



Introduction
Liver cancer is the sixth most common cancer, and the fourth most common cause of cancer-related death reported in CA: A Cancer Journal for Clinicians [1], with an annual incidence of 841,080 patients [1]. It is estimated that about 42,810 individuals will be diagnosed with liver cancer in the United States in 2020, of whom 30,160 will die [2]. In virtually all countries, males exhibit incidence and mortality rates 2 to 3 times higher than women [1, 3]. As such, addressing the high mortality and poor prognosis associated with liver cancer remains an urgent priority.
In recent years, some studies have reported significant differences in survival rates between men and women among those with liver cancer [4–8]. Also, multivariate Cox regression analyses reveal that race [5–8], marriage [6], and economic status [9] also affect the survival of individuals with liver cancer. In contrast, however, some other studies have reported no significant prognostic differences between males and females [8]. Some recent studies have reported that estrogen may play a role in the prognosis of patients with liver cancer [10–12], while others have reported no such effect [3]. Unfortunately, most—if not all—of these studies were performed using a pool of patients in surgical and non-operative states, even though surgery is a vital factor influencing patient prognosis [13]. As such, they could not fully reveal the true impact of gender differences on the prognosis of liver cancer patients in natural states.
To reveal the real-world situation, our study focused on factors affecting prognosis in patients with liver cancer who had not undergone surgery and, in addition, we also performed related in vitro experiments. The results revealed a significant difference between males and females in terms of survival among those with liver cancer. The results of in vitro experiments revealed that, although estrone did not have a significant effect on liver cancer cells, estradiol played a central role.
Results
Meta-analysis of the influence of gender on the OS of patients with liver cancer
The literature search retrieved 424 unique citations. After screening of titles and abstracts, 87 full-text articles remained for assessment, reporting that females had longer survival than males in different type cancer (pooled HR 0.86 [95% CI: 0.83–0.89]; p < 0.001; I2 = 98%) (Supplementary Figure 1). Finally, 6 studies including 98,010 individuals were reviewed to appraise the effect of gender on the OS of liver cancer patients. The forest plot of gender for the efficacy in reducing the risk for prognosis in liver cancer patients is shown in Supplementary Figure 2. Among patients with liver cancer, females demonstrated better prognosis than males (pooled HR 0.93 [95% CI: 0.91–0.94]; p < 0.001; I2 = 0%), and homogeneity performed well.
Characteristics of liver cancer patients from the SEER database
Data from 12,312 liver cancer patients housed in the SEER research database, who had not undergone surgery between 2010 and 2015, were included in this study. All participants were randomly divided into the primary (70% [n = 8658]) or validation (30% [n = 3654]) cohort. The baseline characteristics of these cohorts are summarized in Table 1. Among all patients, 27.2% (n = 2375) were female and 72.8% (n = 8966) were male. In total, 17.9% (n = 2200) were ≤ 55 years of age at diagnosis and 82.1% (n = 10,112) were > 55 years of age. The distribution according to race/ethnicity was as follows: white, 69.5% (n = 8553); black, 12.8% (n = 1580); and other (American Indian/AK Native, Asian/Pacific Islander), 17.7% (n = 2179). According to the American Joint Committee on Cancer, 28.5% (n = 3515) of patients were grade I at diagnosis, 47.2% (n = 5809) were grade II, 22.7% (n = 2800) were grade III, and 1.5% (n = 188) were grade IV. Among these individuals, 57.6% (n = 7090) were married, 19.1% (n = 2348) were single, 11.2% (n = 1378) were divorced, and 10.3% (n = 1269) were widowed. According to pathology, 88.7% (n = 10,924) had HCC, 11.1% (n = 996) had intrahepatic cholangiocarcinoma (ICCs), and others were combined. Regarding tumor size, 26.1% (n = 3217) of individuals exhibited lesions < 30 mm and 73.9% (n = 9095) had lesions > 30 mm. Tumor TNM stages are summarized in Table 1. Percentages were similar between the primary and validation cohorts.
