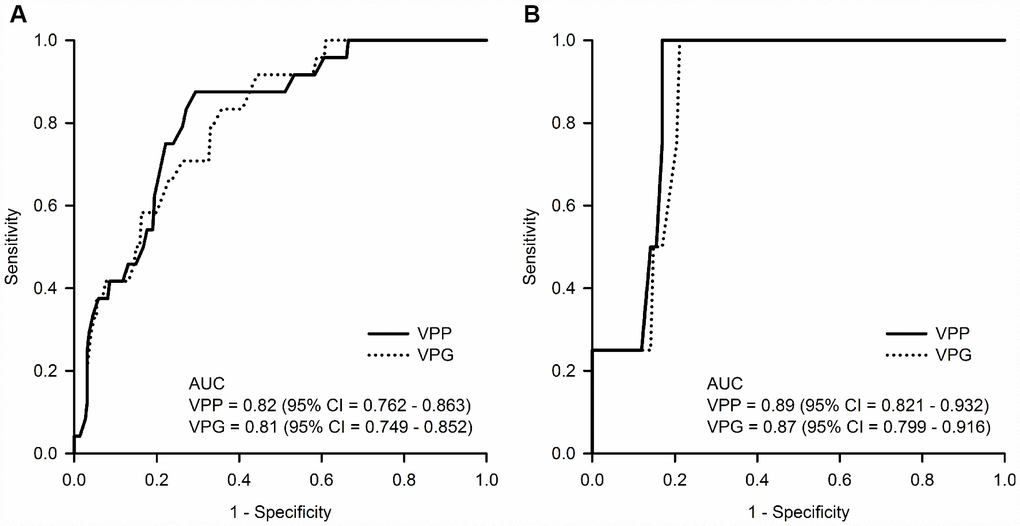
Figure 2. (A) Diagnostic accuracy for prevalent probable REM sleep behavior disorder (pRBD) at the baseline evaluation and (B) predictive accuracy for incident pRBD at the 2-year follow-up evaluation of the baseline pineal parenchyma volume (VPP, mm3) and pineal gland volume (VPG, mm3). Abbreviations: AUC = area under the receiver operator characteristic curve; CI = confidence intervals.
Discussion
In animals, nighttime REM sleep disturbances were induced by lesioning the pineal gland, which reduced pineal melatonin secretion [22]. However, the association between the pineal gland and RBD has never been investigated in humans. The current study directly showed that smaller pineal gland was associated with the more RBD symptoms and the higher risk of incident pRBD in CN elderly individuals.
Considering that the pineal gland volume was highly correlated with the endogenous melatonin level [14–16], our observation seems to be in line with previous studies on the effects of melatonin on RBD. Melatonin treatment decreased the frequency and severity of dream-enacting behaviors and the risk of falls in the elderly RBD patients [10], and the beneficial effects of melatonin (3-12 mg) lasted beyond a year in a series of RBD patients [9]. A couple of clinical trials on the polysomnography-diagnosed RBD patients found that the percentage of REM sleep without atonia and movement time in REM were reduced by administering melatonin before bedtime for 4-6 weeks [7, 8] but relapsed by discontinuing melatonin [8]. Another open-label trial reported that the percentage of tonic REM activity was reduced from 16% to 6% by administering 3-9 mg of melatonin at night, especially in the elderly patients with low endogenous melatonin secretion [23]. A placebo-controlled trial also reported that the percentage of REM sleep increased from 14.7% to 17.8% and the clinical global impression and daytime dysfunction were improved by administering 3 mg melatonin before bedtime in the individuals with disturbed and reduced REM sleep duration [11]. However, it remains unknown how melatonin improves the RBD symptoms. Multiple actions of melatonin such as decreasing muscle tonicity during REM sleep, enhancing GABAergic inhibition, stabilizing circadian clock variability and desynchronization, protecting cytoskeletal structure through its antagonism of calmodulin, enhancing sleep efficiency and shortening sleep latency may underlie the its beneficial effect on RBD [1, 10]. In a glycine/GABA-A receptor knockout transgenic mouse model of RBD, melatonin was efficacious in decreasing REM motor behaviors and restoring REM muscle atonia [24].
