



Introduction
Cancer is the leading cause of death in the world and has become a major public health problem that has persisted worldwide, for a long time. Whether in developed or developing countries, many cancer-related deaths occur every day. For example, based on human epidemiology data, 4,950 people die of cancer every day in the USA [1], this is even worse in China, where over 7,500 people die of cancer, daily [2]. Obviously, all countries will face great challenges in dealing with the huge and increasing burden of cancer at present and in the foreseeable future. To overcome these challenges, it is necessary to increase investment in basic and clinical research to further promote treatment options, which will undoubtedly accelerate the progress of fighting cancer. Patients suffering with cancer still face the challenge of high recurrence rate after surgery and the toxicity of conventional chemotherapy, so safer and more effective treatment schemes are needed.
Targeted molecular therapy holds great promise for the treatment of cancer and represents a revolutionary breakthrough in personalized medicine. Among breast cancer and ovarian cancer patients with BRCA mutations, targeted therapy has always been a hot topic. In this regard, poly ADP ribose polymerase (PARP) inhibitor (PARPi), represent a novel cancer therapy targeting PARP, which have already achieved noteworthy therapeutic effects on cancer. Greater potency might be achieved by inhibiting PARP, because PARPi could sensitize cancer cells to conventional treatments including multiple chemotherapy or radiotherapy that cause DNA damage [3]. Using the genetic concept of synthetic lethality [3, 4], PARP inhibitors are designed to target cancers harbouring specific DNA-repair defects, including those arising in carriers of BRCA1 or BRCA2 mutations [5]. More promisingly, tumors exhibiting BRCAness are sensitive to PARPis, and the concept of BRCAness can be described as a defect in DNA damage response by homologous recombination repair, regardless of the presence of germline BRCA1 or BRCA2 mutations.
Excitingly, numerous studies have demonstrated that PARPis achieve excellent anti-tumor efficacy as monotherapy or combination therapy with conventional treatments in various cancers patients, especially in breast cancer and ovarian cancer. Based on the results of clinical trials, the ASCO guidelines recommended PARP inhibitors for the treatment of ovarian cancer, breast cancer, and pancreatic cancer with BRCA1 / 2 mutations [6–8].
Enhanced understanding of the efficacy of PARPis in ovarian and breast cancer patients carrying BRCAm will provide more accurate treatment information and can improve clinical decision-making. The objective of this study was to perform a meta-analysis to provide a clinical reference by comprehensively evaluating the OS and PFS of ovarian and breast cancer with BRCA mutations.
Results
Literature search
According to the search terms, a total of 2,829 related studies were identified from all searched databases. Because of duplications, 902 studies were removed. After eligibility screening of the titles, abstracts and full texts of the article, 1,895 studies were excluded because they have the characteristics of phase I clinical trial, basic research, preclinical trial, guideline, meeting, nontumor disease and insufficient data. After that, 32 trials related to evaluating the PFS or OS of PARPis in ovarian cancer, breast cancer, lung cancer, prostate cancer, pancreatic cancer, gastric cancer, glioblastoma, colorectal cancer and melanoma were retained. Finally, by analyzing breast and ovarian cancer with BRCA mutations, 15 randomized controlled trials were selected [9–27]. The flowchart of the trial selection process is shown in Figure 1.
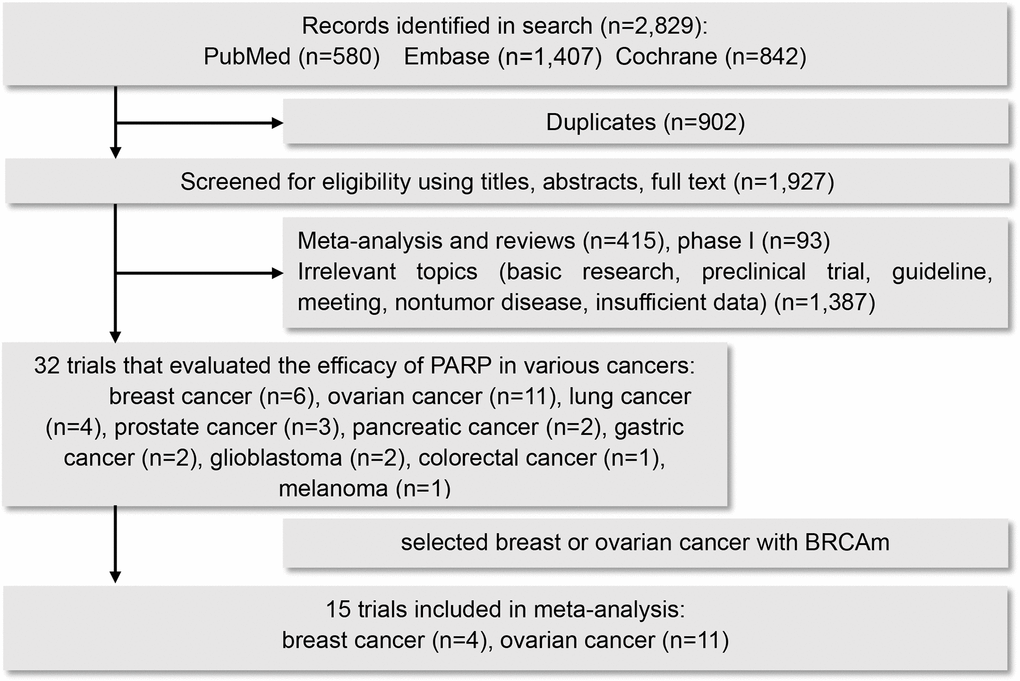
Figure 1. Flow diagram for selection of studies.
Study characteristics
The main characteristics of the eligible trials are showed in Table 1. 15 trials were involved in the analysis, including 11 trials concerning ovarian cancer, 4 trials concerning breast cancer. A total of 3,756 patients carrying BRCA mutations were included in the meta-analysis, of which breast cancer patients accounted for 40% and ovarian cancer patients for 60%. For ovarian cancer, more studies were performed to evaluate the efficacy of PARPis monotherapy as maintenance therapy, while for breast cancer, more studies were performed to evaluate the efficacy of combination of PARPis and conventional chemotherapy. Compared with the other PARPis, olaparib were mostly concerned about in these included clinical trials.
