



Introduction
COPD is a common cause of death in the whole world [1], and the incidence of COPD continue to increase [2]. Respiratory tract infections are a common trigger of COPD exacerbations, and are associated with increased rates of morbidity and mortality. For COPD patients, inhaled corticosteroid (ICS) treatment is important maintenance therapy, and the combination of inhaled long-acting β2-agonists (LABAs) and ICSs can effectively reduce the risk of exacerbations among COPD patients [3–7]. In addition to the clinical benefits of ICSs, the use of ICSs can increase the risk of pneumonia – a common precursor of sepsis in patients with COPD [8–12]. Moreover, COPD patients with sepsis had a higher risk of severe exacerbations, pneumonia, and death compared to those without sepsis [22]. Despite most previous studies have focused on the association between ICSs and pneumonia or serious pneumonia, only a few have investigated the association between ICS treatment and the risk of sepsis [13]. In contrast to the significant association between ICS and the risk of pneumonia, one large-cohort study [13] using the administrative health databases showed that the risk of sepsis is not increased with ICS among patients treated for COPD. Therefore, the association between ICS used and sepsis risk remains unclear, and further study is warranted to clarify this issue.
Several studies [7, 14, 15] have evaluated differences between budesonide/formoterol and fluticasone/salmeterol. For example, Blais et al. found that budesonide/formoterol was associated with less COPD related emergency department visits and hospitalizations and fewer uses of anticholinergic medications than fluticasone/salmeterol [15]. In addition, Janson et al. reported higher rates of pneumonia and pneumonia-related mortality in fluticasone/salmeterol users than budesonide/formoterol users [7]. Further, Larsson et al. demonstrated that budesonide/formoterol was better than fluticasone/salmeterol in reducing the risk of exacerbations in COPD patients [14]. However, the relative risk of severe sepsis between patients with COPD receiving these two combinations is unknown. Therefore, we compared the effects of budesonide/formoterol and fluticasone/salmeterol on the sepsis risk in propensity score-matched COPD patients using data based on Taiwan National Health Insurance Research Database (NHIRD).
