



Introduction
As one of the most universal malignancies of head and neck with poor prognosis and increasing incidence rate worldwide [1], oral carcinoma features distinct geographic disparity regarding its morbidity and prevalence across the world [2]. Its five-year rate of survival is around 63% [3]. The most frequently occurring cancer in the head and neck region is oral squamous cell carcinoma (OSCC), which represents 90% of entire oral carcinomas [4]. Management of oral cancer is based on surgical resection with or without adjuvant radiotherapy or chemoradiotherapy (CRT) [5]. Recent studies also showed that immunotherapy with immune checkpoint inhibitors (ICIs) also exhibited a marked tumor regression effect in some selected patients with OSCC [6, 7]. Although the treatment methods including ICIs have been applied, the prognosis of oral cancer is not substantially improved in the past several decades. Prediction of the prognosis is of major importance in oral cancer and biomarkers can provide guides to form personally optimized treatments of the disease [8]. Therefore, detection and identification of reliable and cost-effective biomarkers is urgently needed for oral cancer.
Parameters derived from the peripheral blood are important sources of biomarkers for oral cancer, including ratio of neutrophils to lymphocytes [9], ratio of platelets to lymphocytes [10], ratio of lymphocytes to monocytes [11], as well as prognostic nutritional index (PNI) [12, 13]. Also called Onodera’s PNI, the PNI indicator is computed from the overall quantity of peripheral blood lymphocytes and serum albumin [14]. PNI is calculated on the formula: 10 × serum level of albumin (g/dl) + 0.005 × peripheral blood quantity (per mm3) of lymphocytes. PNI is capable of reflecting host’s immune and trophic statuses. Previous studies have reported that low PNI played a prognostic role in diverse carcinomas, such as esophageal squamous cell carcinomas [15], gastrointestinal stromal tumors [16], hepatocellular carcinoma [17], non-small cell lung cancer [18], and glioma [19]. Many studies [12, 13, 20–27] have investigated PNI’s prognostic significance to oral cancer prognosis as well. However, the results were not consistent. Therefore, to systemically and comprehensively investigate how prognostically significant PNI was in oral carcinoma, we conducted the present meta-analysis based on the latest retrieved data.
Results
Literature search process
As shown in Figure 1, the number of records identified by initial literature retrieval totaled 216 and following elimination of duplicate items, 112 studies were retained for subsequent examination. Through abstract and title screening, ninety-two articles were excluded, while the remaining 20 studies were evaluated via full-text reading. Subsequently, 10 of them were discarded due to the fact that no survival data provided (n=5), not on oral cancer (n=3), and not reported on PNI (n=2). Finally, ten studies with 3,130 patients [12, 13, 20–27] were enrolled in the present meta-analysis (Figure 1).
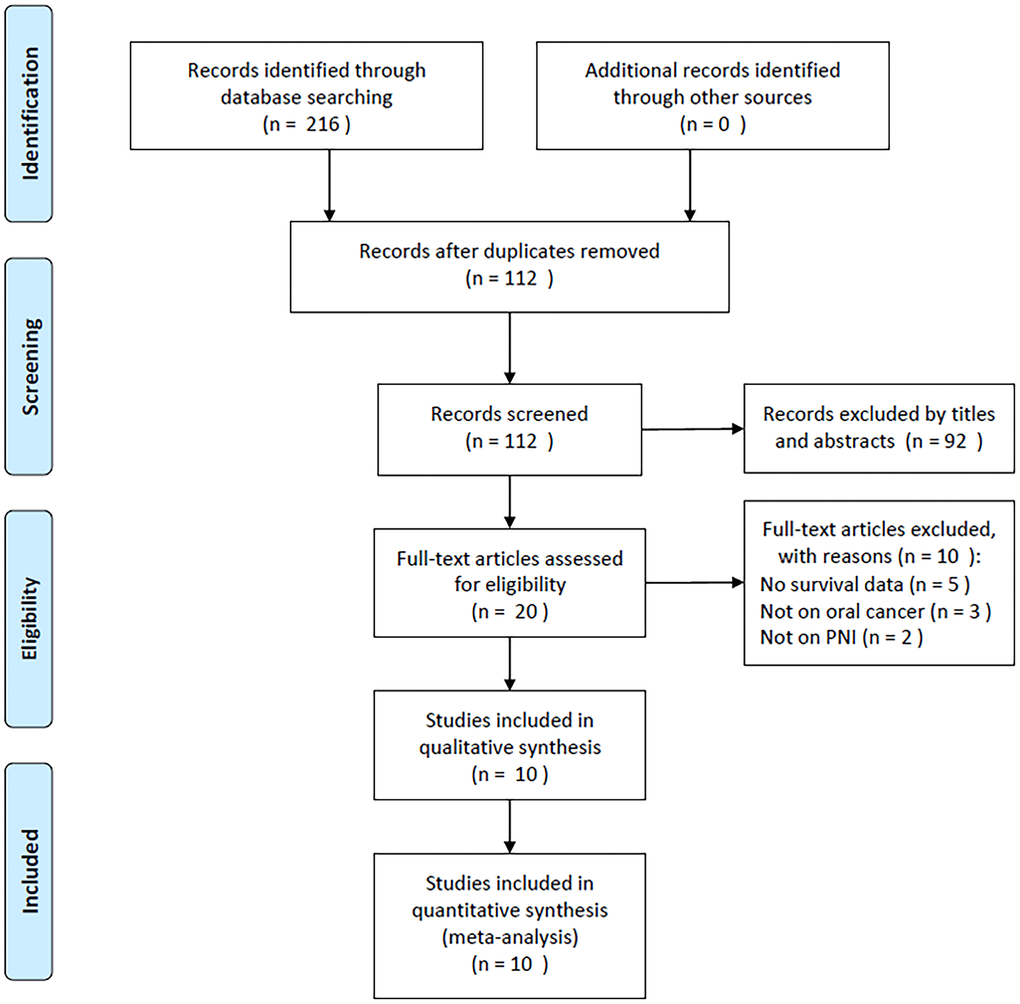
Figure 1. PRISMA flow chart showing selection of articles for review.
Characteristics of included studies
Table 1 demonstrates the baseline traits for the enrolled studies [12, 13, 20–27]. The years of publication ranged between 2020–2022 for these studies. Five studies were conducted in Japan [20–22, 25, 27], four in China [12, 13, 23, 26], and one in Taiwan [24]. Eight studies were published in English language [12, 13, 20–22, 24, 25, 27] and two in Chinese [23, 26]. All studies [12, 13, 20–27] were of retrospective design. Overall sample size was 3,130, varying between 47–1,395. Eight studies included patients with OSCC [13, 20–26], whereas 2 studies recruited oral cancer patients [12, 27]. Eight studies were conducted in single center [12, 20–24, 26, 27] and two studies were multicenter studies [13, 25]. The threshold scope for PNI was 42.685–52.44, with a median of 48.9. Threshold determination was accomplished based on the receiver operating characteristic (ROC) curve in 8 studies [12, 20–26]. Meanwhile, one study used the X-tile software [13], and one study referred to literature [27]. Nine studies reported PNI’s role in prognosticating OS outcome [12, 13, 20, 22–27], six studies provided the data of PNI for DFS prognosis [13, 20, 22, 24, 25, 27], and 2 works reported PNI’s correlation with CSS [20, 21]. The enrolled studies had NOS scores varying between 7–9, and the median value was 8, which indicated that all included studies were of high quality. In the subgroup analysis shown below, PNI cut-off value = 49 and sample size =150 were used to divide into two group. These two values were selected in according to the median value of PNI and sample size. These two values are close to the median value in each category.
