



Introduction
In maintenance hemodialysis (HD) patients, renal anemia is generally treated with erythropoietic medications, including erythropoietin (EPO) and intravenous iron supplements. The introduction of EPOs has revolutionized the care of anemic patients with chronic kidney disease (CKD) and almost completely eradicated the severe anemia of end-stage renal disease (ESRD) patients. Moreover, EPOs decrease the need for recurrent blood transfusions and the risk of iron overload and may improve the patients’ quality of life. Today, EPOs and adjuvant iron therapy are the main treatments for anemia associated with CKD [1, 2].
Treatment of anemia with EPO was associated with improved neuropsychological test performance and electroencephalography measurements in uncontrolled studies of patients with ESRD conducted in the early 1990s [3, 4]. One study suggested that normalization of hemoglobin (Hb) using EPO was associated with further improvements in cognitive function [5], and other studies have suggested that EPO may exert neuroprotective effects independently of raising Hb levels [3, 4].
Due to its protective effects on cognitive function, EPO has been used in the treatment of neuropsychiatric disorders with cognitive impairments, including schizophrenia [6]. Given that the EPO receptor is widely expressed in the nervous system and that EPO easily crosses the intact blood–brain barrier [7], EPO supplementation is able to rescue cognitive decline in aged rats and restore impaired memory in vascular dementia (VaD) rat models [8, 9]. In addition, previous studies illustrated that EPO can attenuate hippocampal neuronal loss, neuroinflammation, and cholinergic deficit in rats [10], and can function as a neuroprotectant against amyloid beta (Aβ) toxicity [11, 12], which is a principal consideration for the development of treatments for Alzheimer’s disease (AD).
The data concerning the effects of EPO and intravenous iron supplementation on specific dementia subtypes among HD patients are scarce. Therefore, we conducted a total population-based retrospective cohort study to test whether EPO and intravenous iron supplementation correlate with the risk of various dementia subtypes including AD, VaD, and unspecified dementia (UnD) in HD patients.
Results
The demographic characteristics and comorbidities of the HD patients in our cohorts are shown in Table 1. We recruited 43,906 HD patients who took EPO and 11,676 HD patients who took iron during the study periods. Of these, 11,189 patients in the EPO cohort (25.5%) and 487 patients in the non-EPO cohort (1.1%) were administered iron therapy for anemia (Figure 1). The most frequent comorbidities were hypertension (88.9%), anemia (51.6%), diabetes mellitus (51.2%), and hyperlipidemia (41.9%). Less than 5% of the study population had a history of atrial fibrillation (AF), and nearly 53.9% were aged 60 years or older.
Table 1. Demographic characteristics and comorbidities of hemodialysis cohort in Taiwan.
| Variable | Total | Without EPO and iron | With EPO and without iron | With iron and without EPO | With EPO and iron | p-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| n | % | n | % | n | % | n | % | n | % | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | 43,906 | 5,789 | 26,441 | 487 | 11,189 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (yr) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (IQR) | 62.4 | (17.9) | 56.5 | (17.8) | 62.5 | (17.9) | 63.6 | (17.3) | 60.6 | (17.4) | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 41–50 | 8,336 | 19.0 | 840 | 14.5 | 4,934 | 18.7 | 79 | 16.2 | 2,483 | 22.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 51–60 | 11,914 | 27.1 | 1,333 | 23.0 | 7,202 | 27.2 | 122 | 25.1 | 3,257 | 29.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 61–70 | 12,437 | 28.3 | 1,711 | 29.6 | 7,453 | 28.2 | 154 | 31.6 | 3,119 | 27.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 71–80 | 8,898 | 20.3 | 1,466 | 25.3 | 5,431 | 20.5 | 102 | 20.9 | 1,899 | 17.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥81 | 2,321 | 5.29 | 439 | 7.58 | 1,421 | 5.37 | 30 | 6.16 | 431 | 3.85 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender | 0.4555 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 21,985 | 50.1 | 2,937 | 50.7 | 13,166 | 49.8 | 239 | 49.1 | 5,643 | 50.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 21,921 | 49.9 | 2,852 | 49.3 | 13,275 | 50.2 | 248 | 50.9 | 5,546 | 49.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Urbanization | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Urban | 24,142 | 55.0 | 3,111 | 53.7 | 14,291 | 54.1 | 360 | 73.9 | 6,380 | 57.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Suburban | 14,437 | 32.9 | 1,954 | 33.8 | 8,870 | 33.6 | 97 | 19.9 | 3,516 | 31.