Results
Characteristics of the study population
Initially, a total of 17,111 patients had the diagnosis of COPD and received a fixed ICS/LABA combination (10,267 patients with fluticasone/salmeterol and 6,844 patients with budesonide/formoterol) were identified after excluding those with previous sepsis. Then, pairwise matching (1:1) resulted in two similar subgroups, with 6,688 patients in each (Figure 1). After propensity score matching, no significant difference was found between the patients who received fluticasone/salmeterol and those who received budesonide/formoterol for all covariates.
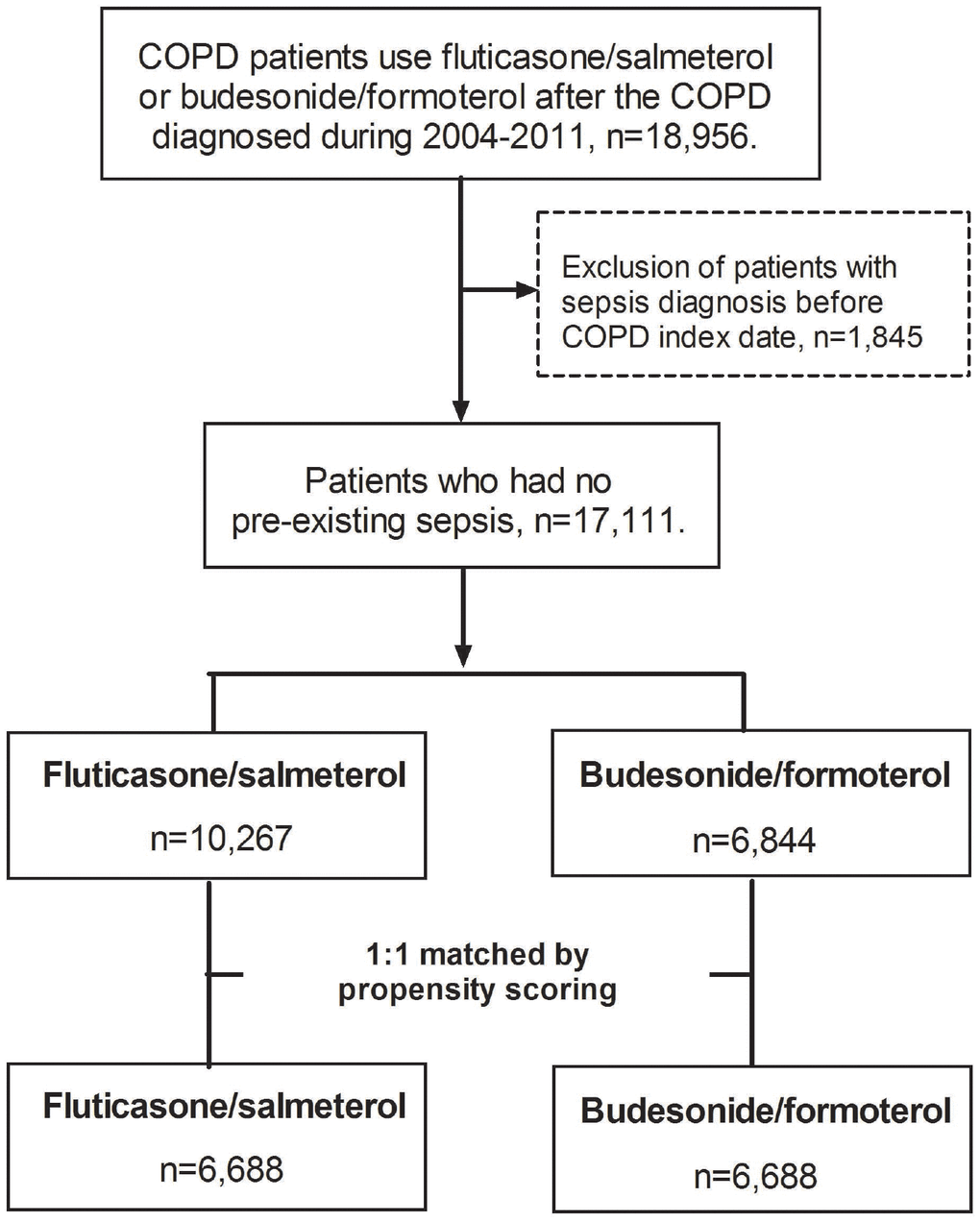
Figure 1. Flowchart of study cohort selection.
Risk of sepsis and death
Table 1 showed event rates of sepsis and mortality of COPD patients prescribed with fluticasone/salmeterol and budesonide/formoterol. During the follow-up period, the incidence of sepsis was 5.74 per 100 person-years for fluticasone/salmeterol group and 4.99 per 100 person-years for budesonide/formoterol group. Fluticasone/salmeterol was associated with a higher risk of sepsis (aHR, 1.15; 95% CI, 1.07-1.24), septic shock (aHR, 1.14; 95% CI, 1.01-1.29) and mortality (aHR, 1.09; 95% CI, 1.01-1.18), than budesonide/formoterol. Furthermore, the cumulative incidence of sepsis was higher among the patients receiving fluticasone/salmeterol than in those receiving budesonide/formoterol (p = 0.0001) (Figure 2). All these differences remained significant in the competing risk analysis (Table 2). Among as-treated analysis, fluticasone/salmeterol was associated with a higher risk of sepsis and death compared to budesonide/formoterol. In the competing risk analysis, the risk of sepsis was similar between the two groups, the patients receiving fluticasone/salmeterol had a trend of higher risk of sepsis than those receiving budesonide/formoterol.