Table 1. The baseline characteristics of the included studies.
| Study | Year | Country/region | Sample size | Age (year) Median (range) | Sex (M/F) | Cancer type | Clinical stage | Study period | Study center | Treatment | PNI cut-off value | Cut-off determination | Survival endpoints | Survival analysis | NOS score | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bao, X. | 2020 | China | 1,395 | 57.23 (20-80) | 878/517 | OC | I-IV | 2007-2018 | Single center | Mixed | 49.3 | ROC curve | OS | Multivariate | 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wu, X. | 2020 | China | 333 | ≤60: 133 >60: 200 | 175/158 | OSCC | I-IV | 2011-2018 | Multicenter | Surgery | 47.4 | X-tile software | OS, DFS | Multivariate | 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yoshida, R. | 2020 | Japan | 47 | 79 (45-90) | 23/24 | OSCC | III-IV | 2004-2011 | Single center | CRT | 42.685 | ROC curve | OS, DFS, CSS | Multivariate | 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yoshimura, T. | 2020 | Japan | 103 | 68 (59-77) | 61/42 | OSCC | I-IV | 2009-2015 | Single center | Surgery | 50.8 | ROC curve | CSS | Multivariate | 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abe, A. | 2021 | Japan | 102 | 65.6 | 73/29 | OSCC | I-IV | 2008-2019 | Single center | Surgery | 42.9 | ROC curve | OS, DFS | Multivariate | 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Duan, F. | 2021 | China | 60 | 62.23 | 36/24 | OSCC | I-IV | 2019-2021 | Single center | Surgery | 48.5 | ROC curve | OS | Multivariate | 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fang, K. H. | 2021 | Taiwan | 360 | 59 (31-88) | 325/35 | OSCC | I-IV | 2007-2017 | Single center | Surgery | 51.75 | ROC curve | OS, DFS | Multivariate | 9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Watabe, Y. | 2021 | Japan | 110 | 68 | 61/49 | OSCC | I-IV | 2004-2012 | Multicenter | Surgery | 52.44 | ROC curve | OS, DFS | Multivariate | 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Xia, X. | 2021 | China | 437 | 61.5 (21-83) | 289/148 | OSCC | I-IV | 2015-2017 | Single center | Surgery | 46.23 | ROC curve | OS | Univariate | 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Kubota, K. | 2022 | Japan | 183 | 66 (26-93) | 103/80 | OC | I-IV | 2005-2017 | Single center | Mixed | 52.44 | Literature | OS, DFS | Multivariate | 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OC, oral cancer; OSCC, oral squamous cell carcinoma; ROC, receiver operating characteristic; OS, overall survival; DFS, disease-free survival; NOS, Newcastle-Ottawa Scale; CSS, cancer-specific survival; M, male; F, female; CRT, chemoradiotherapy. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Prognostic role of PNI for OS in oral cancer
PNI was reported to be prognostically significant for OS of oral cancer in 9 studies involving 3,027 patients [12, 13, 20, 22–27]. We adopted a random-effects model since the heterogeneity was significant (I2=86.8%, Ph=0.000; Table 2 and Figure 2). As indicated by the pooled results of HR=2.44, 95%CI=1.45–4.12, p=0.001, a low PNI was linked significantly to inferior OS in oral cancer. We further performed subgroup analysis, as shown in Table 2, a low PNI was still a significant OS biomarker independent of study center, sample size, TNM stage, type of survival analysis, cut-off value, or method for threshold identification.
Table 2. Subgroup analysis of PNI for OS in patients with oral cancer.
| Subgroup factors | No. of studies | No. of patients | Effect model | HR (95%CI) | p | Heterogeneity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I2(%) | Ph | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total | 9 | 3,027 | Random | 2.44(1.45-4.12) | 0.001 | 86.8 | 0.000 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Geographical regions | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Japan | 4 | 442 | Fixed | 4.01(2.34-6.87) | <0.001 | 0 | 0.908 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| China | 4 | 2,225 | Random | 1.77(0.81-3.82) | 0.150 | 92.8 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Taiwan | 1 | 360 | - | 2.19(1.38-3.47) | 0.001 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sample size | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤150 | 4 | 319 | Fixed | 2.66(1.71-4.15) | <0.001 | 35.4 | 0.200 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >150 | 5 | 2,708 | Random | 2.09(1.05-4.19) | 0.037 | 91.8 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cancer type | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OSCC | 7 | 1,449 | Fixed | 2.66(2.12-3.33) | <0.001 | 13.8 | 0.324 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OC | 2 | 1,578 | Random | 1.59(0.36-7.04) | 0.541 | 83.9 | 0.013 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Study center | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multicenter | 2 | 443 | Fixed | 2.49(1.49-4.17) | 0.001 | 35.3 | 0.214 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single center | 7 | 2,584 | Random | 2.31(1.26-4.23) | 0.007 | 89.1 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TNM stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I-IV | 8 | 2,980 | Random | 2.34(1.34-4.07) | 0.003 | 87.6 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III-IV | 1 | 47 | - | 3.57(1.50-8.47) | 0.004 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatment | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Surgery | 6 | 1,402 | Fixed | 2.60(2.06-3.29) | <0.001 | 23.0 | 0.261 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mixed | 2 | 1,578 | Random | 1.59(0.36-7.04) | 0.541 | 83.9 | 0.013 