Table 1. Baseline characteristics of patients.
| Characteristic | All of patients(n=12312) | Primary cohort(n=8658) | Validation cohort(n=3654) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No of patients | % | No of patients | % | No of patients | % | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤55 | 2200 | 17.9 | 1552 | 17.9 | 648 | 17.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >55 | 10112 | 82.1 | 7106 | 82.1 | 3006 | 82.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White | 8553 | 69.5 | 6052 | 69.9 | 2501 | 68.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Black | 1580 | 12.8 | 1088 | 12.6 | 492 | 13.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other a | 2179 | 17.7 | 1518 | 17.5 | 661 | 18.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 8966 | 72.8 | 6283 | 72.6 | 2683 | 73.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 3346 | 27.2 | 2375 | 27.4 | 971 | 26.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 3515 | 28.5 | 2515 | 29.0 | 1000 | 27.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2 | 5809 | 47.2 | 4039 | 46.7 | 1770 | 48.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | 2800 | 22.7 | 1965 | 22.7 | 835 | 22.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 | 188 | 1.5 | 139 | 1.6 | 49 | 1.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor T | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T0 | 9 | 0.1 | 6 | 0.1 | 3 | 0.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | 5676 | 46.1 | 3991 | 46.1 | 1684 | 46.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 3068 | 24.9 | 2166 | 25.0 | 902 | 24.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 2772 | 22.5 | 1947 | 22.5 | 825 | 22.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 505 | 4.1 | 354 | 4.1 | 151 | 4.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TX | 283 | 2.3 | 194 | 2.2 | 89 | 2.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor N | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | 10640 | 86.4 | 7476 | 86.3 | 3164 | 86.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 1062 | 8.6 | 763 | 8.8 | 299 | 8.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NX | 610 | 5.0 | 419 | 4.8 | 191 | 5.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor M | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M0 | 10855 | 88.2 | 7626 | 88.1 | 3229 | 88.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| M1 | 1457 | 11.8 | 1032 | 11.9 | 425 | 11.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Marital status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Divorced | 1378 | 11.2 | 952 | 11.0 | 426 | 11.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single | 2348 | 19.1 | 1639 | 18.9 | 709 | 19.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Married | 7090 | 57.6 | 5005 | 57.8 | 2085 | 57.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Separated | 185 | 1.5 | 134 | 1.5 | 51 | 1.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Windowed | 1269 | 10.3 | 899 | 10.4 | 370 | 10.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unmarried or Domestic partner | 42 | 0.3 | 29 | 0.3 | 13 | 0.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor size (mm c) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤30 | 3217 | 26.1 | 2265 | 26.2 | 952 | 26.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >30 | 9095 | 73.9 | 6393 | 73.8 | 2702 | 73.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Histologic Type | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ICCs | 1367 | 11.1 | 996 | 11.5 | 371 | 10.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HCC | 10924 | 88.7 | 7648 | 88.3 | 3276 | 89.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Combined b | 21 | 0.2 | 14 | 0.2 | 7 | 0.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: HCC, hepatocellular carcinoma; ICCs, intrahepatic cholangiocarcinomas. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a Contain American Indian/AK Native, Asian/Pacific Islander. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| b HCC+ICCs. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| c millimeter. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Survival analysis
Univariate and multivariate Cox regression hazards models were used to analyze prognostic factors in patients with liver cancer (Tables 2, 3). In the univariate Cox models, age, sex, race, grade, tumor TNM stage, marital status, tumor size, and histological type were significantly associated with OS of non-surgical liver cancer patients (p < 0.05). Multivariate Cox analysis confirmed that all of those variables were independent prognostic factors for OS (p < 0.05).
