



Introduction
Apolipoprotein B (Apo B) is the major protein constituent of low-density lipoprotein cholesterol (LDL-C). Increased serum level of LDL-C is recognized to be an independent risk factor for atherosclerotic-related events [1], such as carotid arteriosclerosis stenosis (CAS) ≥ 50% and ischemic stroke (IS). According to the amount of cholesterol ester in the core of LDL-C particle, LDL-C particles are different in sizes and densities such as small, intermediate and large dense LDLs, containing one molecule of Apo B per LDL-C particle regardless of its size. Although in most cases, the independent risk factor for atherosclerotic-related events is not smaller LDL particles, subjects with more of this type of LDL particles will be at higher risk for future cardiovascular events. However, epidemiological studies still fail to distinguish the relative atherogenicity caused by different sizes of LDL particles. This suggests that it is not the composition (sizes and densities) of LDL-C particles, but its quantity (Apo B content) that is the key factor of atherosclerosis. Smaller LDL particles are more likely to enter the arterial wall, and are more susceptible to oxidation, which is essentially as a result of the conformation-changing of Apo B with decreasing LDL particles size. For most individuals, the serum level of Apo B is largely concordant with that of LDL-C, and adds minor effect to LDL-C based risk assessment. However, in a subgroup with inconsistence between the serum levels of Apo B and LDL-C, there is a redundant risk is related to an excess risk of atherosclerotic cardiovascular disease (ASCVD) [2]. On the other hand, statins can control LDL-C levels, but a residual risk of ASCVD still remains, related to high Apo B levels, especially in people with obesity, metabolic syndrome or (and) diabetes [3]. In statin-treated patients, Apo B levels rather than LDL-C levels indeed better predict subsequent ASCVD events. Hence, Apo B levels are more closely associated with ASCVD than LDL-C levels, are the principal drivers of this process, and may be demonstrably a better biomarker for assessing potential ASCVD risk. Statin therapy is linked to decreases risk of ASCVD events, but the profits could be declined by inherent genetic risk. Thus, it is a promising public approach for early ASCVD prevention based on earlier genetic assessment of subjects at increased risk of higher Apo B serum concentrations.
The ATP-sensitive potassium channels (KATP) plays as essential well-fidelity metabolic sensors, and also as an important end effector of ischemic preservation, indicating that KATP couples metabolic abnormalities to protection against ischemic-related injury. This also emphasizes KATP as novel targets for prevention and treatment of ASCVD. The structure of KATP is large heteromultimeric protein complex, consisted of four inwardly-rectifying potassium channel subunits (pore-forming subunits, Kir6.x) and four sulfonylurea receptor subunits (regulatory subunits, SURx). The Kir6.x pore-forming subunits are encoding respectively by KCNJ8 (Kir6.1) and KCNJ11 (Kir6.2) (chromosomal mapping to 12p12.1) while SURx regulatory subunits are respectively by ABCC8 (SUR1) and ABCC9 (SUR2) (chromosomal mapping to 11p15.1). The subunit constitution of KATP possibly remodel with different physiological and pathological circumstances, involving in substitute splicing of these coding genes as mentioned above, which can result in different subunits being functional in different status. The KATP has extremely high genetic diversity. KATP mutations were not only correlated with serum lipid disorder [e.g., triglyceride (TIRG), total cholesterol (TC), LDL-C or (and) high-density lipoprotein cholesterol (HDL-C)] [4–6] and ASCVD [7, 8] but also exhibited ethnic and geographical heterogeneity (e.g., Europeans, Africans or East Asians). Nevertheless, the associations of KATP mutations with Apo B serum level and its related ASCVD in China are still unclear. Theoretically, the relationship shows the characteristics of ethnic-specific genetic pleiotropy [9] but there may be a mutual genetic basis between lipid disorder and ASCVD [10].
The occurrence and development of elevated Apo B serum concentration and its related ASCVD arises from complex interaction between genetic and environment factors. The exosome-derived microRNAs (exo-miRs) are one of the main classes of non-coding RNAs, and play a critical role as bridge that links genetic and environment factors. Exosomes are important extracellular vesicles with lipid bilayer membrane, and carry cell-specific medium for mediating intercellular communication, especially microRNAs (miRs). The miRs are a class of small (about 22-25 nucleotides long) and endogenous single-stranded RNAs, with an established function of regulating genes at transcriptional and post-transcriptional steps. The exo-miRs take part in almost every physiological or pathological processes ranging from elevated Apo B level to ASCVD. However, the circulating expression profile of exo-miRs and its effect in the process from genotype (KATP variants) to phenotype (elevated Apo B serum levels) remain elusive. In present study we investigate possible associations of KATP variants with the risks of increased Apo B serum levels (≥ 80 mg/dL) and ASCVD (e.g., CAS ≥ 50% and new-onset IS) in South China, and identify the plasma expression profile of exo-miRs among subjects under specific genotype (KATP variants)-phenotype (Apo B ≥ 80 mg/dL) correlations.
Results
Clinical baseline characteristics of participants
Participants with or without higher Apo B serum concentration (≥ 80 mg/dL) showed significant differences on serum concentration of TRIG, TC and LDL-C (all P<0.001), as shown in Table 1. After a median follow-up of 50.6-months, there was no significant difference on NYHA functional classification between the two groups as well as combined medication, including antiplatelet drugs, beta-receptor blockers (BBs), calcium channel blockers (CCBs), digoxin, diuretics, hypoglycemic agents, mineralocorticoid receptor antagonists (MRAs), nitrates, renin-angiotensin system inhibitors (RSIs), statins, and warfarin (all P>0.05), as shown in Table 2.
Table 1. Baseline characteristics of study subjects.
| Apo B ≥ 80 mg/dL (N/%) | P value | ||
| NO | YES | ||
| N | 522 | 522 | - |
| Male: Female | 406:116 | 395:127 | 0.420 |
| Age (Y) | 64.9±11.5 | 63.8±10.4 | 0.121 |
| Smoking (%) | 264(50.6) | 282(54.0) | 0.265 |
| Drinking (%) | 68(13.0) | 82(15.7) | 0.217 |
| SBP (mmHg) | 137.9±22.1 | 138.9±23.5 | 0.452 |
| DBP (mmHg) | 77.6±14.1 | 78.5±12.1 | 0.266 |
| BMI (kg/m2) | 24.6±4.5 | 24.7±3.7 | 0.813 |
| Medical condition | |||
| EH (%) | 332(63.6) | 324(62.1) | 0.608 |
| CHD (%) | 426(81.6) | 406(77.8) | 0.124 |
| T2D (%) | 268(51.3) | 257(49.2) | 0.496 |
| AF (%) | 16(3.1) | 22(4.2) | 0.321 |
| Blood biochemical index | |||
| TRIG (mmol/L) | 1.39±0.91 | 1.69±0.86 | <0.001 |
| TC (mmol/L) | 3.54±0.85 | 5.02±1.09 | <0.001 |
| HDL-C (mmol/L) | 1.10±0.29 | 1.09±0.27 | 0.848 |
| LDL-C (mmol/L) | 1.82±0.55 | 2.86±0.78 | <0.001 |
| ApoA1 (mg/dL) | 103.0±24.2 | 103.4±18.9 | 0.758 |
| WBC (×109/L) | 8.47±2.79 | 8.44±2.98 | 0.852 |
| HGB (g/L) | 132.4±18.5 | 131.6±17.6 | 0.467 |
| PLT (×109/L) | 233.1±52.5 | 234.2±66.2 | 0.780 |
| FBG (mmol/L) | 5.54±1.40 | 5.66±1.32 | 0.182 |
| P2hBS (mmol/L) | 8.73±2.71 | 9.07±2.98 | 0.053 |
| HbA1C (%) | 5.9±1.1 | 6.0±1.3 | 0.183 |
| Scr (μmol/L) | 93.0±44.3 | 90.1±33.0 | 0.911 |
| BUN (mmol/L) | 5.76±2.17 | 5.74±1.952 | 0.247 |
| UA (μmol/L) | 406.0±113.6 | 415.9±108.6 | 0.150 |
| ALT (U/L) | 27.9±31.5 | 30.3±27.3 | 0.180 |
| AST (U/L) | 47.6±74.9 | 49.2±58.8 | 0.698 |
| Alb (g/L) | 37.2±3.9 | 37.4±4.0 | 0.632 |
| Na+ (mmol/L) | 140.5±3.1 | 140.3±3.2 | 0.324 |
| K+ (mmol/L) | 3.74±0.41 | 3.73±0.39 | 0.452 |
| HsCRP (mg/L) | 11.6±18.7 | 13.9±22.6 | 0.076 |
| ACE (U/L) | 32.8±19.7 | 35.1±22.6 | 0.076 |
| Renin (pg/mL) | 24.7±27.8 | 26.3±29.6 | 0.390 |
| Ang I (ng/L) | 2.23±1.69 | 2.08±1.55 | 0.146 |
| Ang II (ng/L) | 63.5±89.2 | 71.9±101.7 | 0.157 |
| ALD (ng/L) | 181.0±121.4 | 178.8±117.4 | 0.771 |
| Echocardiography | |||
| RVD (cm) | 1.74±0.18 | 1.75±0.19 | 0.230 |
| RAD (cm) | 3.36±0.35 | 3.34±0.28 | 0.494 |
| LVD (cm) | 4.83±0.53 | 4.78±0.59 | 0.145 |
| LAD (cm) | 3.08±0.59 | 3.14±0.53 | 0.114 |
| LVEF (%) | 56.8±9.7 | 56.5±9.1 | 0.675 |
Table 2. Partial baseline characteristics of study participants at the end of the follow-up.
