



Introduction
The Gram-negative microaerophilic bacterium Helicobacter pylori (H. pylori) is identified as a key pathogenic agent that can be transmitted from person to person, causing chronic gastritis, peptic ulcer, and gastric cancer [1–3]. Since 1994, the International Agency for Research on Cancer has categorized H. pylori as a Group 1 carcinogenic agent [4]. Research has shown that approximately 50% of the world’s population is infected with H. pylori [5], with a median infection rate of 44.2% in China (95% CI, 43.0–45.5%), representing nearly 600 million infected individuals [6]. Despite recent studies suggested a gradual decline in H. pylori infection rates in numerous developed nations, the prevalence continues to be alarmingly high in the majority of developing countries [5]. Therefore, understanding the risk factors for H. pylori infection is of utmost importance.
Numerous studies have shown that H. pylori infection not only affects the stomach and proximal duodenum, but also the intestinal tract on the anal side. For instance, meta-analyses have found that individuals infected with H. pylori have a higher prevalence of colorectal adenomas and cancers [2, 7–11]. However, the relationship between H. pylori and lower digestive tract (such as colorectal tumors or polyps) remains controversial, with most studies having relatively small sample sizes [12, 13]. Furthermore, no research has yet revealed the association between H. pylori infection and the prevalence of comorbidities in the upper and lower digestive tract.
In summary, we conducted a retrospective analysis of the database containing information on 3867 Chinese patients. The aim of this research was to identify any potential associations between various diseases of the upper and lower digestive tract and H. pylori infection. Additionally, we aimed to identify the risk factors associated with H. pylori infection, thereby facilitated the formulation of evidence-driven decision-making frameworks and targeted intervention strategies.
Results
Relationship between upper digestive tract diseases and H. pylori infection rate
All the 3867 patients in this study have undergone gastroscopy, 2419 cases (62.55%) were diagnosed to have H. pylori infection. Among them, the infection rates of H. pylori in patients with esophageal squamous cell cancer, chronic atrophic gastritis, gastric ulcer, duodenal ulcer, compound ulcer, gastric polyp, gastric MALT lymphoma and gastric cancer were 77.27%, 80.48%, 87.32%, 78.96%, 92.00%, 65.09%, 87.50% and 93.33%, respectively, and there was significant statistical difference between the infected groups and non-infected groups (P < 0.05) (Table 2 and Supplementary Table 1).
Table 2. Comparison of H. pylori infection rate in patients with upper digestive tract diseases.
| Disease | H. pylori infection (+) (n = 2419) | H. pylori infection (−) (n = 1448) | Total (n = 3867) | Infection rate | P-value |
| Reflux esophagitis | 182 | 173 | 355 | 51.27% | P < 0.001 |
| Esophagus cancer | 34 | 10 | 44 | 77.27% | 0.042* |
| Chronic atrophic gastritis | 169 | 41 | 210 | 80.48% | P < 0.001 |
| Gastric ulcer | 62 | 9 | 71 | 87.32% | P < 0.001 |
| Duodenal ulcer | 259 | 69 | 328 | 78.96% | P < 0.001 |
| Compound ulcer | 23 | 2 | 25 | 92.00% | 0.002** |
| Gastric polyp | 783 | 420 | 1203 | 65.09% | 0.029* |
| Gastric MALT lymphoma | 14 | 2 | 16 | 87.50% | 0.039* |
| Gastric cancer | 28 | 2 | 30 | 93.33% | P < 0.001 |
Relationship between lower digestive tract diseases and H. pylori infection rate
Among the 3867 patients included in this study, 2875 patients underwent colonoscopy either simultaneously or within three months. Among them, the infection rates of H. pylori in colorectal polyp and colorectal adenocarcinoma patients were 63.28% and 75.76%, respectively, and there was significant statistical difference between the infected groups and non-infected groups (P < 0.05) (Table 3 and Supplementary Table 2).