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CRT | 1 | 47 | - | 3.57(1.50-8.47) | 0.004 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PNI cut-off value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤49 | 5 | 979 | Fixed | 2.77(2.14-3.60) | <0.001 | 18.5 | 0.297 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >49 | 4 | 2,048 | Random | 2.10(0.88-4.99) | 0.094 | 86.9 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cut-off determination | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ROC curve | 7 | 2,511 | Random | 2.38(1.27-4.45) | 0.007 | 89.2 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| X-tile/literature | 2 | 516 | Fixed | 2.48(1.52-4.04) | <0.001 | 0 | 0.426 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Survival analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multivariate | 8 | 2,590 | Random | 1.30(1.10-1.55) | 0.003 | 83.3 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Univariate | 1 | 437 | - | 3.33(2.25-4.93) | <0.001 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OC, oral cancer; OSCC, oral squamous cell carcinoma; ROC, receiver operating characteristic; OS, overall survival; CRT, chemoradiotherapy. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
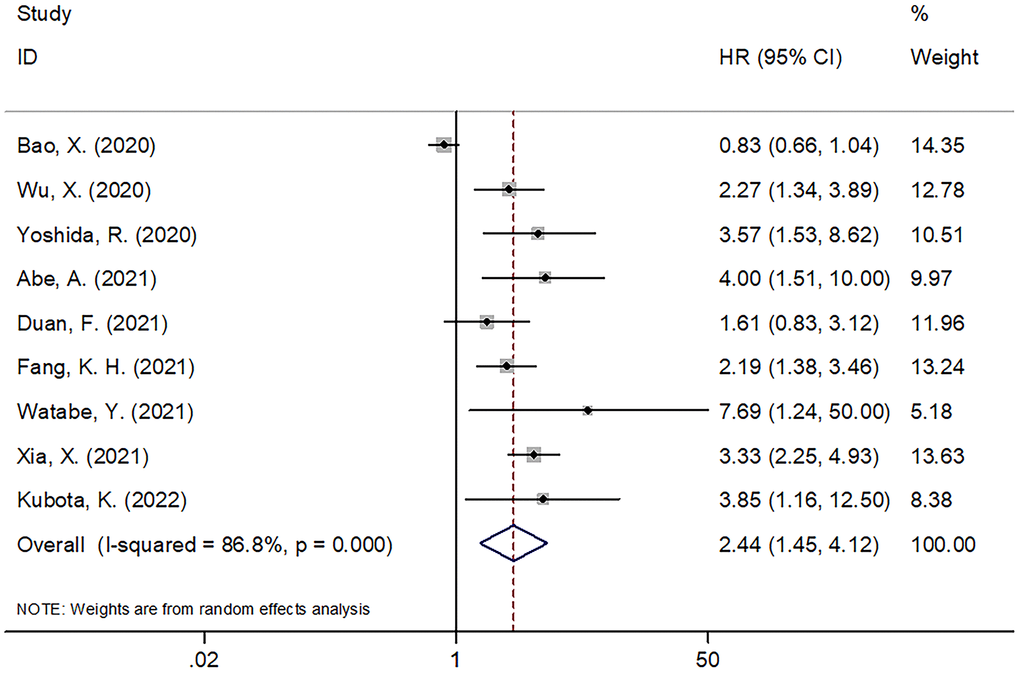
Figure 2. The forest plot of the association between PNI and OS in patients with oral cancer.
Prognostic significance of PNI for DFS and CSS in oral cancer
Six studies with 1,135 patients [13, 20, 22, 24, 25, 27] provided the data on PNI and DFS for the oral carcinoma population. Since the heterogeneity (I2=24.2, Ph=0.252) was insignificant, we chose a fixed-effects model. As displayed in Table 3 plus Figure 3, the pooled HR was 1.92, while the 95% CIs were 1.53–2.42 (p<0.001), suggesting that a low PNI was connected to shortened DFS in oral cancer. As implied by subgroup analysis, a low PNI was still a significant DFS predictor in various subgroups of sample size, cancer type, study center, geographical locations, TNM stage, treatment method, threshold and method for identifying threshold (Table 3). Two studies including 150 patients [20, 21] analyzed PNI’s prognostic value for CSS. According to Figure 4, the pooled data revealed insignificant correlation of PNI with CSS in oral carcinoma (HR=1.89, 95%CI=0.61–5.84, p=0.267).
Table 3. Subgroup analysis of PNI for DFS and CSS in patients with oral cancer.
| Subgroup factors | No. of studies | No. of patients | Effect model | HR (95%CI) | p | Heterogeneity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I2(%) | Ph | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total | 6 | 1,135 | Fixed | 1.92(1.53-2.42) | <0.001 | 24.2 | 0.252 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Geographical regions | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Japan | 4 | 442 | Fixed | 2.94(1.91-4.51) | <0.001 | 0 | 0.983 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| China | 1 | 333 | - | 2.02(1.25-3.26) | 0.004 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Taiwan | 1 | 360 | - | 1.46(1.05-2.03) | 0.026 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sample size | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤150 | 3 | 259 | Fixed | 2.84(1.76-4.60) | <0.001 | 0 | 0.959 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >150 | 3 | 876 | Fixed | 1.71(1.32-2.22) | <0.001 | 37.5 | 0.202 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cancer type | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OSCC | 5 | 952 | Fixed | 1.86(1.47-2.36) | <0.001 | 23.8 | 0.263 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OC | 1 | 183 | - | 3.33(1.28-8.65) | 0.014 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Study center | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multicenter | 2 | 443 | Fixed | 2.20(1.45-3.33) | <0.001 | 0 | 0.481 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single center | 4 | 692 | Fixed | 1.81(1.38-2.39) | <0.001 | 45.9 | 0.136 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TNM stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I-IV | 5 | 1,088 | Fixed | 1.88(1.49-2.38) | <0.001 | 30.6 | 0.217 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III-IV | 1 | 47 | - | 3.31(1.01-10.84) | 0.048 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatment | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Surgery | 4 | 905 | Fixed | 1.81(1.42-2.31) | <0.001 | 30.3 | 0.231 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mixed | 1 | 183 | - | 3.33(1.28-8.65) | 0.014 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CRT | 1 | 47 | - | 3.31(1.01-10.84) | 0.048 | - | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PNI cut-off value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤49 | 3 | 482 | Fixed | 2.31(1.60-3.35) | <0.001 | 0 | 0.647 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >49 | 3 | 653 | Random | 2.10(1.19-3.70) | 0.011 | 52.1 | 0.124 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cut-off determination | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ROC curve | 4 | 619 | Fixed | 1.81(1.38-2.38) | <0.001 | 41.2 | 0.164 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| X-tile/literature | 2 | 516 | Fixed | 2.23(1.45-3.43) | <0.001 | 0 | 0.357 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OC, oral cancer; OSCC, oral squamous cell carcinoma; ROC, receiver operating characteristic; DFS, disease-free survival; CRT, chemoradiotherapy. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
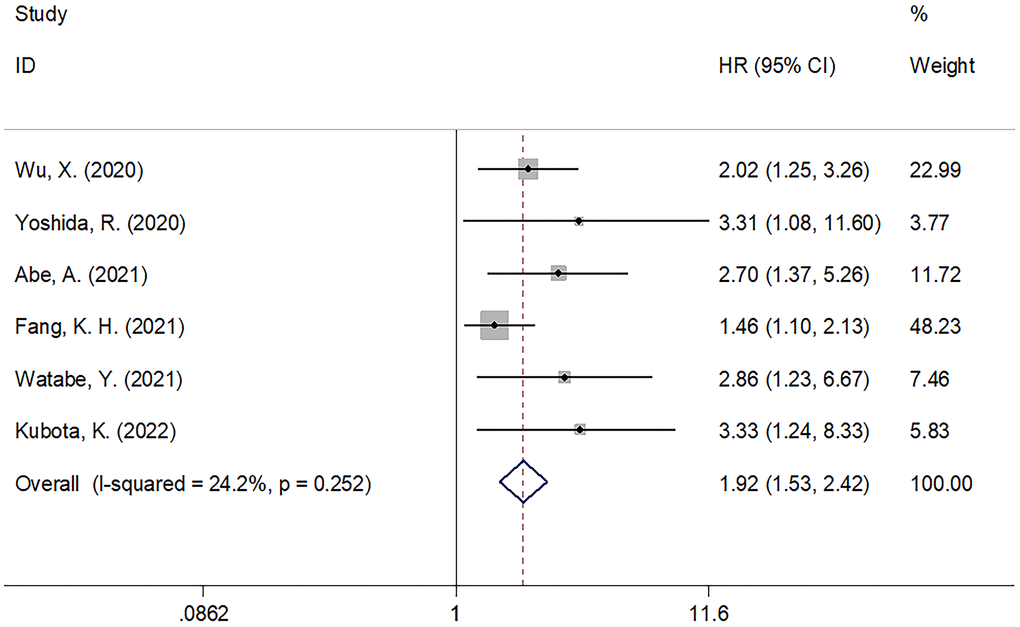
Figure 3. The forest plot of the association between PNI and DFS in patients with oral cancer.
