



Introduction
Myocardial infarction (MI) is accompanied by a mechanical deformation of cardiomyocytes, which can be adaptive and maladaptive, leading to chronic heart failure [1]. Currently, myocardial remodelling is considered a complex multistage process, in which the structural and geometric characteristics of left ventricle (LV) are altered and it is manifested as a hypertrophy and dilatation of cardiac chambers with the development of systolic and diastolic dysfunction [2]. A traditionally used indicator of cardiomyocyte stretching and the development and progression of chronic heart failure is N-terminal pro b-type natriuretic peptide (NT-proBNP) [3,4]. However, its application is limited by its biological variations, and its dependence on gender, age and body mass index. NT-proBNP levels in the serum of patients may vary depending on other pathologies as well, such as infections or kidney diseases [4].
Growth-stimulating factor ST2 may represent a more promising marker of early cardiac remodelling, and it is expressed on cardiomyocytes as a response to an increase in biomechanical stress [5]. ST2 is a member of interleukine-1 (IL-1) family receptors [6], and it plays a role in the activation of IL-33, which has antihypertrophic and antifibrotic effects on cardiomyocytes during biomechanical stress. However, an excessive increase in serum ST2 levels is accompanied by the inhibition of the antihypertrophic effects of IL-33 [7]. Therefore, the elucidation of ST2 role and the changes in its levels during the hospitalization of patients suffering from MI may be helpful in predicting the development of LV remodelling and chronic heart failure in postinfarction period.
In this study, we aimed to determine ST2 and NT-proBNP contents in the sera of MI patients during their hospitalization and the potential correlation between the levels of these markers and the development of adaptive or maladaptive variants of cardiac remodelling.
Results
Echocardiographic parameters and postinfarction remodelling variant
Patients were divided into two groups according to the variant of postinfarction remodelling. The results of echocardiographic examination are presented in Table 1. Patients with maladaptive remodelling were shown to be characterized by a more severe impairment of systolic and diastolic cardiac function. An increase in the linear dimensions of LV chamber was indicated. Therefore, EDD, ESD, EDV and ESV values were 1.2, 1.3, 1.2 and 1.6 folds, respectively, higher in patients with maladaptive cardiac remodelling, compared with those in patients with adaptive cardiac remodelling.
Table 1. Structural and functional myocardial parameters in patients with ST-elevated myocardial infraction, according to the postinfarction remodelling variant.
| Variable | Control, n= 30 Мe (Q1;Q3) | Patients with adaptive cardiac remodelling n=67 Мe (Q1;Q3) | Patients with maladaptive cardiac remodelling n=20 Мe (Q1;Q3) | Р | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ejection fraction (%) | 60.5 (60.0;62.0) | 52.0 (48.0; 59.0) | 43.0 (35.0; 45.0) | Р1-2=0.022 Р2-3=0.013 Р1-3=0.016 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| End-diastolic dimension (сm) | 5.2 (5.025;5.3) | 5.4 (5.2; 5.8) | 6.1 (5.9; 6.4) | Р1-2=0.231 Р2-3=0.029 P1-3=0.023 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| End-systolic dimension (сm) | 3.5 (3.4;3.6) | 3.9 (3.6; 4.3) | 5.0 (4.4; 5.2) | Р1-2=0.342 Р2-3=0.026 P1-3=0.021 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| End-diastolic volume (mL) | 130.0 (121.5;135.0) | 147.0 (132.5; 169.0) | 176.5 (171.0; 209.0) | Р1-2=0.187 Р2-3=0.031 P1-3=0.031 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| End-systolic volume (mL) | 52.0 (47.0;54.0) | 68.0 (58.0; 83.5) | 109.5 (88.0; 124.0) | Р1-2=0.025 Р2-3=0.032 P1-3=0.011 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left atrial (cm) | 3.95 (3.8;4.0) | 4.1 (3.8; 4.3) | 4,6 (4.0; 4.7) | Р1-2=0.411 Р2-3=0.035 P1-3=0.421 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right atrial (cm) | 3.95 (3.8;4.0) | 4.0 (3.8; 4.4) | 3.9 (3.7; 4.5) | Р1-2=0.309 Р2-3=0.267 P1-3=0.341 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right ventricle (cm) | 1.8 (1.7;2.0) | 1.8 (1.8; 1.8) | 1.8 (1.8; 2.0) | Р1-2=0.169 Р2-3=0.277 P1-3=0.211 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interventricular septum (сm) | 1.0 (1.0;1.1) | 1.1 (1.0; 1.2) | 1.10 (1.1; 1.2) | Р1-2=0.248 Р2-3=0.041 P1-3=0.029 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LV posterior wall dimension (cm) | 1.0 (0.9;1.0) | 1.1 (1.0; 1.2) | 1.1 (1.1; 1.3) | Р1-2=0.038 Р2-3=0.022 P1-3=0.137 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Myocardial weight (g) | 224,5 (212,4;244.5) | 277.2 (239.9; 289.8) | 318.9 (290.5; 378.1) | Р1-2=0.111 Р2-3=0.078 P1-3=0.027 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Е (cm/с) | 68.0 (64.25;70.75) | 56.0 (47.0; 66.0) | 46.0 (44.0; 54.0) | Р1-2=0.255 Р2-3=0.032 P1-3=0.087 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| А (сm/с) | 62.0 (56.25;67.75) | 68.5 (57.0; 80.0) | 65.0 (50.0; 70.50) | Р1-2=0.207 Р2-3=0.318 P1-3=0.133 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Е/А | 1.12 (1.07;1.22) | 0.7 (0.6; 0.9) | 0.7 (0.7; 1.4) | Р1-2=0.115 Р2-3=0.143 P1-3=0.099 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulmonary artery pressure (mm Hg) | 21.0(19.25;23.0) | 25.0 (20.0;28.0) | 29.5 (24.0;38.5) | Р1-2=0.023 Р2-3=0.033 P1-3=0.251 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LV: left ventricular; E: wave of early diastolic filling, A: atrial wave of active filling | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
LVEF in the maladaptive remodelling group, estimated using the Simpson method, was shown to be 1.2-fold lower than that in the adaptive remodelling group (Table 2) [9]. A decrease in the Е/А ratio was observed in the patients belonging to both remodelling variant groups.
