



Introduction
Patients with end-stage renal disease (ESRD) have a higher prevalence of peripheral arterial disease (PAD) than the general population [1, 2]. PAD can manifest with mild or no symptoms, intermittent claudication, or chronic limb-threatening ischemia (CLTI) [3]. CLTI is a late stage of PAD, defined as limb pain that occurs at rest or impending limb loss caused by severe compromise of blood flow to the affected extremity [3]. Patients with CLTI have the worst PAD outcomes; however, the progression to CLTI is often variable and unpredictable [4]. Thus, approaches to maximize early detection and management of CLTI have been an issue in managing patients undergoing hemodialysis.
Frailty is the increased susceptibility to stressors resulting from impairments across physiological, psychological, and socioeconomic domains [5]. It is characterized by muscle weakness, inadequate nutrition, reduced physical activity, and comorbidities, differentiating it from traditional risk factors [6]. Observational studies have established a significant correlation between frailty and various outcomes such as mortality, cognitive dysfunction, quality of life, and cardiovascular disease in the dialysis population [7–14]. Frailty is highly prevalent in the hemodialysis population, with an estimated prevalence of 29–46% [10, 15, 16]. Recent meta-analyses also noted that the prevalence of frailty was approximately 50% in patients with lower extremity PAD [17–21]. PAD may also be a contributing factor to the diagnosis of frailty [5, 22]. The relationship between PAD and frailty in patients undergoing dialysis remains to be comprehensively investigated. Prospective data are needed to clarify the causal relationship and prognostic value of frailty in adverse events among patients undergoing hemodialysis [23, 24].
We hypothesize that frailty might result in delayed recognition and treatment of PAD and lead to CLTI [23]. The Hsinchu Vascular Access (Hsinchu VA) study was a prospective cohort study that investigated the relationship between clinical factors and incident cardiovascular diseases in patients undergoing hemodialysis [24]. In a substantial proportion of these patients, performance-based frailty status was assessed at enrollment, and PAD events were prospectively documented during the follow-up period [24]. We conducted a pre-planned secondary analysis of the Hsinchu VA study to test the hypothesis that frail patients would have a higher incidence of CLTI than non-frail patients and examine the association of frailty with other major adverse limb events (MALE).
Results
Study participants
This current analysis included 828 patients who had completed the frailty assessment from the original cohort of 1,136 patients. Baseline characteristics were similar to those in patients undergoing hemodialysis in a recent nationwide registry in Taiwan (Supplementary Table 1).
Table 1 shows the baseline characteristics and comorbidities of the study participants. The mean age (standard deviation) of the study participants was 67 (14) years, and 395 (48%) were female. The median duration of hemodialysis was 3.7 (interquartile range (IQR), 0.6–5.6) years, and the median duration of follow-up was 4 (IQR, 2.8–5.0) years. The study participants had various comorbidities: 724 (87%) had hypertension, 436 (53%) had diabetes mellitus (DM), 202 (24%) had hyperlipidemia, and 119 (14%) were smokers. Some patients had pre-existing vascular diseases at enrollment, including 217 (26%) with coronary artery disease (CAD), 73 (8.8%) with PAD, and 76 (9.2%) with cerebrovascular accident (CVA).
Table 1. Baseline characteristics of the study participants stratified by frailty status.
| Variable | Overall, N = 828a | Not Frail, N = 231a | Pre-Frail, N = 317a | Frail, N = 280a | P-valueb | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Demographic and socioeconomic factors | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | 67 (14) | 62 (13) | 65 (15) | 71 (12) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age >65 years | 432 (52%) | 88 (38%) | 149 (47%) | 195 (70%) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female sex | 395 (48%) | 91 (39%) | 149 (47%) | 155 (55%) | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 22.9 (4.2) | 23.1 (4.0) | 22.9 (4.3) | 22.7 (4.4) | 0.40 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education >6 years | 514 (62%) | 161 (70%) | 211 (67%) | 142 (51%) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Married | 636 (77%) | 175 (76%) | 255 (80%) | 206 (74%) | 0.13 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 119 (14%) | 41 (18%) | 44 (14%) | 34 (12%) | 0.20 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Comorbidities | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 724 (87%) | 204 (88%) | 278 (88%) | 242 (86%) | 0.80 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DM | 436 (53%) | 97 (42%) | 158 (50%) | 181 (65%) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperlipidemia | 202 (24%) | 63 (27%) | 79 (25%) | 60 (21%) | 0.30 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CAD | 217 (26%) | 47 (20%) | 84 (26%) | 86 (31%) | 0.03 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAD | 73 (8.8%) | 14 (6.1%) | 25 (7.9%) | 34 (12%) | 0.04 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CVA or ICH | 76 (9.2%) | 9 (3.9%) | 29 (9.1%) | 38 (14%) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CHF | 101 (12%) | 28 (12%) | 33 (10%) | 40 (14%) | 0.35 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AF | 114 (14%) | 23 (10.0%) | 41 (13%) | 50 (18%) | 0.03 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver disease | 90 (11%) | 21 (9.1%) | 43 (14%) | 26 (9.3%) | 0.15 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| COPD | 19 (2.3%) | 9 (3.9%) | 6 (1.9%) | 4 (1.4%) | 0.15 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cancer | 72 (8.7%) | 12 (5.2%) | 35 (11%) | 25 (8.9%) | 0.06 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dialysis factors | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dialysis vintage (years) | 3.7 (0.6, 5.6) | 4.0 (0.8, 6.8) | 3.4 (0.6, 5.6) | 3.2 (0.6, 5.2) | 0.14 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fluid removal (%) | 3.57 (1.42) | 3.74 (1.43) | 3.64 (1.33) | 3.34 (1.47) | 0.007 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dialysis frequency <3 per week | 56 (6.8%) | 14 (6.1%) | 21 (6.6%) | 21 (7.5%) | 0.80 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Albumin (g/dL) | 3.83 (0.34) | 3.92 (0.30) | 3.84 (0.35) | 3.75 (0.32) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Kt/V (Daugirdas) | 1.69 (0.29) | 1.71 (0.31) | 1.68 (0.27) | 1.69 (0.30) | 0.80 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hb (g/dL) | 10.80 (1.37) | 11.01 (1.43) | 10.78 (1.37) | 10.65 (1.30) | 0.02 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medications | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antiplatelet | 212 (26%) | 56 (24%) | 79 (25%) | 77 (28%) | 0.70 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Warfarin | 11 (1.3%) | 2 (0.9%) | 3 (0.9%) | 6 (2.1%) | 0.40 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Beta-blocker | 145 (18%) | 48 (21%) | 54 (17%) | 43 (15%) | 0.30 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RAAS inhibitors | 133 (16%) | 39 (17%) | 58 (18%) | 36 (13%) | 0.20 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 123 (15%) | 28 (12%) | 54 (17%) | 41 (15%) | 0.30 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aMean (SD); n (%); Median (IQR). bKruskal–Wallis rank sum test; Pearson’s Chi-squared test; Fisher’s exact test. Abbreviations: AF: atrial fibrillation; BMI: body mass index; CAD: coronary artery disease; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident; DM: diabetes mellitus; Hb: hemoglobin; ICH: intracerebral hemorrhage; IQR: interquartile range; PAD: peripheral arterial disease; RAAS: renin-angiotensin-aldosterone system; SD: standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Prevalence of and factors associated with frailty
As shown in Table 1, 280 (34%) participants were categorized as frail, 317 (38%) as pre-frail, and 231 (28%) as robust. Frailty was more prevalent in patients who were older, female, and with low education levels. DM and CVA were associated with frailty. After multivariate adjustment, older age (>65 years), female sex, DM, CVA, and serum albumin levels remained significantly associated with frailty (Supplementary Table 2).
