



Introduction
Neuroblastoma (NB) is the most common extracranial solid tumor in children, accounting for 8% of all pediatric malignancies [1]. The mortality rate of NB is 0.85–1.1 cases per 100,000 children in the world [2]. Most of the low-risk NB patients resolve spontaneously without chemotherapy [3]. However, high-risk patients, accounting for nearly 50% of NB, have been extensively metastatic at the time of diagnosis. Despite various treatments such as surgery, chemotherapy, radiotherapy, and immunotherapy, the survival rate is still less than 40% [4]. Unfortunately, the pathogenesis of NB has not yet been fully understood [5, 6]. Studies have found that about 1–2% of NB cases are familial [2]. PHOX2B [7] or ALK [8] gene mutations are considered to be the main cause of familial NB. However, sporadic neuroblastoma is the main form of NB [9]. Increasing evidence shows that genetic variants play a key role in the development of NB [10–12]. In recent years, several NB susceptibility loci have been identified through genome-wide association studies (GWASs), such as BARD1 [13], LMO1 [14], HACE1 [15], TP53 [16], CASC15 [17], MLF1 [18], and CDKN1B [19]. Moreover, many polymorphisms were also identified to influence chemotherapy and outcome in patients with neuroblastoma [20, 21]. The identification of these susceptible loci has deepened the understanding of the pathogenesis of NB [22, 23]. However, more gene single nucleotide polymorphisms (SNPs) involved in the process of tumorigenesis await to be revealed.
N6-methyladenosine (m6A) is the most common and abundant post-transcriptional modification of eukaryotic mRNA [24, 25]. The formation of m6A is dynamically converted by methyltransferase complexes (“writers”; METTL3, METTL14, and WTAP), demethylases (“erasers”; FTO and ALKBH5), and binding proteins (“readers”; YTHDF1/2/3, YTHDC1) [26, 27]. Recently, it has been confirmed that m6A modified disorders are involved in human carcinogenesis, including osteosarcoma [28], glioblastoma [29], colorectal cancer [30], acute myeloid leukemia [31], gastric cancer [32], glioma [33], and bladder cancer [34]. The abnormal modification level of m6A may affect the individual’s cancer susceptibility [35]. YTH domain contains protein 1 (YTHDC1), an important m6A recognition protein, is involved in mRNA splicing and the export of methylated mRNAs [36, 37], but its role has not yet been deeply understood.
Considering the evidence that m6A is closely related to tumorigenesis and metastasis, we speculate that there may be a significant correlation between the genetic variation of m6A modified gene YTHDC1 and the risk of NB. Therefore, we performed this study by recruiting 898 NB patients and 1734 controls to explore the relationship between YTHDC1 SNPs and NB risk in Chinese children.
Results
Association between YTHDC1 gene polymorphisms and NB susceptibility
In this study, 896 NB cases and 1733 controls were successfully genotyped. The three polymorphisms of YTHDC1 were consistent with Hardy-Weinberg equilibrium (HWE) (P = 0.696 for rs2293596 T>C, P = 0.556 for rs2293595 T>C, P = 0.968 for rs3813832 T>C). The genotype distribution frequencies of case and control groups were shown in Table 1. The results showed that in the rs3813832 T>C polymorphism, relative to the TT genotype, TC genotype could significantly reduce the susceptibility of NB [adjusted odds ratio (AOR) = 0.81, 95% confidence interval (CI) = 0.68–0.96, P = 0.018]. In addition, we used rs2293596 TT/TC, rs2293595 TC/CC, or rs3813832 TC/CC as protective genotypes to further investigate the combined effect of these three SNPs. The combined genotype analysis revealed that individuals carrying 3 protective genotypes had a prominent lower risk of NB compared with individuals carrying 0–2 protective genotypes (AOR = 0.80, 95% CI = 0.68–0.94, P = 0.006).
Table 1. Association between YTHDC1 gene polymorphisms and neuroblastoma risk.
| Genotype | Cases (N = 896) | Controls (N = 1733) | Pa | Crude OR (95% CI) | P | Adjusted OR (95% CI)b | Pb | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs2293596 T>C (HWE = 0.696) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | 580 (64.73) | 1144 (66.01) | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC | 272 (30.36) | 525 (30.29) | 1.02 (0.86–1.22) | 0.811 | 1.03 (0.86–1.23) | 0.778 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 44 (4.91) | 64 (3.69) | 1.36 (0.91–2.02) | 0.132 | 1.36 (0.91–2.02) | 0.130 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Additive | 0.283 | 1.08 (0.94–1.25) | 0.283 | 1.08 (0.94–1.25) | 0.267 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dominant | 316 (35.27) | 589 (33.99) | 0.513 | 1.06 (0.89–1.25) | 0.511 | 1.06 (0.90–1.26) | 0.486 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recessive | 852 (95.09) | 1669 (96.31) | 0.136 | 1.35 (0.91–1.99) | 0.137 | 1.35 (0.91–2.00) | 0.137 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs2293595 T>C (HWE = 0.556) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | 343 (38.28) | 601 (34.68) | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC | 411 (45.87) | 829 (47.84) | 0.87 (0.73–1.04) | 0.121 | 0.86 (0.72–1.03) | 0.102 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 142 (15.85) | 303 (17.48) | 0.82 (0.65–1.04) | 0.107 | 0.82 (0.65–1.04) | 0.107 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Additive | 0.070 | 0.90 (0.80–1.01) | 0.070 | 0.90 (0.80–1.01) | 0.067 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dominant | 553 (61.72) | 1132 (65.32) | 0.068 | 0.86 (0.72–1.01) | 0.068 | 0.85 (0.72–1.01) | 0.059 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recessive | 754 (84.15) | 1430 (82.52) | 0.289 | 0.89 (0.72–1.11) | 0.289 | 0.89 (0.72–1.11) | 0.309 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs3813832 T>C (HWE = 0.968) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | 499 (55.69) | 902 (52.05) | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC | 314 (35.04) | 697 (40.22) | 0.81 (0.69–0.97) | 0.020 | 0.81 (0.68–0.96) | 0.018 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CC | 83 (9.26) | 134 (7.73) | 1.12 (0.83–1.50) | 0.452 | 1.13 (0.84–1.52) | 0.403 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Additive | 0.424 | 0.95 (0.84–1.08) | 0.424 | 0.95 (0.84–1.08) | 0.446 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dominant | 397 (44.31) | 831 (47.95) | 0.076 | 0.86 (0.73–1.02) | 0.076 | 0.86 (0.73–1.02) | 0.075 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recessive | 813 (90.74) | 1599 (92.27) | 0.176 | 1.22 (0.92–1.62) | 0.177 | 1.24 (0.93–1.65) | 0.148 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Combined effect of protective genotypesc | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0–2 | 428 (47.77) | 735 (42.41) | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | 468 (52.23) | 998 (57.59) | 0.009 | 0.81 (0.69–0.95) | 0.008 | 0.80 (0.68–0.94) | 0.006 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: OR: odds ratio; CI: confidence interval; HWE: Hardy-Weinberg equilibrium. aχ2 test for genotype distributions between neuroblastoma patients and cancer-free controls. bAdjusted for age and gender. cProtective genotypes were rs2293596 TT/TC, rs2293595 TC/CC and rs968697 TC/CC. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Stratification analysis
Subsequently, we conducted a stratified analysis based on age, gender, sites of origin, and clinical stage to further explore the relationship between YTHDC1 gene SNPs (rs2293596 T>C, rs2293595 T>C and rs3813832 T>C) and the risk of NB (Table 2). In the subgroup of clinical stage III + IV, the rs3813832 TC/CC genotype carriers suffer from a relatively lower risk of NB (AOR = 0.77, 95% CI = 0.62–0.96, P = 0.022). In addition, individuals with 3 protective genotypes had an observably decreased risk of NB (AOR = 0.80, 95% CI = 0.65–0.98, P = 0.032) in subgroup of children over 18 months of age. As to the participants’ gender, we found that male carrying the 3 protective genotypes also showed a lower NB risk (AOR = 0.77, 95% CI = 0.62–0.96, P = 0.021). From the sites of origin, individuals with 3 protective genotypes were less likely to have NB that original from mediastinum (AOR = 0.67, 95% CI = 0.51–0.90, P = 0.007). In terms of clinical stage, individuals carrying 3 protective genotypes displayed a weak susceptibility at clinical stages I + II + 4s (AOR = 0.78, 95% CI = 0.64–0.96, P = 0.019) and III + IV (AOR = 0.77, 95% CI = 0.62–0.97, P = 0.023).
Table 2. Stratification analysis for association between YTHDC1 gene genotypes and neuroblastoma susceptibility.
| Variables | rs2293595 (case/control) | AOR (95% CI)a | Pa | rs3813832 (case/control) | AOR (95% CI)a | Pa | Protective genotypes (case/control) | AOR (95% CI)a | Pa | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TT | TC/CC | TT | TC/CC | 0-2 | 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, month | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤18 | 146/265 | 198/448 | 0.80 (0.62–1.04) | 0.098 | 197/378 | 147/335 | 0.84 (0.65–1.09) | 0.188 | 177/327 | 167/386 | 0.80 (0.62–1.03) | 0.085 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >18 | 197/336 | 355/684 | 0.89 (0.71–1.10) | 0.284 | 302/524 | 250/496 | 0.87 (0.71–1.08) | 0.205 | 251/408 | 301/612 | 0.80 (0.65–0.98) | 0.032 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 156/265 | 250/479 | 0.88 (0.69–1.13) | 0.325 | 222/396 | 184/348 | 0.94 (0.74–1.20) | 0.639 | 191/318 | 215/426 | 0.83 (0.65–1.06) | 0.131 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 187/336 | 303/653 | 0.83 (0.66–1.04) | 0.102 | 277/506 | 213/483 | 0.80 (0.65–1.00) | 0.05 | 237/417 | 253/572 | 0.77 (0.62–0.96) | 0.021 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sites of origin | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adrenal gland | 97/601 | 151/1132 | 0.82 (0.62–1.07) | 0.143 | 145/902 | 103/831 | 0.76 (0.58–1.00) | 0.051 | 117/735 | 131/998 | 0.81 (0.62–1.06) | 0.119 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Retroperitoneal | 110/601 | 208/1132 | 0.99 (0.77–1.27) | 0.93 | 164/902 | 154/831 | 1.02 (0.80–1.29) | 0.888 | 141/735 | 177/998 | 0.91 (0.71–1.16) | 0.43 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mediastinum | 85/601 | 128/1132 | 0.80 (0.60–1.08) | 0.143 | 121/902 | 92/831 | 0.83 (0.62–1.11) | 0.206 | 111/735 | 102/998 | 0.67 (0.51–0.90) | 0.007 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Others | 46/601 | 59/1132 | 0.69 (0.46–1.03) | 0.07 | 64/902 | 41/831 | 0.70 (0.47–1.05) | 0.087 | 52/735 | 53/998 | 0.76 (0.51–1.13) | 0.178 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I + II + 4s | 184/601 | 285/1132 | 0.83 (0.67–1.02) | 0.08 | 256/902 | 213/831 | 0.91 (0.74–1.11) | 0.346 | 228/735 | 241/998 | 0.78 (0.64–0.96) | 0.019 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III + IV | 150/601 | 244/1132 | 0.85 (0.67–1.07) | 0.157 | 230/902 | 164/831 | 0.77 (0.62–0.96) | 0.022 | 189/735 | 205/998 | 0.77 (0.62–0.97) | 0.023 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: AOR: adjusted odds ratio; CI: confidence interval. aAdjusted for age and gender, omitting the corresponding stratify factor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Knockdown of YTHDC1 significantly inhibits proliferation of neuroblastoma cells
SK-N-BE (2) and SK-N-SH cells transfected with YTHDC1 siRNAs (siRNA-NC, siRNA-488, siRNA-554, and siRNA-702) were collected and lysed for Western blotting after 48 h (Figure 1A). The results showed that the expression level of YTHDC1 in SK-N-BE (2) cells transfected with siRNA-488/siRNA-554/siRNA-702 was about 50% (P < 0.05)/35% (P < 0.01)/42% (P < 0.05) compared with control group (Figure 1B). In SK-N-SH cells transfected with siRNA-488/siRNA-554/siRNA-702, the expression level YTHDC1 was about 66% (P > 0.05)/39% (P < 0.01)/88% (P > 0.05). These results showed that YTHDC1 siRNA could significantly reduce the expression of YTHDC1 in SK-N-BE (2) and SK-N-SH cells.