Table 2. Baseline clinical and anamnestic characteristics of patients, according to the postinfarction left ventricular remodelling variant Мe (Q1;Q3).
| Variable | Patients with adaptive cardiac remodelling n=67 | Patients with maladaptive cardiac remodelling n=20 | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Men | 49 (73.1%) | 16 (80%) | 0.54 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Arterial hypertension | 47 (70.1%) | 18 (90%) | 0.04 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoking | 34 (50.7%) | 13 (65%) | 0.28 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history of IHD | 5 (7.5%) | 0 (0%) | 0.21 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 6 (9%) | 5 (25%) | 0.03 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Early postinfarction angina | 20 (29.9%) | 10 (50%) | 0.04 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Previous MI | 3 (4.5%) | 5 (25%) | 0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cerebrovascular accident/transient ischemic attack in history | 5 (7.5%) | 1 (5%) | 0.7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Percutaneous coronary intervention history | 3 (4.5%) | 2 (10%) | 0.35 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes/impaired glucose tolerance history | 8 (11.9%) | 5 (25%) | 0.15 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lesion depth | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q-wave MI | 47 (70.1%) | 18 (90%) | 0.33 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Q-wave MI | 20 (29.9%) | 2 (10%) | 0.14 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Localization of MI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| posterior side of the left ventricle | 40 (59.7%) | 4 (20%) | <0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| posterior extending to the front side of the right ventricle | 10 (14.9%) | 2 (10%) | 0.11 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| front side of the left ventricle | 17 (25.4%) | 14 (70%) | <0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Acute heart failure (Killip) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | 58 (86.6%) | 9 (45%) | <0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 9 (13.4%) | 9 (45%) | <0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 0 | 1 (5%) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 0 | 1 (5%) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cardiac arrhythmias | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ventricular tachycardia | 3 (4.5%) | 0 | 0.36 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Atrial fibrillation | 3 (4.5%) | 2 (10%) | 0.37 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Third-degree atrioventricular block | 2 (3%) | 1 (5%) | 0.29 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Early post-infarction angina | 3 (4.5%) | 2 (10%) | 0.35 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrent MI | 2 (3%) | 1 (5%) | 0,66 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart failure | 2 (3%) | 0 | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| coronary artery bypass grafting | 0 | 2 (10%) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Death | 1 (1.5%) | 0 | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatment strategy/drug groups | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β-blockers | 66 (98.5%) | 20 (100%) | 0.58 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Angiotensin-converting-enzyme inhibitor | 54 (80.6%) | 15 (75%) | 0.59 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Calcium channel blocker | 46 (68.7%) | 14 (70%) | 0.91 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Loop diuretics | 20 (29.9%) | 14 (70%) | 0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiazide diuretics | 2 (3%) | 3 (15%) | 0.04 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Spironolactone | 24 (35.8%) | 14 (70%) | 0.01 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nitrates | 8 (11.9%) | 7 (35%) | 0.02 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 67 (100) | 20 (100) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heparin | 35 (52.2%) | 15 (75%) | 0.07 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clopidogrel | 65 (97%) | 20 (100%) | 0.99 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statins | 47 (70.1%) | 11 (55%) | 0.21 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thrombolytic therapy | 8 (11.9%) | 3 (15%) | 0.72 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Percutaneous coronary intervention | 64 (95.5%) | 20 (100%) | 0.98 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IHD: ischemic heart disease; MI: myocardial infraction. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
According to the patients’ medical records, coronary artery disease (CAD) risk factors were more frequently observed in patients belonging to the maladaptive remodelling group, than in the adaptive remodelling group, such as AH, observed in 90% of patients in this group, while in 50% of patients, clinical signs of angina pectoris were noticeable prior to the MI development. In 25% of patients with maladaptive remodelling, MI had been previously diagnosed (Table 2).
Q-wave MI and anterior localization were observed more frequently in patients with the pathological variant of remodelling. In contrast to this, non-Q-wave MI and posterior localization were more frequently observed in patients with adaptive cardiac remodelling. Adaptive remodelling was shown to correlate significantly with the presence of acute heart failure Killip class I, while patients in the maladaptive remodelling group were shown to have acute heart failure of Killip classes II-IV.