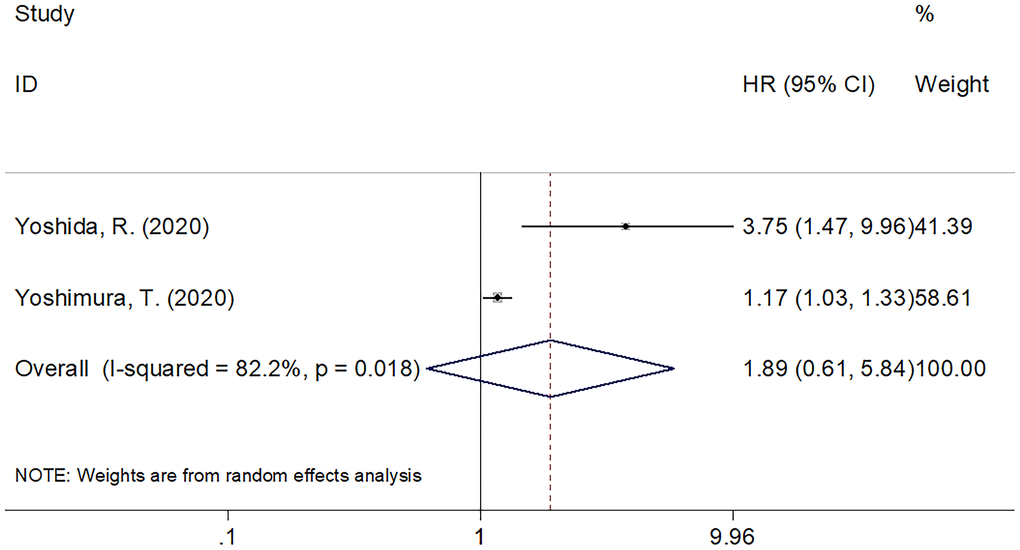
Figure 4. The forest plot of the association between PNI and CSS in patients with oral cancer.
The correlation between PNI and clinicopathological factors in oral cancer
Data of PNI and clinicopathological traits in oral cancer were provided by 6 studies involving 1,420 patients in total [13, 20, 23, 24, 26, 27]. PNI’s correlations with the following parameters were examined: gender (male vs. female), age (years; ≥65 vs. <65), TNM stage (III–IV vs. I–II), N stage (N+ vs. N0), T stage (T3-4 vs. T1-2) and differentiation (Poor, moderate vs well). As suggested by the pooled data in Figure 5 combined with Table 4, a low PNI was linked significantly to age ≥ 65 years (OR=2.29, 95%CI=1.76-2.98, p<0.001) and III-IV TNM stage (OR=2.16, 95%CI=1.60-2.91, p<0.001). Nevertheless, the correlations of PNI with gender (OR=0.94, 95%CI=0.71-1.24, p=0.656), T stage (OR=1.78, 95%CI=0.97-3.26, p=0.064), N stage (OR=1.17, 95%CI=0.74-1.87, p=0.498), or differentiation (OR=1.57, 95%CI=0.81-3.04, p=0.184) were insignificant (Table 4 and Figure 5).
Table 4. The correlation between PNI and clinicopathological features in patients with oral cancer.
| Variables | No. of studies | No. of patients | Effects model | OR (95%CI) | p | Heterogeneity | |
| I2(%) | Ph | ||||||
| Sex (male vs female) | 6 | 1,420 | Fixed | 0.94(0.71-1.24) | 0.656 | 12 | 0.339 |