Table 1. Incidences (per 100 person-years) and risk of sepsis and mortality among fluticasone/salmeterol and budesonide/formoterol.
| Fluticasone/salmeterol cohort | Budesonide/formoterol cohort | Crude HR (95%CI) | Adjustedb HR (95%CI) | Competing risk HR (95%CI) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| event | Person-year | IRa | event | Person-year | IRa | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mortality | 1242 | 27636.96 | 4.49 | 1151 | 27801.28 | 4.14 | 1.09 (1.00-1.18) | 1.09 (1.01-1.18) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sepsis | 1449 | 25229.12 | 5.74 | 1281 | 25685.67 | 4.99 | 1.15 (1.07-1.24) | 1.15 (1.07-1.24) | 1.13 (1.05-1.22) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Septic shock | 543 | 23103.66 | 2.35 | 488 | 23743.05 | 2.06 | 1.14 (1.01-1.29) | 1.14 (1.01-1.29) | 1.14 (1.01-1.28) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aIR, incidence rate, per 100 person-years. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| badjusted for propensity score. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
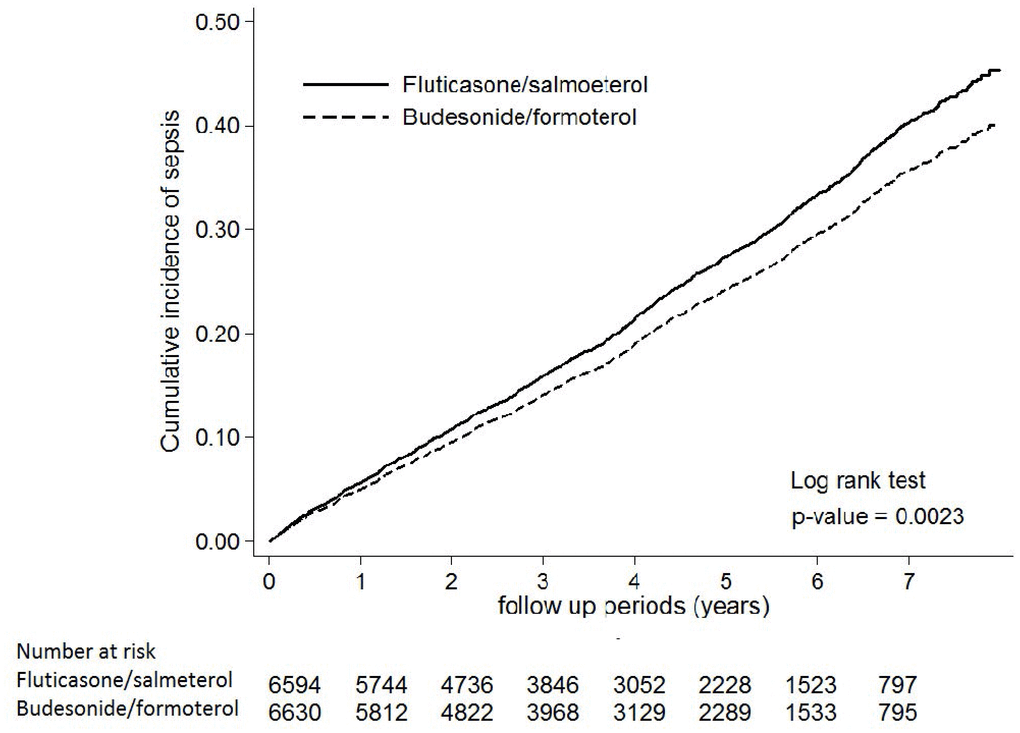
Figure 2. Cumulative incidence curve for sepsis in the patients prescribed with fluticasone/salmeterol and budesonide/formoterol. Times to events were compared using log-rank tests.
Table 2. Sensitivity analyses for risk of sepsis and mortality among fluticasone/salmeterol and budesonide/formoterol.