Follow-up and events
The median follow-up was 1,461 (IQR, 1,016–1,826) days. During the follow-up period, 4 (0.5%) patients received renal transplantation, 106 (13%) were transferred to non-study facilities, and 231 (28%) died (shown in Supplementary Figure 1). During the follow-up period, CLTI occurred in 104 patients (13%), 28 (3%) underwent amputation, and 101 (12%) underwent intervention. MALE occurred in 108 (13%) patients (shown in Figure 1). The Kaplan–Meier analysis demonstrated a graded relationship between CLTI events and frailty status (not frail, 6.5%; pre-frail, 11%; frail, 20%; P < 0.001) (shown in Figure 2 and Supplementary Table 3). There was also a graded effect between mortality and frailty status (not frail, 13%; pre-frail, 27%; frail, 41%; Supplementary Table 3).
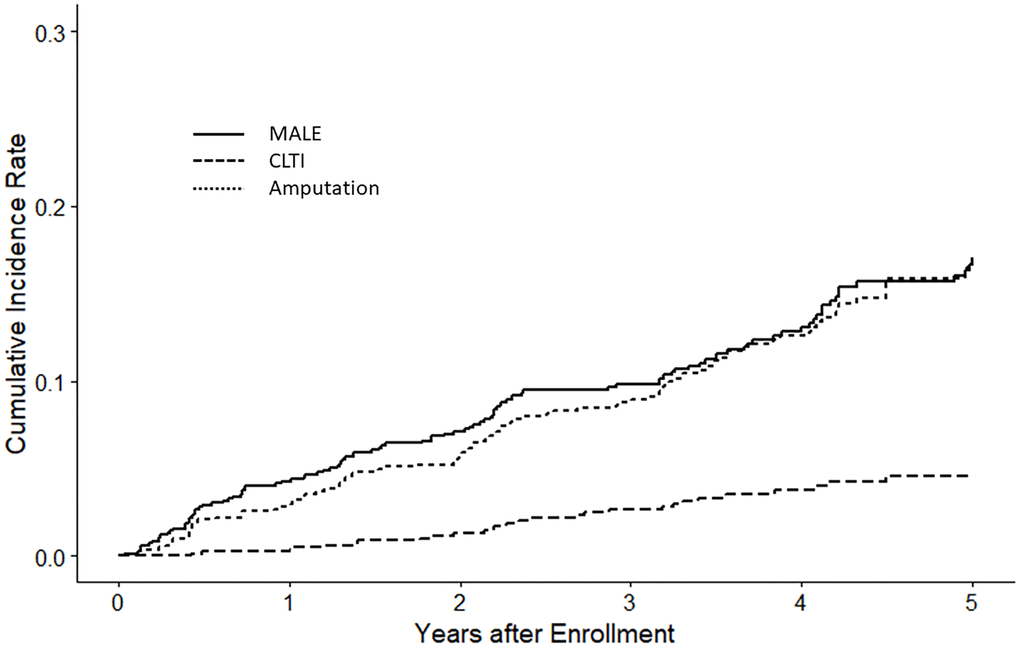
Figure 1. Kaplan–Meier plot of lower limb vascular events. The figure presents lower limb vascular events within the entire study cohort, encompassing major adverse limb events (MALE), chronic limb-threatening ischemia (CLTI), and amputations.
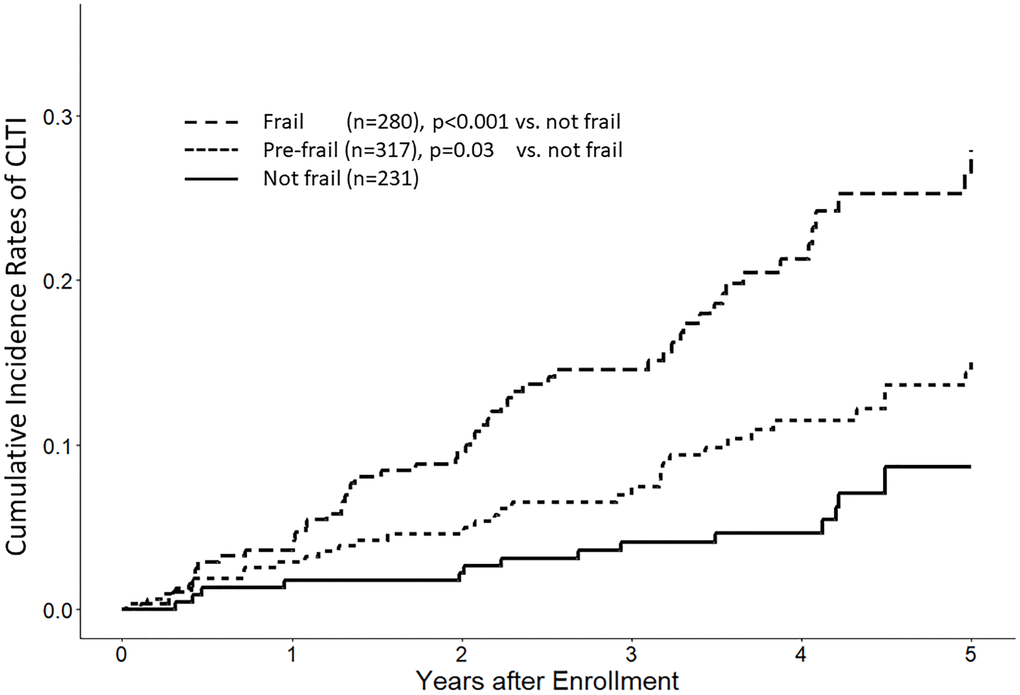
Figure 2. Kaplan–Meier plot of critical limb ischemia events by frailty status. This figure depicts the time to the occurrence of the first chronic limb-threatening ischemia (CLTI) event, categorized based on frailty status.
Cox regression analyses
Univariate Cox proportional hazards regression analysis showed that age, smoking, comorbidities (DM, hyperlipidemia, CAD, CVA, and atrial fibrillation), antiplatelet and statin use, and frailty status were associated with an increased risk of CLTI (Table 2). Frail patients had a more than threefold higher risk of CLTI than those who were non-frail (hazard ratio (HR) 3.94; 95% confidence interval (CI) 2.22, 6.99; P < 0.001). DM (HR 4.43; 95% CI 2.72–7.22; P < 0.001) and frailty status (HR 3.94; 95% CI 2.22–6.99; P < 0.001) were the most significant factors associated with the occurrence of CLTI. After adjusting for age, BMI, educational level, smoking, DM, hypertension, hyperlipidemia, CAD, CVA or ICH, atrial fibrillation, Kt/V, and hemoglobin in the multivariate analysis, frailty status remained significantly associated with an increased risk of CLTI (HR 3.26; 95% CI 1.76–5.85; P < 0.001) (Table 2).