VPP and VPG showed good diagnostic accuracy for prevalent pRBD and predictive accuracy for incident pRBD in the current study, indicating that VPP or VPG may be potential biomarkers of isolated RBD in cognitively normal elderly individuals. However, the reduced VPP or VPG of the elderly individuals with isolated pRBD or those who are destined to have isolated pRBD in the future may be associated with prodromal α-synucleinopathies rather than RBD itself. Indeed, PD patients showed diminished endogenous melatonin production compared to controls [25]. In addition, melatonin directly blocked the α-synuclein fibril formation, destabilized preformed α-synuclein fibrils, and decreased α-synuclein-induced cytotoxicity [26]. Nevertheless, the changes of pineal gland volume in the patients with α-synucleinopathies have not been directly investigated yet.
This study has a couple of strengths. First, we excluded the volume of pineal cysts (VPC) when we estimated the pineal parenchyma volume because pineal cysts do not contain pinealocytes [21, 27], and exclude the subjects with extremely large cystic glands from the current study. Although both VPP and VPG were associated with the prevalent and incident pRBD in the current study, pineal parenchyma volume (i.e., non-cystic volume) better reflected the levels of endogenous melatonin secretion than total pineal gland volume in adult individuals [14, 15]. Although we did not directly investigate the association between VPC and RBD, this result may suggest that the presence of the pineal cysts itself may not affect RBD symptoms. Second, we excluded the subjects who were depressive and/or were taking antidepressants since depression may increase the risk of RBD and antidepressants, selective serotonin reuptake inhibitor (SSRI) and serotonin norepinephrine reuptake inhibitor (SNRI) in particular, may produce dream-enacting behavior and loss of normal REM sleep atonia [1, 28]. However, this study also has several limitations. First, although the RBDSQ is well validated in polysomnography-confirmed RBD patients [1, 29], it may be subject to recall bias and misclassification bias. However, it seems unlikely that systematic errors would be made in reporting behavioral features of RBD since the current study included CN individuals who were examined only through comprehensive clinical and neuropsychological assessments. In addition, we tried to reduce the risk of misclassification bias by confirming the association of VPP and VPG with the RBDSQ item 6 score as well as RBDSQ total score. The RBDSQ item 6 queries the core symptoms of RBD with a good specificity [30]. Second, we cannot completely rule out the possibility that non-RBD symptoms might have influence the RBDSQ scores. For example, some patients with restless leg syndrome (RLS) or severe obstructive sleep apnea (OSA) showed the behaviors mimicking RBD during sleep [31, 32]. Although we exclude the participants with OSA by excluding the participants who got 5 points or higher in STOPBANG, the participants with pRBD showed modestly higher STOPBANG score than those without pRBD at baseline. Third, we could not adjust for the volume of pineal calcification because we did not perform additional brain computed tomography or high-resolution T2-weighted MRI. Although the effects of pineal calcification on melatonin production or human REM sleep remain unclear, a couple of previous studies argue that pineal calcification may inhibit the capacity for pineal melatonin synthesis and be associated with polysomnographic sleep parameters in humans [19, 33]. Furthermore, calcifications can appear hypointense on T1-weighted images, which may lead underestimation of the VPP. Fourth, although we excluded individuals who took exogenous melatonin over the past 6 weeks, we did not directly quantify the endogenous nocturnal melatonin levels in the blood. Fifth, the sample size was small. In the statistical power analysis with α error probability of 0.05 (G*Power version 3.1; http://www.gpower.hhu.de), the statistical power (1–beta error) for the prevalent and incident pRBD was 0.52 and 0.54, respectively. However, the association of pineal gland volume and the prevalent and incident pRBD was statistically significant despite the low statistical power in the current study. Sixth, since the small number of converters at 2-year follow-up, the accuracies of cutoff values of the baseline VPP and VPG for predicting incident pRBD may need to be further validated in future studies with a larger sample size and longer follow-up. Finally, the follow-up duration was short.
In summary, the smaller pineal gland was associated with the more current RBD symptoms and the higher future risk of RBD in cognitively normal elderly individuals, and VPP or VPG may be a candidate biomarker of RBD.