| Apo B ≥ 80 mg/dL (N/%) | P value | ||
| NO | YES | ||
| Sample(N) | 522 | 522 | - |
| NYHA | |||
| I | 140(43.8) | 162(50.6) | 0.053 |
| II | 157(49.1) | 134(41.9) | |
| III | 21(6.5) | 16(5.0) | |
| IV | 2(0.6) | 8(2.5) | |
| Combined medication | |||
| (A) Antiplatelet drugs | 298(93.1) | 300(93.8) | 0.750 |
| (B) Warfarin | 10(3.1) | 17(3.3) | 0.169 |
| (C) Statins | 296(92.5) | 297(92.8) | 0.880 |
| (D) RSIs | 205(66.1) | 221(69.1) | 0.431 |
| (E) BBs | 222(69.4) | 210(65.6) | 0.311 |
| (F) MRAs | 67(20.9) | 74(23.1) | 0.504 |
| (G) CCBs | 76(23.8) | 91(28.4) | 0.177 |
| (H) Diuretics | 80(25.0) | 88(27.5) | 0.472 |
| (J) Digoxin | 30(9.4) | 30(9.4) | 1.000 |
| (K) Nitrates | 49(15.3) | 41(14.1) | 0.655 |
| (L) Hypoglycemic agents | 152(47.5) | 179(53.1) | 0.155 |
Association between KATP SNPs and increased Apo B serum concentration (≥ 80 mg/dL)
Only KATP rs11046182 was correlated with higher risk of elevated serum Apo B concentration (≥ 80 mg/dL) (GG genotype, adjusted OR=2.17, 95% CI: 1.55-3.05, P<0.001), as shown in Table 3.
Table 3. Association of KATP SNPs with elevated Apo B levels (≥ 80 mg/dL) in study subjects.
| KATP SNPs | Apo B ≥ 80 mg/dL (N/%) | χ2 | P value | Cude OR (95% CI) | Cude P value | Adjusted OR (95% CI)* | Adjusted P value* | Adjusted OR (95% CI)# | Adjusted P value# | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NO | YES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs11046182 | G | 298(57.1) | 345(66.1) | 8.944 | 0.003 | 1.47(1.14-1.88) | 0.003 | 1.52(1.17-1.98) | 0.002 | 2.17(1.55-3.05) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA+GA | 224(42.9) | 177(33.9) | 1.00 | 1.00 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs78148713 | CC+CT | 30(5.7) | 14(2.7) | 6.074 | 0.014 | 0.45(0.24-0.86) | 0.016 | 0.46(0.24-0.90) | 0.022 | 0.90(0.39-2.10) | 0.811 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T | 492(94.3) | 508(97.3) | 1.00 | 1.00 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs145456027 | CC+CT | 14(2.7) | 10(1.9) | 0.682 | 0.409 | 1.00 | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T | 508(97.3) | 512(98.1) | 1.41(0.62-3.21) | 0.411 | 1.82(0.79-4.23) | 0.162 | 1.37(0.44-4.29) | 0.585 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs147265929 | GG+GT | 32(6.1) | 46(8.8) | 2.716 | 0.099 | 1.00 | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T | 490(93.9) | 476(91.2) | 0.68(0.42-1.08) | 0.101 | 0.64(0.40-1.05) | 0.078 | 0.60(0.32-1.13) | 0.114 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Model 1: After adjustment for gender, age, smoking, drinking, WBC, BMI, EH, T2D, liver function (ALT, AST and Alb), renal function (Scr, BUN and UA), HsCRP, HbA1C, HCY, and RAAS activity (ACE, renin, Ang I, Ang II and ALD). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| #Model 2: It is the same as Model 1, and including dyslipidemia (TRIG, TC, LDL-C, HDL-C and Apo AI). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Association between KATP SNPs and CAS ≥ 50%
KATP rs11046182 was also correlated with elevated CAS ≥ 50% risk (GG genotype, adjusted OR=2.63, 95% CI: 1.25-5.54, P=0.011) while rs78148713 and rs147265929 were not (P=0.917 and 0.360, respectively), as shown in Table 4. In addition, the OR value of increased CAS ≥ 50% risk for KATP rs145456027 will not be estimated due to possible bias.
Table 4. Association of KATP SNPs with CAS ≥ 50% in study participants.
| KATP SNPs | CAS ≥ 50% (N/%) | χ2 | P value | Cude OR (95% CI) | Cude P-value | Adjusted OR (95% CI)* | Adjusted P value* | Adjusted OR (95% CI)# | Adjusted P value# | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NO | YES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs11046182 | G | 605(60.9) | 38(76.0) | 4.610 | 0.032 | 2.04(1.05-3.95) | 0.035 | 2.78(1.34-5.77) | 0.006 | 2.63(1.25-5.54) | 0.011 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA+GA | 389(39.1) | 12(24.0) | 1.00 | 1.00 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs78148713 | CC+CT | 42(4.2) | 2(4.0) | 0.006 | 0.938 | 0.94(0.22-4.02) | 0.938 | 0.88(0.19-4.13) | 0.868 | 0.92(0.19-4.37) | 0.917 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T | 952(95.8) | 48(96.0) | 1.00 | 1.00 | 1.00 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs145456027 | CC+CT | 24(2.4) | 0(0.0) | 1.236 | 0.266 | - | - | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T | 970(97.6) | 50(100.0) | - | - | - | - | - | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs147265929 | GG+GT | 74(7.4) | 4(8.0) | 0.021 | 0.884 | 1.00 | 1.00 | 1.00 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T | 920(92.6) | 46(92.0) | 0.93(0.32-2.64) | 0.884 | 0.58(0.19-1.79) | 0.341 | 0.59(0.19-1.84) | 0.360 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Model 1: After adjustment for gender, age, smoking, drinking, WBC, BMI, EH, T2D, liver function (ALT, AST and Alb), renal function (Scr, BUN and UA), HsCRP, HbA1C, HCY, and RAAS activity (ACE, renin, Ang I, Ang II and ALD). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| #Model 3: It is the same as Model 1, and including dyslipidemia (TRIG, TC, LDL-C, Apo B, HDL-C and Apo AI). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Association between KATP rs11046182 and new-onset IS
Subjects carrying GG genotype of KATP rs11046182 were correlated with elevated new-onset IS risk (adjusted HR=2.24, 95% CI: 1.11-4.50, P=0.024) via a median follow-up of 50.6 months, as shown in Figure 1.
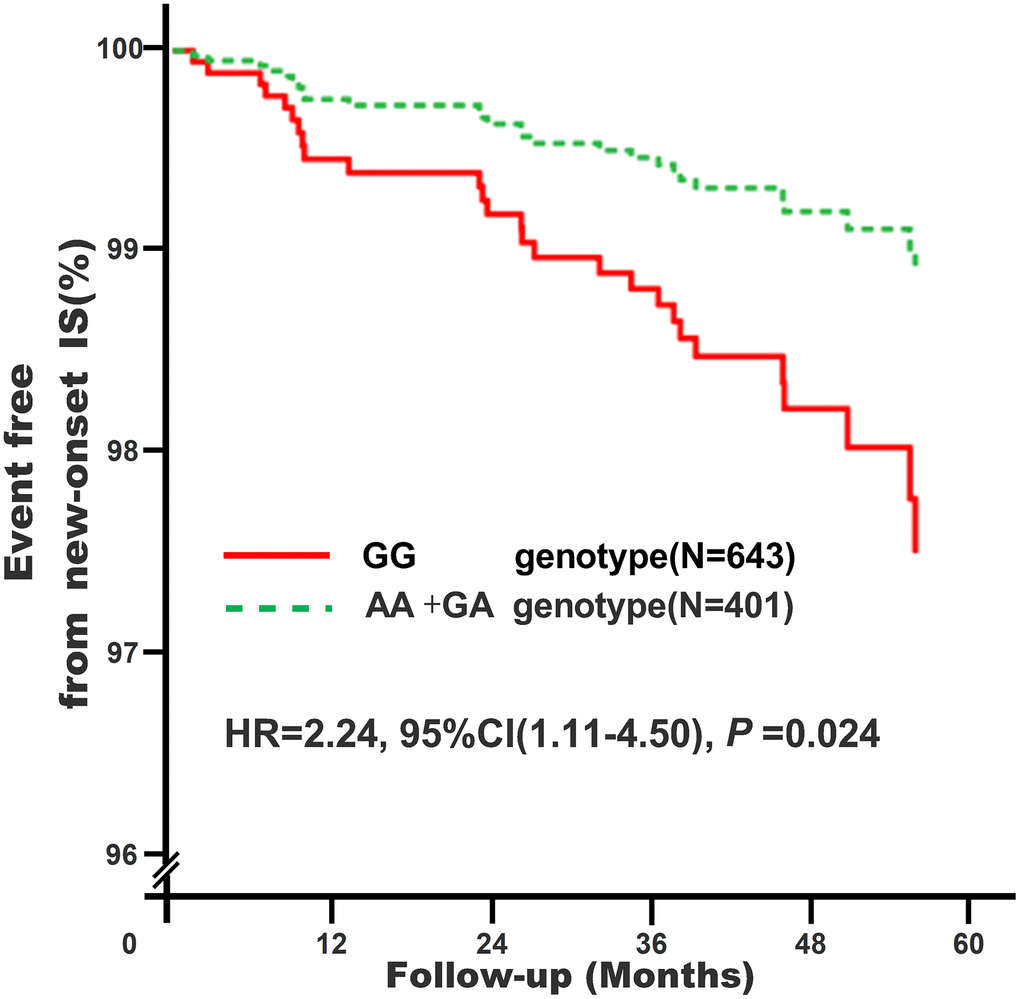
Figure 1. Association of KATP rs11046182 with new-onset IS in study subjects*. *Model 4: After adjustment for gender, age, smoking, drinking, WBC, BMI, liver function (ALT, AST and Alb), renal function (Scr, BUN and UA), HsCRP, HbA1C, HCY, and RAAS activity (ACE, renin, Ang I, Ang II and ALD), dyslipidemia (TRIG, TC, LDL-C, Apo B, HDL-C and Apo AI), medical condition (EH, CAD, T2D and AF), NYHA functional classification, combined medication (antiplatelet drugs, warfarin, statins, RSIs, BBs, MRAs, CCBs, diuretics, digoxin, nitrates, and hypoglycemic agents) and echocardiography index (RVD, RAD, LVD, LAD, and LVEF).