Table 1. Characteristics of the eligible trials in the meta-analysis.
| Cancer type | Trial, year | Phase | Therapeutic regimen | All patients (Exp/Con) | Cancer stage | Median PFS (Exp/Con) | |
| PARP inhibitor | Control | ||||||
| Ovarian cancer | Kaye 2012 | II | Olaparib | Pegylated liposomal doxorubicin | 64/33 | Recurrent ovarian cancer | 6.5 or 8.8/7.1 months |
| Ledermann 2012,2014,2016 | II | Olaparib | Placebo | 136/129 | Relapsed high-grade serous ovarian cancer | 11.2/4.3 months | |
| Oza 2014 | II | Olaparib plus chemotherapy, then olaparib | Chemotherapy then no further treatment | 81/81 | Recurrent high-grade serous ovarian cancer | not reported/9.7months | |
| Mirza 2016 | III | Niraparib | Placebo | 372/181 | Recurrent high grade serous ovarian cancer | 21.0/5.5 months | |
| Pujade-Lauraine 2017 | III | Olaparib | Placebo | 196/99 | Relapsed high-grade ovarian cancer | 19.1/5.5 months | |
| Coleman 2017 | III | Rucaparib | Placebo | 375/189 | Recurrent high-grade ovarian carcinoma | 16.6/5.4 months | |
| Moore 2018 | III | Olaparib | Placebo | 260/131 | Newly diagnosed high-grade ovarian, primary peritoneal, or fallopian tube carcinoma | 49.9/13.8 months | |
| Ray-Coquard 2019 | III | Olaparib plus bevacizumab | Placebo plus bevacizumab | 537/269 | Newly diagnosed high-grade ovarian cancer, primary peritoneal cancer, or fallopian-tube cancer | 37.2/21.7 months | |
| González-Martín 2019 | III | Niraparib | Placebo | 487/246 | Newly diagnosed high-grade ovarian cancer, primary peritoneal cancer, or fallopian-tube cancer | 22.1/10.9 months | |
| Coleman 2019 | III | Veliparib plus carboplatin and paclitaxel then veliparib | Placebo plus carboplatin and paclitaxel then placebo | 382/375 | Newly diagnosed high-grade ovarian, fallopian tube, or primary peritoneal carcinoma | 34.7/22.0 months | |
| Penson 2020 | III | Olaparib | Single-agent nonplatinum chemotherapy | 178/88 | Relapsed high-grade ovarian cancer | 13.2/8.5 months | |
| Breast cancer | Robson 2017,2019 | III | Olaparib | Standard therapy (capecitabine, eribulin, or vinorelbine) | 205/97 | Metastatic breast cancer | 7.0/4.2 months |
| Han 2018 | II | Veliparib plus carboplatin /paclitaxel | Placebo plus carboplatin /paclitaxel | 95/98 | Recurrent/metastatic breast cancer | 14.1/12.3 months | |
| Litton 2018, 2020 | III | Talazoparib | Standard therapy (capecitabine, eribulin, or vinorelbine | 287/144 | Advanced Breast Cancer | 8.6/5.6 months | |
| Diéras 2020 | III | Olaparib | Placebo plus carboplatin and paclitaxel | 337/172 | Advanced Breast Cancer | 14.5/12.6 months | |
Efficacy of PARPis in breast or ovarian cancer with BRCAm, BRCA1m, BRCA2m
Significantly, patients with breast or ovarian cancer in PARPis treatment groups had a considerable advantage in PFS compared with control groups (for breast cancer, BRCAm: HR 0.64, 95% CI=0.55-0.75, P<0.001; BRCA1m: HR 0.64, 95% CI=0.53-0.78, P<0.001; BRCA2m:HR 0.62, 95% CI=0.51-0.76, P<0.001; for ovarian cancer, BRCAm: HR 0.33, 95% CI=0.27-0.42, P<0.001; BRCA1m: HR 0.38, 95% CI=0.29-0.48, P<0.001; BRCA2m: HR 0.24, 95% CI=0.10-0.59, P=0.002). However, compared with the control groups, PARPis did not improve OS in breast cancer or ovarian cancer patients (for breast cancer, BRCAm: HR 0.87, 95% CI=0.76-1.01, P=0.065; for ovarian cancer, BRCAm: HR 0.78, 95% CI=0.61-1.01, P=0.058). For breast cancer, no substantial heterogeneity was observed in subgroups of BRCAm, BRCA1m or BRCA2m cancers when assessing both PFS and OS; for ovarian cancer, heterogeneity exited in subgroups of BRCAm and BRCAm1 cancers when assessing PFS, but not in the other subgroups when assessing PFS or OS (see Figures 2, 3 and Supplementary Figures 1, 2).