Table 3. Comparison of H. pylori infection rate in patients with lower digestive tract diseases.
| Disease | H. pylori infection (+) (n = 1765) | H. pylori infection (−) (n = 1110) | Total (n = 2875) | Infection rate | P-value |
| Colorectal polyp | 1308 | 759 | 2067 | 63.28% | 0.001** |
| Colorectal cancer | 75 | 24 | 99 | 75.76% | 0.003** |
| Inflammatory bowel disease | 19 | 12 | 31 | 61.29% | 0.991 |
Relationship between upper and lower digestive tract comorbidities and H. pylori infection rate
The study included a total of 2875 patients who underwent gastroenteroscopy during the same period, we also analyzed the relationship between H. pylori infection and comorbidities of the upper and lower digestive tract. The H. pylori infection rates among patients with chronic atrophic gastritis and colorectal polyp, peptic ulcer and colorectal polyp, gastric polyp and colorectal polyp, as well as chronic atrophic gastritis and colorectal adenocarcinoma were found to be 79.85%, 79.72%, 66.24%, and 92.86% respectively, and the infection rate in the infected groups was significantly higher than that in the non-infected groups (P < 0 .05) (Table 4).
Table 4. Comparison of H. pylori infection rate in patients with upper and lower digestive tract comorbidities.
| Disease | H. pylori infection (+) (n = 1765) | H. pylori infection (−) (n = 1110) | Total (n = 2875) | Infection rate | P-value |
| Reflux esophagitis and Colorectal polyp | 101 | 100 | 201 | 50.25% | 0.001** |
| Esophagus cancer and Colorectal polyp | 4 | 3 | 7 | 57.14% | P > 0.05 |
| Chronic atrophic gastritis and Colorectal polyp | 107 | 27 | 134 | 79.85% | P < 0.001 |
| Peptic ulcer and Colorectal polyp | 169 | 43 | 212 | 79.72% | P < 0.001 |
| Gastric polyp and Colorectal polyp | 471 | 240 | 711 | 66.24% | 0.002** |
| Gastric cancer and Colorectal polyp | 5 | 1 | 6 | 83.33% | P > 0.05 |
| Reflux esophagitis and Colorectal cancer | 8 | 3 | 11 | 72.73% | P > 0.05 |
| Chronic atrophic gastritis and Colorectal cancer | 13 | 1 | 14 | 92.86% | 0.015* |
| Peptic ulcer and Colorectal cancer | 8 | 1 | 9 | 88.89% | P > 0.05 |
| Gastric polyp and Colorectal cancer | 27 | 8 | 35 | 77.14% | P > 0.05 |
Independent risk factors related to H. pylori infection
Figure 1 details the results of the logistic regression analysis on the study population. It reveals a significant correlation between age, marital status, and fasting blood-glucose with the risk of H. pylori infection. The variables that were significant in univariate analysis (P < 0.05) were further examined in multivariate analysis. The findings indicate that age and being married are independent risk factors for H. pylori infection (Table 5).
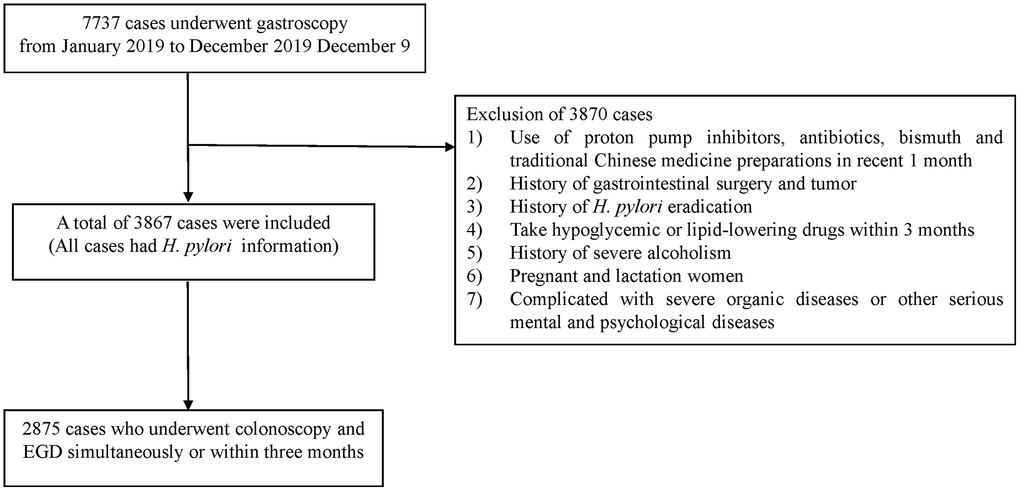
Figure 1. Patient flow chart.