Clinical characteristics of participants with increased Apo B serum concentration (≥ 80 mg/dL) in plasma exo-miRs expression profiling analyses
As shown in Table 5, no significant differences showed in clinical characteristics (all P>0.05) between the two genotypes (AA+GA vs. GG) of KATP rs11046182 among subjects with increased Apo B serum concentration (≥ 80 mg/dL).
Table 5. Clinical characteristics between different genotypes of KATP rs11046182 in subjects with elevated Apo B serum levels (≥ 80 mg/dL) in plasma exo-miRs expression profiling and bioinformatics analysis.
| Genotypes of KATP rs11046182 | P value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA+GA | GG | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | 5 | 5 | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male: Female | 3:2 | 3:2 | 1.000 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (Y) | 47.8±7.5 | 48.4±8.8 | 0.910 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP (mmHg) | 123.4±4.8 | 125.6±7.9 | 0.610 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DBP (mmHg) | 74.4±6.9 | 76.8±8.8 | 0.643 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 23.5±3.7 | 23.9±3.2 | 0.859 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TRIG (mmol/L) | 1.21±0.22 | 1.22±0.19 | 0.973 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC (mmol/L) | 3.91±1.24 | 4.01±0.84 | 0.876 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C (mmol/L) | 2.38±0.46 | 2.46±0.58 | 0.803 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C(mmol/L) | 1.46±0.25 | 1.45±0.39 | 0.955 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Apo B (mg/dL) | 105.0±22.0 | 119.6±19.1 | 0.294 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Apo A1 (mg/dL) | 152.6±32.4 | 152.0±28.5 | 0.976 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WBC (×109/L) | 7.42±2.76 | 6.59±4.27 | 0.727 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HGB (g/L) | 130.0±19.0 | 133.6±10.9 | 0.723 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PLT (×109/L) | 199.4±49.9 | 241.4±45.3 | 0.201 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBG (mmol/L) | 4.84±0.52 | 4.93±0.72 | 0.827 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P2hBS (mmol/L) | 6.63±0.90 | 6.59±0.97 | 0.948 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1C (%) | 5.3±0.6 | 5.5±0.3 | 0.406 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Scr (μmol/L) | 84.0±26.0 | 77.2±26.0 | 0.690 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BUN (mmol/L) | 4.88±0.88 | 5.20±0.69 | 0.540 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA (μmol/L) | 406.0±40.6 | 385.2±81.4 | 0.623 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALT (U/L) | 21.5±14.1 | 19.4±5.8 | 0.763 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AST (U/L) | 21.4±9.1 | 21.2±2.4 | 0.963 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alb (g/L) | 37.0±2.6 | 40.6±3.8 | 0.123 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Na+ (mmol/L) | 142.4±2.7 | 141.7±4.2 | 0.788 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| K+ (mmol/L) | 4.17±0.41 | 4.23±0.42 | 0.836 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HsCRP (mg/L) | 9.8±4.0 | 11.5±6.7 | 0.642 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MAU (ACR*, mg/g) | 123.2±49.1 | 148.6±51.7 | 0.449 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HCY (μmol/L) | 11.4±2.2 | 10.4±2.9 | 0.531 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ACE (U/L) | 33.4±24.3 | 36.9±14.7 | 0.791 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Renin (pg/mL) | 22.9±25.7 | 29.7±36.6 | 0.742 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ang I (ng/L) | 2.06±1.41 | 2.64±2.28 | 0.645 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ang II (ng/L) | 151.9±114.1 | 166.1±203.4 | 0.896 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALD (ng/L) | 222.9±60.2 | 331.4±107.4 | 0.084 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *ACR: urinary albumin-to-creatinine ratio. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
DE exo-miRs under cross-talk status between KATP rs11046182 and elevated Apo B serum concentration (≥ 80 mg/dL)
A total of 615 exo-miRs were detected by implementing strict data quality control. Using reads per million (RPM) values < 10, and P < 0.05 as threshold cutoff to exclude the low expression of exo-miRs, 41 exo-miRs were then found to be obviously DE between the two genotypes (AA+GA vs. GG) of rs11046182, as shown in Supplementary Figure 1, Figure 2 and Table 6. Twenty eight exo-miRs were up-regulated in participants with GG genotype of rs11046182 compared to those with A-allele (AA+GA) while 13 exo-miRs were down-regulated, as shown in Table 6. In particular, miR-22-3p had the highest expression level among the 41 DE exo-miRs. The highest up-regulated and down-regulated miRs were miR-320d (5.34-fold changes) and miR-493-5p (5.04-fold changes), respectively. The miR-208a-3p, miR-208b-3p and miR-499a-5p belong to the miR-208 family based on highly homologous sequence. Besides miR-208 family, there were also anther three exo-miRs families as follows: miR-193 (e.g., 193a-5p and 193b-5p), miR-320 (e.g., 320c~320e), and miR-378 (e.g., 378a-3p, 378b~378h). In addition, only 6 of the 41 DE exo-miRs were found to be obviously DE between the two genotypes (AA+GA vs. GG) of rs11046182 in participants with decreased serum Apo B levels (< 80 mg/dL). 2 exo-miRs (miR-31-5p and miR-497-5p) were up-regulated and 4 exo-miRs (miR-320c/d, miR-4429 and miR-134-5p) were down-regulated in subjects carrying GG genotype of rs11046182 compared to those with AA+GA genotype, as shown in Supplementary Figure 2 and Supplementary Table 9. It exhibited opposite expression patterns in subjects with or without increased Apo B serum levels (≥ 80 mg/dL) under the genetic background of KATP rs11046182.
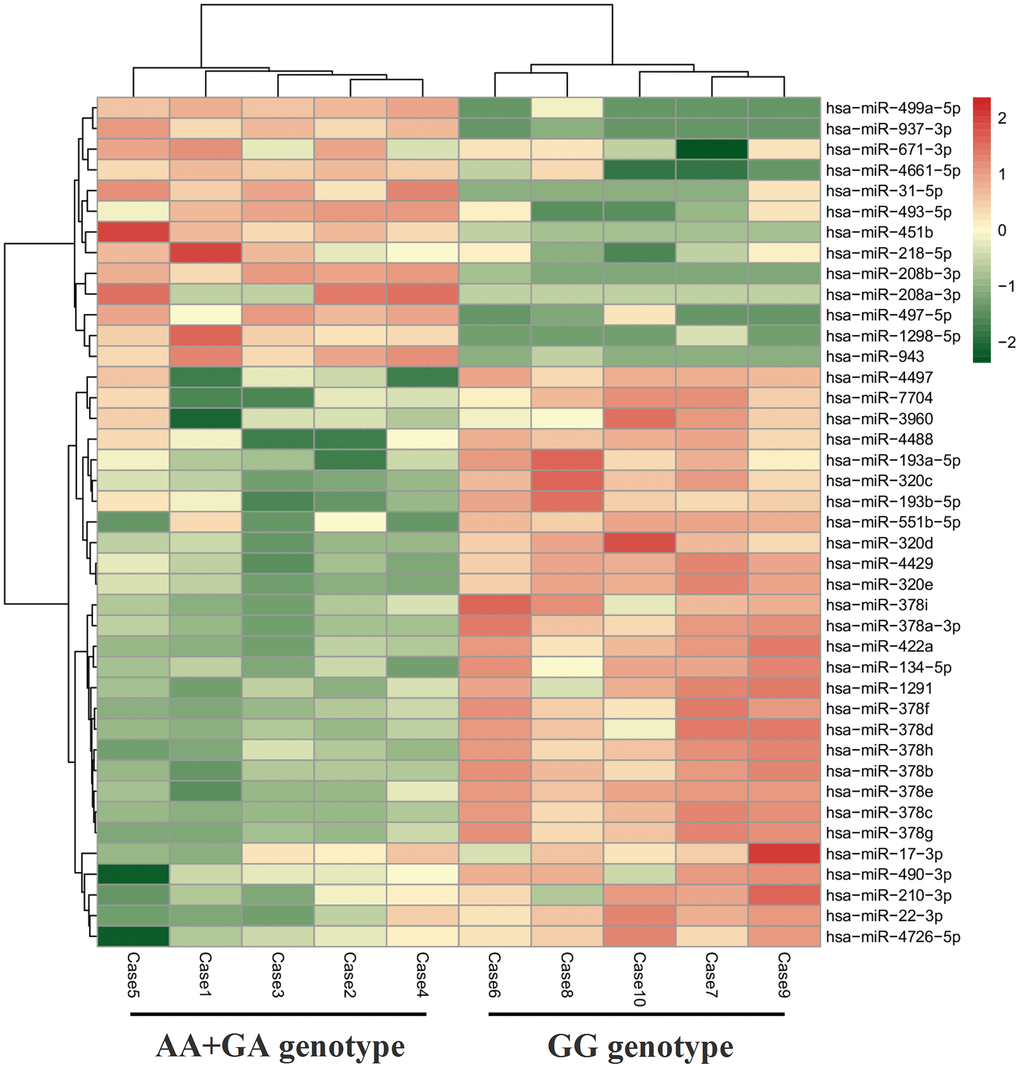
Figure 2. Heatmap of DE exo-miRs between different genotypes of KATP rs11046182 in subjects with elevated Apo B serum levels (≥ 80 mg/dL).