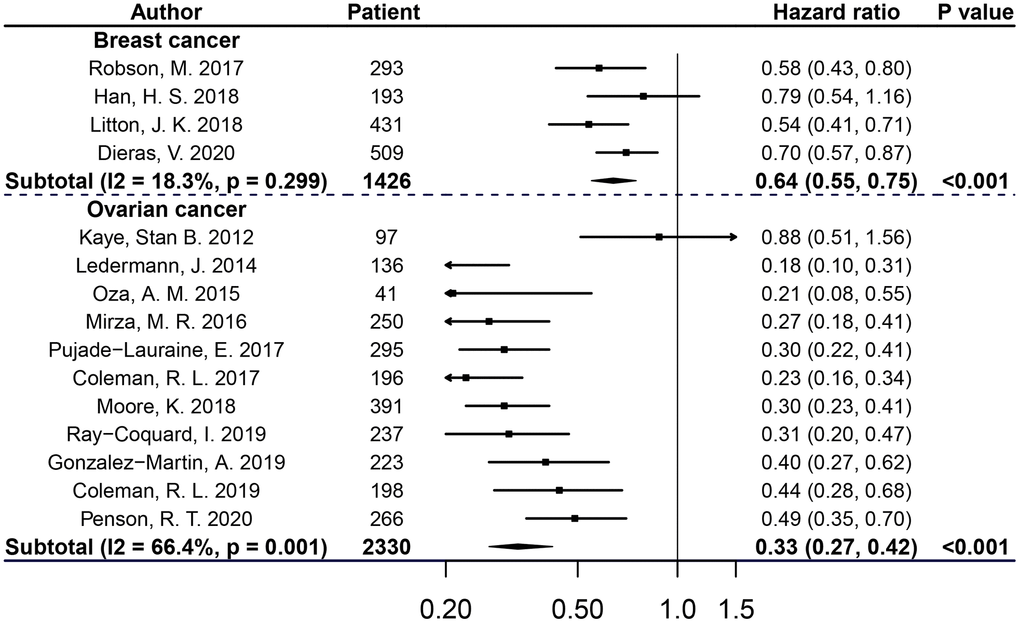
Figure 2. PFS of breast or ovarian cancer patients with BRCAm treated with PARPis.
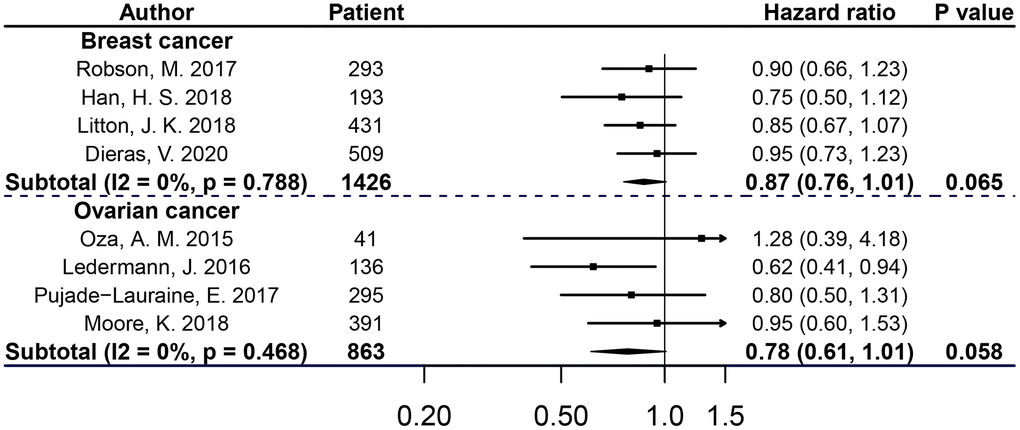
Figure 3. OS of breast or ovarian cancer patients with BRCAm treated with PARPis.
The efficacy of each PARPi in BRCAm cancer by pooling data from breast and ovarian cancer patients
Compared with the control groups, all PARPis included in the analysis were statistically significant in improving PFS of patients with BRCAm cancers. Compared olaparib group with control group, HRs for PFS and OS of cancer patients with BRCAm were 0.37 (95% CI=0.27-0.50, P<0.001), 0.83 (95% CI=0.68-1.01, P=0.059), respectively (see Figure 4).
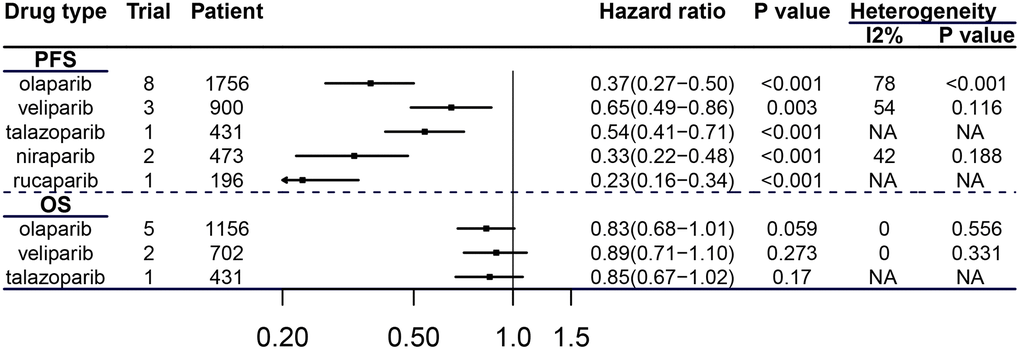
Figure 4. Efficacy of each PARPi in breast and ovarian cancer patients with BRCAm.
The efficacy of PARP inhibitors used with different intervention methods
Compared with the control groups, PAPRis with different intervention methods were all statistically significant beneficial for PFS of patients carrying BRCAm by integrating data from these two cancer types. (parp+ct vs ct+placebo: HR 0.48, 95% CI=0.32-0.72, P<0.001; parp vs ct: HR 0.56, 95% CI=0.47-0.67, P<0.001; parp vs placebo: HR 0.28, 95% CI=0.24-0.34, P<0.001); for subgroup of “parp vs placebo” PARPis had a statistically significant advantage over placebo for OS of patients in these subgroup (see Figure 5) (HR 0.76, 95% CI=0.76-0.99, P=0.042).
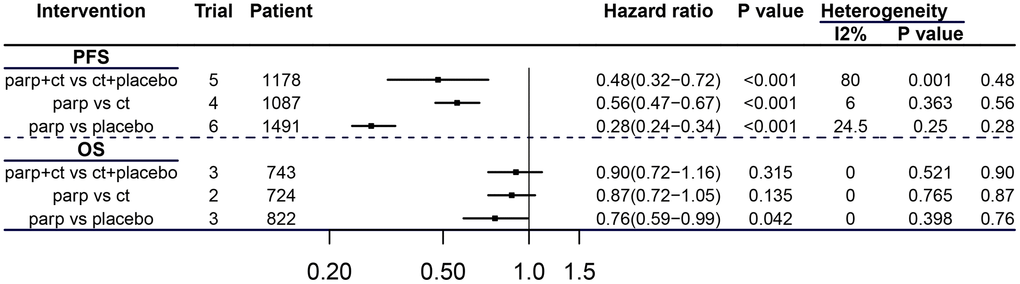
Figure 5. Efficacy of PARPis with different interventions in breast and ovarian cancer patients with BRCAm. CT = chemotherapy.