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Rural | 5,327 | 12.1 | 724 | 12.5 | 3,280 | 12.4 | 30 | 6.16 | 1,293 | 11.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Comorbidity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Coronary heart disease | 17,539 | 40.0 | 2,385 | 41.2 | 10,704 | 40.5 | 205 | 42.1 | 4,245 | 37.9 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 39,044 | 88.9 | 5,044 | 87.1 | 23,539 | 89.0 | 434 | 89.1 | 10,027 | 89.6 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes | 2,2465 | 51.2 | 3,180 | 54.9 | 13,480 | 51.0 | 270 | 55.4 | 5,535 | 49.5 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Atrial fibrillation | 618 | 1.41 | 89 | 1.54 | 382 | 1.44 | 7 | 1.44 | 140 | 1.25 | 0.4010 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart failure | 10,167 | 23.2 | 1,412 | 24.4 | 6,061 | 22.9 | 111 | 22.8 | 2,583 | 23.1 | 0.1197 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperlipidemia | 18,384 | 41.9 | 2,169 | 37.5 | 11,124 | 42.1 | 216 | 44.4 | 4,875 | 43.6 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anemia | 22,671 | 51.6 | 2,686 | 46.4 | 13,776 | 52.1 | 255 | 52.4 | 5,954 | 53.2 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Annual DDDs, median (IQR) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO (N=41,425) | 140.6 | (201.9) | 116.8 | (194.2) | 192.8 | (202.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Iron (N=13,020) | 8.60 | (14.5) | 6.64 | (11.1) | 8.70 | (14.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Days between index date and drug use, median (IQR) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO (N=41,425) | 8 | (69) | 11 | (119) | 5 | (25) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Iron (N=13,020) | 132 | (533.5) | 170 | (504) | 130 | (534) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Follow-up years, mean (SD) | 4.48 | (3.14) | 3.03 | (2.65) | 4.47 | (3.14) | 4.61 | (3.19) | 5.24 | (3.13) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dementia | 1,621 | 3.69 | 286 | 4.94 | 1,002 | 3.79 | 28 | 5.75 | 305 | 2.73 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| All-cause mortality | 19,154 | 43.6 | 3,274 | 56.6 | 11,556 | 43.7 | 217 | 44.6 | 4,107 | 36.7 | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SD, standard deviation; DDDs, defined daily doses; IQR, interquartile range; EPO, erythropoietin. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
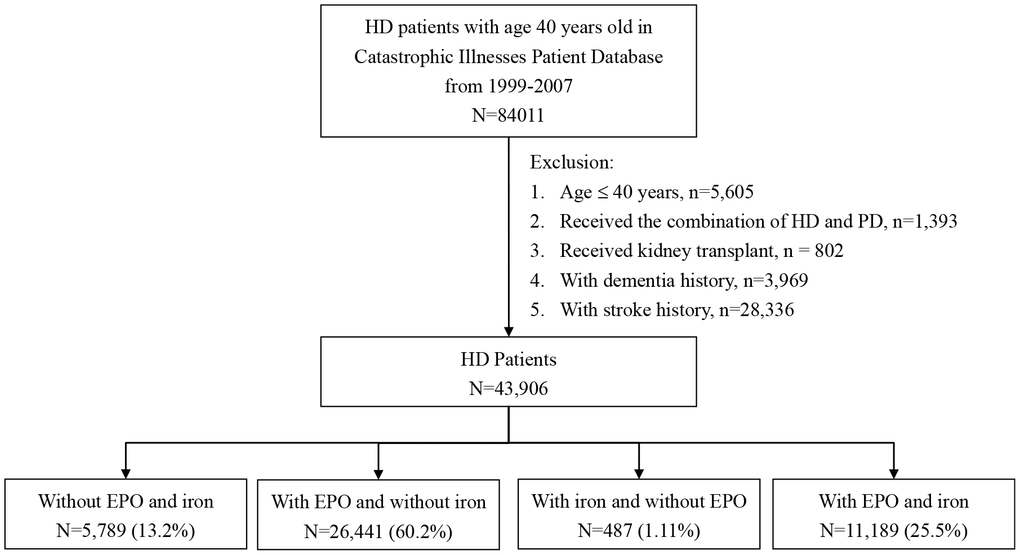
Figure 1. Flow chart for classification of study subjects.
Annual cumulative exposure to EPO and iron
Biosimilar EPOs can be discriminated from the endogenous protein by slight differences that may include posttranslational modification; consequently, they may be similar—but not identical—to the originator EPOs [13]. A previous population-based study indicated that EPO consumption by HD patients was similar for biosimilar and originator EPOs [14]. Defined daily dose (DDD) is the assumed average maintenance dose per day for a drug used for its main indication in adults [15]. To investigate the effect of dose, and to avoid higher cumulative EPO doses with longer patient follow-up periods, the cumulative use of EPOs was calculated as total prescribed annual DDDs (i.e., the same as total dispensed DDD under this system). Upon dementia diagnosis, the cumulative EPO dosage was recorded as the total of annual DDDs from drug initiation to the day before the diagnosis. Patients who took EPO at least once after the index date were defined as EPO users; the remaining patients were defined as non-EPO users. Similarly, patients who received intravenous iron at least once after the index date were defined as iron users; the remaining patients were defined as non-iron users. Upon dementia diagnosis, the cumulative iron dosage was recorded as the total annual DDDs from drug initiation to the day before the diagnosis.
Therefore, using the daily records of prescribed erythropoietic medications during the follow-up period, we categorized patients who had received erythropoietic medications as the treatment group and those who did not receive the drugs as the control group.
Factors associated with dementia incidence
The results of our analysis examining the association between the use of EPO or intravenous iron and the risk of developing dementia are shown in Table 2. Stratified Cox proportional hazard regressions showed that the hazard ratio (HR) for dementia in HD patients who took EPO within the follow-up period was 0.48 [95% confidence interval (CI) 0.42 to 0.54; p<0.0001] in comparison with the HD patients in the non-EPO cohort. We further analyzed the HR value after adjusting the data for diabetes, hyperlipidemia, hypertension, anemia, coronary artery disease, heart failure, and AF. The HR value obtained was 0.61 (95% CI 0.54-0.70; p<0.0001) in HD patients who took EPO.