| Sensitivity analyses | Crude HR (95%CI) | Adjusteda HR (95%CI) |
| Primary analysis | ||
| Mortality | 1.086(1.002-1.176) | 1.090(1.006-1.181) |
| Sepsis | 1.150(1.067-1.240) | 1.153(1.069-1.243) |
| Septic shock | 1.143(1.012-1.292) | 1.143(1.012-1.292) |
| ITT analysis + competing risk | ||
| Mortality | - | - |
| Sepsis | 1.131(1.047-1.222) | |
| Septic shock | 1.136(1.005-1.284) | |
| As-treated analysis | ||
| Mortality | 1.237(1.095-1.398) | 1.227(1.086-1.387) |
| Sepsis | 1.177(1.048-1.321) | 1.173(1.045-1.317) |
| Septic shock | 1.208(1.01-1.445) | 1.201(1.004-1.437) |
| As-treated analysis + competing risk | ||
| Mortality | - | - |
| Sepsis | 1.118(0.988-1.266) | |
| Septic shock | 1.188(0.993-1.422) |
Discussion
In this study, the COPD patients receiving fluticasone/salmeterol had a higher risk of sepsis, septic shock and death than those receiving budesonide/formoterol. Similar trends were obtained using intention-to-treat and as-treated analyses with or without competing risk analysis. Moreover, using fluticasone/salmeterol was associated with higher risk of sepsis-related organ dysfunction, and most types of infections than budesonide/formoterol. A cohort study in Italy [16] reported that the incidence of hospitalization, oral corticosteroid use, and antibiotic use was lower for budesonide/formoterol compared to fluticasone/salmeterol. Another retrospective claims-based study from major U.S. health plans [17] reported that COPD patients receiving budesonide/formoterol treatment had lower average COPD-related, pneumonia-related, and all-cause costs compared to those receiving fluticasone/salmeterol treatment. In addition, the PATHOS study reported that budesonide/formoterol was associated with the lower rate of COPD-related hospitalization, and shorter hospital stay for exacerbations compared with fluticasone/salmeterol. In contrast, fluticasone/salmeterol was associated with higher risk of pneumonia and more pneumonia-related hospital admissions compared to the budesonide/formoterol group [7, 14]. Taken together, these findings may suggest that budesonide/formoterol treatment is associated with fewer adverse effects compared with fluticasone/salmeterol treatment. By this study, our findings add to the growing evidence of significant differences between fluticasone/salmeterol and budesonide/formoterol in terms of adverse effects in patients with COPD.
The following differences between budesonide/formoterol and fluticasone/salmeterol can support our findings. Budesonide and fluticasone differ in their pharmacokinetic properties, and the rates of uptake and elimination are slower for fluticasone [18]. In addition, the mean residence time in the systemic circulation has been reported to be shorter for budesonide than for fluticasone (4.41 hours versus 12.78 hours, respectively), and the quantity of expectorated fluticasone has been reported to be significantly higher compared to budesonide (ratio 5.21; P = 0.006) [20]. Fluticasone has been reported to be approximately 10 times more potent than budesonide in inhibiting the release of IL-6, IL-8, and TNF-α production from human alveolar macrophages [20]. In summary, all these differences can make fluticasone retention longer in the airway and exhibit greater immunosuppressive effect than budesonide, and thereby fluticasone can be associated with higher risk of bacterial colonization and infection-associated exacerbations than budensonide [18–20]. Other than the pharmacokinetic differences between budesonide and fluticasone, their differences in individual dosage might be related the risk of sepsis. Based on the findings of the study [22] investigating the association between ICS and risk of serious pneumonia, the risk was twofold with fluticasone (RR 2.01; 95% CI 1.93 to 2.10), and the risk was increasing with the daily dose. In contrast, the risk of serious pneumonia was only 1.17 with budesonide (95% CI 1.09 to 1.26), and the dose-response relationship was not as evident as fluticasone. Moreover, this study [22] also demonstrated that the effect of ICS on the risk of pneumonia would peak in the first year of use and remains elevated and stable even up to 5 years of continuous use.
This study has the major strength. A large COPD cohort in a real world was enrolled in this study and the effect of many confounding factor were minimized. Thus, our results could reveal the status of COPD patients in Taiwan and could be generalized to other sites.
This study has several limitations. First, the result of pulmonary function test results was not available, so the severity of COPD was not determined. Second, although many confounding factors was collected and adjusted in this study, it is still possible that residual confounding factors were exists.
In summary, long-term treatment with budesonide/formoterol was associated with lower rates of sepsis, septic shock and death than fluticasone/salmeterol in COPD patients. Clinicians should keep alert higher risk of sepsis and death among COPD patients receiving fluticasone/salmeterol than budesonide/formoterol.