Table 6. DE exo-miRs between different genotypes of KATP rs11046182 in subjects with elevated Apo B serum levels (≥ 80 mg/dL).
| miR ID | Genotypes | Fold | P value | Up/down | ||
| AA+GA | GG | |||||
| 1 | hsa-miR-31-5p | 1.34 | 0.24 | -2.45 | 0.004751 | down |
| 2 | hsa-miR-451b | 8.10 | 0.44 | -4.21 | 0.005722 | down |
| 3 | hsa-miR-499a-5p | 26.82 | 4.04 | -2.73 | 0.007623 | down |
| 4 | hsa-miR-671-3p | 101.36 | 19.11 | -2.41 | 0.018733 | down |
| 5 | hsa-miR-208b-3p | 2.42 | 1.02 | -1.25 | 0.018905 | down |
| 6 | hsa-miR-937-3p | 3.25 | 1.16 | -1.48 | 0.024341 | down |
| 7 | hsa-miR-493-5p | 82.78 | 2.522 | -5.04 | 0.025111 | down |
| 8 | hsa-miR-208a-3p | 0.75 | 0.20 | -1.91 | 0.025430 | down |
| 9 | hsa-miR-218-5p | 76.76 | 4.22 | -4.19 | 0.029824 | down |
| 10 | hsa-miR-1298-5p | 5.43 | 1.01 | -2.43 | 0.035482 | down |
| 11 | hsa-miR-497-5p | 1.19 | 0.32 | -1.89 | 0.041277 | down |
| 12 | hsa-miR-4661-5p | 14.27 | 5.58 | -1.35 | 0.043491 | down |
| 13 | hsa-miR-943 | 1.51 | 0.24 | -2.65 | 0.049052 | down |
| 14 | hsa-miR-490-3p | 1.46 | 24.78 | 4.09 | 2.50E-05 | up |
| 15 | hsa-miR-378c | 70.22 | 1822.48 | 4.70 | 3.03E-05 | up |
| 16 | hsa-miR-378g | 6.52 | 59.63 | 3.19 | 5.65E-05 | up |
| 17 | hsa-miR-378f | 8.04 | 107.65 | 3.74 | 6.95E-05 | up |
| 18 | hsa-miR-1291 | 2.77 | 20.19 | 2.87 | 7.18E-05 | up |
| 19 | hsa-miR-378e | 1.07 | 23.87 | 4.48 | 0.000129 | up |
| 20 | hsa-miR-378h | 0.60 | 10.85 | 4.17 | 0.000132 | up |
| 21 | hsa-miR-378i | 138.95 | 1124.06 | 3.02 | 0.000135 | up |
| 22 | hsa-miR-378a-3p | 2047.51 | 19589.27 | 3.26 | 0.000162 | up |
| 23 | hsa-miR-320d | 245.90 | 9941.44 | 5.34 | 0.000258 | up |
| 24 | hsa-miR-422a | 4.49 | 46.97 | 3.39 | 0.000264 | up |
| 25 | hsa-miR-378d | 45.59 | 968.59 | 4.41 | 0.000309 | up |
| 26 | hsa-miR-378b | 0.70 | 18.01 | 4.69 | 0.000455 | up |
| 27 | hsa-miR-22-3p | 7649.18 | 25786.91 | 1.75 | 0.000498 | up |
| 28 | hsa-miR-4429 | 12.16 | 248.78 | 4.35 | 0.001036 | up |
| 29 | hsa-miR-320e | 50.86 | 955.40 | 4.23 | 0.001090 | up |
| 30 | hsa-miR-4726-5p | 0.57 | 3.75 | 2.71 | 0.001247 | up |
| 31 | hsa-miR-7704 | 0.77 | 9.68 | 3.66 | 0.001776 | up |
| 32 | hsa-miR-210-3p | 41.14 | 152.05 | 1.89 | 0.002202 | up |
| 33 | hsa-miR-320c | 649.53 | 12815.27 | 4.30 | 0.002883 | up |
| 34 | hsa-miR-134-5p | 497.18 | 13530.88 | 4.77 | 0.003356 | up |
| 35 | hsa-miR-4488 | 0.96 | 6.53 | 2.77 | 0.003878 | up |
| 36 | hsa-miR-3960 | 1.66 | 23.22 | 3.81 | 0.004081 | up |
| 37 | hsa-miR-193a-5p | 321.15 | 3274.08 | 3.35 | 0.007049 | up |
| 38 | hsa-miR-551b-5p | 0.51 | 4.36 | 3.08 | 0.008227 | up |
| 39 | hsa-miR-193b-5p | 22.09 | 256.94 | 3.54 | 0.023852 | up |
| 40 | hsa-miR-17-3p | 4.74 | 17.37 | 1.87 | 0.024641 | up |
| 41 | hsa-miR-4497 | 0.81 | 4.21 | 2.38 | 0.025088 | up |
GO analysis of enriched categories
Three terms of GO enriched categories analysis was carried out for those candidate target genes (CTGs) regulated by the top 10 DE exo-miRs, as shown in Figure 3. The CTGs of DE exo-miRs in high Apo B levels subjects with GG genotype of rs11046182 were obviously associated with the following biological processes: regulation of signaling, apoptotic process, protein complex subunit organization, vesicle-mediated transport, oxidation-reduction/homeostatic/lipid metabolic process, angiogenesis and autophagy so on, involving in the following cellular component such as vesicle, endoplasmic reticulum, mitochondrion and membrane protein/transcription factor/transmembrane transporter complex. Molecular functions affected by predicted target genes of DE exo-miRs, and can be mainly classified into two types: binding regulation (e.g., protein, ion, DNA, enzyme and ATP) and activity regulation (e.g., transcription factor, kinase activity, gated channel and oxidoreductase).
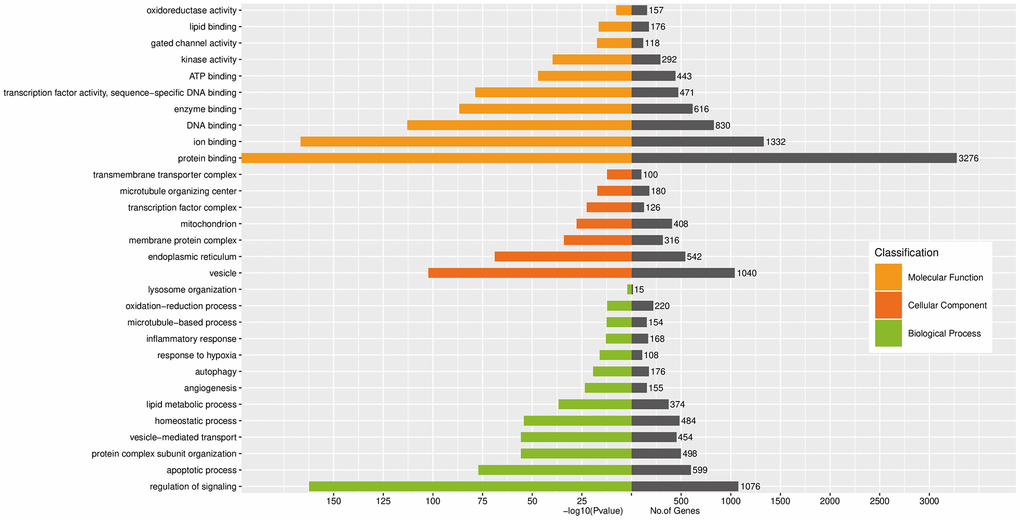
Figure 3. GO analysis of enriched biological processes, cellular component and molecular functions regulated by CTGs of top 10 DE exo-miRs.