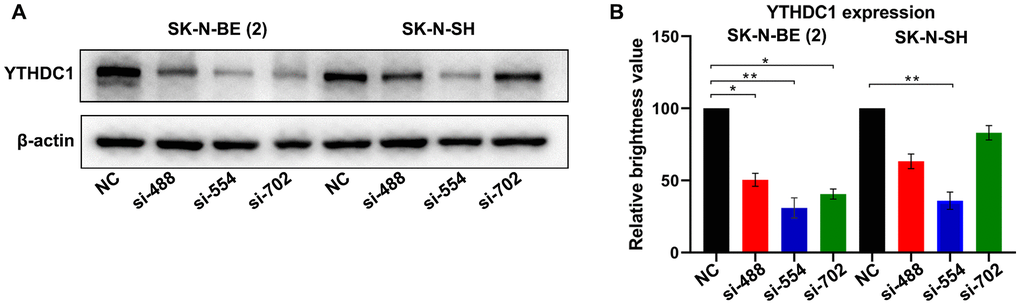
Figure 1. Verification of the silencing effect of different interference sites of YTHDC1 in NB cells. (A) YTHDC1 expression in SK-N-BE (2) and SK-N-SH cells transfected with YTHDC1 siRNAs (siRNA-488, siRNA-554, siRNA-702 and siRNA-NC) were detected by Western blot. (B) Quantitative analysis of YTHDC1 expression in SK-N-BE (2) and SK-N-SH cells.
CCK-8 assay was used to evaluate the cell viability of SK-N-BE (2) and SK-N-SH transfected with YTHDC1 siRNAs (Figure 2A, 2B). The results showed that the activities of SK-N-BE (2) and SK-N-SH cells transfected with siRNA-488 were not obviously affected in different time periods. The proliferation activities of SK-N-BE (2) and SK-N-SH cells transfected with siRNA-554 and siRNA-702 were suppressed dramatically at 72 h (P < 0.05). These results indicated that silencing YTHDC1 would significantly inhibit the proliferation of NB cells.
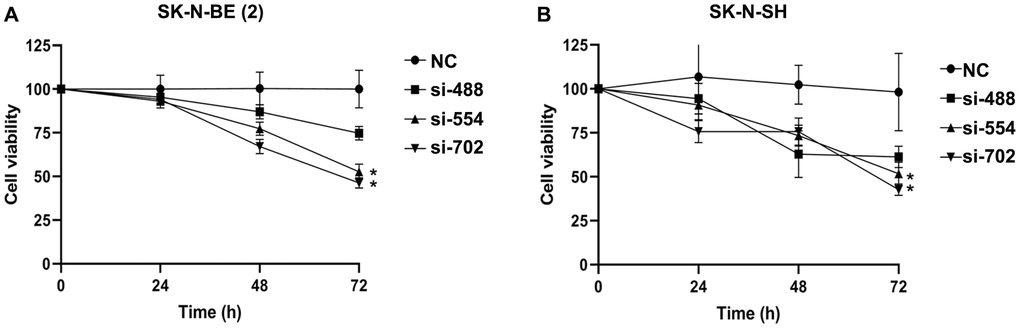
Figure 2. The cell viability of NB transfected with YTHDC1 siRNAs were measured by CCK-8 assay. (A) The cell viability of SK-N-BE (2) transfected with YTHDC1 siRNAs at 24 h, 48 h, 72 h. (B) The SK-N-SH cell viability transfected with YTHDC1 siRNAs. Data were represented as the means ± SD. *P < 0.05.
Knockdown of YTHDC1 inhibits migration of neuroblastoma cells
We further investigated the effect of YTHDC1 silencing on the migration of NB cells through wound healing assays (Figure 3A, 3B). These data showed that the migration inhibition rate of SK-N-BE (2) cells transfected with YTHDC1 siRNA-488/554/702 reached 18% (P > 0.05)/50% (P < 0.01)/55% (P < 0.01). However, among SK-N-SH cells, only the cell line transfected with siRNA-554 was obviously suppressed in the migration ability, with an inhibition rate of 43%.
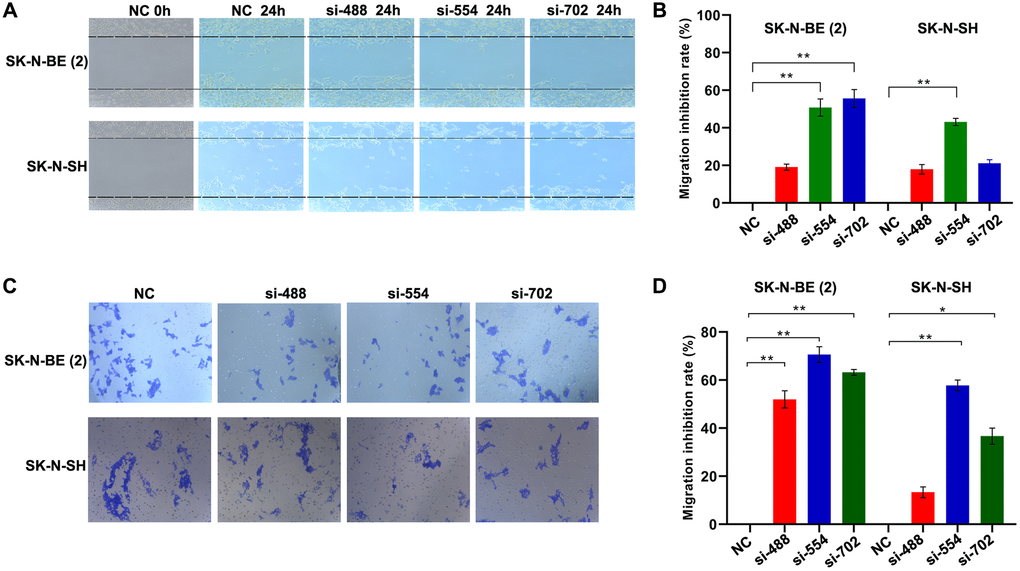
Figure 3. Silencing YTHDC1 inhibited NB cells migration. (A) Migration ability of SK-N-BE (2) and SK-N-SH cells were evaluated by wound healing assay after transfection for 24 h. (B) Quantitative analysis of the migration inhibition rate of SK-N-BE (2) and SK-N-SH cells. (C) Identifying migration ability of SK-N-BE (2) and SK-N-SH cells transfected with YTHDC1 siRNAs for 24 h by transwell migration assay. (D) Quantitative analysis of SK-N-BE (2) and SK-N-SH cell migration inhibition rate. Data were represented as the means ± SD, *P < 0.05, **P < 0.01.
We also investigated the effect of YTHDC1 silencing on the migration of NB cells through migration assays (Figure 3C, 3D). Migration assay results exhibited that the migration inhibition rate of SK-N-BE (2) cells transfected with siRNA-488/554/702 reached 51%/70%/63%, relative to the NC group (P < 0.01). The migration inhibition rate of SK-N-SH cells transfected with siRNA-488 was 13% (P > 0.05), whereas inhibition rate of cells transfected with siRNA-554 and siRNA-702 exceeded 57% and 40% (P < 0.01). These results indicate that silencing the expression of YTHDC1 reduces the migration ability of the NB cells.