The scope of the applied therapy did not differ between the groups, but the patients with maladaptive cardiac remodelling were shown to be prescribed loop, thiazide, potassium-sparing diuretics and nitrates more often.
Cardiac remodelling markers
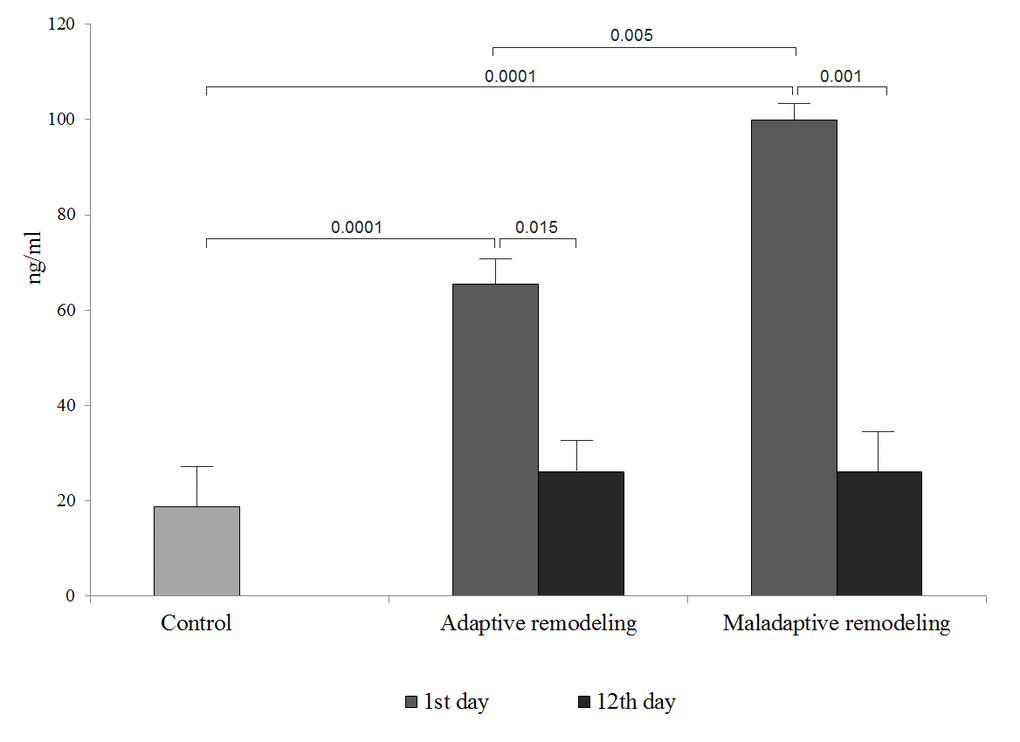
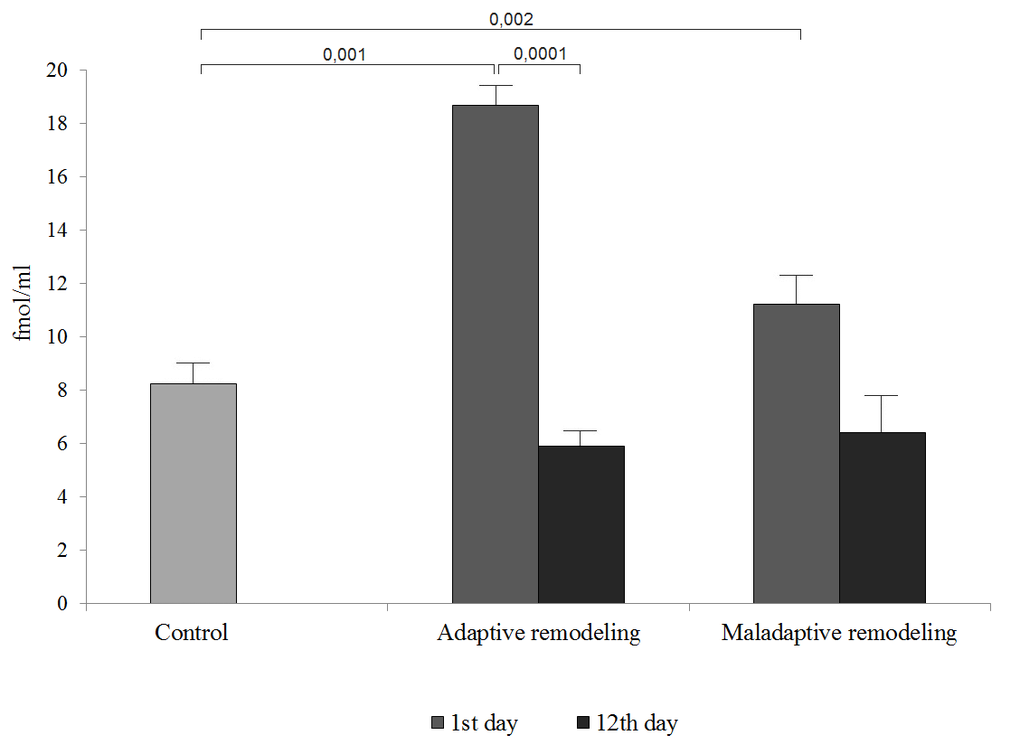
ST2 and NT-proBNP levels in the sera of patients belonging to the adaptive and maladaptive cardiac remodelling group, at day 1 after the MI, were shown to be higher than those in the control group. ST2 levels were 2.3- and 1.4-fold higher, respectively, while those of the NT-proBNP were 3.5- and 5.3-fold higher, respectively.