KEGG analysis of enrichment pathways
KEGG analyses of top 10 DE exo-miRs showed that the top 30 enrichment pathways were mainly associated with metabolic pathways, environmental information/genetic information processing (e.g., endocytosis, signaling pathways of PI3K-Akt, MAPK and Ras, and protein processing in endoplasmic reticulum, etc), metabolism-related diseases (e.g., T2D, non-alcoholic fatty liver disease, and insulin resistance, etc), and organismal systems (e.g., insulin signaling pathway, platelet activation, and Toll-like receptor signaling pathway, etc), as shown in Figure 4.
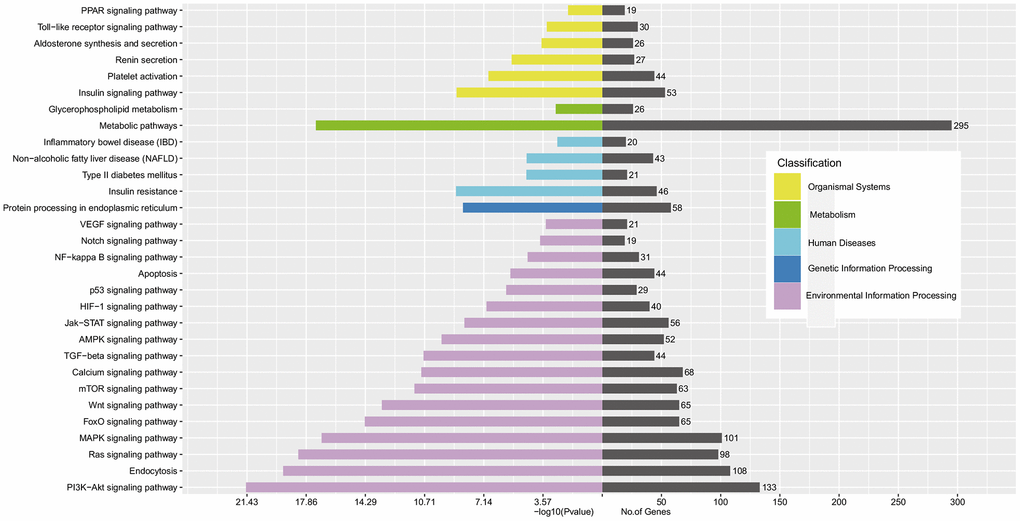
Figure 4. KEGG analysis of enrichment pathway regulated by CTGs of top 10 DE exo-miRs.
Target interactome network of top 10 DE exo-miRs
Using combined score greater than > 0.9 as threshold cutoff, a miRs/gene and gene/gene interaction network was consisted of 10 exo-miRs and 65 CTGs, regulated by differently regulated exo-miRs among increased Apo B serum levels (≥ 80 mg/dL) subjects with GG genotype of rs11046182, as shown in Figure 5. The highly correlated CTGs were as follows: ATP binding cassette subfamily A member 1 (ABCA1), carnitine palmitoyltransferase 1A (CPT1A), cytochrome b(558) subunit beta [CYBB, also NADPH oxidase 2 (NOX2)], hypoxia-inducible factor-1alpha (HIF-1α), jagged 1 (JAG1), Notch homolog 1 (translocation-associated) (Notch1), peroxisome proliferator-activated receptor-gamma coactivator-1alpha (PGC-1α), peroxisome proliferator-activated receptor-alpha (PPARα), 6-phosphofructo-2-kinase/fructose-2,6-biphosphatase 2 (PFKFB2), and solute carrier family 2 member 1 [SLC2A1, also called glucose transporter 1 (GLUT1)], etc.
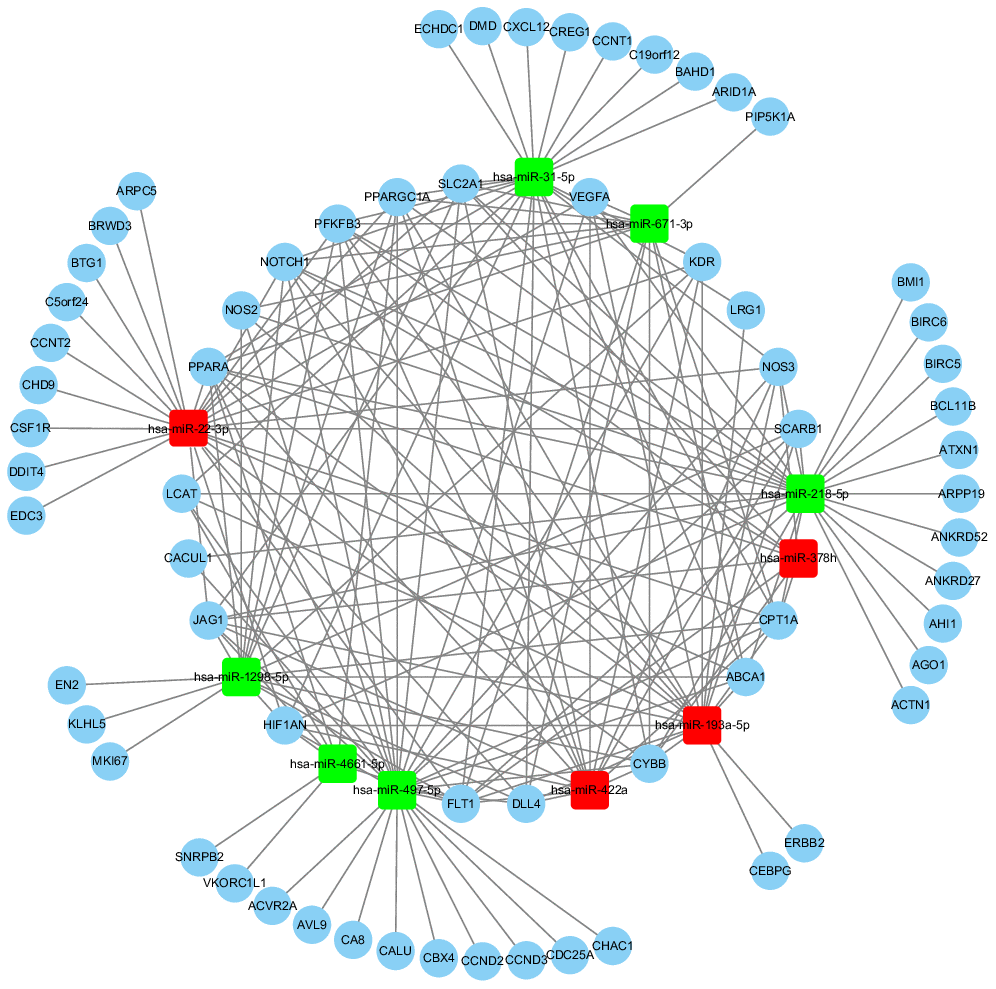
Figure 5. The cross-talk diagram on miRs-gene and gene-gene from top 10 DE exo-miRs. **Using combined score > 0.9 as threshold cutoff, 10 exo-miRs and 65 CTGs were included in the internet. Red color represents the up-regulated exo-miRs; Green color represents the down-regulated exo-miRs.
Discussion
To the best of our knowledge, this is the first comprehensive study to examine the possible associations of KATP SNPs with elevated Apo B serum concentration (≥ 80 mg/dL [11]) and ASCVD in south China. The data indicate that the GG genotype of rs11046182 was only linked to increased risk (about increased by 1.17-fold) of elevated Apo B serum levels rather than the other types of serum lipid disorder (e.g., TRIG, TC, LDL-C, HDL-C or (and) Apo AI, Supplementary Tables 3–7). The effects were not related to the other 3 KATP variants (e.g., rs78148713, rs145456027 and rs147265929). Interestingly, in this study there was no significant difference on body mass index (BMI), SBP, P2hBS, hypersensitive C-reactive protein (HsCRP) in subjects with or without higher Apo B serum levels (≥ 80 mg/dL) (Table 1), but its average levels of BMI (> 24.0 kg/m2), SBP (> 130 mmHg), P2hBS (> 7.8 mmol/L), HsCRP (> 3 mg/L) were higher than normal especially in higher Apo B level group, which was also complicated with higher serum levels of TRIG, TC and LDL-C. On the other hand, subjects with GG genotype of KATP rs11046182 were indeed related to higher serum levels of P2hBS and HsCRP besides high Apo B serum levels (Supplementary Table 8). It is suggesting that high Apo B serum level participants with GG genotype of KATP rs11046182 sustain a status of metabolic disorders and inflammation. Insulin resistance (IR) acts a major role in the pathogenesis of this process. Indeed, a previous study reported that KATP rs5219 was correlated with IR [12]. The loci also act an important role in process of glucose-induced insulin secretion among Turks [13] as well as the other two KATP variants (rs1799854 and rs1799859), the effect was not existed in Caribbeans (rs5219) [14] and Poles (rs1799854) [8]. On the other hand, blood lipid disorder is heterogeneous disease characterized by irregular levels of serum lipids and lipoproteins. Our findings are partially accordant with some similar studies. KATP rs1799854 (TT genotype) was linked to higher serum HDL level among non-diabetic patients in Nigeria as well as lower serum levels of TG, TC and LDL [4]. KATP rs1799854 and rs1799859 were linked to increased TRIG serum level among Croatia diabetic patients receiving sulfonylurea treatment [5]. KATP rs5219 (KK+EK genotype) was correlated with higher TC/HDL-C ratio among young Chinese Han people with prediabetes [6]. These findings indicated that KATP rs11046182 could be a latent genetic predisposition marker for elevated Apo B serum levels for Southern Chinese.