Materials and Methods
Study participants
The present sample of 245 CN elderly individuals comprised 157 and 88 subjects from the participants of the baseline evaluation of the Korean Longitudinal Study on Cognitive Aging and Dementia (KLOSCAD) [34] and the first follow-up evaluation of the Korean Longitudinal Study on Health and Aging (KLOSHA) [35], respectively, which were conducted from November 2010 to October 2012. Both the KLOSCAD and KLOSHA were population-based prospective elderly cohort studies. The KLOSCAD study randomly sampled 30 villages and towns from 13 specific districts across South Korea, and randomly selected 10% and 20% of the elderly adults from urban and rural areas, respectively, using resident rosters and data on residents aged ≥ 60 years. The KLOSHA study randomly selected community-dwelling Korean elderly adults aged ≥ 65 years from the resident roster of Seongnam, one of the largest satellite cities of Seoul. Among the 221 participants who did not have pRBD at the baseline evaluation, 146 completed the 2-year follow-up evaluation. In the current study, we excluded the following conditions: cognitive disorders such as dementia and mild cognitive impairment (MCI); major psychiatric and/or neurologic disorders that could affect cognitive function; any history of brain tumors, substance abuse or dependence, and use of clonazepam, antidepressants (SSRI, SNRI, and others), or exogenous melatonin over the past 6 weeks; any serious medical condition that could affect the structure and/or function of the pineal gland or abnormalities in pineal gland morphology such as neoplastic lesions or extremely large cystic gland (diameter greater than 15.0 mm) [36]; and conditions that could mimic the symptoms of RBD such as RLS and OSA. We diagnosed RLS using the Cambridge-Hopkins Restless Leg Syndrome questionnaire (CHRLSq) [37] and defined OSA as a STOPBANG questionnaire [38] score of ≥ 5 points.
The study protocol was approved by the institutional review board of the Seoul National University Bundang Hospital. All the participants were fully informed of the study protocol, and written informed consent was provided by them or their legal guardians.
Assessment of cognitive function
In both the KLOSCAD and the KLOSHA, geriatric psychiatrists with expertise in dementia research administered face-to-face standardized diagnostic interviews, detail medical histories, laboratory tests, and physical and neurological examinations using the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet Clinical Assessment Battery (CERAD-K) [39] and the Korean version of the Mini International Neuropsychiatric Interview [40]. In addition, research neuropsychologists administered the Digit Span Test [41], Frontal Assessment Battery [42], Geriatric Depression Scale (GDS) [43], Cumulative Illness Rating Scale (CIRS) [44], and CERAD-K Neuropsychological Assessment Battery (CERAD-K-N) [39, 45]. All participants performed -1.0 SD of the age-, gender-, and education-adjusted norms of elderly Koreans on the Mini-Mental State Examination (MMSE) [46]. Using a study-specific standard interview, trained research nurses collected data on age, sex, years of education, intracranial volume (ICV), history of head injury, amount of smoking (packs/day), and alcohol drinking (standard units/week) over the past twelve months period.
A panel of research neuropsychiatrists determined the participants’ final diagnoses in both the KLOSCAD [34] and the KLOSHA [35]. Two neuropsychiatrists (K.W.K and J.W.H) participated in both panels. In both the KLOSCAD and the KLOSHA, we diagnosed dementia and other Axis I mental disorders according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria [47] and MCI according to the criteria by the International Working Group on MCI [48]. We defined CN as functioning independently in the community and showing no evidence of cognitive impairment in objective neuropsychological tests.
Assessment of RBD symptoms
We evaluated behavioral features of RBD using the RBDSQ [29]. The RBDSQ is a self-reported screening instrument for diagnosing RBD and is comprised of 10 items assessing the most prominent clinical features of RBD: items 1 to 4, the frequency and content of dreams and their relationship to nocturnal movements and behavior; item 5, self-injuries and injuries to the bed partner; item 6, four subsections specifically assessing nocturnal motor behavior, e.g. questions about nocturnal vocalization (6.1), sudden limb movements (6.2), complex movements (6.3) or bedside items that fall down (6.4); items 7 and 8, nocturnal awakenings; item 9, disturbed sleep in general; and item 10, the presence of any neurological disorder. Each item could be answered as ‘‘yes’’ or ‘‘no’’. The RBDSQ score ranges from 0-13 points, with higher scores indicating more features associated with RBD. We defined pRBD individuals as having a total score of 5 or higher on the RBDSQ [29]. The questionnaire was completed by the subjects with aid from their partners if needed.