Table 5. Multivariate analysis of H. pylori infection.
| Variables | OR (95% CI) | P-value |
| Married | 1.435 (1.042–1.977) | 0.027* |
| Age | 1.007 (1.001–1.013) | 0.022* |
| Fasting blood-glucose | 1.028 (0.971–1.087) | 0.671 |
Discussion
The relationship between H. pylori infection and upper digestive tract diseases has been extensively studied. H. pylori infection could cause histological, chronic and active inflammation, and the inflammatory response will be reduced after H. pylori eradication [14]. Therefore, H. pylori has been identified as a pathogenic factor that directly causes chronic gastritis and a Class I biological carcinogenic factor in gastric cancer [1]. The underlying mechanisms primarily involve inflammation, reduced acidity, heightened gastrin levels, and a weakened mucosal barrier function [2, 7–11, 15]. In this respect, our study also reached a similar conclusion: the infection rate of H. pylori increased significantly in patients with esophageal squamous cell carcinoma, chronic atrophic gastritis, gastric ulcer, duodenal ulcer, gastric MALT lymphoma and gastric cancer, and the differences were statistically significant compared with the non-infected group. But the relationship between H. pylori and lower digestive tract diseases is less definitive.
Recently, emerging epidemiologic studies released the connection between H. pylori infection and lower digestive tract diseases, particularly colorectal polyp and colorectal cancer. However, these findings remain inconclusive [16–19]. This may be partly attributed to differences in H. pylori detection methods, study regions and participant races, as well as small sample sizes. In our study, a relatively large sample size (2875) of patients underwent colonoscopy, among which, 1765 patients were identified by RUC as being infected with H. pylori, and the results showed that H. pylori infection was positively correlated with the prevalence of colorectal polyps and colorectal cancer.
The association between H. pylori infection and colorectal adenoma as well as colorectal cancer may be attributed to the following reasons: prolonged H. pylori infection may precipitate chronic atrophic gastritis, consequently impeding gastric acid secretion and disrupting the equilibrium of gastrointestinal flora [20, 21], this disruption can either trigger hypergastrinemia, stimulate the proliferation of colorectal mucosa [22], or ultimately progress to colorectal cancer. Concurrently, H. pylori infection can promote the expression of COX-2, whose pivotal role in initiating, progressing, enabling invasion, and facilitating metastasis of colorectal tumors is well-established [23]. Furthermore, studies have documented a heightened positivity rate of H. pylori DNA in colon cancer mucosa compared to normal mucosa [24], implying that H. pylori may directly provoke intestinal mucosa and induce the occurrence of colorectal lesions.
It is noteworthy that upper and lower gastrointestinal comorbidities are frequently encountered in clinical practice, however, the intricate relationship between these conditions and H. pylori infection remains unclear, which is also what we focused on in this study. Our study found that the H. pylori infection rate of patients with chronic atrophic gastritis combined with colon cancer or colon polyp was significantly higher than that of the non-comorbidities group; meanwhile, the H. pylori infection rate of patients with peptic ulcer or gastric polyp combined with colorectal polyp was also higher than that of the non-comorbidities group. This innovative discovery indicated that gastric mucosa colonization of H. pylori not only causes diseases of the upper digestive tract such as chronic atrophic gastritis, but may also affect intestinal health at the same time, this reminds us that when patients are found to have upper digestive tract diseases caused by H. pylori infection, it is advisable for them to undergo regular colonoscopy, pathological biopsy, and other monitoring means, especially when they have lower digestive tract symptoms.
Numerous clinical studies have shown that the main risk factors for H. pylori infection are related to family living conditions, lifestyle habits, and environmental factors, age and microbiota. Interestingly, our study has uncovered a significant finding: age and marital status may serve as independent risk factors for H. pylori infection. As age increases, the immune defense function of the human body also evolves. Simultaneously, the cumulative effect of other risk factors, including adverse family living conditions, smoking and drinking habits, and other unhealthy lifestyle practices, heighten the risk of H. pylori infection. The risk of H. pylori infection is significantly higher among married individuals compared to singles. This may be attributed to the high H. pylori infection rates in China and the oral-to-oral, stomach-to-oral, or fecal-to-oral transmission within families.
This study also has the following limitations. First, our data was derived from a single center in China. Therefore, the generalizability of our findings needs to be validated among other populations. Additionally, in this study, only RUT method was used to detect H. pylori infection and all the samples were collected from the gastric antrum, the result of RUT may be affected by many factors, such as the number and site of biopsies taken, the drugs taken by the patient recently (H2 receptor antagonists, proton pump inhibitors, etc.) [25]. Lastly, the long-term impact of H. pylori infection duration on digestive tract diseases needs to be further explored.