Cholesterol-rich, Apo B-containing lipoproteins are now widely accepted as the most important causal agents of ASCVD [15]. CAS no less than 50% is known as a new subtype of ASCVD besides acute myocardial infarction (AMI) and stroke [16]. In this study we further found that subjects carrying with GG genotype (the high Apo B risk genotype) of rs11046182 were also linked to moderate risk (about a 0.63-fold increase) of CAS ≥ 50% at studying enrollment, and further correlated with high risk (about a 1.24-fold increase) of new-onset IS after median follow-up of 50.6-months. These findings are partially accordant with the other related studies that found that KATP rs61688134 was associated with AMI among Italians [7] while KATP rs1799854 was with stroke in diabetic Polish [8]. These results suggest that KATP rs11046182 may be an optimal marker of elevated risk of Apo B related ASCVD.
The interplay between genetic and environment factors causes the development of dyslipidemia and related ASCVD. The circulating exo-miRs, as bridge that links genetic and environment factors, play an essential effect in physiological or pathological processes from elevated Apo B level to ASCVD. However, the expression profile of exo-miRs in biological process from genotype (KATP rs11046182) to phenotype (Apo B ≥ 80 mg/dL) is still largely unclear. Our results firstly characterized the circulating expression profile of exo-miRs (Table 4) among increased Apo B level subjects with the two genotypes of KATP rs11046182. Synchronously, studies had shown that those DE exo-miRs played a crucial effect in development of arteriosclerosis (e.g., miR-17-3p [17], miR-22-3p [18], miR-490-3p [19], miR-193 family [20], miR-320 family [21] and miR-378 family [22], etc), involving in endothelial cells dysfunction, vascular smooth muscle cells proliferation and migration, plaque angiogenesis, apoptosis, autophagy and macrophage lipid deposition. Many studies showed that miR-31-5p [23], miR-210-3p [24] and miR-208 family [25] were significantly associated with the stenosis degree of atherosclerotic plaques as well as unstable phenotype, suggesting that these exo-miRs could be correlated with the potential cardiovascular events risk. Our findings were in favor of recent observations that reported the DE miRs (e.g., miR-17-5p [26], miR-210 [27], miR-218 [28], miR-422a [29], miR-497 [30], miR-4429 [31], miR-208 family [25], miR-320 family [31] and miR-378 family [32]) in patients with IS, and part of them could be as markers for an early diagnosis of stroke. In a 4-year prospective study for identifying the markers of CAS related IS, Gacon J et al. [25] reported that elevated miR-208b-3p level were obviously linked to cerebral ischaemic events risk. This finding was accordant with the investigation by Jin F et al. [28] who reported that miR-378 and miR-218 were independent predicting factors for the severity in patients with acute IS. Further, the plasma level of miR-210 [33] was related to a worsening prognosis of stroke while miR-17 to future stroke recurrence [34]. Under the genetic condition of KATP rs11046182, these exo-miRs (e.g., miR-17-3p, miR-22-3p, miR-31-5p, miR-134-5p, miR-210-3p, miR-490-3p, miR-208 family, miR-320 family and miR-378 family) run through the whole pathological processes from the accumulation of cardiovascular risk factors (e.g., smoking, physical inactivity, unhealthy diet, obesity and aging) to the occurrence of atherosclerotic-related events and even death. In addition, there were another four exo-miRs as follows: miR-1291, miR-4488, miR-4726-5p, and miR-7704. However, the relationships of the 4 exo-miRs with cardiovascular disease are still unknown, needing further research.
To further evaluate the roles of exo-miRs under interaction between genetic and environment factors, GO and KEGG analysis for the top 10 DE exo-miRs related 1156 CTGs were carried out among elevated Apo B ≥ 80 mg/dL subjects with GG genotype of rs11046182. GO analyses (Figure 3) showed that enrichment of CTAs acted pivotal roles in BP, CC and MF, accordant with a regulatory role for these exo-miRs in the processes of transcription and translation [35] on dyslipidemia and related ASCVD. KEGG pathways analyses (Figure 4) showed that metabolic pathways, PI3K-Akt signaling pathway and endocytosis were the three most significant differentially regulated pathways. In particular, PI3K-Akt signaling pathway, which acts a principal role in regulating growth factor signals (e.g., glucose/lipid/protein metabolism, etc) under disease status (e.g., obesity and T2D) [36]. These results suggested that those DE exo-miRs might act a key effect in elevated Apo B serum levels and its induced ASCVD by regulating these 3 pathways, especially PI3K-Akt signaling pathway.
Strengths and limitations
The major advantage of the research was firstly evaluate the associations of KATP mutations with the risk of increased Apo B concentration (≥ 80 mg/dL) and ASCVD in South China, and characterize the circulating expression profile of exo-miRs under interplay status between genetic (KATP variants) and environmental (elevated Apo B serum levels) factors, intimating that the possible epigenetic modification effect of exo-miRs in development of dyslipidemia and its related atherosclerotic vascular events. The major disadvantages of the study were as follows: Firstly, due to the sample size (N=1044), large-scale subgroup analysis based on Apo B serum level (< 80 mg/dL vs. ≥ 80 mg/dL) and genotypes (GG vs. AA + GA) of KATP rs11046182 will help to further verify the hypothesis that the occurrence and development of increased Apo B serum concentration and its related ASCVD arises from complex interaction between genetic and environment factors. Secondly, Bonferroni correction was executed to correct significance thresholds, but false-positive results may still occur. Thirdly, a rudimentary bioinformatics analysis was only executed, and the non-specific effect and miss-distance effect may exist, owing to lack of verification at the cellular and molecular levels. Therefore, the results of the study should be interpreted carefully.
Conclusions
KATP rs11046182 was correlated with increased risks of elevated serum Apo B concentration (≥ 80 mg/dL) and ASCVD, suggesting that this variant is a prospective clinical translational target for precision prevention and early-detection strategies for those disorders, and needs further verification by prospective studies with large sample sizes in different ethnic populations. The potential molecular regulatory may be involved in these significantly DE exo-miRs (especially the top 10 DE exo-miRs) and metabolic related pathways (especially PI3K-Akt pathway) under those cross-talk status, warrant further research.
Materials and Methods
Study subjects
The ethics approval (K-2017-043-02) of this study was granted from Guangzhou First People’s Hospital, South China University of Technology. The present study was conducted in consistent with the Helsinki Declaration and the ethics guidelines of the institutional. A total of 522 participants with increased Apo B serum levels (≥ 80 mg/dL) and 522 counterpart subjects (< 80 mg/dL) were enrolled to the research from South China. All participants with blood lipid disorder were newly identified referring to guidelines [11] as follows: increased serum concentrations of Apo B (≥ 80 mg/dL), TRIG (≥ 1.7 mmol/L), TC (≥ 5.2 mmol/L) or (and) LDL-C (≥ 1.4 mmol/L), and (or) decreased serum concentrations of apolipoprotein AI (Apo AI) (< 120 mg/dL) and HDL-C (< 1.0 mmol/L). The combined medical conditions including essential hypertension (EH) [37], coronary atherosclerotic heart disease (CAD) [38], atrial fibrillation (AF) [39] or (and) type 2 diabetes mellitus (T2D) [40] were also evaluated referring to relevant guidelines. Potential participants were excluded from the study if they had if they had (1) past history of stroke or transient ischemic attack, (2) Elevated levels (>3 times upper limit of normal) of aspartate aminotransferase (AST) and alanine aminotransferase (ALT), (3) decreased level (<90ml/min•1.73 m2) of estimated glomerular filtration rate (eGFR), (4) or (and) any other medical disorders or drugs that could result in kinds of dyslipidemia as mentioned above. Participant’s medical records were assembled via interviewing patient himself and physicians as well as reviewing of medical records. Standard analytical methods were performed to assess blood biochemical indexes on admission to the study. Bilateral carotid ultrasound was executed on enrollment to the study referring to relevant recommendations [41].
Genotyping assay
Four KATP single nucleotide polymorphisms (SNPs) (e.g., rs11046182, rs78148713, rs145456027 and rs147265929) were genotyped with the MassARRAY (Sequenom) system as previously described methods [42]. Primer software (Version 5.0, Cambridge, USA) was used to design the specific primers for the 4 KATP variants based on the KATP gene sequence information in GenBank (NC_000012.12:g.21768149G>A; NC_000012.12:g.21777582T>C; NC_000012.11:g.21943896T>C; NC_000011.10:g.17391521T>G) (Supplementary Table 1). The specific primers of KATP SNPs were composited by Invitrogen (Guangzhou, China). The SNPs determination accuracy was 100% for each variant of KATP.