On day 12 after the MI, significant changes were observed only in the ST2 levels, which decreased in the adaptive and maladaptive cardiac remodelling groups, 2.5 and 3.8 folds, respectively.
We demonstrated that the increased levels of ST2 on day 1 after the MI were associated with the development of the pathological variant of postinfarction remodelling, and its levels were 1.5 folds increased in comparison with those in the adaptive remodelling group. However, NT-proBNP levels were similar in both groups during the hospitalization period (Fig. 1, 2).
We analysed the relationships between ST2 levels and LV functional characteristics. We demonstrated an inverse correlation between the ST2 and LVEF (r=-0.545, P=0.001) and direct correlation between medium strength and EDV (r=0.510, P=0.003) or ESV (r=0.463, P=0.001). However, NT-proBNP levels were shown to be inversely correlated with EDV volume alone (r=-0.514, P=0.010). Moreover, we were interested in the correlation analysis between troponin T (the classic marker of cardiomyocyte damage) and sST2 concentrations during the MI hospitalization period. The results of the correlation analyses indicated a direct correlation between the levels of sST2 and troponin T in both groups at the time of admission (R = 0.65, P = 0.002) (Table 3).
Table 3. Correlation of N-terminal pro b-type natriuretic peptide, stimulating growth factor ST2 levels and echocardiography parameters.
| Variable | Ejection fraction (%) | End-diastolic dimension (сm) | End-systolic dimension (сm) | |
| ST2, ng/ml | R | -0.545 | 0.510 | 0.463 |
| P | 0.001 | 0.003 | 0.000 | |
| NT-proBNP, fmole/ml | R | - | -0.514 | - |
| P | - | 0.010 | - |
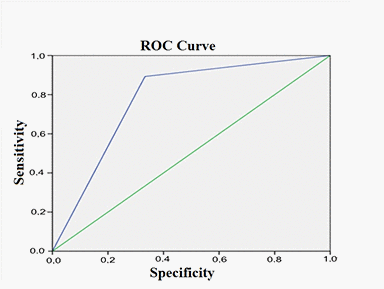
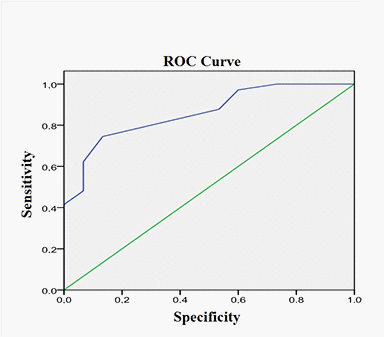
Using the logistic regression analysis, we determined that ST2 levels measured on day 1 after the MI are associated with the development of maladaptive remodelling of LV (OR=4.5, 95% CI=2.0-10.1, P=0.011, AUG=0.81; sensitivity, 78.7%; specificity, 69.4%) (Fig.3), while the levels of NT-proBNP were less significantly associated with the risk of maladaptive remodelling (OR=2.3, 95% CI=2.0-2.01, P=0.032, AUG=0.68; sensitivity, 69.5%; specificity, 45.9%) (Fig.4).
Discussion
The adaptive or physiological variant of cardiac remodelling assumes the absence of the signs of heart failure and minor changes in LV structure. The presence of these symptoms and a progressive heart failure determines the maladaptive or pathological variant of remodelling, which is crucial for the formation and progression of chronic heart failure in patients after the MI [1,2]. Here, we observed that almost a fifth of all patients with STEMI in the postinfarction period showed signs of maladaptive cardiac remodelling.
Maladaptive sequelae after MI often contribute to the unfavourable course of the disease and the mortality of the patients. Despite the significant progress in treatment development, the prognosis is still unfavourable for these patients [9,10].
Here, we determined that the cardiac rhythm disorders, such as ventricular fibrillation, third-degree atrioventricular nodal block, early postinfarction angina and the recurrent MI were more often observed among the patients with maladaptive cardiac remodelling.
In response to the hemodynamic stress and during LV postinfarction remodelling, a number of humoral factors are secreted, including NT-proBNP, an indicator of myocardial stretching [4,7,11], which is considered an adaptive response to injury. NT-proBNP renin-angiotensin-aldosterone system antagonist, its levels increase during natriuresis and diuresis, and it induces vasodilation, reduces heart preload and afterload and blood pressure, and has anti-ischemic effects [12–14]. This molecule is used as a biological marker, which is secreted before troponin can be detected in blood, and its levels reflect the severity of structural and functional impairments of the myocardium [3,4]. NT-proBNP levels were shown to decrease significantly in the patients with adaptive cardiac remodelling, while no significant changes were observed in the maladaptive remodelling group.