Conclusion
This study further revealed the H. pylori infection was closely related to lower digestive tract diseases, as well as upper and lower gastrointestinal comorbidities. Additionally, being married and advancing age may be independent risk factors for H. pylori infection. This is crucial for the management of H. pylori infection and the treatment and prevention of gastrointestinal diseases.
Materials and Methods
Study area
The study was carried out at the Fifth Affiliated Hospital of Sun Yat-sen University, which is situated in Xiangzhou District of Zhuhai City, Guangdong Province, China. The hospital serves the local residents of Xiangzhou District and the surrounding regions, catering to a population of approximately 1.4 million.
Study design and period
The cross-sectional study design was implemented among patients who underwent gastroscopy during their hospitalization between January 2019 and December 2019.
Study population
During the study period, 7737 cases underwent gastroscopy. However, 3870 subjects were excluded due to the following reasons: (1) usage of proton pump inhibitors, antibiotics, bismuth, and traditional Chinese medicine preparations within the past month; (2) a history of gastrointestinal surgery and tumor; (3) a history of H. pylori eradication; (4) intake of hypoglycemic or lipid-lowering drugs within three months; (5) a history of severe alcoholism; and (6) pregnancy or lactation status; (7) presence of severe organic diseases or other serious mental and psychological diseases. Consequently, 3867 cases were included in the analysis. Additionally, 2875 subjects who had undergone colonoscopy and EGD simultaneously or within three months were included in the study (Figure 1).
Data collection
The data on social demographics, clinical factors (including sex, nationality, marital status, smoking history, drinking history, living area, age, BMI, glycosylated hemoglobin, fasting blood glucose, total cholesterol, triglyceride), and gastrointestinal endoscopy results were collected from 3867 subjects who met the admission criteria. The endoscopic procedures were carried out by at least one or two experienced gastroscopists. The endoscopic findings were recorded in the endoscopy center database using a descriptive format. The main diagnostic criteria for digestive tract diseases were based on endoscopic and pathological findings. 3867 subjects had available H. pylori information detected by rapid urease test (RUT).
Data analysis and interpretation
The data were entered and analyzed using SPSS version 23.0, produced by SPSS in Chicago, IL, USA. Based on the results of the RUT test, the patients were divided into two groups: the H. pylori positive group (2419 cases) and the negative group (1448 cases). For continuous variables, the mean ± standard deviation (SD) was calculated, while categorical variables were reported as frequency (%). The Chi-squared test and Mann-Whitney U-test were utilized to compare groups.
A univariate logistic regression analysis was conducted to assess the correlation between H. pylori infection and digestive tract diseases. Variables with a P-value less than 0.05 were selected for further multivariate analysis. The results are presented as odds ratio (OR) and 95% confidence interval (CI). All two-tailed P-values less than 0.05 were considered significant.
Supplementary Materials
Author Contributions
The research was designed and conceived by XL, MG, and JL. WZ and YX were responsible for data analysis and statistical analysis. The specimens were collected by YH, YL, ZZ, and LL. JL contributed to technical support and manuscript revision.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement and Consent
Ethical clearance was obtained from the Ethical Review Board of the Fifth Affiliated Hospital of Sun Yat-sen University (IRB2021-K58-1). The informed consent was waived, as we solely analyzed de-identified data.
Funding
We acknowledge the generous support of the Department of Gastroenterology, Fifth Affiliated Hospital of Sun Yat-sen University. This study was supported by grants from the Foundation of Zhuhai Science and Technology Plan Project (20181117E030040).