Table 2. Incidence, hazard ratios and interaction (between EPO and intravenous iron) for dementia among hemodialysis cohort treated with EPO or intravenous iron.
| Treatment | N | Event | PY | Ratea | Crude HR (95% CI) | P | Adjusted HR (95% CI)b | P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO (annual DDDs) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 6,276 | 314 | 19,759 | 15.89 | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 37,630 | 1,307 | 176,901 | 7.39 | 0.48 (0.42-0.54) | <0.0001 | 0.61 (0.54-0.70) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Low (<71) | 12,369 | 443 | 56,935 | 7.78 | 0.50 (0.43-0.58) | <0.0001 | 0.72 (0.62-0.84) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (71-200) | 12,384 | 394 | 60,536 | 6.51 | 0.42 (0.39-0.49) | <0.0001 | 0.53 (0.46-0.62) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High (≥201) | 12,877 | 470 | 59,431 | 7.91 | 0.51 (0.44-0.59) | <0.0001 | 0.62 (0.54-0.72) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Iron (annual DDDs) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 32,230 | 1,288 | 135,836 | 9.48 | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 11,676 | 333 | 60,824 | 5.47 | 0.59 (0.52-0.66) | <0.0001 | 0.75 (0.65-0.86) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Low (<5) | 3,858 | 86 | 22,302 | 3.86 | 0.41 (0.33-0.52) | <0.0001 | 0.53 (0.41-0.70) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (5-13) | 3,913 | 96 | 19,314 | 4.97 | 0.53 (0.43-0.65) | <0.0001 | 0.61 (0.49-0.75) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High (≥14) | 3,905 | 151 | 19,208 | 7.86 | 0.84 (0.71-0.99) | 0.0388 | 0.98 (0.82-1.17) | 0.8213 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO | Iron | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | No | 5,789 | 286 | 17,514 | 16.33 | 1.00 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | No | 26,441 | 1,002 | 118,322 | 8.47 | 0.53 (0.47-0.61) | <0.0001 | 0.68 (0.59-0.78) | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Yes | 487 | 28 | 2,245 | 12.47 | 0.78 (0.53-1.15) | 0.2144 | 0.90 (0.60-1.34) | 0.5931 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | Yes | 11,189 | 305 | 58,579 | 5.21 | 0.33 (0.28-0.39) | <0.0001 | 0.49 (0.41-0.58) | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interaction P=0.26 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a Incidence rate, per 1000 person-years | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| b Adjusted for days between index date and drug use, age, gender, urbanization level, diabetes, hypertension, coronary heart disease, heart failure, atrial fibrillation, hyperlipidemia, and anemia. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO, erythropoietin; CI, confidence interval; HR, hazard ratio; DDDs, defined daily doses; PY, person-years. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Effects of EPO or iron intake on general risk of dementia
Table 2 also shows the association between the annual DDDs and the risk of dementia. Patients who exhibited higher annual DDDs of EPO exhibited a decreased risk of dementia (28%–47%). Analyzing the annual DDDs of EPO indicated that the low-, medium- and high-dose groups exhibited reduced dementia rates compared with the non-EPO cohort, suggesting a reduction of risk for annual various DDDs of EPO <200.
An additional analysis demonstrated an association between iron use and a reduced dementia risk (HR: 0.75; 95% CI, 0.65–0.86). In the analyses examining risks associated with different iron dosage, only low and medium doses of iron (<5 annual DDDs and 5–13 annual DDDs), but not high doses (≥14 annual DDDs), were associated with a reduced risk of dementia (39%–47%) in patients with HD using the non-iron cohort as a reference group.
Association between combined EPO and iron intake and general risk of dementia
The risk of incident dementia in relation to the combination of EPO and iron use was evaluated in HD patients, as compared with those who used neither drug (Table 2). The Cox proportional hazards model revealed that after adjusting for age, sex, and comorbidities, the risk of incident dementia was reduced both among HD patients who had received both EPO and iron (adjusted HR = 0.49, 95% CI, 0.41–0.58), and those who had used EPO but not iron (adjusted HR = 0.68, 95% CI, 0.59–0.78). In addition, HD patients using EPO and iron treatments experienced a delayed onset of dementia or prevented it altogether (log-rank test, p < 0.0001, Figure 2).
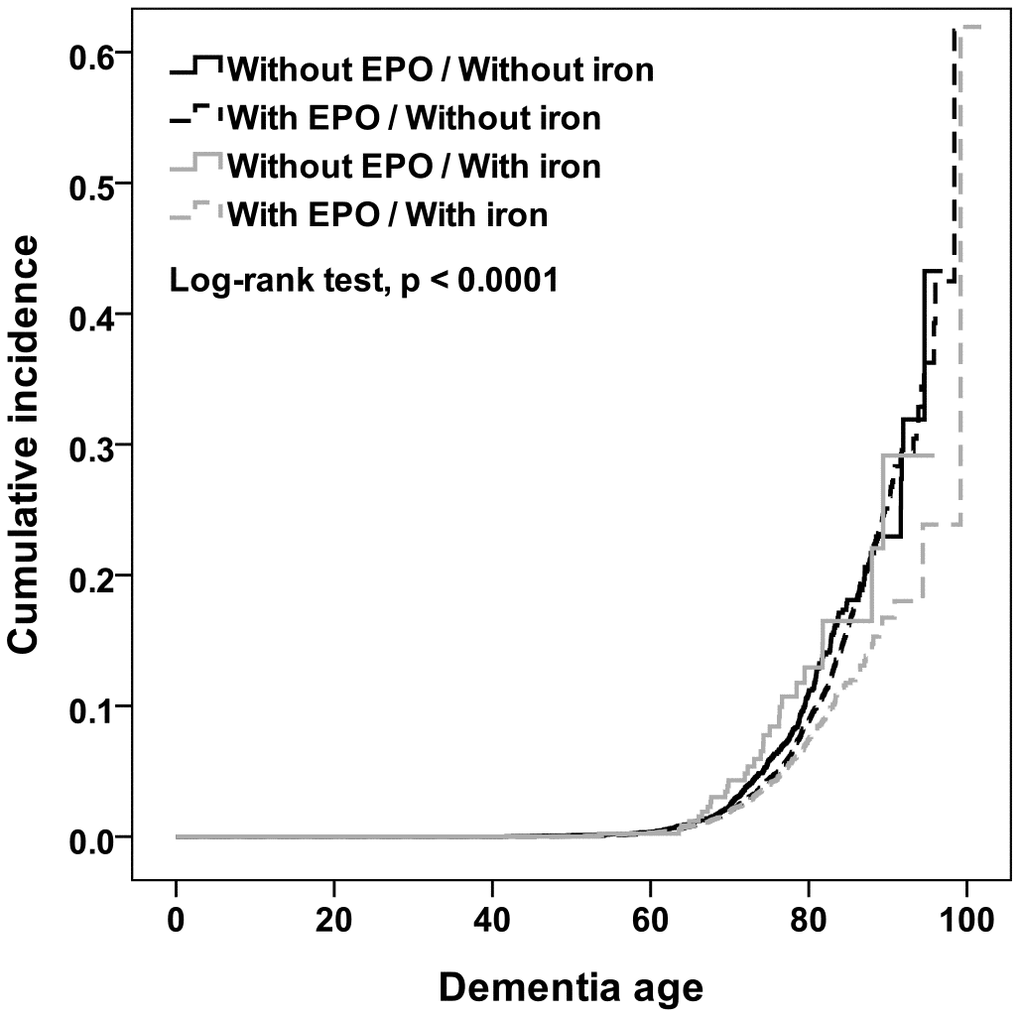
Figure 2. Plot of cumulative probability of dementia incidence depending on dementia age among cohort patients who underwent different EPO and iron treatments.