Discussion
In this study, we systematically evaluated the associations between common genetic variants in YTHDC1 gene and NB risk. We further characterized the YTHDC1 functionality in NB via molecular biology experiments. Taken together, we highlighted a NB-associated SNP rs3813832 T>C in Chinese population and found that YTHDC1 acts as a NB oncogene.
RNA m6A methylation is an important epigenetic transcriptional modification and has the highest abundance in eukaryotes [24]. Its methylation balance depends on the synergy between the methyltransferase complex (eraser) and the demethylase (writer), and its function depends on the m6A binding protein (reader) [38]. Under their dynamic regulation, m6A plays an important regulatory role in various physiological processes [39]. Multiple evidence suggested that abnormalities of m6A modification are associated with human carcinogenesis, including hepatoblastoma [40], Wilms tumor [41], bladder cancer [34], and endometrial cancer [42]. The genetic variants in critical m6A modification genes may affect the individual’s susceptibility risk to cancers. Zeng et al. [43] genotyped 6 SNPs in FTO gene in samples of 537 breast cancer cases and 537 controls. Of the 6 SNPs analyzed, rs16953002 AA genotype significantly predisposed to a higher breast cancer risk compared to GG genotype, whereas rs1477196 AA genotype was associated with decreased breast cancer risk compared to GG genotype. In addition, Meng et al. [30] demonstrated that SND1 gene rs118049207 could significantly increase the risk of colorectal cancer in the Nanjing and Beijing population of China. Further research revealed the rs118049207 acts as an enhancer of the SND1 intron driven by DMRT3. Compared with adjacent normal tissues, the expression of SND1 mRNA in colorectal tumor tissues increased significantly. They speculated that the genetic variation of m6A-modified genes might be a promising predictor of colorectal cancer risk. Polymorphisms in METTL14 gene [44] and METTL3 gene [45] (m6A methyltransferases) were also reported to be associated with predisposition to neuroblastoma. More recently, our group found that YTHDC1 rs2293596 T>C polymorphism predisposed to hepatoblastoma and YTHDC1 gene polymorphisms may have a cumulative effect on hepatoblastoma risk [46]. We also found that YTHDC1 rs2293595 was associated with a significant inverse association with risk of glioma [33]. The combined effect of YTHDC1 polymorphisms significantly increases Wilms tumor susceptibility [47]. These results indicated that m6A gene variants played an extremely important role in the development of tumors.
The m6A binding proteins (YTHDF1-3, YTHDC1, and YTHDC2) that belong to the YTH domain family are highly conserved in eukaryotic cells [48]. YTHDC1, as an important m6A recognition protein, is involved in the regulation of mRNA shear and mRNA nucleus [26, 49]. Although the function of YTHDC1 is still not fully understood, studies have shown that it plays a regulatory role in pre-mRNA splicing by interacting with SR protein. Based on the combination of transcriptome and PAR-CLIP sequencing technology, Xiao et al. [49] circumstantiated that m6A recruited the precursor mRNA splicing factor SRSF3 through its binding protein YTHDC1 to promote its binding to mRNA, while inhibiting the splicing factor SRSF10 binding to mRNA, thereby it promoted that m6A retains modified exons. In addition, some studies also reported that that YTHDC1 interacted with other splicing factors and could be used as potential tumor suppressors for endometrial cancer [42]. The expression of YTHDC1 has been detected in a panel of prostate cell lines and not in the benign prostate cell lines, indicating that YTHDC1 may function as an oncogene in prostate cancer [50]. These findings indicated that YTHDC1 might play an important role in the process of tumor development.
So far, the association between YTHDC1 gene polymorphisms and NB susceptibility is unclear. Therefore, we explore the correlation between YTHDC1 gene polymorphisms and NB susceptibility based on an eight-center case-control study. Our results showed that rs3813832 T>C could significantly reduce the risk of NB. In addition, stratified analysis revealed that individuals with 3 protective genotypes contributed to a decreased risk of NB in certain subgroups. Subsequently, we further explored whether the expression of YTHDC1 affected the occurrence and development of NB through cell experiments. Based on CCK-8, cell scratch, and cell migration experiments, we found that silencing YTHDC1 would significantly inhibit the proliferation and migration of SK-N-BE (2) and SK-N-SH cells. Among three pairs of siRNA series, the inhibitory ability of siRNA-554 was the strongest, followed by siRNA-702, while the inhibitory ability of siRNA-488 was relatively weak. Combining these siRNA target sequences and the comprehensive analysis of rs3813832 T>C polymorphism site, we found that the rs3813832 T>C site was located in the coding sequence region of YTHDC1, and it was just located in the downstream region near siRNA-554. This finding indicated that the rs3813832 T>C polymorphic site might reduce the expression of YTHDC1 by changing the amino acid composition of YTHDC1, and decrease the risk of individuals suffering from NB. These amino composition changes might affect the pre-mRNA splicing and transport of downstream RNA molecules, and thus ultimately inhibit the proliferation and metastasis of NB. The exact molecular mechanism of YTHDC1 rs3813832 T>C on NB risk is worth further exploring.
Although this study has made some important discoveries, there are still several limitations. First of all, the subjects of this study were all Han population and could not represent the overall level of the Chinese population. In addition, the number of subjects was not large enough, which limited the statistical ability to some extent. It is necessary to further increase the number of research samples in future research. Finally, the research on YTHDC1 and NB proliferation/metastasis-related molecular mechanisms needs more exploration. Of note, the potential mechanism of how these SNPs impacts NB proliferation/metastasis awaits to be elucidated.
In conclusion, our findings indicated that YTHDC1 rs3813832 T>C could significantly reduce the susceptibility of NB. In addition, individuals with multiple protective genotypes were less likely to suffer from NB. Silencing YTHDC1 would inhibit the proliferation and migration of NB. The specific role and regulation mechanism of YTHDC1 rs3813832 T>C in the occurrence and development of NB still needs to be fully elucidated.
Materials and Methods
Study population
A total of 898 patients with NB and 1734 controls were recruited from eight hospitals in Guangzhou, Zhengzhou, Changsha, Wenzhou, Taiyuan, Xi’an, Kunming, and Shenyang (Supplementary Table 1). All cases were newly diagnosed and confirmed as NB by pathology. Participants without NB were recruited as healthy controls during the same period in the same geographic area. Specific recruitment details and selection criteria have been described in our previous studies [44, 51]. Informed consent forms were obtained from the parents or guardians of all participants. Our study has been approved by the Institutional Review Board of Guangzhou Women and Children’s Medical Center (Ethic approve No: 201929300).