Table 2. Univariate cox regression analyses of primary and validation cohorts.
| Characteristic | Primary cohorts(n=8658) | Validation cohorts(n=3654) | ||||
| HR | 95%CI | p value | HR | 95%CI | p value | |
| Age | <0.001 | <0.001 | ||||
| ≤55 | Ref | Ref | ||||
| > 55 | 1.165 | (1.080-1.257) | <0.001 | 1.398 | (1.239-1.576) | <0.001 |
| Race | <0.001 | <0.001 | ||||
| White | Ref | Ref | ||||
| Black | 1.154 | (1.061-1.255) | 0.001 | 1.147 | (1.012-1.300) | 0.031 |
| Other | 0.818 | (0.755-0.886) | <0.001 | 0.788 | (0.699-0.889) | <0.001 |
| Sex | 0.001 | 0.047 | ||||
| Male | Ref | Ref | ||||
| Female | 0.898 | (0.842- 0.958) | 0.001 | 0.903 | (0.817-0.998) | 0.047 |
| Grade | <0.001 | <0.001 | ||||
| 1 | Ref | Ref | ||||
| 2 | 1.039 | (0.969-1.115) | 0.284 | 0.995 | (0.894-1.107) | 0.923 |
| 3 | 1.932 | (1.789-2.087) | <0.001 | 1.644 | (1.459-1.852) | <0.001 |
| 4 | 2.169 | (1.764-2.666) | <0.001 | 2.115 | (1.521-2.940) | <0.001 |
| Tumor T | <0.001 | <0.001 | ||||
| TX | Ref | Ref | ||||
| T0 | 1.537 | (0.680-3.474) | 0.301 | 0.936 | (0.295-2.970) | 0.910 |
| T1 | 0.298 | (0.253-0.351) | <0.001 | 0.312 | (0.246-0.397) | <0.001 |
| T2 | 0.354 | (0.299-0.419) | <0.001 | 0.359 | (0.280-0.459) | <0.001 |
| T3 | 0.877 | (0.744-1.033) | 0.116 | 0.875 | (0.688-1.113) | 0.277 |
| T4 | 0.861 | (0.708-1.049) | 0.137 | 0.929 | (0.695-1.243) | 0.620 |
| Tumor N | <0.001 | <0.001 | ||||
| N0 | Ref | Ref | ||||
| N1 | 2.577 | (2.360-2.813) | <0.001 | 2.412 | (2.102-2.769) | <0.001 |
| NX | 2.273 | (2.025-2.553) | <0.001 | 2.564 | (2.175-3.022) | <0.001 |
| Tumor M | <0.001 | <0.001 | ||||
| M0 | Ref | Ref | ||||
| M1 | 3.527 | (3.270-3.804) | <0.001 | 3.219 | (2.866-3.616) | <0.001 |
| Marital status | <0.001 | <0.001 | ||||
| Divorced | Ref | Ref | ||||
| Single | 1.051 | (0.946-1.169) | 0.354 | 0.986 | (0.844-1.152) | 0.863 |
| Married | 0.855 | (0.780-0.938) | 0.001 | 0.795 | (0.694-0.911) | 0.001 |
| Separated | 1.141 | (0.905-1.437) | 0.264 | 1.237 | (0.869-1.762) | 0.238 |
| Windowed | 1.222 | (1.087-1.374) | 0.001 | 0.990 | (0.828-1.183) | 0.911 |
| Unmarried or Domestic partner | 0.515 | (0.256-1.036) | 0.063 | 0.622 | (0.277-1.398) | 0.251 |
| Tumor size(mm) | <0.001 | <0.001 | ||||
| ≤30 | Ref | Ref | ||||
| >30 | 2.382 | (2.208-2.569) | <0.001 | 2.265 | (2.020-2.541) | <0.001 |
| Histologic Type | 0.009 | 0.280 | ||||
| ICCs | Ref | Ref | ||||
| HCC | 0.872 | (0.798-0.952) | 0.002 | 0.895 | (0.776-1.033) | 0.129 |
| Combined | 0.797 | (0.378-1.679) | 0.550 | 0.708 | (0.263-1.903) | 0.493 |
According to the results of multivariate Cox analysis, patients < 55 years of age had a worse prognosis than those ≤ 55 years of age (HR 1.198 [95% CI: 1.109-1.295; p < 0.001) (Table 3). Compared with Caucasians, other races (i.e., American Indian/AK Native, Asian/Pacific Islander) had a better prognosis (HR 0.805 [95% CI: 0.742-0.873; p < 0.001), but blacks did not (p = 0.068) (Table 3). There were significant prognostic differences between males and females among non-surgical liver cancer patients. Females demonstrated a better prognosis than males (p < 0.001) (Figure 1A), and survived longer than males (32.3 ± 0.7 vs. 30.1 ± 0.4 months, respectively; p = 0.001). Compared with males, females had a lower hazard ratio (HR 0.868 [95% CI: 0.810-0.930; p < 0.001). As the clinical grade increased, patient prognosis worsened (p < 0.001); however, grade 2 was not an independent risk factor for prognosis in non-surgical liver cancer patients (p = 0.586). The HRs for tumor TNM stage are shown in Table 3. Patients who were married demonstrated better prognosis (HR 0.805 [95% CI: 0.805-0.953]; p = 0.011), and widowed patients demonstrated poor prognosis (HR 1.251 [95% CI: 1.029-1.410]; p < 0.001). Compared with ICCs, patients with HCC have a worse prognosis (HR 1.168 [95% CI: 1.060-1.287]; p = 0.002).