Table 2. Cox regression analysis for factors associated with chronic limb-threatening ischemia.
| Characteristic | Univariable | Multivariable | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HRa | 95% CIa | P-value | HRa | 95% CIa | P-value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Frailty score | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not frail | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pre-frail | 1.95 | 1.06–3.58 | 0.03 | 1.9 | 1.02–3.57 | 0.04 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Frail | 3.94 | 2.22–6.99 | <0.001 | 3.26 | 1.76–5.85 | < 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Demographic and socioeconomic factors | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age >65 (years) | 2.15 | 1.43–3.22 | <0.001 | 1.62 | 1.05–2.62 | 0.03 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female sex | 0.87 | 0.59–1.28 | 0.48 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI groups (kg/m2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <18.5 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18.5–24 | 2.72 | 1.09–6.78 | 0.03 | 1.77 | 0.69–4.52 | 0.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 24–27 | 2.59 | 0.99–6.83 | 0.05 | 1.28 | 0.46–3.51 | 0.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >27 | 2.98 | 1.10–8.08 | 0.03 | 1.72 | 0.60–4.95 | 0.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education <6 years | 1.76 | 1.20–2.58 | 0.004 | 1.36 | 0.89–2.08 | 0.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Married | 0.78 | 0.51–1.20 | 0.26 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 1.97 | 1.26–3.07 | 0.003 | 2.12 | 1.33–3.40 | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Comorbidities | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DM | 4.43 | 2.72–7.22 | <0.001 | 3.24 | 1.83–5.74 | < 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HTN | 0.55 | 0.29–1.02 | 0.06 | 1.21 | 0.59–2.47 | 0.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperlipidemia | 2.32 | 1.57–3.42 | <0.001 | 1.36 | 0.87–2.12 | 0.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CAD | 2.25 | 1.53–3.32 | <0.001 | 0.95 | 0.61–1.50 | 0.8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CVA or ICH | 2.4 | 1.44–3.99 | <0.001 | 1.5 | 0.89–2.54 | 0.13 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CHF | 1.12 | 0.64–1.97 | 0.69 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Atrial fibrillation | 2.61 | 1.70–4.01 | <0.001 | 1.9 | 1.21–2.98 | 0.005 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| COPD | 1.22 | 0.39–3.84 | 0.74 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dialysis factors | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dialysis vintage (years) | 0.97 | 0.94–1.01 | 0.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cholesterol (mg/dL) | 1 | 0.99–1.00 | 0.34 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Albumin (g/dL) | 1.05 | 0.58–1.90 | 0.86 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Kt/V (Daugirdas) | 0.36 | 0.18–0.72 | 0.004 | 0.76 | 0.35–1.64 | 0.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hb (g/dL) | 1.24 | 1.08–1.42 | 0.002 | 1.24 | 1.08–1.44 | 0.003 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medications | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antiplatelet | 3.05 | 2.07–4.48 | <0.001 | 2.1 | 1.33–3.32 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Warfarin | 1.26 | 0.31–5.12 | 0.74 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Beta-blocker | 1.22 | 0.76–1.97 | 0.41 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RAAS inhibitors | 0.68 | 0.38–1.21 | 0.19 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 1.91 | 1.22–3.00 | 0.005 | 1.11 | 0.69–1.81 | 0.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aHR: Hazard Ratio; CI: Confidence Interval. Abbreviations: BMI: body mass index; CAD: coronary artery disease; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident; DM: diabetes mellitus; Hb: hemoglobin; HTN: hypertension; ICH: intracerebral hemorrhage; RAAS: renin-angiotensin-aldosterone system. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Subgroup analysis
After stratification by age of 65 years, DM, and pre-existing vascular diseases, the frailty status remained associated with CLTI events (Figure 3). Frail patients experienced a higher incidence of CLTI events compared to non-frail dialysis patients, with pre-frail patients exhibiting an intermediate incidence.
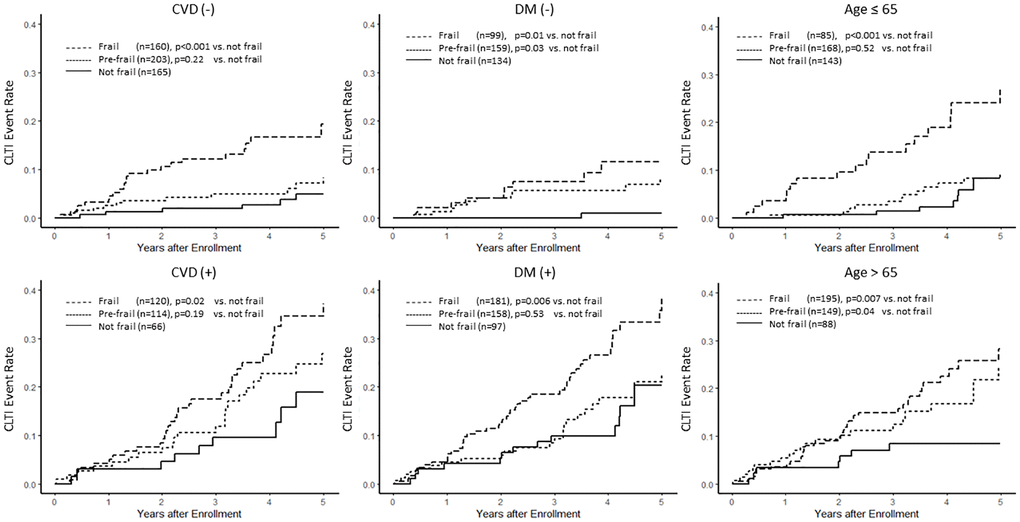
Figure 3. Association between frailty and the risk of chronic limb-threatening ischemia (CLTI) by different subgroups. This figure demonstrates the Kaplan–Meier curves of chronic limb-threatening ischemia (CLTI) stratified by frailty status in different subgroups, including cardiovascular diseases (CVD), diabetes mellitus (DM), and age.
Discussion
The main finding of our study was that frailty was associated with the development of CLTI in patients undergoing hemodialysis. As hypothesized, both frail and pre-frail patients had a higher risk of CLTI events compared to non-frail patients, with a graded effect. Frail individuals exhibited the highest incidence of CLTI events, followed by pre-frail individuals, while non-frail individuals experienced the lowest CLTI events. After adjusting for potential covariates, frail patients exhibited a 3.26-fold increased risk of developing CLTI compared to non-frail patients. Consequently, frailty appears to serve as a predictive factor for CLTI in individuals undergoing hemodialysis.