| Age (years) (≥65 vs <65) | 6 | 1,420 | Fixed | 2.29(1.76-2.98) | <0.001 | 40.2 | 0.138 |
| T stage (T3-4 vs T1-2) | 5 | 1,360 | Random | 1.78(0.97-3.26) | 0.064 | 72.7 | 0.005 |
| N stage (N+ vs N0) | 5 | 1,360 | Random | 1.17(0.74-1.87) | 0.498 | 61.8 | 0.033 |
| Differentiation (Poor, moderate vs well) | 5 | 1,237 | Random | 1.57(0.81-3.04) | 0.184 | 57.3 | 0.053 |
| TNM stage (III-IV vs I-II) | 3 | 1,130 | Fixed | 2.16(1.60-2.91) | <0.001 | 0 | 0.406 |
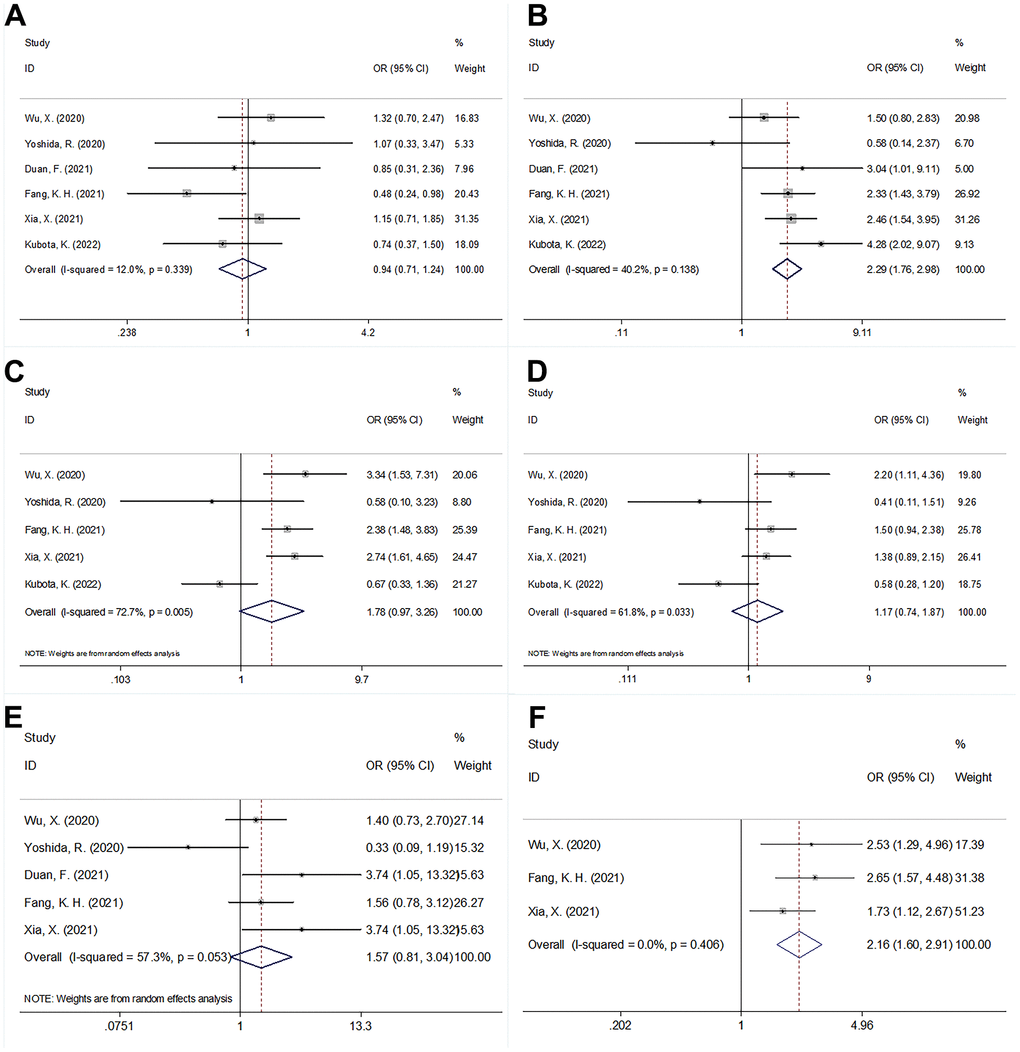
Figure 5. The forest plots of the correlation between PNI and clinicopathological factors in patients with oral cancer. (A) Sex (male vs female); (B) Age (years) (≥65 vs <65); (C) T stage (T3-4 vs T1-2); (D) N stage (N+ vs N0); (E) Differentiation (Poor, moderate vs well); and (F) TNM stage (III-IV vs I-II).
Publication bias
Publication bias was assessed through Begg’s test combined with Funnel plotting. As shown in Figure 6, p values of Begg’s test for OS, DFS, and CSS were 0.602, 0.260, and 0.317, respectively. The funnel plots were symmetrical and the evidence of publication bias was absent in the current meta-analysis.
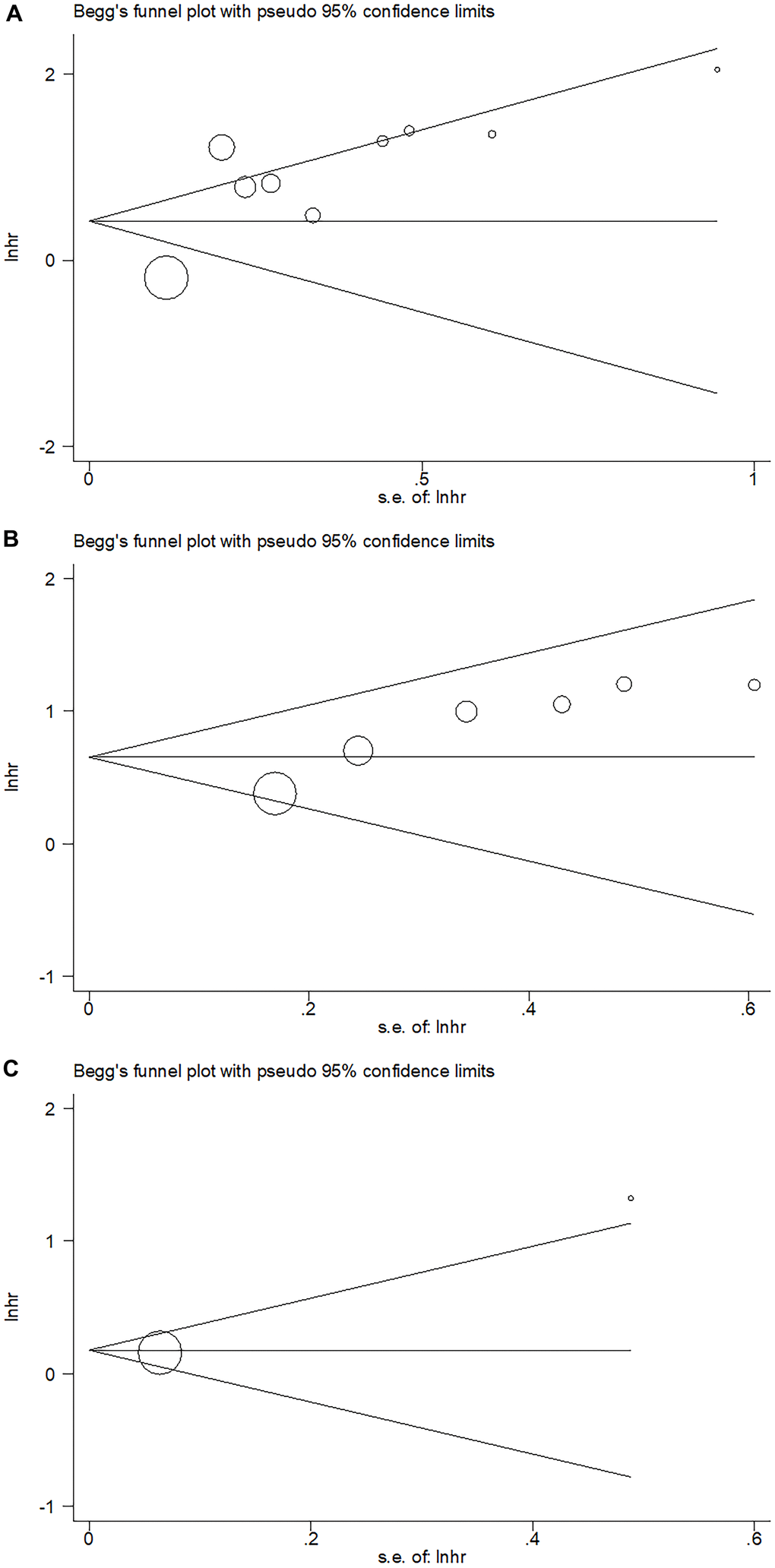
Figure 6. Publication bias examined by Begg’s test. (A) Publication bias for OS, Begg’s test: p=0.602; (B) Publication bias for DFS, Begg’s test: p=0.260; (C) Publication bias for CSS, Begg’s test: p=0.317.