Segmentation of the pineal gland
We performed brain MRI using a Philips 3.0 Tesla Achieva scanners (Philips Medical Systems; Eindohovenm, the Netherlands) within 3 months of the clinical assessments. We obtained 3D structural T1-weighted spoiled gradient echo sequences with the following parameters: acquisition voxel size = 1.0 × 0.5 × 0.5 mm; 1.0 mm sagittal slice thickness with no inter-slice gap; repetition time = 4.61 ms; echo time = 8.15 ms; number of excitations = 1; flip angle = 8°; field of view = 240 × 240 mm; and acquisition matrix size = 175 × 256 × 256 mm in the x-, y-, and z-dimensions. We implemented bias field correction to remove the signal intensity inhomogeneity artifacts of MR images using Statistical Parametric Mapping software (version 8, SPM8; Wellcome Trust Centre for Neuroimaging, London; https://www.fil.ion.ucl.ac.uk/spm) in MATLAB R2014a (MathWorks Inc., Natick, MA, USA). We resliced the MR images into an isotropic voxel size of 1.0 × 1.0 × 1.0 mm3. We measured ICV using FreeSurfer software (version 5.3.0; http://surfer.nmr.mgh.harvard.edu) to adjust for inter-individual variabilities in brain volume.
For each participant, trained researchers blinded to the demographics and clinical characteristics constructed a 3D mask of each pineal gland by manually segmenting the pineal gland slice-by-slice on the resliced T1-weighted MR images using the ITK-SNAP (version 3.4.0; http://www.itksnap.org) volumetric imaging software. We segmented the pineal glands primarily on the sagittal planes and corroborated the results on the axial and coronal planes. We identified the pineal gland using the following structures as guides: the quadrigeminal cisterna, posterior portion of the third ventricle, superior colliculus, and habenula. Except for the portion connected to the habenula, defining of the boundaries of the pineal gland was straightforward as it is surrounded by cerebrospinal fluid [13]. We carefully differentiated the pineal gland from the adjacent vascular structures, especially the vein of Galen and the paired internal cerebral veins. We defined a pineal cyst as an area of homogenous intensity that was isointense to cerebrospinal fluid in T1 sequence images [27, 49] with a diameter of 2.0 mm or greater [27]. We measured the VPG and VPC and estimated the VPP by subtracting VPC from VPG.
To determine inter-rater reliability, we assessed the intraclass correlation coefficients (ICCs) for 30 subjects who were randomly selected from the 258 participants with a time gap of 2 months. The ICCs were 0.971 (95% confidence interval [CI] = 0.940 - 0.986) for the VPG and 0.950 (95% CI = 0.894 - 0.976) for the VPC. The VPG was strongly correlated with the VPP (r = 0.914, p < 0.001) and the VPC (r = 0.701, p < 0.001) in our participants.
Statistical analysis
We compared continuous variables using independent samples t-tests and categorical variables using chi-square tests between groups. We examined the associations of VPP and VPG with RBDSQ-T using multiple linear regression model adjusted for age, sex, years of education, ICV, head injury, smoking, and alcohol drinking as covariates. To test the robustness of our observation, we also examined the associations of VPP and VPG with the RBDSQ-6 using multiple linear regression model adjusted for diagnosis, age, sex, years of education, ICV, head injury, smoking, and alcohol drinking as covariates. In each of the linear regression models, VPP, VPG, RBDSQ-T and RBDSQ-6 were entered as continuous variables. We assessed multicollinearity using collinearity statistical tests (tolerance and variance inflation factor). We compared VPP and VPG between the participants with pRBD and those without pRBD using analysis of covariance that adjusted for age, sex, years of education, ICV, head injury, smoking, and alcohol drinking as covariates. We examined the association of baseline VPP and VPG with the risk of prevalent pRBD at baseline and the risk of incident pRBD at 2-year follow-up evaluation using binary logistic regression analyses that adjusted for age, sex, years of education, ICV, head injury, smoking, and alcohol drinking at the baseline evaluation as covariates. We examined the diagnostic performances of the baseline VPP and VPG for prevalent pRBD at the baseline evaluation and the predictive accuracy for incident pRBD at the 2-year follow-up evaluation using the ROC analyses. We calculated the optimal cutoff values and AUC using Youden index maximum (sensitivity + specificity − 1) [50].