Association between EPO or iron intake and risk of dementia by dementia subtype
Table 3 shows the results of HR analysis for HD patient cohorts by dementia subtype. In comparison with non-EPO patients, HD patients treated with EPO were less likely to experience some subtypes of dementia during the follow-up period after the index healthcare use. Of note, the adjusted HRs for VaD and UnD in patients with HD were 0.44 (p<0.0001) and 0.65 (p<0.0001), respectively. Moreover, iron supplementation correlated with a reduced risk of UnD.
Table 3. Incidence, hazard ratios and interaction (between EPO and intravenous iron) for dementia subtypes among hemodialysis cohort treated with EPO or intravenous iron.
| Treatment | Alzheimer’s disease | Vascular dementia | Unspecified dementia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Event | Ratea | HR (95% CI)b | P | Event | Ratea | HR (95% CI)b | P | Event | Ratea | HR (95% CI)b | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO (annual DDDs) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| None | 10 | 0.51 | 1.00 | 46 | 2.33 | 1.00 | 358 | 13.06 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 36 | 0.20 | 0.65 (0.32–1.32) | 0.2277 | 148 | 0.84 | 0.44 (0.31–0.62) | <0.0001 | 1,123 | 6.35 | 0.65 (0.56–0.74) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Low (<71) | 7 | 0.12 | 0.48 (0.18–1.28) | 0.1410 | 53 | 0.93 | 0.53 (0.35–0.80) | 0.0027 | 383 | 6.73 | 0.77 (0.65–0.90) | 0.0016 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (71–200) | 16 | 0.26 | 0.82 (0.37–1.84) | 0.6349 | 39 | 0.64 | 0.34 (0.22–0.52) | <0.0001 | 339 | 5.60 | 0.56 (0.48–0.66) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High (≥201) | 13 | 0.22 | 0.60 (0.26–1.37) | 0.2214 | 56 | 0.94 | 0.49 (0.33–0.72) | 0.0003 | 401 | 6.75 | 0.65 (0.55–0.76) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Iron (annual DDDs) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| None | 34 | 0.25 | 1.00 | 152 | 1.12 | 1.00 | 1,102 | 8.11 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 12 | 0.20 | 0.84 (0.38–1.84) | 0.6561 | 42 | 0.69 | 0.78 (0.52–1.16) | 0.2112 | 279 | 4.59 | 0.74 (0.64–0.87) | 0.0002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Low (<5) | 3 | 0.13 | 0.44 (0.09–2.07) | 0.2994 | 14 | 0.63 | 0.81 (0.41–1.59) | 0.5426 | 69 | 3.09 | 0.50 (0.37–0.68) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (5–13) | 6 | 0.31 | 1.19 (0.46–3.07) | 0.7145 | 12 | 0.62 | 0.66 (0.39–1.21) | 0.1768 | 78 | 4.04 | 0.58 (0.45–0.74) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High (≥14) | 3 | 0.16 | 0.69 (0.21–2.30) | 0.5447 | 16 | 0.83 | 0.86 (0.51–1.46) | 0.5836 | 132 | 6.87 | 1.01 (0.84–1.21) | 0.9399 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO | Iron | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | No | 10 | 0.57 | 1.00 | 39 | 2.23 | 1.00 | 237 | 13.53 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | No | 24 | 0.20 | 0.58 (0.27–1.23) | 0.1552 | 113 | 0.96 | 0.52 (0.36–0.76) | 0.0006 | 865 | 7.31 | 0.71 (0.61–0.82) | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Yes | 0 | 0.00 | NA | 7 | 3.12 | 1.60 (0.69–3.70) | 0.2770 | 21 | 9.35 | 0.83 (0.52–1.31) | 0.4127 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | Yes | 12 | 0.20 | 0.48 (0.19–1.24) | 0.1303 | 35 | 0.60 | 0.39 (0.24–0.64) | 0.0002 | 258 | 4.40 | 0.50 (0.42–0.61) | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a Incidence rate, per 1000 person-years. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| b Adjusted for days between index date and drug use, age, gender, urbanization level, diabetes, hypertension, coronary heart disease, heart failure, atrial fibrillation, hyperlipidemia, and anemia. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPO, erythropoietin; CI, confidence interval; HR, hazard ratio; DDDs, defined daily doses; PY, person-years. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The interaction between EPO and iron were 0.98, 0.07, and 0.52 in crude model, and 0.98, 0.10, and 0.52 in adjusted model for Alzheimer’s disease, vascular dementia, and unspecified dementia. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Risk of dementia subtypes upon EPO or Iron supplementation
We estimated whether EPO supplementation correlated with reductions in risk for specific dementia subtypes based on the tertile of annual DDDs for EPO use. We observed a reduced risk of VaD (adjusted HR range from 0.34 to 0.53) and UnD (adjusted HR range from 0.56 to 0.77) among EPO users (Table 3).