Discussion
There was inconsistency between former works regarding PNI’s prognostic significance in the oral carcinoma population. In our present meta-analysis, PNI’s exact role in prognosticating oral carcinoma was explored based on data gathered from 10 studies with 3,130 patients. As demonstrated by the pooled results, a low PNI acted as a significant predictor for DFS and OS, but not for CSS among the oral carcinoma population. Besides, a low PNI was linked significantly also to advanced stage of TNM and ≥65 years of age, which suggested the indicator role of PNI for disease progression and senile patients. Taken together, PNI acted as a significant biomarker for prognosticating clinical outcomes of oral carcinoma patients. Given its readily availability and cost efficiency, PNI was promising for prognostication in oral cancer. As far as we know, the present meta-analysis represents the initial attempt to investigate PNI’s prognostic value for oral carcinoma patients.
PNI is calculated according to the lymphocyte counts and albumin levels, therefore, the low levels of lymphocytes and serum albumin could lead to a low PNI. PNI is capable of reflecting host’s immune and trophic statuses. On the one hand, lymphocytes, particularly tumor-infiltrating lymphocytes (TILs), can induce the apoptosis of tumor cells [28]. TILs are an important component of cellular immunity and can eliminate tumor cells through humoral immunity [29]. Hence, lymphopenia can lead to compromised cancer resistance resulting from the immune-response to carcinoma cells [30]. On the other hand, albumin is the most abundant plasma protein, accounting for about half of the total protein content [31]. As an ordinary biomarker of trophic status, low albumin levels are associated with chronic inflammation that triggers IL-1, TNF-α and other cytokine stimulation [32]. Low albumin level indicates a malnutrition status and often occurs in patients with oral cancer because food intake ability is impaired [33]. Therefore, the decrease of PNI reflects the decreased inhibition of inflammatory response and malnutrition, thus affecting prognosis for oral carcinoma patients.
In prior meta-analysis-based works, PNI’s prognostic value in diverse types of carcinomas has been investigated [34–37]. According to a report by Kim et al., lower PNI was a negative predictor linked to progression of carcinomas and inferior survival of renal cell carcinoma patients in a meta-analysis including 9 studies [38]. According to a meta-analysis involving 1,311 patients by Luan et al., low PNI was linked to inferior PFS and OS in diffuse large B-cell lymphoma [36]. A recent meta-analysis involving 3,118 patients indicated that among the esophageal cancer population, there were associations of lower PNI with unfavorable prognostic predictor and inferior prognosis [37]. Dai and colleagues showed in their meta-analysis that among ovarian cancer population, low preoperative PNI was linked to shorter PFS, OS, as well as inferior clinicopathological traits [39]. In the current meta-analysis, we identified the low PNI as a negative prognostic indicator among the oral carcinoma population, showing conformance to the findings in other carcinomas. Besides, correlation of a low PNI with senile patients was noted as well. Therefore, patients with oral cancer ≥ 65 years may be suffer from high risk of tumor progression. The current meta-analysis retrieved literature with no language restriction. Notably, we included studies with a comprehensive literature search. Finally, ten studies with 3,130 patients were included in this meta-analysis. The sample size is relatively large to draw effective results.
Our meta-analysis also has a few shortcomings. Firstly, all included studies are from Asian regions, therefore, our results may more applicable to Asian population. Further works should validate PNI’s prognostic significance among the non-Asian population. Secondly, the cut-off values of PNI were not standard and various PNI cut-off value was used. Although one study [27] adopted 52.44 referring to a previous study [25], the other studies [12, 13, 20–24, 26] used different cut-off values. Thirdly, high heterogeneity existed in some analyses, which may be because retrospective researches are inherent in nature. Therefore, large-scale clinical trials with patients of diverse ethnicities are still needed to validate our findings.
Conclusively, the present meta-analysis suggested the correlations of a low PNI with inferior DFS and OS among the oral carcinoma patients. Oral cancer patients with low PNI may have high-risk of tumor progression.
Materials and Methods
Study guideline and literature search
The procedure of current meta-analysis followed the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [40]. The following electronic databases were fully retrieved: Web of Science, China National Knowledge Infrastructure (CNKI), Cochrane Library, PubMed and Embase. The updating date for last retrieval of literature was April 26, 2022. The following key words were used to retrieve potential research: “oral cancer”, “oral carcinoma”, “oral squamous cell carcinoma”, “OSCC”, “Squamous cell carcinomas of the tongue”, “prognostic nutrition index”, and “PNI”. There was no restriction on publication language. We also checked the references of enrolled works for relevant studies.
Inclusion and exclusion criteria
The inclusion criteria were determined in accordance with the populations, interventions, comparators, outcomes, and study designs (PICOS) guideline.
We formulated the inclusion criteria as follows: (1) P (populations): subjects were diagnosed with oral carcinoma by pathological or histological means; (2) I (interventions): oral cancer patients with the PNI value was evaluated before treatment; (3) C (comparators): a threshold for distinguishing between low/high PNI was identified and the patient groups were divided as low PNI compared with high PNI; (4) O (outcomes): association of PNI with survival outcomes was reported in oral cancer; hazards ratios (HRs) for survival prognoses were reported in text, plus their 95% confidence intervals (CIs), or adequate data were offered for their computation; (5) S (study design): cohort studies, including prospective and retrospective cohorts published in any language.
The exclusion criteria were: (1) reviews, case reports, letters and conference abstracts; (2) absence of extractable survival data; (3) animal studies.
Data extraction and quality assessment
Data from qualified studies were extracted by 2 independent researchers (MD and QS) according to a prespecified protocol. Disputes were all addressed by negotiation to consensus. The extracted information included name of the first author, study country/region, year, sample size, age, carcinoma type, study duration, Tumor–Node–Metastasis (TNM) stage, study center, study design, treatment method, threshold for PNI, method for identifying threshold, survival endpoints, type of survival analysis, HRs, as well as 95% CIs. All survival outcomes can be extracted included but not limited to disease-free survival (DFS), overall survival (OS), as well as cancer-specific survival (CSS). Based on the Newcastle-Ottawa Scale (NOS), the quality of included studies was evaluated by the foregoing MD and QS [41]. Through negotiation, discrepancies in evaluation were addressed until arriving at a consensus. The full score of NOS is 9 and the quality of studies was considered high when the NOS score was ≥6 points.
Statistical analysis
The statistical analyses were entirely accomplished with the aid of Stata Ver. 12.0 (Stata Corp., College Station, TX, USA). PNI’s value for survival prognosis in oral carcinoma was assessed by estimating pooled HRs plus 95% CIs. The inter-study heterogeneity was evaluated by the Q and Higgins I-squared statistics. P for heterogeneity >0.10 and I2 ≤ 50% identified lower heterogeneity, in which case a fixed-effect model was adopted. In other cases, we utilized a random-effects model. The prognostic value of PNI in different patient populations was examined through subgroup analysis. For assessment of PNI’s correlation with clinicopathological traits in oral carcinoma, pooled odds ratios (ORs) plus 95% CIs were utilized. Publication bias was evaluated through Begg’s test combined with Funnel plotting. A p value <0.05 (two-sided) indicated a statistically significant difference.