Efficacy of PARPis in patients with BRCA mutant ovarian cancer at different stages of development
In patients with recurrent ovarian cancer, median PFS was 15.1 months in the PARPis treatment group versus 5.5 months in the control groups, yielding a PFS benefit of 9.6 months; remarkably, in patients with newly diagnosed advanced ovarian cancer, it was 36 months versus 13.5 months, prominently yielding a PFS benefit of 22.5 months (see Table 2). Therefore, the patients of BRCAm ovarian cancer can get better survival when PARPis are administered earlier in cancer progression.
Table 2. Median PFS of patient with BRCA mutant ovarian cancer treated with PARPis.
| Stage of cancer | Trial | Median PFS months(exp) | Median PFS months (con) | N patients (exp) | N patients (con) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrence | Kaye 2012 | 6.5/8.8 | 7.1 | 32/32 | 33 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ledermann2012,2014,2016 | 11.2 | 4.3 | 74 | 62 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Oza 2014 | NA | 9.7 | 20 | 21 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mirza 2016 | 21 | 5.5 | 138 | 65 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pujade-Lauraine 2017 | 19.1 | 5.5 | 196 | 99 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Coleman 2017 | 16.6 | 5.4 | 130 | 66 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Penson 2020 | 13.2 | 8.5 | 178 | 88 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pooled patient-level data | 15.1 | 5.5 | 800 | 434 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Newly diagnosed | Moore 2018 | 49.9 | 13.8 | 260 | 131 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ray-Coquard 2019 | 37.2 | 21.7 | 157 | 80 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| González-Martín 2019 | 22.1 | 10.9 | 152 | 71 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Coleman 2019 | 34.7 | 22 | 108 | 92 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pooled patient-level data | 36 | 13.5 | 677 | 374 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NA=not available. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Publication bias
As visually assessed, substantial asymmetry was not identified in the Begg funnel plot (see Supplementary Figure 3). Moreover, no significant publication bias was found by the Begg rank correlation test and Egger linear regression test.
Discussion
Rapid death is the inevitable outcome of patients with advanced or metastatic breast and ovarian cancer. It is urgent that an effective solution emerges to manage patients of advanced or metastatic breast and ovarian cancer.
Multiple meta-analysis of patients with ovarian cancer or breast cancer had proved that addition of PARPis to therapy was beneficial [28–31]. Moreover, Gu, L., et al. included 12 clinical trials containing six types of cancer patients for meta-analysis, and then concluded that with the acceptable and controllable toxicity profile, PARPis improved survival of cancer patients, and were more beneficial to ovarian cancer patients with BRCAm [32].
In order to evaluate PARPis in-depth and in detail, this meta-analysis comprehensively focused on evaluating the efficacy of each PARPi, with respect to different intervention strategies in patients with BRCAm-positive breast and ovarian cancer, and also differences in the therapeutic effectiveness of PARPis when administered at the time of relapse versus at the time of ovarian cancer diagnosis. In a subgroup of BRCAm cancers, our pooled analysis showed that compared with the control, the PARPis treatment group showed a statistically significant reduction in disease risk progression of patients with breast (36%) or ovarian (67%) cancer. From the perspective of OS data from meta-analysis, more RCTs are needed to confirm whether PARPis effectively improve the OS of BRCA mutant patients with breast or ovarian cancer.
For ovarian cancer, despite standard therapy which includes cytoreductive surgery and conventional chemotherapy, about 70% of patients with newly diagnosed advanced ovarian cancer will face to relapse within the subsequent 3 years [33]. Promisingly, Ibrahim, E.M., et al. demonstrated that in newly diagnosed patients with advanced high-grade ovarian cancer, PARPis significantly decreased the risk of PFS by 46% when compared with placebo [34]. As first-line maintenance therapy, PARPis greatly benefit PFS of patients with newly diagnosed advanced ovarian cancer [35]. Consistent with these results, our study found that the addition of PARPis to standard therapy at the beginning of diagnosis for advanced ovarian cancer patients with BRCAm lead to an additional PFS benefit of 12.9 months, when compared at the time of relapse.
Use PARPis in patients of cancer with homologous recombination deficiency (HRD)
Importantly, by using novel biomarkers of homologous recombination repair deficiency, the benefits of PARPis were extended to wider populations of patients beyond breast or ovarian cancer, even beyond BRCA mutant cancer [36]. For other cancers, in patients with BRCAm and metastatic pancreatic or prostate cancer, olaparid group had a better PFS than control group [37, 38]. Furthermore, for patients with HRD, PARPi used in the populations of ERCC1 or BRCA deficient cancers, might potentiate their therapeutic effects by regulating the signal pathway related to antitumor immunity [39, 40]. ATM (ataxia telangiectasia mutated) promoted survival by decreasing sensitivity to PARP inhibition and playing a role upstream of homologous recombination repair in the repair of certain types of double-strand breaks [41]. PARP inhibitors had a significant killing effect on many cancers with ATM deficient [42–45]. Results from a phases 3 trial enrolled prostate cancer patients with qualifying deleterious or suspected deleterious alterations in at least 1 of 15 prespecified genes in homologous recombination repair: BRCA1, BRCA2, ATM, BRIP1, BARD1, CDK12, CHEK1, CHEK2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D, and RAD54L, indicated that olaparib improved progression-free survival when compared with enzalutamide or abiraterone [38]. However, because there is a lack of reliable clinical data to confirm PARPis are suitable for treating all types of cancer, patients should have genetic testing for defects in BRCA1/2 and other genes related to homologous recombination deficiency, before PARPis are safely applied [46].