Various frailty tests are currently available. We used the original performance-based measures proposed by Fried et al [25]. Although cut-offs for gait speed were modified in our study [22, 26], the frailty prevalence of 34% was consistent with that reported in the United States (29–34%) and Asian countries (35%) [15, 16, 22, 26]. Our data confirmed previous observations that frailty was common in the hemodialysis population and is consistent across different ethnic groups. Nevertheless, approximately 27% of hemodialysis patients (308 out of the total cohort of 1,136 patients) in the study did not undergo performance-based assessments, which could have led to an underestimation of the true prevalence of frailty.
In the general population, the prevalence of PAD is 5.6%, and that of CLTI is 1.3% among individuals who are more than 40 years old [27, 28]. The ESRD population has a much higher prevalence of PAD than the general population [2, 29]. For example, the Dialysis Outcomes and Practice Patterns Study reported an 11.5–37.8% prevalence rate of PAD with significant geographic variations [29]. In our study, at the time of patient enrollment, 8.8% of patients had a diagnosis of PAD. This prevalence appears lower than that reported in previous studies, which may be attributed to several factors. First, some patients were in the early stages of initiating hemodialysis, and ankle-brachial index measurements had not yet been conducted. Second, some patients may have been asymptomatic and, consequently, had not received a PAD diagnosis. Nevertheless, we observed a significantly higher CLTI incidence than the general population during the follow-up period. In the general population, the annual incidence of PAD was 0.2/100 person-years (PY), and the incidence of CLTI was approximately 0.02/100 PY [17]. In the hemodialysis population, the incidence of PAD or CLTI has rarely been reported in prospective studies [30, 31]. In our cohort, patients undergoing hemodialysis exhibited a CLTI incidence rate of 3.3 per 100 PY, significantly higher than that reported in the general population [27]. Our findings were compatible with previous evidence that ESRD patients have an eight to 20-fold risk of mortality from cardiovascular events [32–34]. This trend of increased cardiovascular events among ESRD patients has also been observed in the Asian population [35]. Various investigators have reported an increased risk of myocardial infarction, ischemic stroke, acute limb ischemia, and deep vein thrombosis for ESRD patients [29, 35–39]. ESRD patients have increased susceptibility to cardiovascular disease and dysfunction and often have elevated cardiac troponin serum concentrations due to chronic heart muscle injury. Our findings suggest that beyond traditional biomarkers, frailty can be used as an additional clinical risk stratification marker.
To date, no prospective study has examined the relationship between frailty and CLTI or MALE in patients undergoing hemodialysis. For the first time, our cohort demonstrated that assessing frailty helped identify the risk of CLTI events in patients undergoing hemodialysis. The risk of CLTI associated with frailty was more prominent than that associated with most conventional vascular risk factors, except for DM.
As demonstrated in previous studies, DM, aging, and pre-existing vascular disease are well-established risk factors for CTLI [31]. In this study, frailty status remained a significant predictor of CLTI even after adjusting for these factors in the multivariate analysis. Specifically, frail patients had a more than threefold increased risk of CLTI compared to non-frail patients, with pre-frail patients showing an intermediate risk. This graded relationship between frailty and CLTI incidence persisted across various subgroups, including those stratified by age (65 years), presence of DM, and pre-existing vascular diseases. By adjusting for these variables in the multivariate analysis and subgroup analysis, the study robustly demonstrates that frailty independently contributes to the risk of CLTI. This highlights the importance of considering frailty in the management and prognosis of patients undergoing hemodialysis, as it significantly impacts the risk of severe vascular complications regardless of traditional risk factors.
Numerous studies have presented the possibility of an epidemiological and pathophysiological relationship between PAD and frailty. This connection may arise from factors such as aging, shared risk factors, and chronic inflammation, leading to an overall decline in physical function or the development of microvascular and macrovascular complications due to chronic vascular inflammation [17, 40–42]. In our study, we focused on CLTI. The most intuitive link between frailty and CLTI is their shared risk factors. Various mechanisms may explain this association. Frailty and CLTI may share common biological pathways. The pathophysiology of CLTI involves not only obstructive macrovascular disease but also microvascular changes secondary to inflammation, a hypercoagulable state, impaired angiogenesis, and vasomotor paralysis [43]. Previous studies have demonstrated that frailty is associated with increased coagulation markers and the risk of thromboembolism in older patients [44, 45]. Scientific evidence also suggests that inflammation (interleukin-6 and C-reactive protein), oxidative stress, and endothelial dysfunction play important roles in the pathogenesis of frailty [46–48].
Malnutrition and inflammation are often linked with frailty and may contribute to the progression of chronic limb-threatening ischemia (CLTI). The frailty status, frequently associated with malnutrition or immunocompromised states, is part of the malnutrition-inflammation-atherosclerosis (MIA) syndrome, which has been proposed as a cause of increased mortality in ESRD patients [49]. CLTI, as a manifestation of advanced atherosclerotic vascular disease, could be influenced by these factors. In our study, although low serum albumin levels were associated with frailty, they were not correlated with CLTI in our analysis. This finding aligns with the observations by Koch et al., who reported that nutritional status alone does not predict cardiovascular mortality [50]. Similarly, Struijk et al. indicated that serum albumin levels primarily reflect the presence of systemic diseases rather than being a direct predictor of cardiovascular outcomes in dialysis patients. Additionally, our study did not perform comprehensive nutritional assessments or measure inflammatory biomarkers, limiting our ability to fully evaluate the impact of malnutrition and inflammation on CLTI. The results suggest that while frailty is a significant predictor of CLTI, its association with malnutrition and inflammation requires further investigation.
We also found that frailty was associated with a low educational level; the educational level has been identified as a critical component in improving PAD outcomes [51]. Low levels of education can create significant barriers to effective foot care and access to health resources [52]. Finally, reduced physical activity and walking speed are the hallmarks of frailty, as decreased physical activity is associated with atherosclerotic vascular disease, and exercise has been shown to be beneficial for patients with PAD [53, 54]. Therefore, the correlation is biologically plausible because the beneficial effects of physical activity on cardiovascular risk function may be less in frail patients. Exertional leg symptoms may be masked due to inactivity or slow pace in frail patients in whom PAD was not recognized until CLTI occurred.
This study has several strengths. The prospective design ensured that data on lower limb vascular events were collected after frailty assessment with a comprehensive collection of covariates. These approaches enabled us to analyze the causal relationship between frailty and limb events in a temporal sequence to avoid reverse causation. To reduce the bias arising from outcome misclassification, we used medical records containing imaging information and consulted the treating physicians as required. The frailty assessment was based on performance-based measurements rather than questionnaires, which enabled direct comparison with other studies.
However, it is important to acknowledge some limitations in this study. First, the presence of unmeasured confounding variables cannot be completely ruled out. Second, certain criteria used for assessing frailty were adapted to the aging population in Taiwan, potentially limiting the comparability of prevalence statistics with other populations. Third, the reliance on chart records to define PAD outcomes may have resulted in the underreporting of lower limb events. Additionally, the lack of comprehensive ankle-brachial index screening at enrollment could have made PAD unrecognized. Finally, a significant proportion of patients could not undergo frailty assessments, and their exclusion may have limited the generalizability of our study findings to this subset of the population.