References
- 1. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984; 1:1311–5. https://doi.org/10.1016/s0140-6736(84)91816-6 [PubMed]
- 2. Correa P. Human gastric carcinogenesis: a multistep and multifactorial process--First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res. 1992; 52:6735–40. [PubMed]
- 3. Sugano K, Tack J, Kuipers EJ, Graham DY, El-Omar EM, Miura S, Haruma K, Asaka M, Uemura N, Malfertheiner P, and faculty members of Kyoto Global Consensus Conference. Kyoto global consensus report on Helicobacter pylori gastritis. Gut. 2015; 64:1353–67. https://doi.org/10.1136/gutjnl-2015-309252 [PubMed]
- 4. Møller H, Heseltine E, Vainio H. Working group report on schistosomes, liver flukes and Helicobacter pylori. Int J Cancer. 1995; 60:587–9. https://doi.org/10.1002/ijc.2910600502 [PubMed]
- 5. Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, Malfertheiner P, Graham DY, Wong VWS, Wu JCY, Chan FKL, Sung JJY, Kaplan GG, Ng SC. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology. 2017; 153:420–9. https://doi.org/10.1053/j.gastro.2017.04.022 [PubMed]
- 6. Ren S, Cai P, Liu Y, Wang T, Zhang Y, Li Q, Gu Y, Wei L, Yan C, Jin G. Prevalence of Helicobacter pylori infection in China: A systematic review and meta-analysis. J Gastroenterol Hepatol. 2022; 37:464–70. https://doi.org/10.1111/jgh.15751 [PubMed]
- 7. Koike T, Ohara S, Sekine H, Iijima K, Kato K, Shimosegawa T, Toyota T. Helicobacter pylori infection inhibits reflux esophagitis by inducing atrophic gastritis. Am J Gastroenterol. 1999; 94:3468–72. https://doi.org/10.1111/j.1572-0241.1999.01593.x [PubMed]
- 8. Laine L, Takeuchi K, Tarnawski A. Gastric mucosal defense and cytoprotection: bench to bedside. Gastroenterology. 2008; 135:41–60. https://doi.org/10.1053/j.gastro.2008.05.030 [PubMed]
- 9. Watari J, Chen N, Amenta PS, Fukui H, Oshima T, Tomita T, Miwa H, Lim KJ, Das KM. Helicobacter pylori associated chronic gastritis, clinical syndromes, precancerous lesions, and pathogenesis of gastric cancer development. World J Gastroenterol. 2014; 20:5461–73. https://doi.org/10.3748/wjg.v20.i18.5461 [PubMed]
- 10. Kountouras J, Polyzos SA, Katsinelos P, Zeglinas C, Kountouras C, Vardaka E, Lazaraki G, Gavalas E, Deretzi G. Potential molecular aspects of Helicobacter pylori-related hyperplastic polyp development and progression. Eur J Gastroenterol Hepatol. 2016; 28:851–2. https://doi.org/10.1097/MEG.0000000000000625 [PubMed]
- 11. Lanas A, Chan FKL. Peptic ulcer disease. Lancet. 2017; 390:613–24. https://doi.org/10.1016/S0140-6736(16)32404-7 [PubMed]
- 12. ChangxiChen, Mao Y, Du J, Xu Y, Zhu Z, Cao H. Helicobacter pylori infection associated with an increased risk of colorectal adenomatous polyps in the Chinese population. BMC Gastroenterol. 2019; 19:14. https://doi.org/10.1186/s12876-018-0918-4 [PubMed]
- 13. Wang M, Kong WJ, Zhang JZ, Lu JJ, Hui WJ, Liu WD, Kang XJ, Gao F. Association of Helicobacter pylori infection with colorectal polyps and malignancy in China. World J Gastrointest Oncol. 2020; 12:582–91. https://doi.org/10.4251/wjgo.v12.i5.582 [PubMed]
- 14. Dooley CP, Cohen H, Fitzgibbons PL, Bauer M, Appleman MD, Perez-Perez GI, Blaser MJ. Prevalence of Helicobacter pylori infection and histologic gastritis in asymptomatic persons. N Engl J Med. 1989; 321:1562–6. https://doi.org/10.1056/NEJM198912073212302 [PubMed]
- 15. Tulassay Z, Herszényi L. Gastric mucosal defense and cytoprotection. Best Pract Res Clin Gastroenterol. 2010; 24:99–108. https://doi.org/10.1016/j.bpg.2010.02.006 [PubMed]
- 16. Liou JM, Lin JW, Huang SP, Lin JT, Wu MS. Helicobacter pylori infection is not associated with increased risk of colorectal polyps in Taiwanese. Int J Cancer. 2006; 119:1999–2000. https://doi.org/10.1002/ijc.22050 [PubMed]
- 17. Sonnenberg A, Genta RM. Helicobacter pylori is a risk factor for colonic neoplasms. Am J Gastroenterol. 2013; 108:208–15. https://doi.org/10.1038/ajg.2012.407 [PubMed]