Furthermore, the Cox proportional hazards model revealed a reduced risk of UnD among HD patients who underwent iron supplementation, adjusting for age, sex, and comorbidities (adjusted HR = 0.74, 95% CI, 0.64-0.87) (Table 3).
Effect of combined EPO and iron supplementation on risk of dementia by dementia subtype
Table 3 illustrates the combined effect of EPO and iron supplementation on dementia subtypes. Compared with patients who did not consume EPO nor iron, patients who consumed EPO only presented a reduced risk of VaD (adjusted HR =0.52, 95% CI, 0.36–0.76) and UnD (adjusted HR = 0.71, 95% CI, 0.61–0.82). Similarly, patients who received both EPO and iron supplements concomitantly also presented a reduced risk of VaD (adjusted HR = 0.39, 95% CI, 0.24–0.64) and UnD (adjusted HR = 0.50, 95% CI, 0.42–0.61), but not AD (adjusted HR = 0.48, 95% CI = 0.19–1.24).
Discussion
Our total population-based retrospective cohort study revealed that long-term administration of EPO to HD patients was inversely associated with their general risk of developing dementia as well as specific dementia subtypes, including VaD and UnD. In addition, we also observed a reduced risk of dementia in HD patients supplementing with intravenous iron. To our knowledge, no prior study has explored the association between EPO supplementation, intravenous iron supplementation, and the risk of dementia subtypes.
Here, after controlling for potential confounders, we found that EPO use of less than 71 annual DDDs, 71–200 annual DDDs, and over 201 annual DDDs in cumulative dose is associated with a 28%, 47%, and 38% risk reduction in dementia, respectively, as compared with not using EPO. However, we found no consistent trends in risk reduction with EPO supplementation of 201 annual DDDs or greater. This paradoxical phenomenon could be attributed to the severity of medical comorbidities, or to a partial response to EPO. For example, patients who used higher annual DDDs very likely had higher resistance to EPO [16] or more medical comorbidities that could cause a poorer response. Indeed, 10%–20% of CKD patients with anemia are resistant to EPOs [17]. Despite their potential for neuroprotection, EPOs might not be sufficient to overcome the adverse effects of severe resistance to EPO [18] or other medical comorbidities. Our study was restricted to analyzing data for HD patients, who already suffer from a high risk of developing dementia; therefore, our results may not be applicable to non-HD patients and further research is need to characterize the effects of EPO supplementation among the general population.
The neuroprotective mechanisms of EPOs include decreased neuronal apoptosis, decreased inflammation, promotion of oligodendrocyte differentiation and maturation, and improved white matter survival [19–22]. Two randomized, double-blind studies assessed the effect of EPO treatment on cognitive function [6, 23]. They showed that intravenously-administered EPO leads to better performance in healthy subjects in a test of verbal fluency seven days after treatment [6, 23] and that weekly intravenous injections of EPO lead to improved performance in tests of cognitive function in chronic schizophrenic patients. However, large randomized trials to treat anemia in CKD or ESRD patients with EPO supplementation did not evaluate cognitive function [24]. Thus, there is currently insufficient evidence to justify changing current hemoglobin targets to prevent dementia in patients with CKD or ESRD. To our knowledge, our results here are the first to suggest that EPO supplementation correlates with a reduced risk of dementia and dementia subtypes in HD patients, regardless of whether EPO was used alone or combined with iron. Through our present study, after controlling for potential confounders, we also found that iron supplementation of less than 5 annual DDDs and 5-13 annual DDDs in cumulative dose is associated with a 47% and 39% risk reduction in dementia, respectively, as compared with no use of iron. Although EPOs have become the mainstay of anemia therapy in HD patients, iron deficiency and/or insufficient iron bioavailability emerges as a major limiting factor in the effectiveness of these treatments. Therefore, we conducted a subgroup analysis to study the effect of concomitant EPO and iron supplementation. We observed an adjusted HR of 0.49 (95%CI, 0.41–0.58) when compared with the no-EPO and no-iron subgroups. For many HD patients, intravenous administration of iron is often a prerequisite to elicit an optimal response to EPO.