PAD is common in patients with kidney failure and often presents as the most severe form of CLTI. Despite its high prevalence, the diagnosis of PAD in patients with kidney failure is challenging because patients often do not present with the classic symptoms of claudication [55, 56]. Incorporation of a frailty assessment, a relatively convenient and objective tool, may help stratify the risk of MALE. The National Kidney Foundation Kidney Disease Outcomes Quality Initiative guidelines on cardiovascular disease in patients undergoing dialysis recommend that all patients should be evaluated for PAD when they initiate dialysis, using a vascular physical examination, duplex ultrasound, or invasive testing as clinically indicated [57]. However, given the increasing pressure on healthcare resources, our results suggest that frail patients may represent a high-risk subgroup that may benefit from PAD screening. Considering the negative consequences of MALE, the assessment of frailty may help improve risk stratification.
In conclusion, patients with frailty who undergo hemodialysis have a high prevalence of PAD and are at an increased risk of developing CLTI. Our study found that frailty was independently associated with worse CLTI outcomes, even after adjusting for relevant risk factors. This observation suggests that evaluating the frailty status can be valuable in identifying individuals with an increased risk of CLTI and its associated complications. Further research is necessary to determine whether interventions aimed at mitigating the negative effects of frailty can improve limb outcomes in patients with CLTI.
Methods
Study design and participants
The Hsinchu VA study was a multicenter prospective study investigating the impact of clinical factors on vascular events in patients undergoing maintenance hemodialysis (ClinicalTrials.gov identifier: NCT04692636). The original study cohort enrolled 1,136 patients on maintenance hemodialysis as of January 1, 2018, from 12 hemodialysis centers in Hsin-Chu, Taiwan, including 4 hospital-based dialysis centers and 8 local dialysis clinics. The inclusion criteria were age 18–90 years, receiving maintenance dialysis for more than 6 months, and not being hospitalized in the previous 3 months. Patients from the original cohort who completed the performance-based frailty evaluation were included in this analysis (shown in Supplementary Figure 1). The study was approved by the institutional review board (106-033-E), and all patients provided informed written consent before enrollment.
Collection of data and follow-up of outcomes
Information on patient demographics, comorbidities, medications, lower limb vascular duplexes, hospitalization records, angiography, dialysis-related data, and laboratory results was obtained from the medical records of the dialysis centers. Trained study coordinators collected this information at baseline and every 3 months thereafter, including questionnaires, medical records, imaging studies, and surgery reports. The data obtained by the study coordinators were coded after review by two investigators (MYH and CCW), and discussions with primary physicians were conducted as needed. Patients were followed up until December 31, 2022, and censored in case of death, kidney transplant, or transfer to a non-study center. The primary outcome of Hsinchu VA study was vascular access thrombotic event. PAD-related events including CLTI, MALE, and amputation were secondary outcomes. The primary purpose of this post-hoc analysis was to report the incidence and associated factors of CLTI in the study cohort.
Diagnosis of PAD and adverse limb events
At enrollment, the history of PAD was based on diagnosis from medical records or endovascular or surgical interventions (including amputation) for PAD. After enrollment, major adverse limb events were documented by interval questionnaire and review of medical records every 3 months. The diagnosis was confirmed by two investigators (MYH and CCW) based on the following criteria: abnormal duplex waveform or stenosis >50% on angiography imaging, endovascular or surgical revascularization, or PAD-related amputation or death. MALE encompassed vascular amputation and repeated vascular interventions. CLTI was defined as the presence of ischemic rest pain (Rutherford stage 4), ulcers, or gangrene (Rutherford stages 5 or 6), whether hospitalization or intervention was undertaken or not. Major vascular amputation was defined as an amputation resulting from a vascular event above the forefoot. Peripheral vascular interventions were classified as interventions for PAD, including peripheral angioplasty or vascular surgery, regardless of the Rutherford stage. The methodology for ascertaining the diagnosis of PAD has been previously described [23].
Assessment of frailty
We assessed the Fried frailty phenotype at baseline and 2 years after enrollment [8, 58]. Unintentional weight loss was defined as a loss of more than 3 kg or 5% of the patient’s body weight within the previous year. Exhaustion was determined by a positive response to the questions on the vitality scale of the 36-Item Short Form Health Survey [59]. Low physical activity was defined using the Taiwanese version of the International Physical Activity Questionnaire-Short Form, which calculated calorie consumption and was based on the lowest 20% for each sex (<685 kcal/week in males and <420 kcal/week in females) [60]. We conducted grip strength tests on each hand three times using a handheld dynamometer (JAMAR; Lafayette Instrument Company, Lafayette, IN, USA) and recorded the average of the strongest hand. Cut-off values were defined according to the sex and body mass index (BMI) criteria provided in the study by Fried et al [25]. We measured gait speed by having participants walk at their usual pace over a 5-meter course and recording the fastest speed of the two trials. The Taiwanese-modified Fried criteria were used to determine the cut-off points [22]. Each component of the frailty phenotype was scored as 1 if present and 0 if absent, resulting in a frailty score ranging from 0 to 5. The participants were categorized into three states based on their scores: frail (3–5 points), pre-frail (1–2 points), and non-frail (0 points). The three frailty states were based on a study by Fried et al. and have been shown to be associated with mortality in hemodialysis populations [8, 25].
Covariates
Demographic, socioeconomic, and smoking status data were collected by reviewing patient medical records. BMI was calculated by dividing weight in kilograms by the square of height in meters. BMI values were classified into four categories: underweight (<18.5 kg/m2), normal weight (18.5–24 kg/m2), overweight (24–27 kg/m2), and obese (>27 kg/m2) according to the criteria suggested for the Asian population [61, 62]. Comorbidities, such as CAD (including angina pectoris, myocardial infarction, positive non-invasive or invasive test results, or those requiring interventions), PAD, CVA, congestive heart failure, diabetes mellitus (DM), hypertension, chronic liver disease, atrial fibrillation, chronic obstructive pulmonary disease, and cancer were recorded according to the diagnosis at the dialysis units, documented by the patient’s primary nephrologist.
Statistical analysis
Baseline characteristics were compared according to frailty status using analysis of variance for normally distributed continuous variables, the Kruskal–Wallis test for non-normally distributed continuous variables, and the χ2 test for categorical variables. We used the Shapiro-Wilk test to examine whether the continuous variable was normally distributed. Logistic regression analysis was performed to determine the factors associated with baseline frailty status, which were categorized into binary variables. Outcomes, including PAD events, were tabulated, stratified by frailty status, and assessed using the Kaplan–Meier method with a log-rank test. For each approach, data were censored in case of death, kidney transplantation, transfer to peritoneal dialysis, or loss to follow-up. Only baseline variables were used as exposures for incident PAD events. Factors associated with CLTI were evaluated using Cox proportional hazards regression models. Multivariate adjustment was performed for factors with P-values < 0.10 in the univariate analysis, including frailty score, age, BMI, education levels, smoking, DM, hypertension, hyperlipidemia, CAD, CVA or ICH, atrial fibrillation, Kt/V, hemoglobin, antiplatelet, and statin. The proportionality assumption was graphically checked using a log-log plot and was found to be acceptable for the selected factors. All P-values were two-tailed, and statistical significance was set at P < 0.05. Statistical analysis was performed using the R language and RStudio version 4.2.2, and the gtsummary package was used.