Methods
Patients
A subset of the NHIRD including data on 2,200,000 COPD patient was used for this study. This population was followed between 2004 and 2011. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 491, 492, and 496 were used to identify patients with COPD. Only patients with at least three outpatient or inpatient visits for COPD and those aged between 40 and 100 years were included. We defined the index date as the date of the first fixed prescription for a combination of ICSs/LABAs for COPD. The patients were followed from 1 January 2004 to the either one of the following outcomes, including the end of the study (31 December 2011), emigration or mortality. Ethical approval was obtained from the Institutional Review Board (No. CTH-104-3-5-030).
Outcome measurements
The primary outcome was sepsis, which was defined using ICD-9-CM codes as previously reported.16 Only the first episode of sepsis was included but those with previous sepsis were excluded. The secondary outcome was all-cause mortality. Moreover, the source of infection, and organ dysfunction were recorded as previous reported, [23] Sepsis patients received sympathomimetic or vasopressin were defined as septic shock.
Exposure measures and potential confounders
Comorbidity data were retrieved according to ICD-9-CM codes and the severity of the comorbidities was assessed using Charlson Comorbidity Index (CCI). Concomitant medications, particularly medications for COPD (LABAs, short-acting β2-agonists (SABAs), long-acting muscarinic antagonists (LAMAs), and ICSs), were recorded. Fixed ICS/LABA combinations were defined as ATC codes R03AK06 or R03AK07. COPD exacerbations were only recorded during the period when the ICS/LABA combinations were prescribed.
Statistical analysis
Propensity score method was generated for the likelihood of fluticasone/salmeterol use (with budesonide/formoterol use as reference group). A logistic regression with covariates of index year, age, sex, monthly income, hospital level, the number of outpatient visits, the use of concomitant medication, and underlying comorbidities (Supplementary Table 1) was used to compute the propensity scores. We used cox regression models to assess the crude and adjusted hazard ratios (HRs) of the outcomes in the two groups for propensity scores (continuous). The budesonide/formoterol group was used as the reference group. The crude incidence of sepsis was defined as the total episodes of events divided by the person-years.
This study used intention-to-treat analysis as the primary analysis. In the as-treated analysis, the patients were censored when they switched to another ICS/LABA and when they out of the study. We used Kaplan-Meier method to construct cumulative incidence curves.
We used SAS software version 9.4 (SAS Institute Inc., Cary, NC) for data analysis. A two-sided P value < 0.05 indicated statistical significance in all analyses.
Supplementary Materials
Acknowledgments
Taiwan Clinical Trial Consortium for Respiratory Diseases (TCORE) includes Chong-Jen Yu, MD, PhD, (NTUH, Director of Coordinating Center and Core PI of Committee); Hao-Chien Wang, MD, PhD (NTUH, PI of Committee), Diahn-Warng Perng, MD, PhD (Taipei Veterans General Hospital, PI of Committee), Shih-Lung Cheng, MD, PhD (Far Eastern Memorial Hospital, PI of Committee), Jeng-Yuan Hsu, MD, PhD (Taichung Veterans General Hospital, PI of Committee), Wu-Huei Hsu, MD, PhD (China Medical University Hospital, PI of Committee), Ying-Huang Tsai, MD, PhD (Chang Gung Memorial Hospital, Chia-Yi, PI of Committee), Tzuen-Ren Hsiue, MD, PhD (National Cheng Kung University Hospital, PI of Committee), Meng-Chih Lin, MD, PhD (Chang Gung Memorial Hospital, Kaohsiung, PI of Committee), Hen-I Lin, MD (Cardinal Tien Hospital, PI of Committee), Cheng-Yi Wang, MD, PhD (Cardinal Tien Hospital, PI of Committee), Yeun-Chung Chang, MD, PhD (NTUH, PI of Committee), Ueng-Cheng Yang, PhD (National Yang-Ming University, PI of Committee), Chung-Ming Chen, PhD (NTUH, PI of Committee), Cing-Syong Lin, MD, PhD (Changhua Christian Hospital, PI of Committee), Likwang Chen, PhD (National Health Research Institutes, PI of Committee), Yu-Feng Wei, MD (E-Da Hospital, PI of Committee), Inn-Wen Chong, MD (Kaohsiung Medical University Chung-Ho Memorial Hospital, PI of Committee), Chung-Yu Chen(NTUH, Yun-Lin, PI of Committee).