Strengths and limitations of study
Strengths: Firstly, 1,426 breast cancer patients and 2,300 ovarian cancer patients with BRCA mutations were included in this analysis. Secondly, through reasonable stratification and grouping, the therapeutic characteristics of PARPis in patients with breast or ovarian cancer carrying BRCAm, BRCA1m and BRCA2m were analyzed. Thirdly, after considering the pooled, satisfactory results of median PFS in newly diagnosed patients with BRCA mutant ovarian cancer, we recommended PARPis as the first-line maintenance therapy for BRCAm ovarian cancer.
Limitations: We acknowledge that this evidence-based medical report has some limitations, based on heterogeneity from cancer type, PARPi type and therapeutic schedule, which may reduce the accuracy of our results. Firstly, two cancer types were included in this study, and no further detailed analysis was made in pathological types in each cancer. Secondly, diversification existed in the phase of the treatment for patients, as well as the treatment options of PARPis. Thirdly, data on the OS of several studies was not mature enough or published. Fourthly, although stratification analysis was conducted, a few trials were included in some subgroup analysis.
Conclusions
In this meta-analysis, application of therapy with PARPis provided a substantial PFS benefit among breast and ovarian cancer with BRCA mutations; and among patients with BRCAm ovarian cancer, PARPis provided longer PFS benefit at the stage of newly diagnosed than at the stage of recurrence.
Materials and Methods
We performed a meta-analysis of PARPi efficacy in BRCA mutant cancers according to the recommendations of the Cochrane Handbook and PRISMA statement guidelines [47].
Search strategy
The search strategy and selection criteria are similar to the previous study we published [29]. We conducted a comprehensive systematic search of PubMed, Embase and Cochrane from inception to September 1, 2020 for all RCTs, and then checked the trial registration number and more relevant information in the https://www.clinicaltrials.gov/ and international clinical trials registry platform. For database searches we used the “parp OR poly adp ribose polymerase OR poly adenosine diphosphate ribose polymerase OR olaparib OR veliparib OR iniparib OR rucaparib OR niraparib OR talazoparib” as the search terms in all fields.
Selection criteria
Exclusion criteria and inclusion criteria were prespecified and used in literature search and screening. To be eligible, the selected randomized controlled trials not only met the condition of researching the clinical efficacy of PARPis in patients, but also met the following conditions. Firstly, the population was patients with breast and ovarian cancers carrying BRCA mutations, irrespective of cancer stage or grade, surgery, recurrence, drug resistance, histology. Secondly, intervention: treated with PARPis (olaparib, veliparib, rucaparib, iniparib, talazoparib, niraparib) as monotherapy or combination with conventional chemotherapy or molecular target therapy regardless of dosage and duration. Thirdly, main outcome: the primary outcome was OS or PFS measured as HR. Studies were excluded if they were non-randomized control trials, phase I clinical trials, literature reviews and meta-analysis, case reports, retrospective or prospective observational cohort studies, basic science papers, commentaries, quality of life studies, and cost effectiveness analyses. In addition, we excluded those studies that did not explore PFS and OS or whose data have not yet been published. Moreover, updated and published follow-up data meeting the inclusion criteria which may have appeared in multiple articles or different publications were considered for one trial to analyze.
Data extraction and risk of bias assessment
The key purpose of this meta-analysis was to evaluate the efficacy of PARPis measured by HRs of OS or PFS. Using a pilot-tested data extraction sheet, two investigators independently reviewed the eligible literature, and extracted the data including: cancer type and clinical stage or grade, first author, year of publication, phase of clinical trial, number of patients enrolled, intervention method, hazard ratios (HR) and their 95% confidence intervals (CIs) for OS and PFS stratified by BRCA status. The risk of bias was evaluated by using the Cochrane Risk of Bias Tool that consists of random sequence generation; allocation concealment; blinding of participants and personnel to the study protocol; blinding of outcome assessment; incomplete outcome data; and selective reporting [48]. The risk of bias was divided into three different levels: high, low, or unclear. Two investigators completed the review independently and in the event of any differences, resolved them through discussion and consultation.
Statistical analysis
The primary objectives of the meta-analysis were OS and PFS in breast and ovarian cancers patients with BRCAm. Subgroup analysis was conducted to explore the efficacy of PARPis in breast or ovarian cancer by stratification BRCA1m or BRCA2m, and also to evaluate the efficacy of each PARPi and different intervention methods by integrating data from these two cancer types. Cochrane’s Q-test and I2 statistics were used to assess heterogeneity across the different studies. P ≤ 0.10 or I2 ≥ 50% indicated significant heterogeneity. The random-effect model was used to increase reliability because of the obvious heterogeneity attributed to differences by cancer type, PARPi type and therapeutic schedule in this meta-analysis [32]. Therefore, it was necessary to perform subgroup analysis to reduce heterogeneity and improve reliability. Potential publication bias was assessed by the Begg’s and Egger’s test [49, 50]. P < 0.05 was refer to indicate statistical significance. All analysis was carried out using Stata version 15.1 (StataCorp, College Station, TX, USA).
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this published article (and its supplementary information files).
Supplementary Materials
Author Contributions
Fengping Shao, Yaoyun Duan, Yunhe Zhao, Shanyang He: Conceptualization, Methodology. Fengping Shao, Yunhe Zhao and Yinguang Li: Software, Validation. Fengping Shao, Yaoyun Duan: Data curation, Writing-Original draft preparation. Fengping Shao, Jun Liu: Visualization, Investigation. Fengping Shao, Cai Zhang, Shanyang He: Supervision. Fengping Shao, Yaoyun Duan, Yunhe Zhao and Shanyang He: Writing- Reviewing and Editing.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This study and the article processing charges were supported by the National Natural Sciences Foundation of China [grant number 81772764].