For all analyses, we considered a two-tailed p-value less than 0.05 as statistically significant, and we employed Bonferroni corrections to reduce type I error when multiple comparisons were conducted. We performed all statistical analyses using SPSS for Windows (version 20.0; IBM Corporation; Armonk, NY).
Author Contributions
Conception and design: JP and KWK; Acquisition of the data: JWH, SWS, SB, JHH, JBB, JHK, KWK; Analysis and interpretation of data: All authors; Drafting of the manuscript and figures: JP and KWK; Critical revision of the manuscript for important intellectual content: All authors.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
This study was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health, Welfare, Republic of Korea (grant no. HI09C1379 [A092077]), the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2015R1D1A1A01059251), and Institute for Information and communications Technology Promotion (IITP) grant funded by the Korea government (MSIT) (2018-2-00861, Intelligent SW Technology Development for Medical Data Analysis).
References
- 1. Boeve BF. REM sleep behavior disorder: updated review of the core features, the REM sleep behavior disorder-neurodegenerative disease association, evolving concepts, controversies, and future directions. Ann N Y Acad Sci. 2010; 1184:15–54. https://doi.org/10.1111/j.1749-6632.2009.05115.x [PubMed]
- 2. Haba-Rubio J, Frauscher B, Marques-Vidal P, Toriel J, Tobback N, Andries D, Preisig M, Vollenweider P, Postuma R, Heinzer R. Prevalence and determinants of rapid eye movement sleep behavior disorder in the general population. Sleep. 2018; 41:zsx197. https://doi.org/10.1093/sleep/zsx197 [PubMed]
- 3. Kang SH, Yoon IY, Lee SD, Han JW, Kim TH, Kim KW. REM sleep behavior disorder in the Korean elderly population: prevalence and clinical characteristics. Sleep. 2013; 36:1147–52. https://doi.org/10.5665/sleep.2874 [PubMed]
- 4. Fantini ML, Ferini-Strambi L, Montplaisir J. Idiopathic REM sleep behavior disorder: toward a better nosologic definition. Neurology. 2005; 64:780–86. https://doi.org/10.1212/01.WNL.0000152878.79429.00 [PubMed]
- 5. Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. 2013; 14:744–48. https://doi.org/10.1016/j.sleep.2012.10.009 [PubMed]
- 6. Iranzo A, Tolosa E, Gelpi E, Molinuevo JL, Valldeoriola F, Serradell M, Sanchez-Valle R, Vilaseca I, Lomeña F, Vilas D, Lladó A, Gaig C, Santamaria J. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behaviour disorder: an observational cohort study. Lancet Neurol. 2013; 12:443–53. https://doi.org/10.1016/S1474-4422(13)70056-5 [PubMed]
- 7. Kunz D, Mahlberg R. A two-part, double-blind, placebo-controlled trial of exogenous melatonin in REM sleep behaviour disorder. J Sleep Res. 2010; 19:591–96. https://doi.org/10.1111/j.1365-2869.2010.00848.x [PubMed]
- 8. Kunz D, Bes F. Melatonin as a therapy in REM sleep behavior disorder patients: an open-labeled pilot study on the possible influence of melatonin on REM-sleep regulation. Mov Disord. 1999; 14:507–11. https://doi.org/10.1002/1531-8257(199905)14:3<507::AID-MDS1021>3.0.CO;2-8 [PubMed]