Several studies reported a statistically significant association between NT-proBNP levels and the impaired LV structure and function during postinfarction remodelling, specifically with LV dilatation and systolic dysfunction, which are considered the most unfavourable factors for the development and progression of heart failure [15,16]. However, in this study, only an inverse correlation between the NT-proBNP levels and EDV was observed.
Furthermore, the alterations in the levels of ST2 were more pronounced, since the levels of this molecule increased on day 1 after the MI and decreased by day 12. The increase in the levels of ST2 are associated with the increase in the levels of its synthesis in cardiomyocytes and fibroblasts due to biomechanical stress [7,17,18]. Moreover, ST2 levels were shown to be associated with the functional activity of LV, necrotic zone size. Additionally, this molecule was shown to be a marker of postinfarction remodelling: in patients with heart failure, the disturbance of ST2 signal transmission leads to the gradual remodelling of myocardium [19]. Previous studies showed that ST2 levels are associated with the severity of heart failure, regardless of the risk associated with the increase in NT-proBNP levels and the impact of other risk factors [20–23].
Here, we showed that ST2 levels on day 1 after the MI are significantly higher in the patients with maladaptive cardiac remodelling, compared with those in the adaptive remodelling group. The increase in ST2 levels during the maladaptive remodelling may be connected with the increase in the levels of soluble form of this marker during the cardiomyocyte injury. Additionally, following the MI, the activation of humoral and cellular immune response, which is necessary for cicatrization of the necrotic zone, contributes to the increase in ST2 levels [9]. Furthermore, increased levels of this marker can be explained by considerable hemodynamic decompensation and the induction of inflammation during ischemia/reperfusion [8].
The results demonstrating that by day 12 after the MI, the levels of ST2 decreased, and were similar to the levels determined in the controls. These results are consistent with the previously reported results, obtained using an experimental mouse model of MI, by ligating coronary artery. It was shown that the maximal induction of ST2 transcription in cardiomyocytes occurs 2 h after the MI, lasts for 9 h and decreases after 15 h [24].
Maladaptive cardiac remodelling is characterized by a progressive increase in the volume and wall thickness of LV cavity. Structural changes are accompanied by a decrease in myocardial contractility and diastolic function [18]. Therefore, the results of this study demonstrated a correlation between ST2 levels and EF, EDV and ESV. Furthermore, we observed a decrease in the E/А ratio, indicating impaired LV myocardium relaxation and diastolic dysfunction. Rhythm disturbances were more often observed in patients with the pathological variant of postinfarction remodelling. The obtained data are consistent with the results obtained in the large-scale studies including patients with acute MI, which revealed the correlations with LVEF in early time-points following the MI [15,18].
Conclusion
We observed maladaptive cardiac remodelling in 23% of 87 patients included in this study. ST2 levels were shown to change significantly during the hospitalization period after the MI, but they return to the levels of control by day 12 after the MI. Maladaptive remodelling was shown to be associated with increased levels of this marker, in contrast to that of the NT-proBNP, which did not differ between the analysed groups. ST2 levels on day 1 after the MI may be a useful marker for the prediction of maladaptive remodelling risk, and this marker was shown to have a higher sensitivity and specificity than NT-proBNP.
Methods
This study and all experimental protocols used were approved by the Ethics Committee of the Federal State Budgetary Institution, Research Institute for Complex Issues of Cardiovascular Diseases (protocol No. 10 from 10.06.2015), and was developed in accordance with the Declaration of Helsinki (“Ethical principles for medical research involving human subjects”, amended in 2000) and “Rules for clinical practice in the Russian Federation”, approved by the Ministry of Health of the Russian Federation on 19 June 2003. Written informed consent was obtained from all patients prior to their enrolment.
Study participants
The inclusion criterion was the ST-elevated MI (STEMI) within 24 h prior to the hospital admission, with no age restrictions. The exclusion criteria were: MI requiring complicated percutaneous coronary intervention (PCI) or coronary artery bypass grafting, terminal kidney failure (glomerular filtration rate<15 mL/min), a history of diabetes mellitus and diabetic comas, a known cancer history, the presence of other diseases that may significantly reduce life expectancy, including systemic diseases of connective tissue and other potential inducers of cardiac remodelling, such as malignant arterial hypertension (AH), valvular diseases, cardiomyopathy, arrhythmias and others.
The diagnosis of STEMI was established according to the National Guidelines 2007 of the Russian Society of Cardiology, which includes clinical data indicating angina lasting for 20 min or more, electrocardiographic findings indicating ST-segment elevation by 0.1 mW in two or more contiguous leads or new-onset complete left bundle branch block in ECG and an increase in the level of troponin T greater than 0.1 ng/mL. At least two of these criteria had to be satisfied, while the increase in the levels of biochemical markers of myocardial necrosis was a necessary condition. MI severity class was evaluated using the Killip classification (1967) [25].
Study population
Eighty-seven patients (65 male, 22 female) with STEMI, admitted to the hospital within 24 h from the moment of clinical symptom manifestation, were enrolled in the study during one calendar year (2015). Clinical and anamnestic characteristics are presented in Table 4.