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
This work was supported by Taiwan National Science Foundation grants NSC 101-2325-B-002-064, NSC 102-2325-B-002-087, NSC 103-2325-B-002-027, NSC 104-2325-B-002-035, and NSC-105), Cardinal Tien Hospital (CTH105A-205, CTH106A-2B05, CTH107A-2A13, and CTH108A-2A14) and from National Health Research Institutes (intramural funding).
References
- 1. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380:2095–128. https://doi.org/10.1016/S0140-6736(12)61728-0 [PubMed]
- 2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006; 3:e442. https://doi.org/10.1371/journal.pmed.0030442 [PubMed]
- 3. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J, and TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007; 356:775–89. https://doi.org/10.1056/NEJMoa063070 [PubMed]
- 4. Calverley P, Pauwels R, Vestbo J, Jones P, Pride N, Gulsvik A, Anderson J, Maden C, and TRial of Inhaled STeroids ANd long-acting beta2 agonists study group. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2003; 361:449–56. https://doi.org/10.1016/S0140-6736(03)12459-2 [PubMed]
- 5. Calverley PM, Boonsawat W, Cseke Z, Zhong N, Peterson S, Olsson H. Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur Respir J. 2003; 22:912–19. https://doi.org/10.1183/09031936.03.00027003 [PubMed]
- 6. Szafranski W, Cukier A, Ramirez A, Menga G, Sansores R, Nahabedian S, Peterson S, Olsson H. Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary disease. Eur Respir J. 2003; 21:74–81. https://doi.org/10.1183/09031936.03.00031402 [PubMed]
- 7. Janson C, Larsson K, Lisspers KH, Ställberg B, Stratelis G, Goike H, Jörgensen L, Johansson G. Pneumonia and pneumonia related mortality in patients with COPD treated with fixed combinations of inhaled corticosteroid and long acting β2 agonist: observational matched cohort study (PATHOS). BMJ. 2013; 346:f3306. https://doi.org/10.1136/bmj.f3306 [PubMed]
- 8. Ernst P, Gonzalez AV, Brassard P, Suissa S. Inhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumonia. Am J Respir Crit Care Med. 2007; 176:162–66. https://doi.org/10.1164/rccm.200611-1630OC [PubMed]
- 9. Joo MJ, Au DH, Fitzgibbon ML, Lee TA. Inhaled corticosteroids and risk of pneumonia in newly diagnosed COPD. Respir Med. 2010; 104:246–52. https://doi.org/10.1016/j.rmed.2009.10.002 [PubMed]
- 10. Thornton Snider J, Luna Y, Wong KS, Zhang J, Chen SS, Gless PJ, Goldman DP. Inhaled corticosteroids and the risk of pneumonia in Medicare patients with COPD. Curr Med Res Opin. 2012; 28:1959–67. https://doi.org/10.1185/03007995.2012.743459 [PubMed]
- 11. Yawn BP, Li Y, Tian H, Zhang J, Arcona S, Kahler KH. Inhaled corticosteroid use in patients with chronic obstructive pulmonary disease and the risk of pneumonia: a retrospective claims data analysis. Int J Chron Obstruct Pulmon Dis. 2013; 8:295–304. https://doi.org/10.2147/COPD.S42366 [PubMed]
- 12. Wang CY, Lai CC, Yang WC, Lin CC, Chen L, Wang HC, Yu CJ. The association between inhaled corticosteroid and pneumonia in COPD patients: the improvement of patients’ life quality with COPD in Taiwan (IMPACT) study. Int J Chron Obstruct Pulmon Dis. 2016; 11:2775–83. https://doi.org/10.2147/COPD.S116750 [PubMed]
- 13. Ernst P, Coulombe J, Brassard P, Suissa S. The Risk of Sepsis with Inhaled and Oral Corticosteroids in Patients with COPD. COPD. 2017; 14:137–142. https://doi.org/10.1080/15412555.2016.1238450 [PubMed]