Genotyping
The criteria for choosing potential functional polymorphisms of the YTHDC1 gene have been reported minutely in our previous study [46]. The selection criteria were as follows: SNPs are located in the in the 5′- flanking region, exon, 5′- untranslated region (5′UTR), and 3′UTR of YTHDC1; SNPs should be functional variations predicted by SNPinfo (https://snpinfo.niehs.nih.gov/snpinfo/snpfunc.html); the minor allele frequencies should be >5% in Chinese Han population; no significant linkage disequilibrium (LD) existed between selected SNPs (R2 < 0.8). We first screened out 31 potentially functional SNPs in YTHDC1 via SNPinfo [46]. Among them, rs2293596 T>C and rs223595 T>C are located in the 3′UTR, predicting that they are related to microRNA binding. The rs3813832 T>C polymorphism was predicted to contribute to amino acid alteration. LDlink software (https://ldlink.nci.nih.gov/) result indicated that there was no significant LD (R2 < 0.8) among these three selected SNPs (R2 = 0.153 between rs2293596 and rs2293595; R2 = 0.082 between rs2293596 and rs3813832; R2 = 0.537 between rs2293595 and rs3813832). Genomic DNA was extracted from the participants’ venous blood samples. DNA samples were genotyped for the YTHDC1 SNPs (rs2293596 T>C, rs2293595 T>C, and rs3813832 T>C) by ABI 7900HT real-time quantitative PCR instrument (Applied Biosystem, USA). In addition, 10% of DNA samples were chosen for repeated genotyping and the genotyping accuracy rate was 100%.
Cell culture
Human neuroblastoma cell lines SK-N-BE (2) and SK-N-SH were purchased from the American Type Culture Collection (ATCC, USA). All cells were cultured in EMEM medium (ATCC, USA) containing 10% of fetal bovine serum (FBS; Gibco, USA), in an incubator at 37°C with 95% humidity and 5% CO2.
Cell transfection
Three siRNAs (siRNA-488, siRNA-554, and siRNA-702) targeting YTHDC1 gene were designed and synthesized by OBIO Biotechnology Co., Ltd (Shanghai, China). A scrambled siRNA (siRNA-NC) was synthesized as a negative control. All siRNAs sequences were listed in Supplementary Table 2. SK-N-BE (2) and SK-N-SH cells (4 × 105 cells/well) were added to 6-well plates for 24 h in EMEM with 10% FBS before transfection. SK-N-BE (2) and SK-N-SH cells were transfected with YTHDC1 siRNAs in Lipofectamine™ RNAiMAX Transfection Reagent (Thermo Fisher, USA). After transfection, cells were cultured in the incubator for 24 h for subsequent experiments.
Cell proliferation assay
The CCK-8 kit (Dojindo Molecular Technologies, Japan) was used to measure the cell viability. SK-N-BE (2) and SK-N-SH cells (4 × 103 cells/well) were transferred to 96-well plates and then transfected by YTHDC1 siRNAs after 24 h. The optical density values at 450 nm (OD450) of SK-N-BE (2) and SK-N-SH cells treatment with CCK-8 reagent after transfection for 24 h, 48 h, and 72 h were detected by a microplate reader (Thermo Fisher, USA).
Western blotting
The specific steps of Western blotting have been described in a previously published article [52]. After the incubation with anti-YTHDC1 antibody (1:1000), anti-β-actin antibody (1:1000), the membranes were incubated with peroxidase (HRP)-conjugated secondary antibody (1:4000). All the antibodies employed in this study were listed in Supplementary Table 3. The protein bands were detected using SuperSignal™ West Femto maximum sensitivity substrate (Thermo Fisher, USA) and a ChemiDOCTM XRS+ imaging system (Bio-rad, USA). The signal intensities of different protein bands were analyzed with ImageJ software (NIH, USA).
Wound healing assay
SK-N-BE (2) and SK-N-SH cells (2.0 × 105 cells/well) were transferred into 6-well plates and incubated for 24 h and then transfected with YTHDC1 siRNAs. The cell scratches were performed with 10 μL pipette tips, and the cells were cultured with Opti-MEM (Gibco, USA) in the incubator. After incubation for 48 h, the cells were imaged with the fluorescence inverted microscope (Leica, Germany). The cell migration distances were calculated by Image-Pro Plus 6.0 software (Media Cybernetics, USA).
Migration assay
The migration ability of SK-N-BE (2) and SK-N-SH cells transfected with siRNAs were evaluated using transwell assay in the 24-well plates. These cells transfected with siRNAs (2.5 × 104 cells) were seeded into the 8 μm transwell upper chamber (BD Biosciences, USA) in 150 μL of EMEM basic medium. EMEM medium (700 μL) with 10% FBS was used as a chemo-attractant in the lower chamber. After 24 h, the cells that migrated to the lower surface of chamber were fixed with 70% absolute ethanol and stained with 0.1% crystal violet and imaged using the inverted microscope (Leica, Germany).
Statistical analysis
In this study, statistical analysis was performed by SAS 9.4 software (SAS Institute Inc, USA). The distribution of sample characteristics between all NB cases and the control group was verified using a two-sided χ2 test. The goodness-of-fit chi-square test was used to test whether the genotype frequency in the control conforms to HWE. Based on unconditional logistic regression analysis, the AOR and 95% CI were calculated to assess the association between YTHDC1 polymorphisms and NB risk. In addition, the cell functional experiments were performed independently for three times and the relevant data obtained were displayed with the mean ± SD. The SPSS 20.0 software (IBM, USA) was used for statistical analysis based on the least difference test by one-way analysis of variance (ANOVA). The standard with statistical significance were *P value < 0.05 and **P value < 0.01.
Supplementary Materials
Author Contributions
All authors contributed significantly to this work. Y. Li, T. Lu, J. Wang, Z. Zhuo, L. Miao, Z. Yang, J. Zhang, J. Cheng, H. Zhou, S. Li, L. Li, A. Li and J. He performed the research study and collected the samples and data; J. He analyzed the data; A. Li and J. He conceptualized and designed the research study; Y. Li, T. Lu, Z. Zhuo, A. Li and J. He wrote the paper; J. He prepared all the Tables; T. Lu, Z. Zhuo and L. Miao prepared all the Figures. All authors reviewed the manuscript. In addition, all authors have read and approved the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Funding
This study was supported by grants from National Natural Science Foundation of China (No. 82173593, 82002636, 82002635), Natural Science Foundation of Guangdong Province (No. 2019A1515010360), Natural Science Foundation Project of Hunan Province (No. 2018JJ2210, 2020SK50501), China Postdoctoral Science Foundation (No. 2020T130132, 2020M682668).