Availability of data and materials
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
MD and QS conceived the study and drafted the manuscript. MD and QS conducted the literature search. MD and QS extracted the data. MD made the figures and tables. All authors revised and checked the final manuscript. All authors contributed to the article and approved the submitted version.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Funding
No funding was provided for this study.
References
- 1. Sarode GS, Sarode SC, Maniyar N, Anand R, Patil S. Oral cancer databases: A comprehensive review. J Oral Pathol Med. 2018; 47:547–56. https://doi.org/10.1111/jop.12667 [PubMed]
- 2. Sarode G, Maniyar N, Sarode SC, Jafer M, Patil S, Awan KH. Epidemiologic aspects of oral cancer. Dis Mon. 2020; 66:100988. https://doi.org/10.1016/j.disamonth.2020.100988 [PubMed]
- 3. Inchingolo F, Santacroce L, Ballini A, Topi S, Dipalma G, Haxhirexha K, Bottalico L, Charitos IA. Oral Cancer: A Historical Review. Int J Environ Res Public Health. 2020; 17:3168. https://doi.org/10.3390/ijerph17093168 [PubMed]
- 4. Dioguardi M, Spirito F, Sovereto D, Alovisi M, Troiano G, Aiuto R, Garcovich D, Crincoli V, Laino L, Cazzolla AP, Caloro GA, Di Cosola M, Lo Muzio L. MicroRNA-21 Expression as a Prognostic Biomarker in Oral Cancer: Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022; 19:3396. https://doi.org/10.3390/ijerph19063396 [PubMed]
- 5. Almangush A, Mäkitie AA, Triantafyllou A, de Bree R, Strojan P, Rinaldo A, Hernandez-Prera JC, Suárez C, Kowalski LP, Ferlito A, Leivo I. Staging and grading of oral squamous cell carcinoma: An update. Oral Oncol. 2020; 107:104799. https://doi.org/10.1016/j.oraloncology.2020.104799 [PubMed]
- 6. Sekido K, Imaue S, Tomihara K, Tachinami H, Yamagishi K, Okazawa S, Ikeda A, Fujiwara K, Noguchi M. Durable complete response to immunotherapy with anti-PD-1 antibody nivolumab in a patient with oral squamous cell carcinoma presenting with lung metastasis: A case report. Clin Case Rep. 2021; 9:e04545. https://doi.org/10.1002/ccr3.4545 [PubMed]
- 7. Tian Y, Zhang L, Jin N, Wan Z, Zhang H, Zhang H, Zhang L. Clinical Response to Neoadjuvant Immunotherapy Combined with Targeted Therapy and Chemotherapy in Oral Squamous Cell Carcinoma: Experience in Three Patients. Onco Targets Ther. 2022; 15:353–9. https://doi.org/10.2147/OTT.S355349 [PubMed]
- 8. Liang KH, Lin YY, Chiang SH, Tsai ET, Lo WL, Wang CL, Wang TY, Sun YC, Kao SY, Wu CH, Hung KF. Recent progress of biomarkers in oral cancers. J Chin Med Assoc. 2021; 84:987–92. https://doi.org/10.1097/JCMA.0000000000000616 [PubMed]
- 9. Nakashima H, Matsuoka Y, Yoshida R, Nagata M, Hirosue A, Kawahara K, Sakata J, Arita H, Hiraki A, Nakayama H. Pre-treatment neutrophil to lymphocyte ratio predicts the chemoradiotherapy outcome and survival in patients with oral squamous cell carcinoma: a retrospective study. BMC Cancer. 2016; 16:41. https://doi.org/10.1186/s12885-016-2079-6 [PubMed]
- 10. Acharya S, Rai P, Hallikeri K, Anehosur V, Kale J. Preoperative platelet lymphocyte ratio is superior to neutrophil lymphocyte ratio to be used as predictive marker for lymph node metastasis in oral squamous cell carcinoma. J Investig Clin Dent. 2017; 8. https://doi.org/10.1111/jicd.12219 [PubMed]
- 11. Chen L, Qian J, Lin L, Lin J, Chen Q, Zhuang Z, Hong Y, Wang J, Qiu Y, Pan L, Shi B, Wang J, Liu F, et al. Prognostic value of preoperative lymphocyte-to-monocyte ratio in oral cancer patients and establishment of a dynamic nomogram. Oral Dis. 2021; 27:1127–36. https://doi.org/10.1111/odi.13629 [PubMed]
- 12. Bao X, Liu F, Lin J, Chen Q, Chen L, Chen F, Wang J, Qiu Y, Shi B, Pan L, Lin L, He B. Nutritional assessment and prognosis of oral cancer patients: a large-scale prospective study. BMC Cancer. 2020; 20:146. https://doi.org/10.1186/s12885-020-6604-2 [PubMed]
- 13. Wu X, Jiang Y, Ge H, Diao P, Wang D, Wang Y, Cheng J. Predictive value of prognostic nutritional index in patients with oral squamous cell carcinoma. Oral Dis. 2020; 26:903–11. https://doi.org/10.1111/odi.13318 [PubMed]
- 14. Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. 1984; 85:1001–5. [PubMed]
- 15. Zheng Z, Zhu H, Cai H. Preoperative Prognostic Nutritional Index Predict Survival in Patients With Resectable Esophageal Squamous Cell Carcinoma. Front Nutr. 2022; 9:824839. https://doi.org/10.3389/fnut.2022.824839 [PubMed]
- 16. Yuce E, Alandag C, Cakir E, Fidan E. Prognostic Factors in Gastrointestinal Stromal Tumors (GIST): Could Prognostic Nutritional Index (PNI) be a New Prognostic Factor? J Coll Physicians Surg Pak. 2022; 32:81–5. https://doi.org/10.29271/jcpsp.2022.01.81 [PubMed]
- 17. Ryu T, Takami Y, Wada Y, Sasaki S, Saitsu H. Predictive impact of the prognostic nutritional index in early-staged hepatocellular carcinoma after operative microwave ablation. Asian J Surg. 2022; 45:202–7. https://doi.org/10.1016/j.asjsur.2021.04.043 [PubMed]
- 18. Chen T, Liang G, Xiang Z, He J, Xu X, Tang M. Prognostic value of prognostic nutritional index and its variations in advanced non-small-cell lung cancer patients treated with anlotinib monotherapy. J Clin Lab Anal. 2022; 36:e24300. https://doi.org/10.1002/jcla.24300 [PubMed]
- 19. He Q, Zhao W, Ren Q. The Prognostic Value of the Prognostic Nutritional Index in Operable High-Grade Glioma Patients and the Establishment of a Nomogram. Front Oncol. 2022; 11:724769. https://doi.org/10.3389/fonc.2021.724769 [PubMed]
- 20. Yoshida R, Gohara S, Sakata J, Matsuoka Y, Hirosue A, Kawahara K, Kawaguchi S, Nagao Y, Yamana K, Nagata M, Fukuma D, Toya R, Murakami R, et al. Onodera’s prognostic nutritional index correlates with tumor immune environment and survival in patients with oral squamous cell carcinoma undergoing chemoradiotherapy. Transl Oncol. 2020; 13:100850. https://doi.org/10.1016/j.tranon.2020.100850 [PubMed]
- 21. Yoshimura T, Suzuki H, Takayama H, Higashi S, Hirano Y, Tezuka M, Ishida T, Ishihata K, Nishi Y, Nakamura Y, Imamura Y, Nozoe E, Nakamura N. Impact of Preoperative Low Prognostic Nutritional Index and High Intramuscular Adipose Tissue Content on Outcomes of Patients with Oral Squamous Cell Carcinoma. Cancers (Basel). 2020; 12:3167. https://doi.org/10.3390/cancers12113167 [PubMed]
- 22. Abe A, Hayashi H, Ishihama T, Furuta H. Prognostic impact of the prognostic nutritional index in cases of resected oral squamous cell carcinoma: a retrospective study. BMC Oral Health. 2021; 21:40. https://doi.org/10.1186/s12903-021-01394-6 [PubMed]
- 23. Duan F, Ma R, Liao L, Zhao W, Liu Y. [Efficacy of prognostic nutritional index for predicting prognosis of patients with oral squamous cell carcinoma]. Chin J Clin Oncol Rehabil. 2021; 28:1165–8.