The strengths of this study are its population-based survey with a large sample size, with good follow-up throughout. However, several limitations and precautions are needed for interpreting our results. First, some anemic patients can be asymptomatic and thus might not visit the clinic thereby eluding diagnosis; therefore, the incidence of EPO use in the nonanemic controls was probably overestimated because of the presence of these asymptomatic patients. In addition, unlike a previous study conducted by Kuo KL et al., [25], which analyzed patient hemoglobin levels and medical records, the present study relied on anemia diagnoses by clinicians, which may be less sensitive and delayed. Second, our study was observational in nature and cannot prove causality. Although we adjusted for common health conditions, it’s possible that subclinical disease may also have contributed to cognitive decline. Third, hematological data such as ferritin and transferrin saturation (TSAT) were not available for us to consider them in the present study. Thus, it is not possible to evaluate whether iron was administered correctly or not. However, when it comes to prescribing EPOs to HD patients, physicians in Taiwan should follow the NHI reimbursement criteria to keep serum ferritin at levels >100 ng/mL and/or TSAT at levels > 20% during EPO therapy. We believe that the baseline iron parameters in our study might be in accordance with the NHI reimbursement criteria for all EPO users. Fourth, in the current study, the inclusion criteria of patients with dementia were strict, and only patients with at least three outpatient or inpatient claim records of dementia-related diagnosis codes were included; however, these criteria might still underestimate the number of patients with dementia, particularly among those who rarely visit hospitals or those diagnosed with dementia near the end of 2011. Fifth, patient hemoglobin or hematocrit levels were not available for us to consider them in the present study even though previous studies performed in Taiwan have shown that reasonable hemoglobin targets and favorable outcomes for CKD anemia can be achieved by intravenous iron supplementation [26–29]. Lastly, we did not analyze the effects of antihypertensive and oral hypoglycemic drugs, which may affect the progression of neurodegenerative diseases. Nonetheless, our study demonstrated a 47% risk reduction for developing dementia in HD patients who used EPO supplementation in the range of 71-200 annual DDDs. Moreover, our results suggest that intravenous iron supplementation correlates with lower risks of dementia in HD patients, especially in combination with EPO.
Methods
Data collection
A universal National Health Insurance (NHI) program was implemented in Taiwan in March 1995. Ninety-six percent of the Taiwanese population has been enrolled in this program [30]. By the end of 1996, the Bureau of NHI (BNHI) had contracts with 97% of all Taiwanese hospitals and clinics to join the national health insurance system [31]. The NHRI safeguards the privacy and confidentiality of all beneficiaries and provides health insurance data for research only after ethical approval has been obtained. In this study, access to the National Health Insurance Research Database (NHIRD) was approved by the Chia-Yi Christian Hospital local Institutional Review Board (approval no. CYCH-IRB-2018069). Further research in different independent study cohorts could further test the correlation we have uncovered between EPO use and reduced risk of dementia.
Study population
From the NHIRD database, we selected patients ≥ 40 years old who were beginning chronic HD treatment between January 1, 1999 and December 31, 2010 and who had survived more than 90 days of renal replacement therapy for ESRD (n=78,406). We excluded individuals younger than 40 years of age because their risk of dementia was negligible. ESRD patients are defined as those who had catastrophic illness registration cards for ESRD (International Classification of Diseases, 9th revision, Clinical Modification [ICD-9-CM code 585]) and have started renal replacement therapy [32, 33]. We excluded ESRD patients who received the combination of HD and peritoneal dialysis (PD) (n=1,393) or who had undergone kidney transplantation (n=802) as well as those who had been diagnosed with incident dementia before their index clinic visits (ICD-9-CM codes from 290.0 to 290.4, 294.1, and 331.0 to 331.2) (n=3,969) or with any type of stroke (codes 430-438) diagnosed before or within 90 days of their index clinic visits (n=28,336). Thus, in the end we included a total of 43,906 incident HD patients in this study. For all individuals in the cohort we obtained data on potential confounders, which are documented risk factors for dementia [33], including hypertension (codes 401-405), diabetes (code 250), hyperlipidemia (code 272), coronary heart disease (codes 410-414), AF (code 427.31), anemia (code 280-285), and other forms of heart disease (codes 420-429), recorded during 12 months before their index clinic visits. Each patient was individually tracked from their index clinic visits to the end of 2011 to identify those who subsequently suffered from incident dementia. The date of any form of dementia diagnosis made for the first time during the follow-up period or by the end of the study was considered the study endpoint. In our study, types of dementia other than AD and VaD were categorized as UnD, such as frontotemporal dementia (FTD), Parkinson’s dementia, and dementia with Lewy body (DLB) or dementia of unknown etiology. Therefore, we grouped patients into AD (ICD-9-CM code 331.0), VaD (ICD-9-CM code 290.4), and UnD (ICD-9-CM codes 290.0-290.3, 294.1, 331.1, and 331.2) dementia subtypes [34].
Statistical analysis
The primary endpoint of this study was to determine whether a patient had received ambulatory care visits or had hospitalizations for any type of dementia. We used Pearson’s χ2 test to compare EPO users and iron users with controls in terms of region of residence (urban, suburban, and rural) and selected comorbidities (hypertension, diabetes, hyperlipidemia, coronary heart disease, AF, anemia, and other forms of heart disease) at baseline. We considered these comorbidities only if the condition occurred in an inpatient setting or if there were two or more ambulatory care claims recorded one year before or after the index ambulatory care visit. EPO users and iron users were categorized into tertiles by annual DDDs to explore the potential effects on risk reduction. We measured dementia incidence using Kaplan-Meier analyses during the follow-up period for the HD patients with/without EPO or iron treatments.
The unadjusted HR along with the 95% CI was obtained by evaluating the association between HD patients with different drug usage and risk of dementia during the follow-up period using Cox proportional hazard regression. The adjusted HR was computed after adjusting for days between index date and drug use, age, gender, urbanization level, hypertension, diabetes, hyperlipidemia, coronary heart disease, AF, anemia, and heart failure. We further analyzed dementia incidence rates between cohorts according to dementia subtypes. All data analyses were conducted using the SAS (ver. 9.4) statistical package for Windows (SAS Institute, Cary, NC), and the significance level was set at 0.05 in a two-sided test.
Author Contributions
K.J.T., P.H.H., C.C.Y., and K.Y.H. designed research; C.C.Y., C.Y.H., F.C.S., and C.H.M. analyzed data; K.J.T. and P.H.H. wrote the first draft of the paper. All authors participated in the revision of the paper.