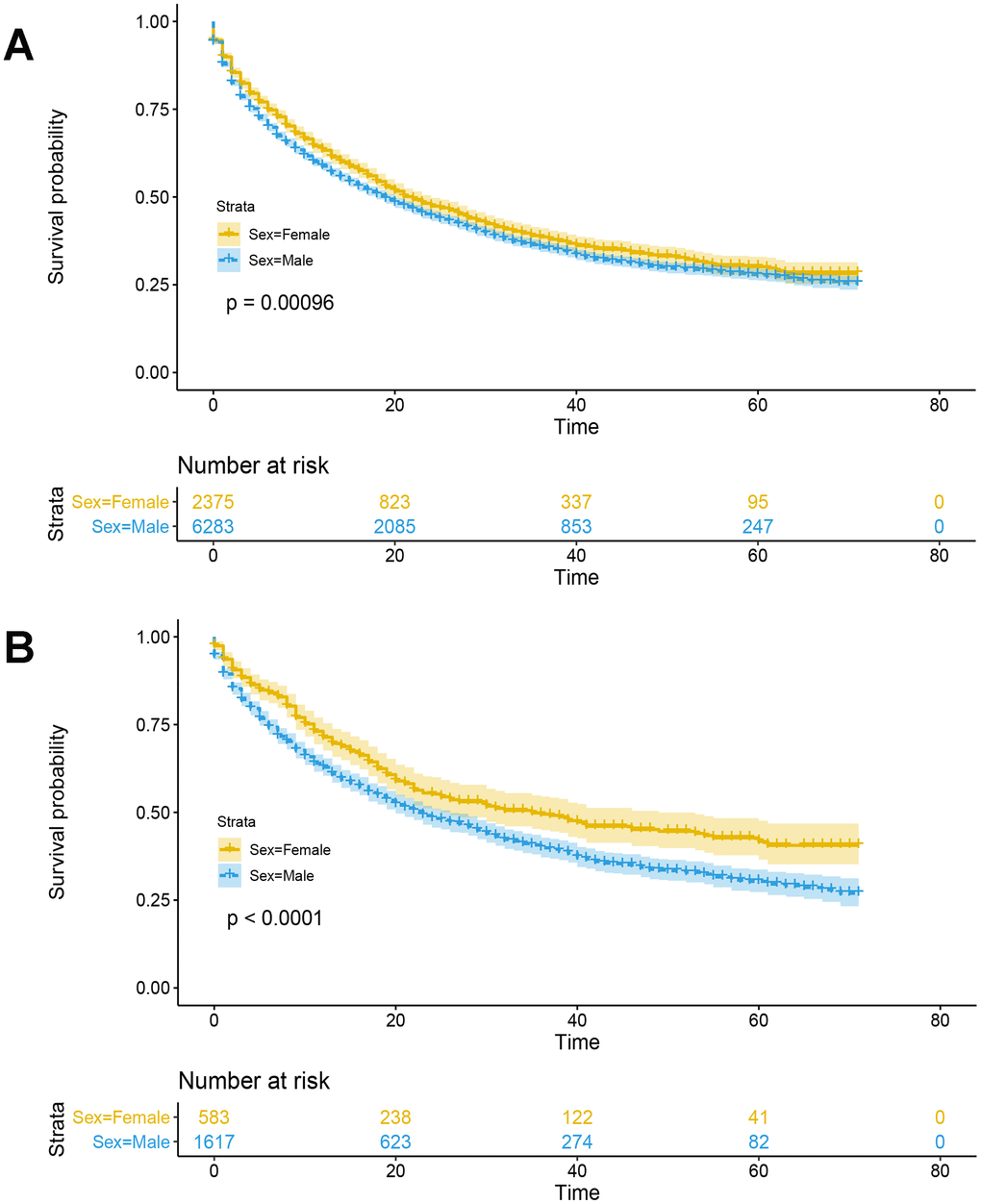
Figure 1. Kaplan-Meier survival analysis with log-rank test was performed in non-surgical liver cancer patients. (A) Kaplan-Meier survival analysis with log-rank test was performed in non-surgical liver cancer patients in the primary cohort. (B) Before menopause (i.e., ≤ 55 years of age), women with liver cancer have a better prognosis than men (p<0.0001, log-rank test).