References
- 1. Nakagawara A, Li Y, Izumi H, Muramori K, Inada H, Nishi M. Neuroblastoma. Jpn J Clin Oncol. 2018; 48:214–41. https://doi.org/10.1093/jjco/hyx176 [PubMed]
- 2. Maris JM, Hogarty MD, Bagatell R, Cohn SL. Neuroblastoma. Lancet. 2007; 369:2106–20. https://doi.org/10.1016/S0140-6736(07)60983-0 [PubMed]
- 3. Hero B, Simon T, Spitz R, Ernestus K, Gnekow AK, Scheel-Walter HG, Schwabe D, Schilling FH, Benz-Bohm G, Berthold F. Localized infant neuroblastomas often show spontaneous regression: results of the prospective trials NB95-S and NB97. J Clin Oncol. 2008; 26:1504–10. https://doi.org/10.1200/JCO.2007.12.3349 [PubMed]
- 4. Matthay KK, Reynolds CP, Seeger RC, Shimada H, Adkins ES, Haas-Kogan D, Gerbing RB, London WB, Villablanca JG. Long-term results for children with high-risk neuroblastoma treated on a randomized trial of myeloablative therapy followed by 13-cis-retinoic acid: a children's oncology group study. J Clin Oncol. 2009; 27:1007–13. https://doi.org/10.1200/JCO.2007.13.8925 [PubMed]
- 5. He X, Qin C, Zhao Y, Zou L, Zhao H, Cheng C. Gene signatures associated with genomic aberrations predict prognosis in neuroblastoma. Cancer Commun (Lond). 2020; 40:105–18. https://doi.org/10.1002/cac2.12016 [PubMed]
- 6. Yue ZX, Xing TY, Gao C, Liu SG, Zhao W, Zhao Q, Wang XS, Jin M, Ma XL. Chromosome band 11q23 deletion predicts poor prognosis in bone marrow metastatic neuroblastoma patients without MYCN amplification. Cancer Commun (Lond). 2019; 39:68. https://doi.org/10.1186/s40880-019-0409-1 [PubMed]
- 7. Bourdeaut F, Trochet D, Janoueix-Lerosey I, Ribeiro A, Deville A, Coz C, Michiels JF, Lyonnet S, Amiel J, Delattre O. Germline mutations of the paired-like homeobox 2B (PHOX2B) gene in neuroblastoma. Cancer Lett. 2005; 228:51–8. https://doi.org/10.1016/j.canlet.2005.01.055 [PubMed]
- 8. Mossé YP, Laudenslager M, Longo L, Cole KA, Wood A, Attiyeh EF, Laquaglia MJ, Sennett R, Lynch JE, Perri P, Laureys G, Speleman F, Kim C, et al. Identification of ALK as a major familial neuroblastoma predisposition gene. Nature. 2008; 455:930–5. https://doi.org/10.1038/nature07261 [PubMed]
- 9. Matthay KK, Maris JM, Schleiermacher G, Nakagawara A, Mackall CL, Diller L, Weiss WA. Neuroblastoma. Nat Rev Dis Primers. 2016; 2:16078. https://doi.org/10.1038/nrdp.2016.78 [PubMed]
- 10. Patton T, Olshan AF, Neglia JP, Castleberry RP, Smith J. Parental exposure to medical radiation and neuroblastoma in offspring. Paediatr Perinat Epidemiol. 2004; 18:178–85. https://doi.org/10.1111/j.1365-3016.2004.00554.x [PubMed]
- 11. Han W, Zhou Y, Zhong R, Wu C, Song R, Liu L, Zou L, Qiao Y, Zhai K, Chang J, Huang L, Liu L, Lu X, et al. Functional polymorphisms in FAS/FASL system increase the risk of neuroblastoma in Chinese population. PLoS One. 2013; 8:e71656. https://doi.org/10.1371/journal.pone.0071656 [PubMed]
- 12. Tonini GP, Capasso M. Genetic predisposition and chromosome instability in neuroblastoma. Cancer Metastasis Rev. 2020; 39:275–85. https://doi.org/10.1007/s10555-020-09843-4 [PubMed]
- 13. Capasso M, Devoto M, Hou C, Asgharzadeh S, Glessner JT, Attiyeh EF, Mosse YP, Kim C, Diskin SJ, Cole KA, Bosse K, Diamond M, Laudenslager M, et al. Common variations in BARD1 influence susceptibility to high-risk neuroblastoma. Nat Genet. 2009; 41:718–23. https://doi.org/10.1038/ng.374 [PubMed]
- 14. Wang K, Diskin SJ, Zhang H, Attiyeh EF, Winter C, Hou C, Schnepp RW, Diamond M, Bosse K, Mayes PA, Glessner J, Kim C, Frackelton E, et al. Integrative genomics identifies LMO1 as a neuroblastoma oncogene. Nature. 2011; 469:216–20. https://doi.org/10.1038/nature09609 [PubMed]
- 15. Diskin SJ, Capasso M, Schnepp RW, Cole KA, Attiyeh EF, Hou C, Diamond M, Carpenter EL, Winter C, Lee H, Jagannathan J, Latorre V, Iolascon A, et al. Common variation at 6q16 within HACE1 and LIN28B influences susceptibility to neuroblastoma. Nat Genet. 2012; 44:1126–30. https://doi.org/10.1038/ng.2387 [PubMed]
- 16. Diskin SJ, Capasso M, Diamond M, Oldridge DA, Conkrite K, Bosse KR, Russell MR, Iolascon A, Hakonarson H, Devoto M, Maris JM. Rare variants in TP53 and susceptibility to neuroblastoma. J Natl Cancer Inst. 2014; 106:dju047. https://doi.org/10.1093/jnci/dju047 [PubMed]
- 17. Russell MR, Penikis A, Oldridge DA, Alvarez-Dominguez JR, McDaniel L, Diamond M, Padovan O, Raman P, Li Y, Wei JS, Zhang S, Gnanchandran J, Seeger R, et al. CASC15-S Is a Tumor Suppressor lncRNA at the 6p22 Neuroblastoma Susceptibility Locus. Cancer Res. 2015; 75:3155–66. https://doi.org/10.1158/0008-5472.CAN-14-3613 [PubMed]
- 18. McDaniel LD, Conkrite KL, Chang X, Capasso M, Vaksman Z, Oldridge DA, Zachariou A, Horn M, Diamond M, Hou C, Iolascon A, Hakonarson H, Rahman N, et al. Common variants upstream of MLF1 at 3q25 and within CPZ at 4p16 associated with neuroblastoma. PLoS Genet. 2017; 13:e1006787. https://doi.org/10.1371/journal.pgen.1006787 [PubMed]