- 9. Boeve BF, Silber MH, Ferman TJ. Melatonin for treatment of REM sleep behavior disorder in neurologic disorders: results in 14 patients. Sleep Med. 2003; 4:281–84. https://doi.org/10.1016/S1389-9457(03)00072-8 [PubMed]
- 10. McCarter SJ, Boswell CL, St Louis EK, Dueffert LG, Slocumb N, Boeve BF, Silber MH, Olson EJ, Tippmann-Peikert M. Treatment outcomes in REM sleep behavior disorder. Sleep Med. 2013; 14:237–42. https://doi.org/10.1016/j.sleep.2012.09.018 [PubMed]
- 11. Kunz D, Mahlberg R, Müller C, Tilmann A, Bes F. Melatonin in patients with reduced REM sleep duration: two randomized controlled trials. J Clin Endocrinol Metab. 2004; 89:128–34. https://doi.org/10.1210/jc.2002-021057 [PubMed]
- 12. Arendt J. Melatonin: characteristics, concerns, and prospects. J Biol Rhythms. 2005; 20:291–303. https://doi.org/10.1177/0748730405277492 [PubMed]
- 13. Reiter RJ. The mammalian pineal gland: structure and function. Am J Anat. 1981; 162:287–313. https://doi.org/10.1002/aja.1001620402 [PubMed]
- 14. Nölte I, Lütkhoff AT, Stuck BA, Lemmer B, Schredl M, Findeisen P, Groden C. Pineal volume and circadian melatonin profile in healthy volunteers: an interdisciplinary approach. J Magn Reson Imaging. 2009; 30:499–505. https://doi.org/10.1002/jmri.21872 [PubMed]
- 15. Liebrich LS, Schredl M, Findeisen P, Groden C, Bumb JM, Nölte IS. Morphology and function: MR pineal volume and melatonin level in human saliva are correlated. J Magn Reson Imaging. 2014; 40:966–71. https://doi.org/10.1002/jmri.24449 [PubMed]
- 16. Sigurdardottir LG, Markt SC, Sigurdsson S, Aspelund T, Fall K, Schernhammer E, Rider JR, Launer L, Harris T, Stampfer MJ, Gudnason V, Czeisler CA, Lockley SW, et al. Pineal gland volume assessed by MRI and its correlation with 6-sulfatoxymelatonin levels among older men. J Biol Rhythms. 2016; 31:461–69. https://doi.org/10.1177/0748730416656948 [PubMed]
- 17. Wetterberg L, Iselius L, Lindsten J. Genetic regulation of melatonin excretion in urine. A preliminary report. Clin Genet. 1983; 24:399–402. https://doi.org/10.1111/j.1399-0004.1983.tb00093.x [PubMed]
- 18. Schmidt F, Penka B, Trauner M, Reinsperger L, Ranner G, Ebner F, Waldhauser F. Lack of pineal growth during childhood. J Clin Endocrinol Metab. 1995; 80:1221–25. https://doi.org/10.1210/jcem.80.4.7536203 [PubMed]
- 19. Tan DX, Xu B, Zhou X, Reiter RJ. Pineal Calcification, Melatonin Production, Aging, Associated Health Consequences and Rejuvenation of the Pineal Gland. Molecules. 2018; 23:301. https://doi.org/10.3390/molecules23020301 [PubMed]
- 20. Park J, Han JW, Lee JR, Byun S, Suh SW, Kim T, Yoon IY, Kim KW. Lifetime coffee consumption, pineal gland volume, and sleep quality in late life. Sleep. 2018; 41:zsy127. https://doi.org/10.1093/sleep/zsy127 [PubMed]
- 21. Gheban BA, Rosca IA, Crisan M. The morphological and functional characteristics of the pineal gland. Med Pharm Rep. 2019; 92:226–34. https://doi.org/10.15386/mpr-1235 [PubMed]
- 22. Mouret J, Coindet J, Chouvet G. [Effect of pinealectomy on sleep stages and rhythms of the male rat]. Brain Res. 1974; 81:97–105. https://doi.org/10.1016/0006-8993(74)90480-6 [PubMed]
- 23. Takeuchi N, Uchimura N, Hashizume Y, Mukai M, Etoh Y, Yamamoto K, Kotorii T, Ohshima H, Ohshima M, Maeda H. Melatonin therapy for REM sleep behavior disorder. Psychiatry Clin Neurosci. 2001; 55:267–69. https://doi.org/10.1046/j.1440-1819.2001.00854.x [PubMed]