- 14. Larsson K, Janson C, Lisspers K, Jørgensen L, Stratelis G, Telg G, Ställberg B, Johansson G. Combination of budesonide/formoterol more effective than fluticasone/salmeterol in preventing exacerbations in chronic obstructive pulmonary disease: the PATHOS study. J Intern Med. 2013; 273:584–94. https://doi.org/10.1111/joim.12067 [PubMed]
- 15. Blais L, Forget A, Ramachandran S. Relative effectiveness of budesonide/formoterol and fluticasone propionate/salmeterol in a 1-year, population-based, matched cohort study of patients with chronic obstructive pulmonary disease (COPD): effect on COPD-related exacerbations, emergency department visits and hospitalizations, medication utilization, and treatment adherence. Clin Ther. 2010; 32:1320–28. https://doi.org/10.1016/j.clinthera.2010.06.022 [PubMed]
- 16. Perrone V, Sangiorgi D, Buda S, Degli Esposti L. Comparative analysis of budesonide/formoterol and fluticasone/salmeterol combinations in COPD patients: findings from a real-world analysis in an Italian setting. Int J Chron Obstruct Pulmon Dis. 2016; 11:2749–55. https://doi.org/10.2147/COPD.S114554 [PubMed]
- 17. Davis JR, Kern DM, Williams SA, Tunceli O, Wu B, Hollis S, Strange C, Trudo F. Health care utilization and costs after initiating budesonide/formoterol combination or fluticasone/salmeterol combination among COPD patients new to ICS/LABA treatment. J Manag Care Spec Pharm. 2016; 22:293–304. https://doi.org/10.18553/jmcp.2016.22.3.293 [PubMed]
- 18. Thorsson L, Edsbäcker S, Källén A, Löfdahl CG. Pharmacokinetics and systemic activity of fluticasone via Diskus and pMDI, and of budesonide via Turbuhaler. Br J Clin Pharmacol. 2001; 52:529–38. https://doi.org/10.1046/j.0306-5251.2001.01493.x [PubMed]
- 19. Dalby C, Polanowski T, Larsson T, Borgström L, Edsbäcker S, Harrison TW. The bioavailability and airway clearance of the steroid component of budesonide/formoterol and salmeterol/fluticasone after inhaled administration in patients with COPD and healthy subjects: a randomized controlled trial. Respir Res. 2009; 10:104. https://doi.org/10.1186/1465-9921-10-104 [PubMed]
- 20. Ek A, Larsson K, Siljerud S, Palmberg L. Fluticasone and budesonide inhibit cytokine release in human lung epithelial cells and alveolar macrophages. Allergy. 1999; 54:691–99. https://doi.org/10.1034/j.1398-9995.1999.00087.x [PubMed]
- 21. Chen CH, Lai CC, Wang YH, Wang CY, Wang HC, Yu CJ, Chen L, and Taiwan Clinical Trial Consortium for Respiratory Diseases (TCORE). The Impact of Sepsis on the Outcomes of COPD Patients: A Population-Based Cohort Study. J Clin Med. 2018; 7:E393. https://doi.org/10.3390/jcm7110393 [PubMed]
- 22. Suissa S, Patenaude V, Lapi F, Ernst P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013; 68:1029–36. https://doi.org/10.1136/thoraxjnl-2012-202872 [PubMed]
- 23. Lai CC, Wang YH, Wang CY, Wang HC, Yu CJ, Chen L, and on the behalf of Taiwan Clinical Trial Consortium for Respiratory Diseases (TCORE). Risk of sepsis and mortality among patients with chronic obstructive pulmonary disease treated with angiotensin-Converting enzyme inhibitors or angiotensin receptor bockers. Crit Care Med. 2019; 47:e14–20. https://doi.org/10.1097/CCM.0000000000003475 [PubMed]