Table 3. Multivariate cox regression analyses of primary and validation cohorts.
| Characteristic | Primary cohort(n=8658) | Validation cohort(n=3654) | ||||
| HR | 95%CI | p value | HR | 95%CI | p value | |
| Age | <0.001 | <0.001 | ||||
| ≤55 | Ref | Ref | ||||
| > 55 | 1.198 | (1.109-1.295) | <0.001 | 1.442 | (1.275-1.630) | <0.001 |
| Race | <0.001 | 0.033 | ||||
| White | Ref | Ref | ||||
| Black | 1.084 | (0.994-1.182) | 0.068 | 1.056 | (0.929-1.200) | 0.404 |
| Other | 0.805 | (0.742-0.873) | <0.001 | 0.863 | (0.763-0.977) | 0.020 |
| Sex | <0.001 | 0.012 | ||||
| Male | Ref | Ref | ||||
| Female | 0.868 | (0.810-0.930) | <0.001 | 0.873 | (0.784-0.971) | 0.012 |
| Grade | <0.001 | <0.001 | ||||
| 1 | Ref | Ref | ||||
| 2 | 0.980 | (0.913-1.053) | 0.586 | 0.974 | (0.874-1.085) | 0.627 |
| 3 | 1.578 | (1.456-1.710) | <0.001 | 1.442 | (1.276-1.631) | <0.001 |
| 4 | 1.615 | (1.311-1.990) | <0.001 | 1.856 | (1.327-2.595) | <0.001 |
| Tumor T | <0.001 | <0.001 | ||||
| TX | Ref | Ref | ||||
| T0 | 1.722 | (0.754-3.932) | 0.197 | 1.074 | (0.332-3.477) | 0.905 |
| T1 | 0.489 | (0.410-0.582) | <0.001 | 0.499 | (0.385-0.645) | <0.001 |
| T2 | 0.554 | (0.463-0.663) | <0.001 | 0.564 | (0.433-0.734) | <0.001 |
| T3 | 1.014 | (0.853-1.206) | 0.874 | 1.026 | (0.794-1.325) | 0.846 |
| T4 | 0.907 | (0.739-1.113) | 0.349 | 1.026 | (0.756-1.392) | 0.871 |
| Tumor N | <0.001 | <0.001 | ||||
| N0 | Ref | Ref | ||||
| N1 | 1.447 | (1.311-1.597) | <0.001 | 1.529 | (1.312-1.783) | <0.001 |
| NX | 1.431 | (1.264-1.621) | <0.001 | 1.790 | (1.500-2.136) | <0.001 |
| Tumor M | <0.001 | <0.001 | ||||
| M0 | Ref | Ref | ||||
| M1 | 2.190 | (2.013-2.383) | <0.001 | 2.038 | (1.793-2.317) | <0.001 |
| Marital status | <0.001 | <0.001 | ||||
| Divorced | Ref | Ref | ||||
| Single | 1.060 | (0.952-1.198) | 0.288 | 1.016 | (0.868-1.189) | 0.845 |
| Married | 0.805 | (0.805-0.953) | 0.011 | 0.797 | (0.694-0.915) | 0.001 |
| Separated | 1.221 | (0.969-1.540) | 0.091 | 1.411 | (0.990-2.011) | 0.057 |