References
- 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020; 70:7–30. https://doi.org/10.3322/caac.21590 [PubMed]
- 2. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66:115–32. https://doi.org/10.3322/caac.21338 [PubMed]
- 3. Lord CJ, Ashworth A. PARP inhibitors: synthetic lethality in the clinic. Science. 2017; 355:1152–58. https://doi.org/10.1126/science.aam7344 [PubMed]
- 4. Sonnenblick A, de Azambuja E, Azim HA
Jr , Piccart M. An update on PARP inhibitors—moving to the adjuvant setting. Nat Rev Clin Oncol. 2015; 12:27–41. https://doi.org/10.1038/nrclinonc.2014.163 [PubMed] - 5. Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, Santarosa M, Dillon KJ, Hickson I, Knights C, Martin NM, Jackson SP, Smith GC, Ashworth A. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005; 434:917–21. https://doi.org/10.1038/nature03445 [PubMed]
- 6. Sohal DP, Kennedy EB, Cinar P, Conroy T, Copur MS, Crane CH, Garrido-Laguna I, Lau MW, Johnson T, Krishnamurthi S, Moravek C, O’Reilly EM, Philip PA, et al. Metastatic pancreatic cancer: ASCO guideline update. J Clin Oncol. 2020; 38:3217–30. https://doi.org/10.1200/JCO.20.01364 [PubMed]
- 7. Tew WP, Lacchetti C, Ellis A, Maxian K, Banerjee S, Bookman M, Jones MB, Lee JM, Lheureux S, Liu JF, Moore KN, Muller C, Rodriguez P, et al. PARP inhibitors in the management of ovarian cancer: ASCO guideline. J Clin Oncol. 2020; 38:3468–93. https://doi.org/10.1200/JCO.20.01924 [PubMed]
- 8. Tung NM, Boughey JC, Pierce LJ, Robson ME, Bedrosian I, Dietz JR, Dragun A, Gelpi JB, Hofstatter EW, Isaacs CJ, Jatoi I, Kennedy E, Litton JK, et al. Management of Hereditary Breast Cancer: American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Guideline. J Clin Oncol. 2020; 38:2080–106. https://doi.org/10.1200/JCO.20.00299 [PubMed]
- 9. Coleman RL, Fleming GF, Brady MF, Swisher EM, Steffensen KD, Friedlander M, Okamoto A, Moore KN, Efrat Ben-Baruch N, Werner TL, Cloven NG, Oaknin A, DiSilvestro PA, et al. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. N Engl J Med. 2019; 381:2403–15. https://doi.org/10.1056/NEJMoa1909707 [PubMed]
- 10. Coleman RL, Oza AM, Lorusso D, Aghajanian C, Oaknin A, Dean A, Colombo N, Weberpals JI, Clamp A, Scambia G, Leary A, Holloway RW, Gancedo MA, et al, and ARIEL3 investigators. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017; 390:1949–61. https://doi.org/10.1016/S0140-6736(17)32440-6 [PubMed]
- 11. González-Martín A, Pothuri B, Vergote I, DePont Christensen R, Graybill W, Mirza MR, McCormick C, Lorusso D, Hoskins P, Freyer G, Baumann K, Jardon K, Redondo A, et al, and PRIMA/ENGOT-OV26/GOG-3012 Investigators. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N Engl J Med. 2019; 381:2391–402. https://doi.org/10.1056/NEJMoa1910962 [PubMed]
- 12. Kaye SB, Lubinski J, Matulonis U, Ang JE, Gourley C, Karlan BY, Amnon A, Bell-McGuinn KM, Chen LM, Friedlander M, Safra T, Vergote I, Wickens M, et al. Phase II, open-label, randomized, multicenter study comparing the efficacy and safety of olaparib, a poly (ADP-ribose) polymerase inhibitor, and pegylated liposomal doxorubicin in patients with BRCA1 or BRCA2 mutations and recurrent ovarian cancer. J Clin Oncol. 2012; 30:372–79. https://doi.org/10.1200/JCO.2011.36.9215 [PubMed]
- 13. Ledermann J, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, Scott C, Meier W, Shapira-Frommer R, Safra T, Matei D, Macpherson E, Watkins C, et al. Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer. N Engl J Med. 2012; 366:1382–92. https://doi.org/10.1056/NEJMoa1105535 [PubMed]
- 14. Ledermann J, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, Scott CL, Meier W, Shapira-Frommer R, Safra T, Matei D, Fielding A, Spencer S, et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: a preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014; 15:852–61. https://doi.org/10.1016/S1470-2045(14)70228-1 [PubMed]
- 15. Ledermann JA, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, Scott C, Meier W, Shapira-Frommer R, Safra T, Matei D, Fielding A, Spencer S, et al. Overall survival in patients with platinum-sensitive recurrent serous ovarian cancer receiving olaparib maintenance monotherapy: an updated analysis from a randomised, placebo-controlled, double-blind, phase 2 trial. Lancet Oncol. 2016; 17:1579–89. https://doi.org/10.1016/S1470-2045(16)30376-X [PubMed]
- 16. Mirza MR, Monk BJ, Herrstedt J, Oza AM, Mahner S, Redondo A, Fabbro M, Ledermann JA, Lorusso D, Vergote I, Ben-Baruch NE, Marth C, Mądry R, et al, and ENGOT-OV16/NOVA Investigators. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N Engl J Med. 2016; 375:2154–64. https://doi.org/10.1056/NEJMoa1611310 [PubMed]
- 17. Moore K, Colombo N, Scambia G, Kim BG, Oaknin A, Friedlander M, Lisyanskaya A, Floquet A, Leary A, Sonke GS, Gourley C, Banerjee S, Oza A, et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N Engl J Med. 2018; 379:2495–505. https://doi.org/10.1056/NEJMoa1810858 [PubMed]