Endpoint
Primary follow-up end-point was new-onset IS. All stroke subjects were survivors of IS, and determined by magnetic resonance image and/or computed tomography scanning of the brain referring to relevant guidelines [43]. Subjects were recruited to the study on the date of initial evaluation for increased Apo B serum levels (≥ 80 mg/dL) since first medical examination. IS-free event survival time was defined as the time from the enrollment date to the date of initial evaluation for IS or last follow-up. The date of final follow-up was Dec 31, 2019. The median follow-up time was 50.6 (range: 43.5-58.7) months.
Identification of exo-miRs expression profile
Another total of 10 participants from South China with only elevated serum Apo B concentration (≥ 80 mg/dL) were newly enrolled to the study (the baseline characteristics was shown in Table 5). Participants with other types of serum lipid disorder were ruled out from the study as described above. All participants combined with smoking, drinking, EH, CAD, AF, T2D, IS, abnormal liver/kidney function, or (and) any other medical disorders or drugs that could result in kinds of dyslipidemia were also excluded from the study as described above. Then, the exo-miRs expression profile was analyzed according to our previous method with minor modifications [44], including blood sample collection, isolation exosomes from plasma, extraction RNA from exosomes, exo-miRs sequencing, and analysis of sequencing data (detail information was presented in methods section of Supplementary Material). In particular, exo-miRs sequencing was executed at Ribobio Co. (Guangzhou, China) with Illumina HiSeq2500 with single-end 50bp (Illumina, Carlsbad, USA). 3' adapter sequence is: 5’-AGATCGGAAGAGCACACGTCT-3’. 5' adapter sequence is: 5’-GTTCAGAGTTCTACAGTCCGACGATC-3’. The novel exo-miRs discovery was performed using miRDeep2 based on miRBase21 (http://www.mirbase.org).
Statistical analysis
The SPSS software (version 24, SPSS Co., USA) was used for statistical analyses. The Hardy-Weinberg equilibrium was evaluated for control subjects as shown in Supplementary Table 2. Continuous variables were presented as mean ± SD while categorical variables were as number (percentage). The independent-samples t-test is used to analyze continuous variables. The χ2 test was carried out to evaluate the associations between KATP variants and those categorical variables. Binary logistic regression analysis was executed to analyze the associations of KATP variants with these types of serum lipid disorder as well as CAS ≥ 50%, Bonferroni correction was carried out to adjust the probability of type I error (false positive). The Cox proportional hazards regression model was carried out to access the crude hazard ratios (HRs) for event free analysis of new-onset IS, adjusted HRs and their 95% confidence intervals (CIs) with corrections for potential covariates. A P value < 0.05 is statistically significant. All probabilities are two-tailed.
The differentially expressed (DE) exo-miRs in increased Apo B levels (≥ 80 mg/dL) subjects with different genotypes (GG vs. AA+GA) of rs11046182 were analyzed with edgeR software referring to the criteria of |log2 (Fold Change)| no less than 1 and P value less than 0.05. Gene Ontology (GO) category and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment were analyzed with the Fisher’s exact test and χ2 test, and followed by false discovery rate (FDR) correction. A corrected P value < 0.05 was performed to choose significant GO categories and KEGG pathways.
Author Contributions
CL was responsible for literature search, study design, the general supervision of the research group, protocol writing, data collection, data processing, data interpretation, data analysis, and the manuscript writing. TWG participated in the most of the experiments and data analysis. YXL and JFZ also participated in some of the experiments, data collection and statistical analysis; YS and TWG participated in patients recruitment, data collection and patients follow-up. The manuscript has been read and approved by all authors.
Acknowledgments
The authors wish to thank all the study participants from the South China Cardiovascular Related Disease Cohort (SCCDC), research staff and students who participated in this work.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This study was funded by the Guangzhou Science and Technology Project of China (2012J4100035 and 201804010214), the National Natural Science Foundation of China (81100235), the Natural Science Foundation of Guangdong China (S2011040004458), the Guangdong Science and Technology Planning Project of China (2014A020212372).
References
- 1. Michos ED, McEvoy JW, Blumenthal RS. Lipid management for the prevention of atherosclerotic cardiovascular disease. N Engl J Med. 2019; 381:1557–67. https://doi.org/10.1056/NEJMra1806939 [PubMed]
- 2. Sniderman AD, Robinson JG. ApoB in clinical care: pro and con. Atherosclerosis. 2019; 282:169–75. https://doi.org/10.1016/j.atherosclerosis.2018.11.001 [PubMed]
- 3. Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019; 139:e1082–e143. https://doi.org/10.1161/CIR.0000000000000698
- 4. Engwa GA, Nwalo FN, Chikezie CC, Onyia CO, Ojo OO, Mbacham WF, Ubi BE. Possible association between ABCC8 C49620T polymorphism and type 2 diabetes in a Nigerian population. BMC Med Genet. 2018; 19:78. https://doi.org/10.1186/s12881-018-0601-1 [PubMed]
- 5. Nikolac N, Simundic AM, Saracevic A, Katalinic D. ABCC8 polymorphisms are associated with triglyceride concentration in type 2 diabetics on sulfonylurea therapy. Genet Test Mol Biomarkers. 2012; 16:924–30. https://doi.org/10.1089/gtmb.2011.0337 [PubMed]
- 6. Xu M, Hu H, Deng D, Chen M, Xu Z, Wang Y. Prediabetes is associated with genetic variations in the gene encoding the Kir6.2 subunit of the pancreatic ATP-sensitive potassium channel (KCNJ11): a case-control study in a Han Chinese youth population. J Diabetes. 2018; 10:121–29. https://doi.org/10.1111/1753-0407.12565 [PubMed]
- 7. Smith KJ, Chadburn AJ, Adomaviciene A, Minoretti P, Vignali L, Emanuele E, Tammaro P. Coronary spasm and acute myocardial infarction due to a mutation (V734I) in the nucleotide binding domain 1 of ABCC9. Int J Cardiol. 2013; 168:3506–13. https://doi.org/10.1016/j.ijcard.2013.04.210 [PubMed]
- 8. Stefanski A, Majkowska L, Ciechanowicz A, Frankow M, Safranow K, Parczewski M, Pilarska K. The common C49620T polymorphism in the sulfonylurea receptor gene (ABCC8), pancreatic beta cell function and long-term diabetic complications in obese patients with long-lasting type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes. 2007; 115:317–21. https://doi.org/10.1055/s-2007-967086 [PubMed]
- 9. Tao J, Ma YT, Xiang Y, Xie X, Yang YN, Li XM, Fu ZY, Ma X, Liu F, Chen BD, Yu ZX, Chen Y. Prevalence of major cardiovascular risk factors and adverse risk profiles among three ethnic groups in the Xinjiang Uygur Autonomous Region, China. Lipids Health Dis. 2013; 12:185. https://doi.org/10.1186/1476-511X-12-185 [PubMed]
- 10. Pan Y, Wang T, Li Y, Guan T, Lai Y, Shen Y, Zeyaweiding A, Maimaiti T, Li F, Zhao H, Liu C. Association of ACE2 polymorphisms with susceptibility to essential hypertension and dyslipidemia in Xinjiang, China. Lipids Health Dis. 2018; 17:241. https://doi.org/10.1186/s12944-018-0890-6 [PubMed]
- 11. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Chapman MJ, De Backer GG, Delgado V, Ference BA, Graham IM, Halliday A, Landmesser U, et al, and ESC Scientific Document Group. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41:111–88. https://doi.org/10.1093/eurheartj/ehz455 [PubMed]
- 12. Wan J, Jiang X, Bai J, Shen D, Wang T. The effects of E23K polymorphism in Kir6.2 subunit on insulin sensitivity in skeletal muscle cells by long-chain fatty acyl CoA. Biochem Biophys Res Commun. 2009; 381:496–501. https://doi.org/10.1016/j.bbrc.2009.02.070 [PubMed]
- 13. Gonen MS, Arikoglu H, Erkoc Kaya D, Ozdemir H, Ipekci SH, Arslan A, Kayis SA, Gogebakan B. Effects of single nucleotide polymorphisms in K(ATP) channel genes on type 2 diabetes in a Turkish population. Arch Med Res. 2012; 43:317–23. https://doi.org/10.1016/j.arcmed.2012.06.001 [PubMed]