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health, Taiwan, and is managed by the National Health Research Institutes. The interpretations and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or the National Health Research Institutes. The authors would also like to acknowledge the support of Dr. Tsung-Hsien Chen in the preparation of this manuscript.
Conflicts of Interest
The authors declare that they have no competing interests.
Funding
This study was supported in part by the National Cheng Kung University, Taiwan Ministry of Health and Welfare Clinical Trial and the Research Center of Excellence (MOHW104-TDU-B-212-113002), China Medical University Hospital, the Academia Sinica Taiwan Biobank Stroke Biosignature Project (BM104010092), and the NRPB Stroke Clinical Trial Consortium (MOST103-2325-B-039 -006).
References
- 1. Hung SC, Tarng DC. ESA and iron therapy in chronic kidney disease: a balance between patient safety and hemoglobin target. Kidney Int. 2014; 86:676–78. https://doi.org/10.1038/ki.2014.179 [PubMed]
- 2. Hung SC, Lin YP, Tarng DC. Erythropoiesis-stimulating agents in chronic kidney disease: what have we learned in 25 years? J Formos Med Assoc. 2014; 113:3–10. https://doi.org/10.1016/j.jfma.2013.09.004 [PubMed]
- 3. Grimm G, Stockenhuber F, Schneeweiss B, Madl C, Zeitlhofer J, Schneider B. Improvement of brain function in hemodialysis patients treated with erythropoietin. Kidney Int. 1990; 38:480–86. https://doi.org/10.1038/ki.1990.229 [PubMed]
- 4. Marsh JT, Brown WS, Wolcott D, Carr CR, Harper R, Schweitzer SV, Nissenson AR. rHuEPO treatment improves brain and cognitive function of anemic dialysis patients. Kidney Int. 1991; 39:155–63. https://doi.org/10.1038/ki.1991.20 [PubMed]
- 5. Pickett JL, Theberge DC, Brown WS, Schweitzer SU, Nissenson AR. Normalizing hematocrit in dialysis patients improves brain function. Am J Kidney Dis. 1999; 33:1122–30. https://doi.org/10.1016/S0272-6386(99)70150-2 [PubMed]
- 6. Ehrenreich H, Hinze-Selch D, Stawicki S, Aust C, Knolle-Veentjer S, Wilms S, Heinz G, Erdag S, Jahn H, Degner D, Ritzen M, Mohr A, Wagner M, et al. Improvement of cognitive functions in chronic schizophrenic patients by recombinant human erythropoietin. Mol Psychiatry. 2007; 12:206–20. https://doi.org/10.1038/sj.mp.4001907 [PubMed]
- 7. Brines ML, Ghezzi P, Keenan S, Agnello D, de Lanerolle NC, Cerami C, Itri LM, Cerami A. Erythropoietin crosses the blood-brain barrier to protect against experimental brain injury. Proc Natl Acad Sci USA. 2000; 97:10526–31. https://doi.org/10.1073/pnas.97.19.10526 [PubMed]
- 8. Jia Z, Xue R, Ma S, Xu J, Guo S, Li S, Zhang E, Wang J, Yang J. Erythropoietin attenuates the memory deficits in aging rats by rescuing the oxidative stress and inflammation and promoting BDNF releasing. Mol Neurobiol. 2016; 53:5664–70. https://doi.org/10.1007/s12035-015-9438-1 [PubMed]
- 9. Ma S, Chen J, Chen C, Wei N, Xu J, Yang G, Wang N, Meng Y, Ren J, Xu Z. Erythropoietin Rescues Memory Impairment in a Rat Model of Chronic Cerebral Hypoperfusion via the EPO-R/JAK2/STAT5/PI3K/ Akt/GSK-3β Pathway. Mol Neurobiol. 2018; 55:3290–99. https://doi.org/10.1007/s12035-017-0568-5 [PubMed]
- 10. Cevik B, Solmaz V, Yigitturk G, Cavusoğlu T, Peker G, Erbas O. Neuroprotective effects of erythropoietin on Alzheimer’s dementia model in rats. Adv Clin Exp Med. 2017; 26:23–29. https://doi.org/10.17219/acem/61044 [PubMed]
- 11. Rodríguez Cruz Y, Strehaiano M, Rodríguez Obaya T, García Rodríguez JC, Maurice T. An Intranasal Formulation of Erythropoietin (Neuro-EPO) Prevents Memory Deficits and Amyloid Toxicity in the APPSwe Transgenic Mouse Model of Alzheimer’s Disease. J Alzheimers Dis. 2017; 55:231–48. https://doi.org/10.3233/JAD-160500 [PubMed]
- 12. Chong ZZ, Li F, Maiese K. Erythropoietin requires NF-kappaB and its nuclear translocation to prevent early and late apoptotic neuronal injury during beta-amyloid toxicity. Curr Neurovasc Res. 2005; 2:387–99. https://doi.org/10.2174/156720205774962683 [PubMed]
- 13. Jelkmann W. Efficacy of recombinant erythropoietins: is there unity of international units? Nephrol Dial Transplant. 2009; 24:1366–68. https://doi.org/10.1093/ndt/gfp058 [PubMed]
- 14. Hörbrand F, Bramlage P, Fischaleck J, Hasford J, Brunkhorst R. A population-based study comparing biosimilar versus originator erythropoiesis-stimulating agent consumption in 6,117 patients with renal anaemia. Eur J Clin Pharmacol. 2013; 69:929–36. https://doi.org/10.1007/s00228-012-1412-5 [PubMed]
- 15. World Health Organization Collaborating Centre for Drug Statistics Methodology. Defined daily dose: definition and general considerations. http://www.whocc.no/ddd/definition_and_general_considera/ (accessed 2017 May 30).