Table 4. Baseline clinical and anamnestic characteristics of patients enrolled in this study Мe (Q1;Q3).
| Variable | n=87 | % | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Men | 65 | 75 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Arterial hypertension | 65 | 75 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoking | 47 | 54 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history of IHD | 22 | 25 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 26 | 30 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Early post-infarction angina | 30 | 34 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Previous MI | 8 | 9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cerebrovascular accident/transient ischemic attack in history | 6 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lesion depth | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q-wave MI | 65 | 75 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Q-wave MI | 22 | 25 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Localization of MI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| posterior | 44 | 51 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| posterior extending to the front side of the right ventricle | 12 | 14 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| front side of the left ventricle | 31 | 36 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Acute heart failure (Killip) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I II III IV | 67 18 1 1 | 77 21 1 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ventricular tachycardia | 3 | 3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Atrial fibrillation | 5 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Atrioventricular block III | 3 | 3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Early post-infarction angina, n (%) | 5 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrent MI | 3 | 3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Comorbidities | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chronic bronchitis | 19 | 22 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peptic ulcer disease in remission | 17 | 20 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chronic pyelonephritis | 20 | 23 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatment strategy/group of drugs | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β-blockers | 82 | 94 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| angiotensin-converting-enzyme inhibitor | 69 | 79 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Calcium channel blocker | 60 | 69 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Loop diuretics | 34 | 39 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiazide diuretics | 5 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Spironolactone | 38 | 44 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nitrates | 15 | 17 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 87 | 100 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heparin | 50 | 57 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clopidogrel | 75 | 96 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statins | 68 | 77.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thrombolytic therapy | 11 | 13 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Percutaneous coronary intervention | 84 | 97 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IHD: ischemic heart disease; MI: myocardial infraction. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Patients with no contraindications during the hospital stay were prescribed combined coronary active anti-thrombotic therapy according to the standard practice (Table 1). Statins were administered to 58 (67%) patients. As a reperfusion therapy, a primary PCI in the culprit artery was implemented in 97% of the patients, and 13% of patients received systemic thrombolysis with 1.5×106 IU of streptokinase.
Echocardiography
On day 10-12, all patients underwent echocardiography using ALOKA ProSound α-10 Model SSD-α10 (ALOKA CO, LTD. Tokyo, Japan) in M- and B-modes, in pulsed wave and constant wave Doppler modes, colour flow Doppler echocardiography, in tissue mode, Doppler and in colour M-mode, Doppler echocardiography, using ultrasound array sensor at 2-4 MHz. The examination was performed in standard positions. The following indicators of structural and functional state of cardiovascular system were evaluated: ejection fraction (EF), left atrial (LA) dimension, LV end-diastolic dimension (EDD), LV end-systolic dimension (ESD), LV end-diastolic volume (EDV), LV end-systolic volume (ESV), interventricular septum (IVS) dimension and LV posterior wall dimension (LVPW). Relative wall thickness index was calculated as well, according to the following formula: RWT=IVST+LVPWT)/LV EDD). Patients were divided into two groups, based on the presence of adaptive or maladaptive remodelling. According to the National Guidelines of the Russian Society of Cardiology and the Society of Heart Failure Specialists on diagnosis and treatment of chronic heart failure, the remodelling was considered adaptive if: (a) LVEF≥45% and/or LV EDD<5.5 cm; (b) RWT=0.3–0.45 cm; (c) diastolic dysfunction in the form of (IVST+LVPWT)=1.3–2.0 cm, and/or LVPWT>1.2 and/or hypertrophic type of transmitral Doppler flow spectrum (TMDF), Е/А (wave of early diastolic filling/atrial wave of active filling)=1.1–2.0. Maladaptive remodelling was characterized by the following: (a) LVEF≤45% and/or LV EDD>5.5 cm; (b) RWT≤0.3 cm; (c) diastolic dysfunction in the form of (IVST+LVPWT)>2.0 cm and/or Е/А=1.1-2.0. Adaptive remodelling group included 67 patients, while the maladaptive remodelling group included 20 patients. The control group consisted of 30 patients without cardiovascular diseases who were compatible in gender and age with the patients of the main group.
Laboratory assays
Serum was separated from venous blood by centrifugation at 3,000 ×g for 20 min and stored at -70°C. ST2 levels were measured using Presage ST2 assay (Critical Diagnostics, San Diego, CA, USA). This assay has a within-run coefficient of variation (CV)<6.5% and total CV<9.1% at a mean concentration of 16.9 ng/mL. We determined NT-proBNP levels with the Biomedica kit (Bratislava, Slovakia). The intra-assay CVs were 5% and 8% at a mean concentration of 13 fmol/mL. Troponin T levels were measured with Roche CARDIAC (Roche Diagnostics, Mannheim, Germany). All Roche assays were performed with the use of the Elecsys 2010 system (Roche Diagnostics): Troponin T (fourth generation) with a limit of detection of 0.01 ng/mL, a 99th-percentile cutoff point of less than 0.01 ng/mL, and a CV of less than 10% at 0.035 ng/mL.