Data availability statement
The data that support the findings of this study are not publicly available but are available from the corresponding authors (CCW and CWY) upon reasonable request.
Author Contributions
MYH: Research idea and study design; data acquisition; data analysis/interpretation; statistical analysis. CCW: Research idea and study design; data acquisition; data analysis/interpretation; supervision or mentorship. CCL: Data acquisition. CCH: Data acquisition. CHC: Data acquisition. LPD: Data acquisition. CWY: Data acquisition. SYC: Statistical analysis. Each author contributed important intellectual content during manuscript drafting or revision and agreed to be personally accountable for the individual’s own contributions and to ensure that questions pertaining to the accuracy or integrity of any portion of the work, even one in which the author was not directly involved, are appropriately investigated, and resolved, including with documentation in the literature, if appropriate.
Acknowledgments
The authors thank the healthcare professionals at the participating sites and all study participants for their support.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement and Consent
This study protocol was reviewed and approved by the institutional review board, approval number (106-033-E). All patients provided informed written consent before enrollment.
Funding
This study was supported by grants from the National Taiwan University Hospital, Hsin-Chu Branch (107-HCH025, 108-HCH046, 109-HCH001, 109-HCH057, and 109-HCH068) and Ministry of Science and Technology (109-2314-B-002-241-MY3, 112-2314-B-002-30, 112-2314-B-002-MY3, and 111-2314-B-002-288). The funders had no role in the design, data collection, data analysis, and reporting of this study.
References
- 1. de Vinuesa SG, Ortega M, Martinez P, Goicoechea M, Campdera FG, Luño J. Subclinical peripheral arterial disease in patients with chronic kidney disease: prevalence and related risk factors. Kidney Int Suppl. 2005; S44–7. https://doi.org/10.1111/j.1523-1755.2005.09310.x [PubMed]
- 2. O'Hare AM, Glidden DV, Fox CS, Hsu CY. High prevalence of peripheral arterial disease in persons with renal insufficiency: results from the National Health and Nutrition Examination Survey 1999-2000. Circulation. 2004; 109:320–3. https://doi.org/10.1161/01.CIR.0000114519.75433.DD [PubMed]
- 3. Aboyans V, Ricco JB, Bartelink MEL, Björck M, Brodmann M, Cohnert T, Collet JP, Czerny M, De Carlo M, Debus S, Espinola-Klein C, Kahan T, Kownator S, et al, and ESC Scientific Document Group. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018; 39:763–816. https://doi.org/10.1093/eurheartj/ehx095 [PubMed]
- 4. Dormandy J, Belcher G, Broos P, Eikelboom B, Laszlo G, Konrad P, Moggi L, Mueller U. Prospective study of 713 below-knee amputations for ischaemia and the effect of a prostacyclin analogue on healing. Hawaii Study Group. Br J Surg. 1994; 81:33–7. https://doi.org/10.1002/bjs.1800810110 [PubMed]
- 5. Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004; 59:255–63. https://doi.org/10.1093/gerona/59.3.m255 [PubMed]
- 6. Singh M, Stewart R, White H. Importance of frailty in patients with cardiovascular disease. Eur Heart J. 2014; 35:1726–31. https://doi.org/10.1093/eurheartj/ehu197 [PubMed]
- 7. Sergi G, Veronese N, Fontana L, De Rui M, Bolzetta F, Zambon S, Corti MC, Baggio G, Toffanello ED, Crepaldi G, Perissinotto E, Manzato E. Pre-frailty and risk of cardiovascular disease in elderly men and women: the Pro.V.A. study. J Am Coll Cardiol. 2015; 65:976–83. https://doi.org/10.1016/j.jacc.2014.12.040 [PubMed]
- 8. Johansen KL, Chertow GM, Jin C, Kutner NG. Significance of frailty among dialysis patients. J Am Soc Nephrol. 2007; 18:2960–7. https://doi.org/10.1681/ASN.2007020221 [PubMed]
- 9. Ng JK, Kwan BC, Chow KM, Cheng PM, Law MC, Pang WF, Leung CB, Li PK, Szeto CC. Frailty in Chinese Peritoneal Dialysis Patients: Prevalence and Prognostic Significance. Kidney Blood Press Res. 2016; 41:736–45. https://doi.org/10.1159/000450563 [PubMed]
- 10. Lee HJ, Son YJ. Prevalence and Associated Factors of Frailty and Mortality in Patients with End-Stage Renal Disease Undergoing Hemodialysis: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021; 18:3471. https://doi.org/10.3390/ijerph18073471 [PubMed]
- 11. Oki R, Hamasaki Y, Tsuji S, Suzuki K, Tsuneishi S, Imafuku M, Komaru Y, Miyamoto Y, Matsuura R, Doi K, Nangaku M. Clinical frailty assessment might be associated with mortality in incident dialysis patients. Sci Rep. 2022; 12:17651. https://doi.org/10.1038/s41598-022-22483-8 [PubMed]
- 12. Sy J, McCulloch CE, Johansen KL. Depressive symptoms, frailty, and mortality among dialysis patients. Hemodial Int. 2019; 23:239–46. https://doi.org/10.1111/hdi.12747 [PubMed]
- 13. Alfaadhel TA, Soroka SD, Kiberd BA, Landry D, Moorhouse P, Tennankore KK. Frailty and mortality in dialysis: evaluation of a clinical frailty scale. Clin J Am Soc Nephrol. 2015; 10:832–40. https://doi.org/10.2215/CJN.07760814 [PubMed]
- 14. Bao Y, Dalrymple L, Chertow GM, Kaysen GA, Johansen KL. Frailty, dialysis initiation, and mortality in end-stage renal disease. Arch Intern Med. 2012; 172:1071–7. https://doi.org/10.1001/archinternmed.2012.3020 [PubMed]
- 15. Johansen KL, Delgado C, Kaysen GA, Chertow GM, Chiang J, Dalrymple LS, Segal MR, Grimes BA. Frailty Among Patients Receiving Hemodialysis: Evolution of Components and Associations With Mortality. J Gerontol A Biol Sci Med Sci. 2019; 74:380–6. https://doi.org/10.1093/gerona/gly206 [PubMed]
- 16. McAdams-DeMarco MA, Tan J, Salter ML, Gross A, Meoni LA, Jaar BG, Kao WH, Parekh RS, Segev DL, Sozio SM. Frailty and Cognitive Function in Incident Hemodialysis Patients. Clin J Am Soc Nephrol. 2015; 10:2181–9. https://doi.org/10.2215/CJN.01960215 [PubMed]