| Windowed | 1.251 | (1.029-1.410) | <0.001 | 1.042 | (0.867-1.252) | 0.659 |
| Unmarried or Domestic partner | 0.547 | (0.272-1.101) | 0.091 | 0.572 | (0.253-1.286) | 0.177 |
| Tumor size | <0.001 | <0.001 | ||||
| ≤30 | Ref | Ref | ||||
| >30 | 1.752 | (1.617-1.899) | <0.001 | 1.657 | (1.466-1.873) | <0.001 |
| Histologic Type | 0.005 | 0.038 | ||||
| ICCs | Ref | Ref | ||||
| HCC | 1.168 | (1.060-1.287) | 0.002 | 1.2220 | (1.042-1.429) | 0.013 |
| Combined | 0.802 | (0.380-1.692) | 0.563 | 0.862 | (0.318-2.335) | 0.771 |
Prognostic nomogram for OS and ROC of the model
Based on independent prognostic factors identified in the multivariate Cox regression analysis, a prognostic nomogram was developed for liver cancer patients to predict 3-and 5-year survival probabilities (Figure 2). In primary cohorts, the area under the ROC curves (AUROCs) of the model was 0.730 (p < 0.001) (Figure 3A), the consistency index of the model was 71.56 (95%CI: 71.17-71.96), and the internal calibration curve for the probability of survival at 3-and 5-years showed a good agreement between the nomogram-predicted probability of OS and actual survival (Figure 3B, 3C). In the validation cohort, AUROCs were 0.734 (p < 0.001) (Figure 3D), the consistency index was 70.74 (95%CI: 70.13-71.35), there was also a well-performed calibration curve for survival prediction (Figure 3E, 3F). Therefore, the nomogram could reliably predict the 3- and 5-year OS probabilities. Furthermore, independent nomograms were developed for patients ≤ 55 and > 55 years of age (Supplementary Figures 3, 4).
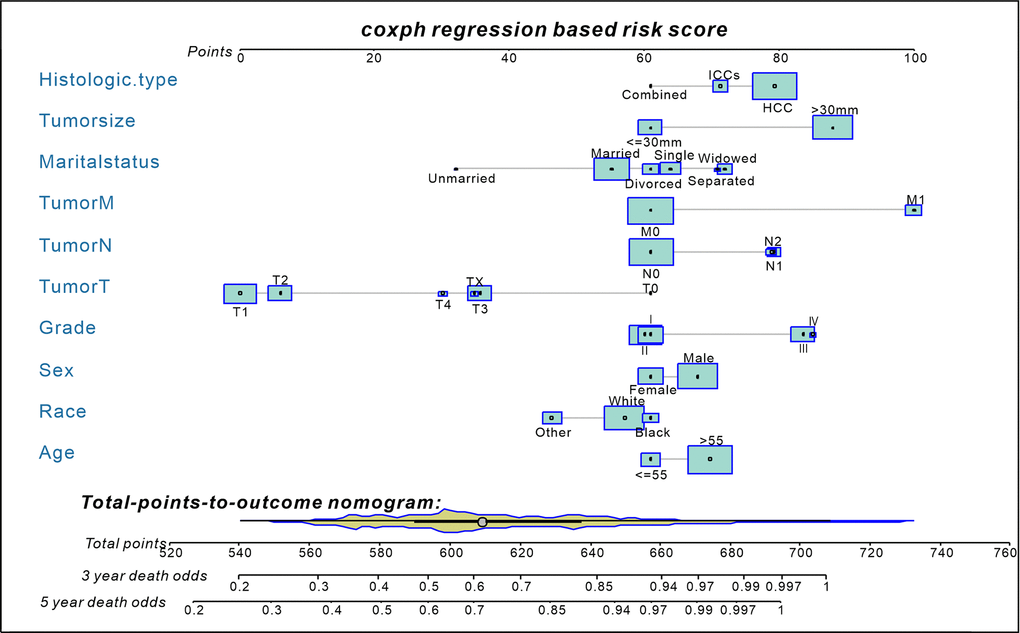
Figure 2. A nomogram for predict 3- and 5-year death odds of non-surgical liver cancer patients (established by Cox regression model). The yellow Violin Plot and the light blue box display the distribution of patients in the primary cohort. The size of the light blue box represents the proportion of patients. Abbreviations: HCC, hepatocellular carcinoma; ICCs, intrahepatic cholangiocarcinomas; Combined=HCC+ICCs.