- 24. Brooks PL, Peever JH. Impaired GABA and glycine transmission triggers cardinal features of rapid eye movement sleep behavior disorder in mice. J Neurosci. 2011; 31:7111–21. https://doi.org/10.1523/JNEUROSCI.0347-11.2011 [PubMed]
- 25. Videnovic A, Noble C, Reid KJ, Peng J, Turek FW, Marconi A, Rademaker AW, Simuni T, Zadikoff C, Zee PC. Circadian melatonin rhythm and excessive daytime sleepiness in Parkinson disease. JAMA Neurol. 2014; 71:463–69. https://doi.org/10.1001/jamaneurol.2013.6239 [PubMed]
- 26. Ono K, Mochizuki H, Ikeda T, Nihira T, Takasaki J, Teplow DB, Yamada M. Effect of melatonin on α-synuclein self-assembly and cytotoxicity. Neurobiol Aging. 2012; 33:2172–85. https://doi.org/10.1016/j.neurobiolaging.2011.10.015 [PubMed]
- 27. Pu Y, Mahankali S, Hou J, Li J, Lancaster JL, Gao JH, Appelbaum DE, Fox PT. High prevalence of pineal cysts in healthy adults demonstrated by high-resolution, noncontrast brain MR imaging. AJNR Am J Neuroradiol. 2007; 28:1706–09. https://doi.org/10.3174/ajnr.A0656 [PubMed]
- 28. McCarter SJ, St Louis EK, Sandness DJ, Arndt K, Erickson M, Tabatabai G, Boeve BF, Silber MH. Antidepressants increase REM sleep muscle tone in patients with and without REM sleep behavior disorder. Sleep. 2015; 38:907–17. https://doi.org/10.1016/j.sleep.2015.02.005 [PubMed]
- 29. Stiasny-Kolster K, Mayer G, Schäfer S, Möller JC, Heinzel-Gutenbrunner M, Oertel WH. The REM sleep behavior disorder screening questionnaire—a new diagnostic instrument. Mov Disord. 2007; 22:2386–93. https://doi.org/10.1002/mds.21740 [PubMed]
- 30. Bolitho SJ, Naismith SL, Terpening Z, Grunstein RR, Melehan K, Yee BJ, Coeytaux A, Gilat M, Lewis SJ. Investigating rapid eye movement sleep without atonia in Parkinson’s disease using the rapid eye movement sleep behavior disorder screening questionnaire. Mov Disord. 2014; 29:736–42. https://doi.org/10.1002/mds.25832 [PubMed]
- 31. Gaig C, Iranzo A, Pujol M, Perez H, Santamaria J. Periodic limb movements during sleep mimicking REM sleep behavior disorder: a new form of periodic limb movement disorder. Sleep. 2017; 40:zsw063. https://doi.org/10.1093/sleep/zsw063 [PubMed]
- 32. Iranzo A, Santamaría J. Severe obstructive sleep apnea/hypopnea mimicking REM sleep behavior disorder. Sleep. 2005; 28:203–06. https://doi.org/10.1093/sleep/28.2.203 [PubMed]
- 33. Mahlberg R, Kienast T, Hädel S, Heidenreich JO, Schmitz S, Kunz D. Degree of pineal calcification (DOC) is associated with polysomnographic sleep measures in primary insomnia patients. Sleep Med. 2009; 10:439–45. https://doi.org/10.1016/j.sleep.2008.05.003 [PubMed]
- 34. Han JW, Kim TH, Kwak KP, Kim K, Kim BJ, Kim SG, Kim JL, Kim TH, Moon SW, Park JY, Park JH, Byun S, Suh SW, et al. Overview of the Korean Longitudinal Study on Cognitive Aging and Dementia. Psychiatry Investig. 2018; 15:767–74. https://doi.org/10.30773/pi.2018.06.02 [PubMed]
- 35. Park JH, Lim S, Lim J, Kim K, Han M, Yoon IY, Kim J, Chang Y, Chang CB, Chin HJ. An overview of the Korean longitudinal study on health and aging. Psychiatry Investig. 2007; 4:84–95.