- 16. Bamgbola OF. Pattern of resistance to erythropoietin-stimulating agents in chronic kidney disease. Kidney Int. 2011; 80:464–74. https://doi.org/10.1038/ki.2011.179 [PubMed]
- 17. KDOQI, and National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Anemia in Chronic Kidney Disease. Am J Kidney Dis. 2006 (Suppl 3); 47:S11–145. https://doi.org/10.1053/j.ajkd.2006.03.010 [PubMed]
- 18. Icardi A, Paoletti E, De Nicola L, Mazzaferro S, Russo R, Cozzolino M. Renal anaemia and EPO hyporesponsiveness associated with vitamin D deficiency: the potential role of inflammation. Nephrol Dial Transplant. 2013; 28:1672–79. https://doi.org/10.1093/ndt/gft021 [PubMed]
- 19. Zhang L, Chopp M, Zhang RL, Wang L, Zhang J, Wang Y, Toh Y, Santra M, Lu M, Zhang ZG. Erythropoietin amplifies stroke-induced oligodendrogenesis in the rat. PLoS One. 2010; 5:e11016. https://doi.org/10.1371/journal.pone.0011016 [PubMed]
- 20. Chattopadhyay A, Choudhury TD, Bandyopadhyay D, Datta AG. Protective effect of erythropoietin on the oxidative damage of erythrocyte membrane by hydroxyl radical. Biochem Pharmacol. 2000; 59:419–25. https://doi.org/10.1016/S0006-2952(99)00277-4 [PubMed]
- 21. Vairano M, Dello Russo C, Pozzoli G, Battaglia A, Scambia G, Tringali G, Aloe-Spiriti MA, Preziosi P, Navarra P. Erythropoietin exerts anti-apoptotic effects on rat microglial cells in vitro. Eur J Neurosci. 2002; 16:584–92. https://doi.org/10.1046/j.1460-9568.2002.02125.x [PubMed]
- 22. Sugawa M, Sakurai Y, Ishikawa-Ieda Y, Suzuki H, Asou H. Effects of erythropoietin on glial cell development; oligodendrocyte maturation and astrocyte proliferation. Neurosci Res. 2002; 44:391–403. https://doi.org/10.1016/S0168-0102(02)00161-X [PubMed]
- 23. Miskowiak KW, Favaron E, Hafizi S, Inkster B, Goodwin GM, Cowen PJ, Harmer CJ. Erythropoietin modulates neural and cognitive processing of emotional information in biomarker models of antidepressant drug action in depressed patients. Psychopharmacology (Berl). 2010; 210:419–28. https://doi.org/10.1007/s00213-010-1842-7 [PubMed]
- 24. Kalantar-Zadeh K, Regidor DL, McAllister CJ, Michael B, Warnock DG. Time-dependent associations between iron and mortality in hemodialysis patients. J Am Soc Nephrol. 2005; 16:3070–80. https://doi.org/10.1681/ASN.2005040423 [PubMed]
- 25. Kuo KL, Hung SC, Tseng WC, Tsai MT, Liu JS, Lin MH, Hsu CC, Tarng DC, Ou SM, Yang CY, Lin YP, Lin YS, Hung SC, Hung TP, and Taiwan Society of Nephrology Renal Registry Data System. Association of Anemia and Iron Parameters With Mortality Among Patients Undergoing Prevalent Hemodialysis in Taiwan: the AIM - HD Study. J Am Heart Assoc. 2018; 7:e009206. https://doi.org/10.1161/JAHA.118.009206 [PubMed]
- 26. Tarng DC, Chen TW, Huang TP. Iron metabolism indices for early prediction of the response and resistance to erythropoietin therapy in maintenance hemodialysis patients. Am J Nephrol. 1995; 15:230–37. https://doi.org/10.1159/000168837 [PubMed]
- 27. Tarng DC, Huang TP, Chen TW. Mathematical approach for estimating iron needs in hemodialysis patients on erythropoietin therapy. Am J Nephrol. 1997; 17:158–64. https://doi.org/10.1159/000169091 [PubMed]
- 28. Tarng DC, Huang TP. Hyporesponsiveness to erythropoietin. Perit Dial Int. 1997; 17:99–100. [PubMed]
- 29. Tarng DC, Huang TP, Chen TW, Yang WC. Erythropoietin hyporesponsiveness: from iron deficiency to iron overload. Kidney Int Suppl. 1999; 69:S107–18. https://doi.org/10.1038/sj.ki.4490858 [PubMed]
- 30. Lu JF, Hsiao WC. Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood). 2003; 22:77–88. https://doi.org/10.1377/hlthaff.22.3.77 [PubMed]
- 31. Chiang TL. Taiwan’s 1995 health care reform. Health Policy. 1997; 39:225–39. https://doi.org/10.1016/S0168-8510(96)00877-9 [PubMed]
- 32. Lin HF, Li YH, Wang CH, Chou CL, Kuo DJ, Fang TC. Increased risk of cancer in chronic dialysis patients: a population-based cohort study in Taiwan. Nephrol Dial Transplant. 2012; 27:1585–90. https://doi.org/10.1093/ndt/gfr464 [PubMed]
- 33. Hung PH, Yeh CC, Hsiao CY, Sung PS, Muo CH, Sung FC, Hung KY, Tsai KJ. End stage renal disease is associated with development of dementia. Oncotarget. 2017; 8:107348–55. https://doi.org/10.18632/oncotarget.22458 [PubMed]
- 34. Lin CE, Chung CH, Chen LF, Chi MJ. Increased risk of dementia in patients with Schizophrenia: A population-based cohort study in Taiwan. Eur Psychiatry. 2018; 53:7–16. https://doi.org/10.1016/j.eurpsy.2018.05.005 [PubMed]