- 17. Wang Y, Wu X, Hu X, Yang Y. Prevalence of frailty in patients with lower extremity peripheral arterial disease: A systematic review and meta-analysis. Ageing Res Rev. 2022; 82:101748. https://doi.org/10.1016/j.arr.2022.101748 [PubMed]
- 18. Strom JB, Secemsky EA. Seeing the entire elephant: The challenges of frailty assessment for peripheral artery disease. Vasc Med. 2022; 27:258–60. https://doi.org/10.1177/1358863X221088860 [PubMed]
- 19. Al-Damluji MS, Smolderen KG, Meng C, Dai F, Nanna MG, Sumpio B, Henke P, Mena-Hurtado C. Frailty and outcomes following revascularization of lower-extremity peripheral artery disease: Insights from the Vascular Quality Initiative (VQI). Vasc Med. 2022; 27:251–7. https://doi.org/10.1177/1358863X221083701 [PubMed]
- 20. Jakubiak GK, Pawlas N, Cieślar G, Stanek A. Chronic Lower Extremity Ischemia and Its Association with the Frailty Syndrome in Patients with Diabetes. Int J Environ Res Public Health. 2020; 17:9339. https://doi.org/10.3390/ijerph17249339 [PubMed]
- 21. Bielecka-Dabrowa A, Ebner N, Dos Santos MR, Ishida J, Hasenfuss G, von Haehling S. Cachexia, muscle wasting, and frailty in cardiovascular disease. Eur J Heart Fail. 2020; 22:2314–26. https://doi.org/10.1002/ejhf.2011 [PubMed]
- 22. Chen LJ, Chen CY, Lue BH, Tseng MY, Wu SC. Prevalence and Associated Factors of Frailty Among Elderly People in Taiwan. Int J Gerontol. 2014; 8:114–9. https://doi.org/10.1016/j.ijge.2013.12.002
- 23. Hsieh MY, Chuang SY, Lee CK, Luo CM, Cheng CH, Liao MT, Lin PL, Yang TF, Wu CC. Risks and outcomes of critical limb ischemia in hemodialysis patients: a prospective cohort study. Clin Kidney J. 2022; 16:585–95. https://doi.org/10.1093/ckj/sfac263 [PubMed]
- 24. Luo CM, Hsieh MY, Cheng CH, Chen CH, Liao MT, Chuang SY, Wu CC. Association of Frailty With Thrombosis of Hemodialysis Vascular Access: A Prospective Taiwanese Cohort Study. Am J Kidney Dis. 2022; 80:353–63.e1. https://doi.org/10.1053/j.ajkd.2021.12.017 [PubMed]
- 25. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA, and Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001; 56:M146–56. https://doi.org/10.1093/gerona/56.3.m146 [PubMed]
- 26. Lo YL, Hsieh YT, Hsu LL, Chuang SY, Chang HY, Hsu CC, Chen CY, Pan WH. Dietary Pattern Associated with Frailty: Results from Nutrition and Health Survey in Taiwan. J Am Geriatr Soc. 2017; 65:2009–15. https://doi.org/10.1111/jgs.14972 [PubMed]
- 27. Aday AW, Matsushita K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ Res. 2021; 128:1818–32. https://doi.org/10.1161/CIRCRESAHA.121.318535 [PubMed]
- 28. Song P, Rudan D, Zhu Y, Fowkes FJI, Rahimi K, Fowkes FGR, Rudan I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: an updated systematic review and analysis. Lancet Glob Health. 2019; 7:e1020–30. https://doi.org/10.1016/S2214-109X(19)30255-4 [PubMed]
- 29. Rajagopalan S, Dellegrottaglie S, Furniss AL, Gillespie BW, Satayathum S, Lameire N, Saito A, Akiba T, Jadoul M, Ginsberg N, Keen M, Port FK, Mukherjee D, Saran R. Peripheral arterial disease in patients with end-stage renal disease: observations from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Circulation. 2006; 114:1914–22. https://doi.org/10.1161/CIRCULATIONAHA.105.607390 [PubMed]
- 30. Levin SR, Arinze N, Siracuse JJ. Lower extremity critical limb ischemia: A review of clinical features and management. Trends Cardiovasc Med. 2020; 30:125–30. https://doi.org/10.1016/j.tcm.2019.04.002 [PubMed]
- 31. Howard DP, Banerjee A, Fairhead JF, Hands L, Silver LE, Rothwell PM, and Oxford Vascular Study. Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial Events: Implications for Prevention. Circulation. 2015; 132:1805–15. https://doi.org/10.1161/CIRCULATIONAHA.115.016424 [PubMed]
- 32. Foley RN, Parfrey PS, Sarnak MJ. Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol. 1998; 9:S16–23. [PubMed]
- 33. Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998; 32:S112–9. https://doi.org/10.1053/ajkd.1998.v32.pm9820470 [PubMed]
- 34. de Jager DJ, Grootendorst DC, Jager KJ, van Dijk PC, Tomas LM, Ansell D, Collart F, Finne P, Heaf JG, De Meester J, Wetzels JF, Rosendaal FR, Dekker FW. Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA. 2009; 302:1782–9. https://doi.org/10.1001/jama.2009.1488 [PubMed]
- 35. Liu J, Zhang H, Diao Z, Guo W, Huang H, Zuo L, Liu W. Epidemiological analysis of death among patients on maintenance hemodialysis: results from the beijing blood purification quality Control and Improvement Center. BMC Nephrol. 2023; 24:236. https://doi.org/10.1186/s12882-023-03271-6 [PubMed]
- 36. Ocak G, Vossen CY, Rotmans JI, Lijfering WM, Rosendaal FR, Parlevliet KJ, Krediet RT, Boeschoten EW, Dekker FW, Verduijn M. Venous and arterial thrombosis in dialysis patients. Thromb Haemost. 2011; 106:1046–52. https://doi.org/10.1160/TH11-06-0422 [PubMed]
- 37. Casserly LF, Dember LM. Thrombosis in end-stage renal disease. Semin Dial. 2003; 16:245–56. https://doi.org/10.1046/j.1525-139x.2003.16048.x [PubMed]
- 38. Findlay MD, Thomson PC, Fulton RL, Solbu MD, Jardine AG, Patel RK, Stevens KK, Geddes CC, Dawson J, Mark PB. Risk Factors of Ischemic Stroke and Subsequent Outcome in Patients Receiving Hemodialysis. Stroke. 2015; 46:2477–81. https://doi.org/10.1161/STROKEAHA.115.009095 [PubMed]
- 39. Trespalacios FC, Taylor AJ, Agodoa LY, Abbott KC. Incident acute coronary syndromes in chronic dialysis patients in the United States. Kidney Int. 2002; 62:1799–805. https://doi.org/10.1046/j.1523-1755.2002.00638.x [PubMed]