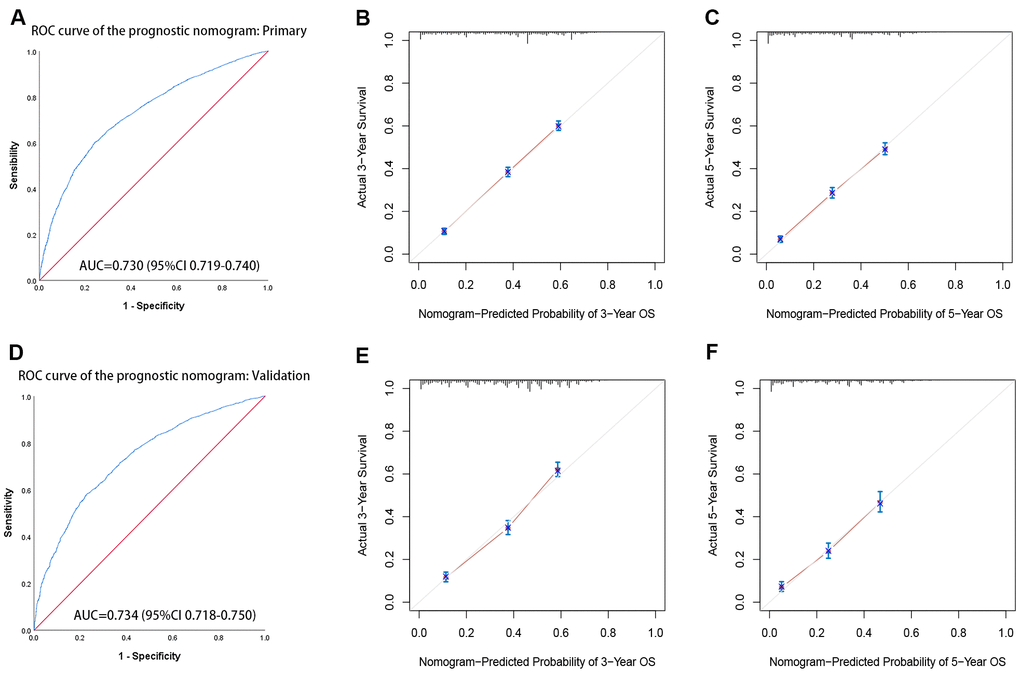
Figure 3. The receiver operating characteristic (ROC) curves and calibration curve of the prognostic nomogram. (A) ROC curves of the prognostic nomogram in the primary cohort. (B, C) The calibration curve of the nomogram-predicted probability in the primary cohort (3-year OS and 5-year OS, respectively). (D) ROC curves of the prognostic nomogram in the validation cohort. (E, F) The calibration curve of the nomogram-predicted probability in the validation cohort (3-year OS and 5-year OS, respectively). Age, sex, race, grade, tumor TNM stage, marital status, tumor size, and histological type are pooled in the primary(a) and validation(b) cohorts. AUC= area under the curve.