- 36. Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006; 239:650–64. https://doi.org/10.1148/radiol.2393050823 [PubMed]
- 37. Allen RP, Burchell BJ, MacDonald B, Hening WA, Earley CJ. Validation of the self-completed Cambridge-Hopkins questionnaire (CH-RLSq) for ascertainment of restless legs syndrome (RLS) in a population survey. Sleep Med. 2009; 10:1097–100. https://doi.org/10.1016/j.sleep.2008.10.007 [PubMed]
- 38. Chung F, Elsaid H. Screening for obstructive sleep apnea before surgery: why is it important? Curr Opin Anaesthesiol. 2009; 22:405–11. https://doi.org/10.1097/ACO.0b013e32832a96e2 [PubMed]
- 39. Lee JH, Lee KU, Lee DY, Kim KW, Jhoo JH, Kim JH, Lee KH, Kim SY, Han SH, Woo JI. Development of the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet (CERAD-K): clinical and neuropsychological assessment batteries. J Gerontol B Psychol Sci Soc Sci. 2002; 57:47–53. https://doi.org/10.1093/geronb/57.1.P47 [PubMed]
- 40. Yoo SW, Kim YS, Noh JS, Oh KS, Kim CH, NamKoong K, Chae JH, Lee GC, Jeon SI, Min KJ. Validity of Korean version of the mini-international neuropsychiatric interview. Anxiety Mood. 2006; 2:50–55.
- 41. Wechsler D. Instruction Manual for the Wechsler Memory Scale Revised. New York (NY): Psychological Corporation; 1987.
- 42. Kim TH, Huh Y, Choe JY, Jeong JW, Park JH, Lee SB, Lee JJ, Jhoo JH, Lee DY, Woo JI, Kim KW. Korean version of frontal assessment battery: psychometric properties and normative data. Dement Geriatr Cogn Disord. 2010; 29:363–70. https://doi.org/10.1159/000297523 [PubMed]
- 43. Kim JY, Park JH, Lee JJ, Huh Y, Lee SB, Han SK, Choi SW, Lee DY, Kim KW, Woo JI. Standardization of the korean version of the geriatric depression scale: reliability, validity, and factor structure. Psychiatry Investig. 2008; 5:232–38. https://doi.org/10.4306/pi.2008.5.4.232 [PubMed]
- 44. Miller MD, Paradis CF, Houck PR, Mazumdar S, Stack JA, Rifai AH, Mulsant B, Reynolds CF
3rd . Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992; 41:237–48. https://doi.org/10.1016/0165-1781(92)90005-N [PubMed] - 45. Lee DY, Lee KU, Lee JH, Kim KW, Jhoo JH, Kim SY, Yoon JC, Woo SI, Ha J, Woo JI. A normative study of the CERAD neuropsychological assessment battery in the Korean elderly. J Int Neuropsychol Soc. 2004; 10:72–81. https://doi.org/10.1017/S1355617704101094 [PubMed]
- 46. Kim JL, Park JH, Kim BJ, Kim MD, Kim SK, Chi YK, Kim TH, Moon SW, Park MH, Bae JN, Woo JI, Ryu SH, Yoon JC, et al. Interactive influences of demographics on the Mini-Mental State Examination (MMSE) and the demographics-adjusted norms for MMSE in elderly Koreans. Int Psychogeriatr. 2012; 24:642–50. https://doi.org/10.1017/S1041610211002456 [PubMed]
- 47. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th Edition, Text Revision. Washington (DC): American Psychiatric Association Press; 2000.
- 48. Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, Nordberg A, Bäckman L, Albert M, Almkvist O, Arai H, Basun H, Blennow K, et al. Mild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004; 256:240–46. https://doi.org/10.1111/j.1365-2796.2004.01380.x [PubMed]
- 49. Jinkins JR, Xiong L, Reiter RJ. The midline pineal “eye”: MR and CT characteristics of the pineal gland with and without benign cyst formation. J Pineal Res. 1995; 19:64–71. https://doi.org/10.1111/j.1600-079X.1995.tb00172.x [PubMed]
- 50. Youden WJ. Index for rating diagnostic tests. Cancer. 1950; 3:32–35. https://doi.org/10.1002/1097-0142(1950)3:1<32::AID-CNCR2820030106>3.0.CO;2-3 [PubMed]