- 19. Capasso M, McDaniel LD, Cimmino F, Cirino A, Formicola D, Russell MR, Raman P, Cole KA, Diskin SJ. The functional variant rs34330 of CDKN1B is associated with risk of neuroblastoma. J Cell Mol Med. 2017; 21:3224–30. https://doi.org/10.1111/jcmm.13226 [PubMed]
- 20. Avitabile M, Lasorsa VA, Cantalupo S, Cardinale A, Cimmino F, Montella A, Capasso D, Haupt R, Amoroso L, Garaventa A, Quattrone A, Corrias MV, Iolascon A, Capasso M. Association of PARP1 polymorphisms with response to chemotherapy in patients with high-risk neuroblastoma. J Cell Mol Med. 2020; 24:4072–81. https://doi.org/10.1111/jcmm.15058 [PubMed]
- 21. Olivera GG, Yáñez Y, Gargallo P, Sendra L, Aliño SF, Segura V, Sanz MÁ, Cañete A, Castel V, Font De Mora J, Hervás D, Berlanga P, Herrero MJ. MTHFR and VDR Polymorphisms Improve the Prognostic Value of MYCN Status on Overall Survival in Neuroblastoma Patients. Int J Mol Sci. 2020; 21:2714. https://doi.org/10.3390/ijms21082714 [PubMed]
- 22. Avitabile M, Succoio M, Testori A, Cardinale A, Vaksman Z, Lasorsa VA, Cantalupo S, Esposito M, Cimmino F, Montella A, Formicola D, Koster J, Andreotti V, et al. Neural crest-derived tumor neuroblastoma and melanoma share 1p13.2 as susceptibility locus that shows a long-range interaction with the SLC16A1 gene. Carcinogenesis. 2020; 41:284–95. https://doi.org/10.1093/carcin/bgz153 [PubMed]
- 23. Testori A, Lasorsa VA, Cimmino F, Cantalupo S, Cardinale A, Avitabile M, Limongelli G, Russo MG, Diskin S, Maris J, Devoto M, Keavney B, Cordell HJ, et al. Exploring Shared Susceptibility between Two Neural Crest Cells Originating Conditions: Neuroblastoma and Congenital Heart Disease. Genes (Basel). 2019; 10:663. https://doi.org/10.3390/genes10090663 [PubMed]
- 24. Meyer KD, Saletore Y, Zumbo P, Elemento O, Mason CE, Jaffrey SR. Comprehensive analysis of mRNA methylation reveals enrichment in 3' UTRs and near stop codons. Cell. 2012; 149:1635–46. https://doi.org/10.1016/j.cell.2012.05.003 [PubMed]
- 25. Zhao W, Qi X, Liu L, Ma S, Liu J, Wu J. Epigenetic Regulation of m6A Modifications in Human Cancer. Mol Ther Nucleic Acids. 2020; 19:405–12. https://doi.org/10.1016/j.omtn.2019.11.022 [PubMed]
- 26. Zhao BS, Roundtree IA, He C. Post-transcriptional gene regulation by mRNA modifications. Nat Rev Mol Cell Biol. 2017; 18:31–42. https://doi.org/10.1038/nrm.2016.132 [PubMed]
- 27. Yang Y, Hsu PJ, Chen YS, Yang YG. Dynamic transcriptomic m6A decoration: writers, erasers, readers and functions in RNA metabolism. Cell Res. 2018; 28:616–24. https://doi.org/10.1038/s41422-018-0040-8 [PubMed]
- 28. Zhou C, Zhang Z, Zhu X, Qian G, Zhou Y, Sun Y, Yu W, Wang J, Lu H, Lin F, Shen Z, Zheng S. N6-Methyladenosine modification of the TRIM7 positively regulates tumorigenesis and chemoresistance in osteosarcoma through ubiquitination of BRMS1. EBioMedicine. 2020; 59:102955. https://doi.org/10.1016/j.ebiom.2020.102955 [PubMed]
- 29. Zhang S, Zhao BS, Zhou A, Lin K, Zheng S, Lu Z, Chen Y, Sulman EP, Xie K, Bögler O, Majumder S, He C, Huang S. m6A Demethylase ALKBH5 Maintains Tumorigenicity of Glioblastoma Stem-like Cells by Sustaining FOXM1 Expression and Cell Proliferation Program. Cancer Cell. 2017; 31:591–606.e6. https://doi.org/10.1016/j.ccell.2017.02.013 [PubMed]
- 30. Meng Y, Li S, Gu D, Xu K, Du M, Zhu L, Chu H, Zhang Z, Wu Y, Fu Z, Wang M. Genetic variants in m6A modification genes are associated with colorectal cancer risk. Carcinogenesis. 2020; 41:8–17. https://doi.org/10.1093/carcin/bgz165 [PubMed]
- 31. Li Z, Weng H, Su R, Weng X, Zuo Z, Li C, Huang H, Nachtergaele S, Dong L, Hu C, Qin X, Tang L, Wang Y, et al. FTO Plays an Oncogenic Role in Acute Myeloid Leukemia as a N6-Methyladenosine RNA Demethylase. Cancer Cell. 2017; 31:127–41. https://doi.org/10.1016/j.ccell.2016.11.017 [PubMed]
- 32. Yang Z, Jiang X, Li D, Jiang X. HBXIP promotes gastric cancer via METTL3-mediated MYC mRNA m6A modification. Aging (Albany NY). 2020; 12:24967–82. https://doi.org/10.18632/aging.103767 [PubMed]
- 33. He J, Yuan L, Lin H, Lin A, Chen H, Luo A, Zhuo Z, Liu X. Genetic variants in m6A modification core genes are associated with glioma risk in Chinese children. Mol Ther Oncolytics. 2021; 20:199–208. https://doi.org/10.1016/j.omto.2020.12.013 [PubMed]
- 34. Han J, Wang JZ, Yang X, Yu H, Zhou R, Lu HC, Yuan WB, Lu JC, Zhou ZJ, Lu Q, Wei JF, Yang H. METTL3 promote tumor proliferation of bladder cancer by accelerating pri-miR221/222 maturation in m6A-dependent manner. Mol Cancer. 2019; 18:110. https://doi.org/10.1186/s12943-019-1036-9 [PubMed]