- 24. Fang KH, Chang SW, Lee YC, Huang EI, Lai CH, Chang GH, Tsai MS, Hsu CM, Tsai YT. Preoperative prognostic nutritional index predicts prognosis of patients with oral cavity cancer. Oral Dis. 2022; 28:1816–30. https://doi.org/10.1111/odi.13840 [PubMed]
- 25. Watabe Y, Aoki K, Ichikawa H, Matsuzaki H, Ito A, Tanaka JI, Kamiyama I, Shigematsu S. A preoperative prognostic nutritional index is a prognostic indicator in oral squamous cell carcinoma patients undergoing radical surgery. Int J Oral Maxillofac Surg. 2021; 50:1413–21. https://doi.org/10.1016/j.ijom.2021.01.009 [PubMed]
- 26. Xia X, Zhang W, Yuan H, Liu F, Jiang B. Value of preoperative prognostic nutrition index in predicting prognosis of oral squamous cell carcinoma patients initially undergoing radical operation. Journal of Clinical Medicine in Practice. 2021; 25:6–10. https://doi.org/10.7619/jcmp.20210831
- 27. Kubota K, Ito R, Narita N, Tanaka Y, Furudate K, Akiyama N, Chih CH, Komatsu S, Kobayashi W. Utility of prognostic nutritional index and systemic immune-inflammation index in oral cancer treatment. BMC Cancer. 2022; 22:368. https://doi.org/10.1186/s12885-022-09439-x [PubMed]
- 28. Gooden MJ, de Bock GH, Leffers N, Daemen T, Nijman HW. The prognostic influence of tumour-infiltrating lymphocytes in cancer: a systematic review with meta-analysis. Br J Cancer. 2011; 105:93–103. https://doi.org/10.1038/bjc.2011.189 [PubMed]
- 29. Ogiya R, Niikura N, Kumaki N, Bianchini G, Kitano S, Iwamoto T, Hayashi N, Yokoyama K, Oshitanai R, Terao M, Morioka T, Tsuda B, Okamura T, et al. Comparison of tumor-infiltrating lymphocytes between primary and metastatic tumors in breast cancer patients. Cancer Sci. 2016; 107:1730–5. https://doi.org/10.1111/cas.13101 [PubMed]
- 30. Wada Y, Nakashima O, Kutami R, Yamamoto O, Kojiro M. Clinicopathological study on hepatocellular carcinoma with lymphocytic infiltration. Hepatology. 1998; 27:407–14. https://doi.org/10.1002/hep.510270214 [PubMed]
- 31. Zhou QP, Li XJ. C-Reactive Protein to Albumin Ratio in Colorectal Cancer: A Meta-Analysis of Prognostic Value. Dose Response. 2019; 17:1559325819889814. https://doi.org/10.1177/1559325819889814 [PubMed]
- 32. Oñate-Ocaña LF, Aiello-Crocifoglio V, Gallardo-Rincón D, Herrera-Goepfert R, Brom-Valladares R, Carrillo JF, Cervera E, Mohar-Betancourt A. Serum albumin as a significant prognostic factor for patients with gastric carcinoma. Ann Surg Oncol. 2007; 14:381–9. https://doi.org/10.1245/s10434-006-9093-x [PubMed]
- 33. Chojkier M. Inhibition of albumin synthesis in chronic diseases: molecular mechanisms. J Clin Gastroenterol. 2005; 39:S143–6. https://doi.org/10.1097/01.mcg.0000155514.17715.39 [PubMed]
- 34. Xue S, Zhao H, Zhang K, Zhang H, Wang W. Prognostic and Clinicopathological Correlations of Pretreatment Prognostic Nutritional Index in Renal Cell Carcinoma: A Meta-Analysis. Urol Int. 2022; 106:567–80. https://doi.org/10.1159/000521353 [PubMed]
- 35. Lv X, Zhang Z, Yuan W. Pretreatment Prognostic Nutritional Index (PNI) as a Prognostic Factor in Patients with Biliary Tract Cancer: A Meta-Analysis. Nutr Cancer. 2021; 73:1872–81. https://doi.org/10.1080/01635581.2020.1817955 [PubMed]
- 36. Luan C, Wang F, Wei N, Chen B. Prognostic nutritional index and the prognosis of diffuse large b-cell lymphoma: a meta-analysis. Cancer Cell Int. 2020; 20:455. https://doi.org/10.1186/s12935-020-01535-x [PubMed]
- 37. Liao G, Zhao Z, Yang H, Chen M, Li X. Can Prognostic Nutritional Index be a Prediction Factor in Esophageal Cancer?: A Meta-Analysis. Nutr Cancer. 2020; 72:187–93. https://doi.org/10.1080/01635581.2019.1631859 [PubMed]
- 38. Kim SI, Kim SJ, Kim SJ, Cho DS. Prognostic nutritional index and prognosis in renal cell carcinoma: A systematic review and meta-analysis. Urol Oncol. 2021; 39:623–30. https://doi.org/10.1016/j.urolonc.2021.05.028 [PubMed]
- 39. Dai Y, Liu M, Lei L, Lu S. Prognostic significance of preoperative prognostic nutritional index in ovarian cancer: A systematic review and meta-analysis. Medicine (Baltimore). 2020; 99:e21840. https://doi.org/10.1097/MD.0000000000021840 [PubMed]
- 40. Moher D, Liberati A, Tetzlaff J, Altman DG, and PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009; 62:1006–12. https://doi.org/10.1016/j.jclinepi.2009.06.005 [PubMed]
- 41. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010; 25:603–5. https://doi.org/10.1007/s10654-010-9491-z [PubMed]