- 40. Okuyama M, Takeuchi H, Uchida HA, Kakio Y, Okuyama Y, Umebayashi R, Wada K, Sugiyama H, Sugimoto K, Rakugi H, Kasahara S, Wada J. Peripheral artery disease is associated with frailty in chronic hemodialysis patients. Vascular. 2018; 26:425–31. https://doi.org/10.1177/1708538118756690 [PubMed]
- 41. Farah BQ, Santos MF, Cucato GG, Kanegusuku H, Sampaio LMM, Monteiro FA, Wolosker N, Puech-Leão P, Correia MA, Ritti-Dias RM. Effect of frailty on physical activity levels and walking capacity in patients with peripheral artery disease: A cross-sectional study. J Vasc Nurs. 2021; 39:84–8. https://doi.org/10.1016/j.jvn.2021.07.001 [PubMed]
- 42. Heikkilä K, Coughlin PA, Pentti J, Kivimäki M, Halonen JI. Physical activity and peripheral artery disease: Two prospective cohort studies and a systematic review. Atherosclerosis. 2019; 286:114–20. https://doi.org/10.1016/j.atherosclerosis.2019.05.008 [PubMed]
- 43. Farber A, Eberhardt RT. The Current State of Critical Limb Ischemia: A Systematic Review. JAMA Surg. 2016; 151:1070–7. https://doi.org/10.1001/jamasurg.2016.2018 [PubMed]
- 44. Kanapuru B, Ershler WB. Inflammation, coagulation, and the pathway to frailty. Am J Med. 2009; 122:605–13. https://doi.org/10.1016/j.amjmed.2009.01.030 [PubMed]
- 45. Folsom AR, Boland LL, Cushman M, Heckbert SR, Rosamond WD, Walston JD. Frailty and risk of venous thromboembolism in older adults. J Gerontol A Biol Sci Med Sci. 2007; 62:79–82. https://doi.org/10.1093/gerona/62.1.79 [PubMed]
- 46. Walston J, McBurnie MA, Newman A, Tracy RP, Kop WJ, Hirsch CH, Gottdiener J, Fried LP, and Cardiovascular Health Study. Frailty and activation of the inflammation and coagulation systems with and without clinical comorbidities: results from the Cardiovascular Health Study. Arch Intern Med. 2002; 162:2333–41. https://doi.org/10.1001/archinte.162.20.2333 [PubMed]
- 47. Yao X, Li H, Leng SX. Inflammation and immune system alterations in frailty. Clin Geriatr Med. 2011; 27:79–87. https://doi.org/10.1016/j.cger.2010.08.002 [PubMed]
- 48. McAdams-DeMarco MA, Ying H, Thomas AG, Warsame F, Shaffer AA, Haugen CE, Garonzik-Wang JM, Desai NM, Varadhan R, Walston J, Norman SP, Segev DL. Frailty, Inflammatory Markers, and Waitlist Mortality Among Patients With End-stage Renal Disease in a Prospective Cohort Study. Transplantation. 2018; 102:1740–6. https://doi.org/10.1097/TP.0000000000002213 [PubMed]
- 49. Stenvinkel P, Heimbürger O, Lindholm B, Kaysen GA, Bergström J. Are there two types of malnutrition in chronic renal failure? Evidence for relationships between malnutrition, inflammation and atherosclerosis (MIA syndrome). Nephrol Dial Transplant. 2000; 15:953–60. https://doi.org/10.1093/ndt/15.7.953 [PubMed]
- 50. Koch M, Kutkuhn B, Grabensee B, Ritz E. Apolipoprotein A, fibrinogen, age, and history of stroke are predictors of death in dialysed diabetic patients: a prospective study in 412 subjects. Nephrol Dial Transplant. 1997; 12:2603–11. https://doi.org/10.1093/ndt/12.12.2603 [PubMed]
- 51. McDermott MM, Polonsky TS, Kibbe MR, Tian L, Zhao L, Pearce WH, Gao Y, Guralnik JM. Racial differences in functional decline in peripheral artery disease and associations with socioeconomic status and education. J Vasc Surg. 2017; 66:826–34. https://doi.org/10.1016/j.jvs.2017.02.037 [PubMed]
- 52. Chernev I, Chernev A. Education Level Among Patients with Major Limb Amputation. Cureus. 2020; 12:e7673. https://doi.org/10.7759/cureus.7673 [PubMed]
- 53. McDermott MM, Spring B, Tian L, Treat-Jacobson D, Ferrucci L, Lloyd-Jones D, Zhao L, Polonsky T, Kibbe MR, Bazzano L, Guralnik JM, Forman DE, Rego A, et al. Effect of Low-Intensity vs High-Intensity Home-Based Walking Exercise on Walk Distance in Patients With Peripheral Artery Disease: The LITE Randomized Clinical Trial. JAMA. 2021; 325:1266–76. https://doi.org/10.1001/jama.2021.2536 [PubMed]
- 54. McDermott MM. Exercise training for intermittent claudication. J Vasc Surg. 2017; 66:1612–20. https://doi.org/10.1016/j.jvs.2017.05.111 [PubMed]
- 55. Kaminski MR, Raspovic A, McMahon LP, Lambert KA, Erbas B, Mount PF, Kerr PG, Landorf KB. Factors associated with foot ulceration and amputation in adults on dialysis: a cross-sectional observational study. BMC Nephrol. 2017; 18:293. https://doi.org/10.1186/s12882-017-0711-6 [PubMed]
- 56. Jaar BG, Plantinga LC, Astor BC, Fink NE, Longenecker C, Tracy RP, Marcovina SM, Powe NR, Coresh J. Novel and traditional cardiovascular risk factors for peripheral arterial disease in incident-dialysis patients. Adv Chronic Kidney Dis. 2007; 14:304–13. https://doi.org/10.1053/j.ackd.2007.04.005 [PubMed]
- 57. K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005; 45:S1–153. [PubMed]
- 58. Johansen KL, Dalrymple LS, Delgado C, Kaysen GA, Kornak J, Grimes B, Chertow GM. Comparison of self-report-based and physical performance-based frailty definitions among patients receiving maintenance hemodialysis. Am J Kidney Dis. 2014; 64:600–7. https://doi.org/10.1053/j.ajkd.2014.03.016 [PubMed]
- 59. Tseng HM, Lu JF, Gandek B. Cultural issues in using the SF-36 Health Survey in Asia: results from Taiwan. Health Qual Life Outcomes. 2003; 1:72. https://doi.org/10.1186/1477-7525-1-72 [PubMed]
- 60. Liou YM, Jwo CJ, Yao KG, Chiang LC, Huang LH. Selection of appropriate Chinese terms to represent intensity and types of physical activity terms for use in the Taiwan version of IPAQ. J Nurs Res. 2008; 16:252–63. https://doi.org/10.1097/01.jnr.0000387313.20386.0a [PubMed]
- 61. Shiwaku K, Anuurad E, Enkhmaa B, Kitajima K, Yamane Y. Appropriate BMI for Asian populations. Lancet. 2004; 363:1077. https://doi.org/10.1016/S0140-6736(04)15856-X [PubMed]
- 62. Huang KC. Obesity and its related diseases in Taiwan. Obes Rev. 2008 (Suppl 1); 9:32–4. https://doi.org/10.1111/j.1467-789X.2007.00435.x [PubMed]