- 18. Oza AM, Cibula D, Benzaquen AO, Poole C, Mathijssen RH, Sonke GS, Colombo N, Špaček J, Vuylsteke P, Hirte H, Mahner S, Plante M, Schmalfeldt B, et al. Olaparib combined with chemotherapy for recurrent platinum-sensitive ovarian cancer: a randomised phase 2 trial. Lancet Oncol. 2015; 16:87–97. https://doi.org/10.1016/S1470-2045(14)71135-0 [PubMed]
- 19. Penson RT, Valencia RV, Cibula D, Colombo N, Leath CA 3rd, Bidziński M, Kim JW, Nam JH, Madry R, Hernández C, Mora PA, Ryu SY, Milenkova T, et al. Olaparib versus nonplatinum chemotherapy in patients with platinum-sensitive relapsed ovarian cancer and a germline BRCA1/2 mutation (SOLO3): a randomized phase III trial. J Clin Oncol. 2020; 38:1164–74. https://doi.org/10.1200/JCO.19.02745 [PubMed]
- 20. Pujade-Lauraine E, Ledermann JA, Selle F, Gebski V, Penson RT, Oza AM, Korach J, Huzarski T, Poveda A, Pignata S, Friedlander M, Colombo N, Harter P, et al, and SOLO2/ENGOT-Ov21 investigators. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017; 18:1274–84. https://doi.org/10.1016/S1470-2045(17)30469-2 [PubMed]
- 21. Ray-Coquard I, Pautier P, Pignata S, Pérol D, González-Martín A, Berger R, Fujiwara K, Vergote I, Colombo N, Mäenpää J, Selle F, Sehouli J, Lorusso D, et al, and PAOLA-1 Investigators. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. N Engl J Med. 2019; 381:2416–28. https://doi.org/10.1056/NEJMoa1911361 [PubMed]
- 22. Diéras V, Han HS, Kaufman B, Wildiers H, Friedlander M, Ayoub JP, Puhalla SL, Bondarenko I, Campone M, Jakobsen EH, Jalving M, Oprean C, Palácová M, et al. Veliparib with carboplatin and paclitaxel in BRCA-mutated advanced breast cancer (BROCADE3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2020; 21:1269–82. https://doi.org/10.1016/S1470-2045(20)30447-2 [PubMed]
- 23. Han HS, Diéras V, Robson M, Palácová M, Marcom PK, Jager A, Bondarenko I, Citrin D, Campone M, Telli ML, Domchek SM, Friedlander M, Kaufman B, et al. Veliparib with temozolomide or carboplatin/paclitaxel versus placebo with carboplatin/paclitaxel in patients with BRCA1/2 locally recurrent/metastatic breast cancer: randomized phase II study. Ann Oncol. 2018; 29:154–61. https://doi.org/10.1093/annonc/mdx505 [PubMed]
- 24. Litton JK, Hurvitz SA, Mina LA, Rugo HS, Lee KH, Gonçalves A, Diab S, Woodward N, Goodwin A, Yerushalmi R, Roché H, Im YH, Eiermann W, et al. Talazoparib versus chemotherapy in patients with germline BRCA1/2-mutated HER2-negative advanced breast cancer: final overall survival results from the EMBRACA trial. Ann Oncol. 2020; 31:1526–35. https://doi.org/10.1016/j.annonc.2020.08.2098 [PubMed]
- 25. Litton JK, Rugo HS, Ettl J, Hurvitz SA, Gonçalves A, Lee KH, Fehrenbacher L, Yerushalmi R, Mina LA, Martin M, Roché H, Im YH, Quek RG, et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med. 2018; 379:753–63. https://doi.org/10.1056/NEJMoa1802905 [PubMed]
- 26. Robson M, Im SA, Senkus E, Xu B, Domchek SM, Masuda N, Delaloge S, Li W, Tung N, Armstrong A, Wu W, Goessl C, Runswick S, Conte P. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N Engl J Med. 2017; 377:523–33. https://doi.org/10.1056/NEJMoa1706450 [PubMed]
- 27. Robson ME, Tung N, Conte P, Im SA, Senkus E, Xu B, Masuda N, Delaloge S, Li W, Armstrong A, Wu W, Goessl C, Runswick S, Domchek SM. OlympiAD final overall survival and tolerability results: Olaparib versus chemotherapy treatment of physician’s choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann Oncol. 2019; 30:558–66. https://doi.org/10.1093/annonc/mdz012 [PubMed]
- 28. Poggio F, Bruzzone M, Ceppi M, Conte B, Martel S, Maurer C, Tagliamento M, Viglietti G, Del Mastro L, de Azambuja E, Lambertini M. Single-agent PARP inhibitors for the treatment of patients with BRCA-mutated HER2-negative metastatic breast cancer: a systematic review and meta-analysis. ESMO Open. 2018; 3:e000361. https://doi.org/10.1136/esmoopen-2018-000361 [PubMed]
- 29. Shao F, Liu J, Duan Y, Li L, Liu L, Zhang C, He S. Efficacy and safety of PARP inhibitors as the maintenance therapy in ovarian cancer: a meta-analysis of nine randomized controlled trials. Biosci Rep. 2020; 40:BSR20192226. https://doi.org/10.1042/BSR20192226 [PubMed]
- 30. Staropoli N, Ciliberto D, Del Giudice T, Iuliano E, Cucè M, Grillone F, Salvino A, Barbieri V, Russo A, Tassone P, Tagliaferri P. The era of PARP inhibitors in ovarian cancer: ”class action“ or not? a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2018; 131:83–89. https://doi.org/10.1016/j.critrevonc.2018.08.011 [PubMed]
- 31. Al Hadidi S, Aburahma A, Badami S, Upadhaya S. PARP (Poly(ADP-Ribose) Polymerase) Inhibitors in Platinum-Sensitive Recurrent Ovarian Cancer: A Meta-Analysis of Randomized Controlled Trials. Oncol Res Treat. 2018; 41:226–35. https://doi.org/10.1159/000486418 [PubMed]