- 14. Ezenwaka C, Kalloo R, Uhlig M, Schwenk R, Eckel J. The E23K variant in the Kir6.2 subunit of the ATP-sensitive K+ channel does not augment impaired glucose tolerance in Caribbean subjects with a family history of type 2 diabetes. J Endocrinol. 2005; 185:439–44. https://doi.org/10.1677/joe.1.06117 [PubMed]
- 15. Robinson JG, Williams KJ, Gidding S, Borén J, Tabas I, Fisher EA, Packard C, Pencina M, Fayad ZA, Mani V, Rye KA, Nordestgaard BG, Tybjærg-Hansen A, et al. Eradicating the Burden of Atherosclerotic Cardiovascular Disease by Lowering Apolipoprotein B Lipoproteins Earlier in Life. J Am Heart Assoc. 2018; 7:e009778. https://doi.org/10.1161/JAHA.118.009778 [PubMed]
- 16. Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, Wilson DP, Brown WV. National Lipid Association recommendations for patient-centered management of dyslipidemia: part 1 - executive summary. J Clin Lipidol. 2014; 8:473–88. https://doi.org/10.1016/j.jacl.2014.07.007 [PubMed]
- 17. An JH, Chen ZY, Ma QL, Wang HJ, Zhang JQ, Shi FW. LncRNA SNHG16 promoted proliferation and inflammatory response of macrophages through miR-17-5p/NF-κB signaling pathway in patients with atherosclerosis. Eur Rev Med Pharmacol Sci. 2019; 23:8665–77. https://doi.org/10.26355/eurrev_201910_19184 [PubMed]
- 18. Tang Y, Jin X, Xiang Y, Chen Y, Shen CX, Zhang YC, Li YG. The lncRNA MALAT1 protects the endothelium against ox-LDL-induced dysfunction via upregulating the expression of the miR-22-3p target genes CXCR2 and AKT. FEBS Lett. 2015; 589:3189–96. https://doi.org/10.1016/j.febslet.2015.08.046 [PubMed]
- 19. Liu Y, Chen Y, Tan L, Zhao H, Xiao N. Linc00299/miR-490-3p/AURKA axis regulates cell growth and migration in atherosclerosis. Heart Vessels. 2019; 34:1370–80. https://doi.org/10.1007/s00380-019-01356-7 [PubMed]
- 20. Sun Y, Zhang S, Yue M, Li Y, Bi J, Liu H. Angiotensin II inhibits apoptosis of mouse aortic smooth muscle cells through regulating the circNRG-1/miR-193b-5p/NRG-1 axis. Cell Death Dis. 2019; 10:362. https://doi.org/10.1038/s41419-019-1590-5 [PubMed]
- 21. Xu X, Ma C, Liu C, Duan Z, Zhang L. Knockdown of long noncoding RNA XIST alleviates oxidative low-density lipoprotein-mediated endothelial cells injury through modulation of miR-320/NOD2 axis. Biochem Biophys Res Commun. 2018; 503:586–92. https://doi.org/10.1016/j.bbrc.2018.06.042 [PubMed]
- 22. Liu S, Yang Y, Jiang S, Xu H, Tang N, Lobo A, Zhang R, Liu S, Yu T, Xin H. MiR-378a-5p Regulates Proliferation and Migration in Vascular Smooth Muscle Cell by Targeting CDK1. Front Genet. 2019; 10:22. https://doi.org/10.3389/fgene.2019.00022 [PubMed]
- 23. Infante T, Forte E, Punzo B, Cademartiri F, Cavaliere C, Soricelli A, Salvatore M, Napoli C. Correlation of circulating miR-765, miR-93-5p, and miR-433-3p to obstructive coronary heart disease evaluated by cardiac computed tomography. Am J Cardiol. 2019; 124:176–82. https://doi.org/10.1016/j.amjcard.2019.04.016 [PubMed]
- 24. Eken SM, Jin H, Chernogubova E, Li Y, Simon N, Sun C, Korzunowicz G, Busch A, Bäcklund A, Österholm C, Razuvaev A, Renné T, Eckstein HH, et al. MicroRNA-210 enhances fibrous cap stability in advanced atherosclerotic lesions. Circ Res. 2017; 120:633–44. https://doi.org/10.1161/CIRCRESAHA.116.309318 [PubMed]
- 25. Gacoń J, Badacz R, Stępień E, Karch I, Enguita FJ, Żmudka K, Przewłocki T, Kabłak-Ziembicka A. Diagnostic and prognostic micro-RNAs in ischaemic stroke due to carotid artery stenosis and in acute coronary syndrome: a four-year prospective study. Kardiol Pol. 2018; 76:362–69. https://doi.org/10.5603/KP.a2017.0243 [PubMed]
- 26. Wu J, Du K, Lu X. Elevated expressions of serum miR-15a, miR-16, and miR-17-5p are associated with acute ischemic stroke. Int J Clin Exp Med. 2015; 8:21071–79. [PubMed]
- 27. Wang LQ, Wang CL, Xu LN, Hua DF. The expression research of miR-210 in the elderly patients with COPD combined with ischemic stroke. Eur Rev Med Pharmacol Sci. 2016; 20:4756–60. [PubMed]
- 28. Jin F, Xing J. Circulating pro-angiogenic and anti-angiogenic microRNA expressions in patients with acute ischemic stroke and their association with disease severity. Neurol Sci. 2017; 38:2015–23. https://doi.org/10.1007/s10072-017-3071-x [PubMed]
- 29. Li DB, Liu JL, Wang W, Li RY, Yu DJ, Lan XY, Li JP. Plasma exosomal miR-422a and miR-125b-2-3p serve as biomarkers for ischemic stroke. Curr Neurovasc Res. 2017; 14:330–37. https://doi.org/10.2174/1567202614666171005153434 [PubMed]
- 30. Wang J, Lin M, Ren H, Yu Z, Guo T, Gu B. Expression and clinical significance of serum miR-497 in patients with acute cerebral infarction. Clin Lab. 2019; 65. https://doi.org/10.7754/Clin.Lab.2018.181001 [PubMed]
- 31. Jickling GC, Ander BP, Zhan X, Noblett D, Stamova B, Liu D. microRNA expression in peripheral blood cells following acute ischemic stroke and their predicted gene targets. PLoS One. 2014; 9:e99283. https://doi.org/10.1371/journal.pone.0099283 [PubMed]
- 32. Wang P, He Q, Liu C, He SZ, Zhu SY, Li YW, Su W, Xiang ST, Zhao B. Functional polymorphism rs3783553 in the 3'-untranslated region of IL-1A increased the risk of ischemic stroke: a case-control study. Medicine (Baltimore). 2017; 96:e8522. https://doi.org/10.1097/MD.0000000000008522 [PubMed]
- 33. Zeng L, Liu J, Wang Y, Wang L, Weng S, Chen S, Yang GY. Cocktail blood biomarkers: prediction of clinical outcomes in patients with acute ischemic stroke. Eur Neurol. 2013; 69:68–75. https://doi.org/10.1159/000342896 [PubMed]
- 34. Kim JM, Jung KH, Chu K, Lee ST, Ban J, Moon J, Kim M, Lee SK, Roh JK. Atherosclerosis-related circulating MicroRNAs as a predictor of stroke recurrence. Transl Stroke Res. 2015; 6:191–97. https://doi.org/10.1007/s12975-015-0390-1 [PubMed]
- 35. Liu X, Fortin K, Mourelatos Z. MicroRNAs: biogenesis and molecular functions. Brain Pathol. 2008; 18:113–21. https://doi.org/10.1111/j.1750-3639.2007.00121.x [PubMed]
- 36. Huang X, Liu G, Guo J, Su Z. The PI3K/AKT pathway in obesity and type 2 diabetes. Int J Biol Sci. 2018; 14:1483–96. https://doi.org/10.7150/ijbs.27173 [PubMed]
- 37. Carey RM, Whelton PK, and 2017 ACC/AHA Hypertension Guideline Writing Committee. Prevention, detection, evaluation, and management of high blood pressure in adults: synopsis of the 2017 American college of cardiology/American heart association hypertension guideline. Ann Intern Med. 2018; 168:351–58. https://doi.org/10.7326/M17-3203 [PubMed]
- 38. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio AL, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, et al, and ESC Scientific Document Group. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European society of cardiology (ESC). Eur Heart J. 2018; 39:119–77. https://doi.org/10.1093/eurheartj/ehx393 [PubMed]
- 39. January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC
Jr , Ellinor PT, Ezekowitz MD, Field ME, Furie KL, Heidenreich PA, Murray KT, Shea JB, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society in collaboration with the society of thoracic surgeons. Circulation. 2019; 140:e125–51. https://doi.org/10.1161/CIR.0000000000000665 [PubMed] - 40. Olokoba AB, Obateru OA, Olokoba LB. Type 2 diabetes mellitus: a review of current trends. Oman Med J. 2012; 27:269–73. https://doi.org/10.5001/omj.2012.68 [PubMed]
- 41. Meschia JF, Klaas JP, Brown RD
Jr , Brott TG. Evaluation and management of atherosclerotic carotid stenosis. Mayo Clin Proc. 2017; 92:1144–57. https://doi.org/10.1016/j.mayocp.2017.02.020 [PubMed] - 42. Liu C, Li Y, Guan T, Lai Y, Shen Y, Zeyaweiding A, Zhao H, Li F, Maimaiti T. ACE2 polymorphisms associated with cardiovascular risk in Uygurs with type 2 diabetes mellitus. Cardiovasc Diabetol. 2018; 17:127. https://doi.org/10.1186/s12933-018-0771-3 [PubMed]
- 43. Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, Fang MC, Fisher M, Furie KL, Heck DV, Johnston SC, Kasner SE, Kittner SJ, et al, and American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2014; 45:2160–236. https://doi.org/10.1161/STR.0000000000000024 [PubMed]
- 44. Liu C, Lai Y, Ying S, Zhan J, Shen Y. Plasma exosome-derived microRNAs expression profiling and bioinformatics analysis under cross-talk between increased low-density lipoprotein cholesterol level and ATP-sensitive potassium channels variant rs1799858. J Transl Med. 2020; 18:459. https://doi.org/10.1186/s12967-020-02639-8 [PubMed]