Statistical analysis
Statistical analyses of data obtained in this study was performed using software tool STATISTICA 6.1 (StatSoft, Tulsa, OK, USA) and SPSS 10.0 for Windows (SPSS Inc., Chicago, IL, USA). The results are presented as median and the first and third quartiles (Q1 and Q3). We used the non-parametric Mann-Whitney-Wilcoxon tests for the analysis of quantitative data that was not normally distributed. Spearman correlation analysis was used to determine the relationship between the variables. The analysis of the frequency ratio differences between two independent groups was performed using the Fisher's exact test with two-sided confidence interval. P values lower than 0.05 were considered statistically significant. The identification of the most informative indicators for the estimation of postinfarction remodelling with the determination of odds ratio (OR) and 95% confidence interval (CI) was performed by using stepwise logistic regression analysis and defining the area under receiver operating curve (AUC).
Ethical approval
The study protocol was approved by the local ethics committee of the Federal State Budgetary Scientific Institution Research Institute for Complex Issues of Cardiovascular Diseases.
Author Contributions
OG, YD: principal investigator, study coordinator, and investigator, participated in all stages of recruitment of the patients and in analysis of the data, and drafted and critically reviewed the manuscript. EU, YS and OA: study coordinator and investigator, participated in all stages of recruitment of the patients and in analysis of the data, and drafted and critically reviewed the manuscript. VK, and AS: study investigator, participated in all stages of recruitment of patients, in the statistical analysis as well as writing the paper, and critically reviewed the manuscript. OB, OP and VK were principal investigators. All authors have read and approved the final manuscript.
Acknowledgments
The authors wish to thank Elena Semibratova for assistance in writing this article.
Conflicts of Interest
This manuscript has been read and approved by all the authors. This paper is unique and is not under consideration by any other journal and has not been published elsewhere. The authors of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
References
- 1. Opie LH, Commerford PJ, Gersh BJ, Pfeffer MA. Controversies in ventricular remodelling. Lancet. 2006; 367:356–67. https://doi.org/10.1016/S0140-6736(06)68074-4 [PubMed]
- 2. Gerdes AM, Capasso JM. Structural remodeling and mechanical dysfunction of cardiac myocytes in heart failure. J Mol Cell Cardiol. 1995; 27:849–56. https://doi.org/10.1016/0022-2828(95)90000-4 [PubMed]
- 3. Gravning J, Smedsrud MK, Omland T, Eek C, Skulstad H, Aaberge L, Bendz B, Kjekshus J, Mørkrid L, Edvardsen T. Sensitive troponin assays and N-terminal pro-B-type natriuretic peptide in acute coronary syndrome: prediction of significant coronary lesions and long-term prognosis. Am Heart J. 2013; 165:716–24. https://doi.org/10.1016/j.ahj.2013.02.008 [PubMed]
- 4. Barbarash OL, Usoltseva EN. Heart failure treatment under control of natriuretic peptides concentration. Complex Issues of Cardiovascular Diseases. 2014; 1:67–74. in Russian. .
- 5. Maries L, Manitiu I. Diagnostic and prognostic values of B-type natriuretic peptides (BNP) and N-terminal fragment brain natriuretic peptides (NT-pro-BNP). Cardiovasc J Afr. 2013; 24:286–89. https://doi.org/10.5830/CVJA-2013-055 [PubMed]
- 6. Pascual-Figal DA, Januzzi JL. The biology of ST2: the International ST2 Consensus Panel. Am J Cardiol. 2015 (Suppl ); 115:3B–7B. https://doi.org/10.1016/j.amjcard.2015.01.034 [PubMed]
- 7. Ciccone MM, Cortese F, Gesualdo M, Riccardi R, Di Nunzio D, Moncelli M, Iacoviello M, Scicchitano P. A novel cardiac bio-marker: ST2: a review. Molecules. 2013; 18:15314–28. https://doi.org/10.3390/molecules181215314 [PubMed]
- 8. Barbarash O, Gruzdeva O, Uchasova E, Dyleva Y, Belik E, Akbasheva O, Karetnikova V, Shilov A. Prognostic value of soluble ST2 during hospitalization for ST-segment elevation myocardial infarction. Ann Lab Med. 2016; 36:313–319. https://doi.org/10.3343/alm.2016.36.4.313 [PubMed]
- 9. Felker GM, Fiuzat M, Thompson V, Shaw LK, Neely ML, Adams KF, Whellan DJ, Donahue MP, Ahmad T, Kitzman DW, Piña IL, Zannad F, Kraus WE, O’Connor CM. Soluble ST2 in ambulatory patients with heart failure: association with functional capacity and long-term outcomes. Circ Heart Fail. 2013; 6:1172–79. https://doi.org/10.1161/CIRCHEARTFAILURE.113.000207 [PubMed]