- 32. Gu L, Du N, Jin Q, Li S, Xie L, Mo J, Shen Z, Mao D, Ji J, Khadaroo PA, Chen B. Magnitude of benefit of the addition of poly ADP-ribose polymerase (PARP) inhibitors to therapy for Malignant tumor: a meta-analysis. Crit Rev Oncol Hematol. 2020; 147:102888. https://doi.org/10.1016/j.critrevonc.2020.102888 [PubMed]
- 33. Ledermann JA, Raja FA, Fotopoulou C, Gonzalez-Martin A, Colombo N, Sessa C, and ESMO Guidelines Working Group. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013 (Suppl 24); 6:vi24–32. https://doi.org/10.1093/annonc/mdt333 [PubMed]
- 34. Ibrahim EM, Refae AA, Bayer AM, Sagr ER. Poly(ADP-ribose) polymerase inhibitors as maintenance treatment in patients with newly diagnosed advanced ovarian cancer: a meta-analysis. Future Oncol. 2020; 16:585–96. https://doi.org/10.2217/fon-2020-0057 [PubMed]
- 35. Lin Q, Liu W, Xu S, Shang H, Li J, Guo Y, Tong J. PARP inhibitors as maintenance therapy in newly diagnosed advanced ovarian cancer: a meta-analysis. BJOG. 2021; 128:485–93. https://doi.org/10.1111/1471-0528.16411 [PubMed]
- 36. Pilié PG, Gay CM, Byers LA, O’Connor MJ, Yap TA. PARP inhibitors: extending benefit beyond BRCA-mutant cancers. Clin Cancer Res. 2019; 25:3759–71. https://doi.org/10.1158/1078-0432.CCR-18-0968 [PubMed]
- 37. Golan T, Hammel P, Reni M, Van Cutsem E, Macarulla T, Hall MJ, Park JO, Hochhauser D, Arnold D, Oh DY, Reinacher-Schick A, Tortora G, Algül H, et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N Engl J Med. 2019; 381:317–27. https://doi.org/10.1056/NEJMoa1903387 [PubMed]
- 38. de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, Chi KN, Sartor O, Agarwal N, Olmos D, Thiery-Vuillemin A, Twardowski P, Mehra N, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2020; 382:2091–102. https://doi.org/10.1056/NEJMoa1911440 [PubMed]
- 39. Chabanon RM, Soria JC, Lord CJ, Postel-Vinay S. Beyond DNA repair: the novel immunological potential of PARP inhibitors. Mol Cell Oncol. 2019; 6:1585170. https://doi.org/10.1080/23723556.2019.1585170 [PubMed]
- 40. Chabanon RM, Muirhead G, Krastev DB, Adam J, Morel D, Garrido M, Lamb A, Hénon C, Dorvault N, Rouanne M, Marlow R, Bajrami I, Cardeñosa ML, et al. PARP inhibition enhances tumor cell-intrinsic immunity in ERCC1-deficient non-small cell lung cancer. J Clin Invest. 2019; 129:1211–28. https://doi.org/10.1172/JCI123319 [PubMed]
- 41. Bryant HE, Helleday T. Inhibition of poly (ADP-ribose) polymerase activates ATM which is required for subsequent homologous recombination repair. Nucleic Acids Res. 2006; 34:1685–91. https://doi.org/10.1093/nar/gkl108 [PubMed]
- 42. Weston VJ, Oldreive CE, Skowronska A, Oscier DG, Pratt G, Dyer MJ, Smith G, Powell JE, Rudzki Z, Kearns P, Moss PA, Taylor AM, Stankovic T. The PARP inhibitor olaparib induces significant killing of ATM-deficient lymphoid tumor cells in vitro and in vivo. Blood. 2010; 116:4578–87. https://doi.org/10.1182/blood-2010-01-265769 [PubMed]
- 43. Schmitt A, Knittel G, Welcker D, Yang TP, George J, Nowak M, Leeser U, Büttner R, Perner S, Peifer M, Reinhardt HC. ATM deficiency is associated with sensitivity to PARP1- and ATR inhibitors in lung adenocarcinoma. Cancer Res. 2017; 77:3040–56. https://doi.org/10.1158/0008-5472.CAN-16-3398 [PubMed]
- 44. Bang YJ, Xu RH, Chin K, Lee KW, Park SH, Rha SY, Shen L, Qin S, Xu N, Im SA, Locker G, Rowe P, Shi X, et al. Olaparib in combination with paclitaxel in patients with advanced gastric cancer who have progressed following first-line therapy (GOLD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017; 18:1637–51. https://doi.org/10.1016/S1470-2045(17)30682-4 [PubMed]
- 45. Bang YJ, Im SA, Lee KW, Cho JY, Song EK, Lee KH, Kim YH, Park JO, Chun HG, Zang DY, Fielding A, Rowbottom J, Hodgson D, et al. Randomized, double-blind phase II trial with prospective classification by ATM protein level to evaluate the efficacy and tolerability of olaparib plus paclitaxel in patients with recurrent or metastatic gastric cancer. J Clin Oncol. 2015; 33:3858–65. https://doi.org/10.1200/JCO.2014.60.0320 [PubMed]
- 46. Konstantinopoulos PA, Norquist B, Lacchetti C, Armstrong D, Grisham RN, Goodfellow PJ, Kohn EC, Levine DA, Liu JF, Lu KH, Sparacio D, Annunziata CM. Germline and somatic tumor testing in epithelial ovarian cancer: ASCO guideline. J Clin Oncol. 2020; 38:1222–45. https://doi.org/10.1200/JCO.19.02960 [PubMed]
- 47. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009; 6:e1000100. https://doi.org/10.1371/journal.pmed.1000100 [PubMed]
- 48. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, and Cochrane Bias Methods Group, and Cochrane Statistical Methods Group. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011; 343:d5928. https://doi.org/10.1136/bmj.d5928 [PubMed]
- 49. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34. https://doi.org/10.1136/bmj.315.7109.629 [PubMed]
- 50. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994; 50:1088–101. https://doi.org/10.2307/2533446 [PubMed]