- 35. Liu H, Gu J, Jin Y, Yuan Q, Ma G, Du M, Ge Y, Qin C, Lv Q, Fu G, Wang M, Chu H, Yuan L, Zhang Z. Genetic variants in N6-methyladenosine are associated with bladder cancer risk in the Chinese population. Arch Toxicol. 2021; 95:299–309. https://doi.org/10.1007/s00204-020-02911-2 [PubMed]
- 36. Fu Y, Dominissini D, Rechavi G, He C. Gene expression regulation mediated through reversible m6A RNA methylation. Nat Rev Genet. 2014; 15:293–306. https://doi.org/10.1038/nrg3724 [PubMed]
- 37. Liu N, Dai Q, Zheng G, He C, Parisien M, Pan T. N(6)-methyladenosine-dependent RNA structural switches regulate RNA-protein interactions. Nature. 2015; 518:560–4. https://doi.org/10.1038/nature14234 [PubMed]
- 38. Meyer KD, Jaffrey SR. Rethinking m6A Readers, Writers, and Erasers. Annu Rev Cell Dev Biol. 2017; 33:319–42. https://doi.org/10.1146/annurev-cellbio-100616-060758 [PubMed]
- 39. Niu Y, Zhao X, Wu YS, Li MM, Wang XJ, Yang YG. N6-methyl-adenosine (m6A) in RNA: an old modification with a novel epigenetic function. Genomics Proteomics Bioinformatics. 2013; 11:8–17. https://doi.org/10.1016/j.gpb.2012.12.002 [PubMed]
- 40. Liu L, Wang J, Sun G, Wu Q, Ma J, Zhang X, Huang N, Bian Z, Gu S, Xu M, Yin M, Sun F, Pan Q. Correction to: m6A mRNA methylation regulates CTNNB1 to promote the proliferation of hepatoblastoma. Mol Cancer. 2020; 19:24. https://doi.org/10.1186/s12943-020-1136-6 [PubMed]
- 41. Hua RX, Liu J, Fu W, Zhu J, Zhang J, Cheng J, Li S, Zhou H, Xia H, He J, Zhuo Z. ALKBH5 gene polymorphisms and Wilms tumor risk in Chinese children: A five-center case-control study. J Clin Lab Anal. 2020; 34:e23251. https://doi.org/10.1002/jcla.23251 [PubMed]
- 42. Zhang B, zur Hausen A, Orlowska-Volk M, Jäger M, Bettendorf H, Stamm S, Hirschfeld M, Yiqin O, Tong X, Gitsch G, Stickeler E. Alternative splicing-related factor YT521: an independent prognostic factor in endometrial cancer. Int J Gynecol Cancer. 2010; 20:492–9. https://doi.org/10.1111/IGC.0b013e3181d66ffe [PubMed]
- 43. Zeng X, Ban Z, Cao J, Zhang W, Chu T, Lei D, Du Y. Association of FTO Mutations with Risk and Survival of Breast Cancer in a Chinese Population. Dis Markers. 2015; 2015:101032. https://doi.org/10.1155/2015/101032 [PubMed]
- 44. Zhuo Z, Lu H, Zhu J, Hua RX, Li Y, Yang Z, Zhang J, Cheng J, Zhou H, Li S, Li L, Xia H, He J. METTL14 Gene Polymorphisms Confer Neuroblastoma Susceptibility: An Eight-Center Case-Control Study. Mol Ther Nucleic Acids. 2020; 22:17–26. https://doi.org/10.1016/j.omtn.2020.08.009 [PubMed]
- 45. Bian J, Zhuo Z, Zhu J, Yang Z, Jiao Z, Li Y, Cheng J, Zhou H, Li S, Li L, He J, Liu Y. Association between METTL3 gene polymorphisms and neuroblastoma susceptibility: A nine-centre case-control study. J Cell Mol Med. 2020; 24:9280–6. https://doi.org/10.1111/jcmm.15576 [PubMed]
- 46. Chen H, Li Y, Li L, Zhu J, Yang Z, Zhang J, Li S, Xin Y, Xia H, He J. YTHDC1 gene polymorphisms and hepatoblastoma susceptibility in Chinese children: A seven-center case-control study. J Gene Med. 2020; 22:e3249. https://doi.org/10.1002/jgm.3249 [PubMed]
- 47. Lin A, Hua RX, Zhou M, Fu W, Zhang J, Zhou H, Li S, Cheng J, Zhu J, Xia H, Liu G, He J. YTHDC1 gene polymorphisms and Wilms tumor susceptibility in Chinese children: A five-center case-control study. Gene. 2021; 783:145571. https://doi.org/10.1016/j.gene.2021.145571 [PubMed]
- 48. Yang N, Ying P, Tian J, Wang X, Mei S, Zou D, Peng X, Gong Y, Yang Y, Zhu Y, Ke J, Zhong R, Chang J, Miao X. Genetic variants in m6A modification genes are associated with esophageal squamous-cell carcinoma in the Chinese population. Carcinogenesis. 2020; 41:761–8. https://doi.org/10.1093/carcin/bgaa012 [PubMed]
- 49. Xiao W, Adhikari S, Dahal U, Chen YS, Hao YJ, Sun BF, Sun HY, Li A, Ping XL, Lai WY, Wang X, Ma HL, Huang CM, et al. Nuclear m(6)A Reader YTHDC1 Regulates mRNA Splicing. Mol Cell. 2016; 61:507–19. https://doi.org/10.1016/j.molcel.2016.01.012 [PubMed]
- 50. Luxton HJ, Simpson BS, Mills IG, Brindle NR, Ahmed Z, Stavrinides V, Heavey S, Stamm S, Whitaker HC. The Oncogene Metadherin Interacts with the Known Splicing Proteins YTHDC1, Sam68 and T-STAR and Plays a Novel Role in Alternative mRNA Splicing. Cancers (Basel). 2019; 11:1233. https://doi.org/10.3390/cancers11091233 [PubMed]
- 51. Zhuo Z, Zhou C, Fang Y, Zhu J, Lu H, Zhou H, Wu H, Wang Y, He J. Correlation between the genetic variants of base excision repair (BER) pathway genes and neuroblastoma susceptibility in eastern Chinese children. Cancer Commun (Lond). 2020; 40:641–6. https://doi.org/10.1002/cac2.12088 [PubMed]
- 52. Lu T, Wu B, Yu Y, Zhu W, Zhang S, Zhang Y, Guo J, Deng N. Blockade of ONECUT2 expression in ovarian cancer inhibited tumor cell proliferation, migration, invasion and angiogenesis. Cancer Sci. 2018; 109:2221–34. https://doi.org/10.1111/cas.13633 [PubMed]