- 10. Shimpo M, Morrow DA, Weinberg EO, Sabatine MS, Murphy SA, Antman EM, Lee RT. Serum levels of the interleukin-1 receptor family member ST2 predict mortality and clinical outcome in acute myocardial infarction. Circulation. 2004; 109:2186–90. https://doi.org/10.1161/01.CIR.0000127958.21003.5A [PubMed]
- 11. Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008; 358:2148–59. https://doi.org/10.1056/NEJMra0800239 [PubMed]
- 12. Mathewkutty S, Sethi SS, Aneja A, Shah K, Iyengar RL, Hermann L, Khakimov S, Razzouk L, Esquitin R, Vedanthan R, Benjamin TA, Grace M, Nisenbaum R, et al. Biomarkers after risk stratification in acute chest pain (from the BRIC Study). Am J Cardiol. 2013; 111:493–98. https://doi.org/10.1016/j.amjcard.2012.10.032 [PubMed]
- 13. He Q, Wang D, Yang XP, Carretero OA, LaPointe MC. Inducible regulation of human brain natriuretic peptide promoter in transgenic mice. Am J Physiol Heart Circ Physiol. 2001; 280:H368–76. https://doi.org/10.1152/ajpheart.2001.280.1.H368 [PubMed]
- 14. Khan SQ, Dhillon O, Kelly D, Squire IB, Struck J, Quinn P, Morgenthaler NG, Bergmann A, Davies JE, Ng LL. Plasma N-terminal B-Type natriuretic peptide as an indicator of long-term survival after acute myocardial infarction: comparison with plasma midregional pro-atrial natriuretic peptide: the LAMP (Leicester Acute Myocardial Infarction Peptide) study. J Am Coll Cardiol. 2008; 51:1857–64. https://doi.org/10.1016/j.jacc.2008.01.041 [PubMed]
- 15. Khan SQ, Quinn P, Davies JE, Ng LL. N-terminal pro-B-type natriuretic peptide is better than TIMI risk score at predicting death after acute myocardial infarction. Heart. 2008; 94:40–43. https://doi.org/10.1136/hrt.2006.108985 [PubMed]
- 16. Kakkar R, Lee RT. The IL-33/ST2 pathway: therapeutic target and novel biomarker. Nat Rev Drug Discov. 2008; 7:827–40. https://doi.org/10.1038/nrd2660 [PubMed]
- 17. Sabatine MS, Morrow DA, Higgins LJ, MacGillivray C, Guo W, Bode C, Rifai N, Cannon CP, Gerszten RE, Lee RT. Complementary roles for biomarkers of biomechanical strain ST2 and N-terminal prohormone B-type natriuretic peptide in patients with ST-elevation myocardial infarction. Circulation. 2008; 117:1936–44. https://doi.org/10.1161/CIRCULATIONAHA.107.728022 [PubMed]
- 18. Januzzi JL
Jr . ST2 as a cardiovascular risk biomarker: from the bench to the bedside. J Cardiovasc Transl Res. 2013; 6:493–500. https://doi.org/10.1007/s12265-013-9459-y [PubMed] - 19. Weir RA, Miller AM, Murphy GE, Clements S, Steedman T, Connell JM, McInnes IB, Dargie HJ, McMurray JJ. Serum soluble ST2: a potential novel mediator in left ventricular and infarct remodeling after acute myocardial infarction. J Am Coll Cardiol. 2010; 55:243–50. https://doi.org/10.1016/j.jacc.2009.08.047 [PubMed]
- 20. Januzzi JL
Jr , Rehman S, Mueller T, van Kimmenade RR, Lloyd-Jones DM. Importance of biomarkers for long-term mortality prediction in acutely dyspneic patients. Clin Chem. 2010; 56:1814–21. https://doi.org/10.1373/clinchem.2010.146506 [PubMed] - 21. Januzzi JL
Jr , Peacock WF, Maisel AS, Chae CU, Jesse RL, Baggish AL, O’Donoghue M, Sakhuja R, Chen AA, van Kimmenade RR, Lewandrowski KB, Lloyd-Jones DM, Wu AH. Measurement of the interleukin family member ST2 in patients with acute dyspnea: results from the PRIDE (Pro-Brain Natriuretic Peptide Investigation of Dyspnea in the Emergency Department) study. J Am Coll Cardiol. 2007; 50:607–13. https://doi.org/10.1016/j.jacc.2007.05.014 [PubMed] - 22. Pascual-Figal DA, Lax A, Perez-Martinez MT, del Carmen Asensio-Lopez M, Sanchez-Mas J, and GREAT Network. Clinical relevance of sST2 in cardiac diseases. Clin Chem Lab Med. 2016; 54:29–35. https://doi.org/10.1515/cclm-2015-0074 [PubMed]
- 23. Dupuy AM, Curinier C, Kuster N, Huet F, Leclercq F, Davy JM, Cristol JP, Roubille F. Multi-Marker Strategy in Heart Failure: Combination of ST2 and CRP Predicts Poor Outcome. PLoS One. 2016; 11:e0157159. https://doi.org/10.1371/journal.pone.0157159 [PubMed]
- 24. Weinberg EO, Shimpo M, De Keulenaer GW, MacGillivray C, Tominaga S, Solomon SD, Rouleau JL, Lee RT. Expression and regulation of ST2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation. 2002; 106:2961–66. https://doi.org/10.1161/01.CIR.0000038705.69871.D9 [PubMed]
- 25. Killip T
3rd , Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967; 20:457–464. https://doi.org/10.1016/0002-9149(67)90023-9 [PubMed]