- 18. Liu IL, Tsai CH, Hsu CH, Hu JM, Chen YC, Tian YF, You SL, Chen CY, Hsiao CW, Lin CY, Chou YC, Sun CA. Helicobacter pylori infection and the risk of colorectal cancer: a nationwide population-based cohort study. QJM. 2019; 112:787–92. https://doi.org/10.1093/qjmed/hcz157 [PubMed]
- 19. Ralser A, Dietl A, Jarosch S, Engelsberger V, Wanisch A, Janssen KP, Middelhoff M, Vieth M, Quante M, Haller D, Busch DH, Deng L, Mejías-Luque R, Gerhard M. Helicobacter pylori promotes colorectal carcinogenesis by deregulating intestinal immunity and inducing a mucus-degrading microbiota signature. Gut. 2023; 72:1258–70. https://doi.org/10.1136/gutjnl-2022-328075 [PubMed]
- 20. Robertson DJ, Sandler RS, Ahnen DJ, Greenberg ER, Mott LA, Cole BF, Baron JA. Gastrin, Helicobacter pylori, and colorectal adenomas. Clin Gastroenterol Hepatol. 2009; 7:163–7. https://doi.org/10.1016/j.cgh.2008.09.006 [PubMed]
- 21. Chao C, Hellmich MR. Gastrin, inflammation, and carcinogenesis. Curr Opin Endocrinol Diabetes Obes. 2010; 17:33–9. https://doi.org/10.1097/MED.0b013e328333faf8 [PubMed]
- 22. Watson SA, Grabowska AM, El-Zaatari M, Takhar A. Gastrin - active participant or bystander in gastric carcinogenesis? Nat Rev Cancer. 2006; 6:936–46. https://doi.org/10.1038/nrc2014 [PubMed]
- 23. Kapetanakis N, Kountouras J, Zavos C, Polyzos SA, Kouklakis G, Venizelos I, Nikolaidou C, Vardaka E, Paikos D, Katsinelos P, Romiopoulos I. Helicobacter pylori infection and colorectal carcinoma: pathologic aspects. J Gastrointest Oncol. 2012; 3:377–9. https://doi.org/10.3978/j.issn.2078-6891.2012.041 [PubMed]
- 24. Hong SN, Lee SM, Kim JH, Lee TY, Kim JH, Choe WH, Lee SY, Cheon YK, Sung IK, Park HS, Shim CS. Helicobacter pylori infection increases the risk of colorectal adenomas: cross-sectional study and meta-analysis. Dig Dis Sci. 2012; 57:2184–94. https://doi.org/10.1007/s10620-012-2245-x [PubMed]
- 25. Uotani T, Graham DY. Diagnosis of Helicobacter pylori using the rapid urease test. Ann Transl Med. 2015; 3:9. https://doi.org/10.3978/j.issn.2305-5839.2014.12.04 [PubMed]
Social-demographic, clinical and related characteristics of the study participants
A total of 3,867 patients were included in the study, consisting of 1,885 male patients and 1,982 female patients. Based on the results of RUT, the patients were categorized into H. pylori infection positive and negative group. Subsequently, a univariate logistic regression analysis was conducted to compare the differences in gender, nationality, marital status, smoking history, drinking history, living area, age, BMI, glycosylated hemoglobin, fasting blood glucose, total cholesterol, and triglyceride levels between the two groups. According to analysis, a significant difference was observed in marital status between the two groups (P < 0.05). The infection rate of H. pylori in married individuals was 63.08%, which was significantly higher than that in single individuals. However, there were no significant differences in gender, nationality, smoking history, drinking history, and living area between the H. pylori positive and negative groups (P > 0.05) (Table 1). Additional, significant differences were observed in age and fasting blood glucose levels between the two groups (P < 0.05). In terms of age, the mean ± SD age of patients in the H. pylori positive group was 53.07 ± 11.55 years, while the mean ± SD age of patients in the negative group was 51.82 ± 11.82 years, there was significant statistical significance between the two groups (P < 0.001). In terms of fasting blood glucose, the mean ± SD glucose level of patients in the H. pylori positive group was 5.28 ± 1.16 mmol/L, while 5.22 ± 1.23 mmol/L in the negative group. The difference in fasting blood glucose levels between the two groups was also statistically significant (P < 0.045). Nonetheless, there were no significant differences in BMI, glycosylated hemoglobin, total cholesterol, and triglyceride levels between the H. pylori positive and negative group (P > 0.05) (Table 1).
Table 1. Social demographic, clinical and other related characteristics of study participants.
(n = 3867)
(n = 2419)
(n = 1448)