Survival differences according to sex and sex hormones: from bench to bedside
The primary hypothesis, that female liver cancer patients have a better prognosis than males is attributable to different estrogen levels, was investigated. Based on previous studies [5, 14, 15], 55 years of age was defined as a surrogate for menopause. As shown in Figure 1B, before menopause (i.e., ≤ 55 years of age), there was an extreme gap between females and males in survival probability (39.4 ± 1.4 vs. 32.7 ± 0.8 months, respectively; p < 0.001). While this gap will be smaller after menopause (i.e., age > 55 years), the difference between females and males (30.5 ± 0.6 vs. 29.3 ± 0.4 months, respectively; p = 0.022) (Supplementary Figure 5) persisted. For further exploration, we obtained 265 male and 139 female liver cancer patients from the TCGA database, differentially expressed genes (DEGs) and KEGG pathway analysis results showed that there were significant differences in steroid hormone biosynthesis between male and female liver cancer patients (Figure 4).
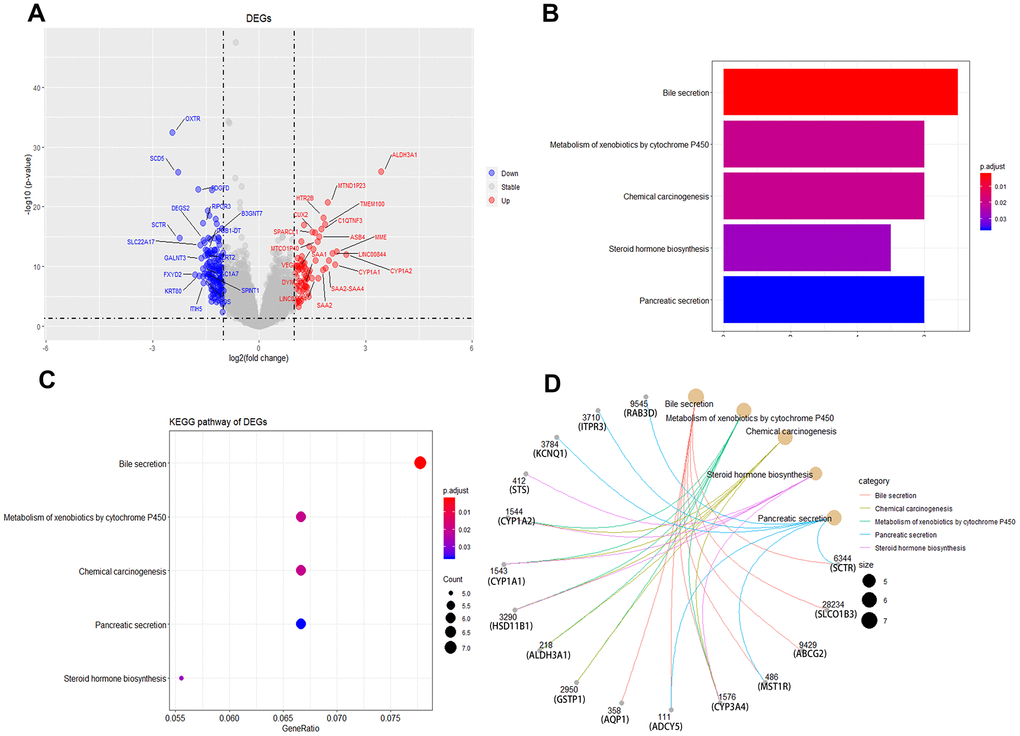
Figure 4. Identification of differentially expressed genes and KEGG enrichment between male and female liver cancer patients. (A) Volcano plot of male and female liver cancer patients in differentially expressed genes (DEGs). (B, C) KEGG enrichment of DEGs. (D) gene network diagram between DEGs and KEGG pathways.
According to a previous study [16], estradiol may be the main source of endogenous estrogen in postmenopausal women. This indicates that gender differences in patient prognosis may be primarily attributable to estrogen in patients with non-surgical liver cancer. To confirm the effect of estrogen on liver cancer, different concentrations of estrone and estradiol were used to stimulate HCC cell lines, including Hep 3B, BEL-7402, and Huh7. The results demonstrated that estradiol inhibited the proliferation of HCC cell lines and increased apoptosis; however, estrone exerted no effect (Figure 5). The most obvious effect was obtained when the concentration of estradiol is 5μmol/L. This result suggests that the difference in prognosis between men and women among liver cancer patients may be mainly attributed to estradiol.
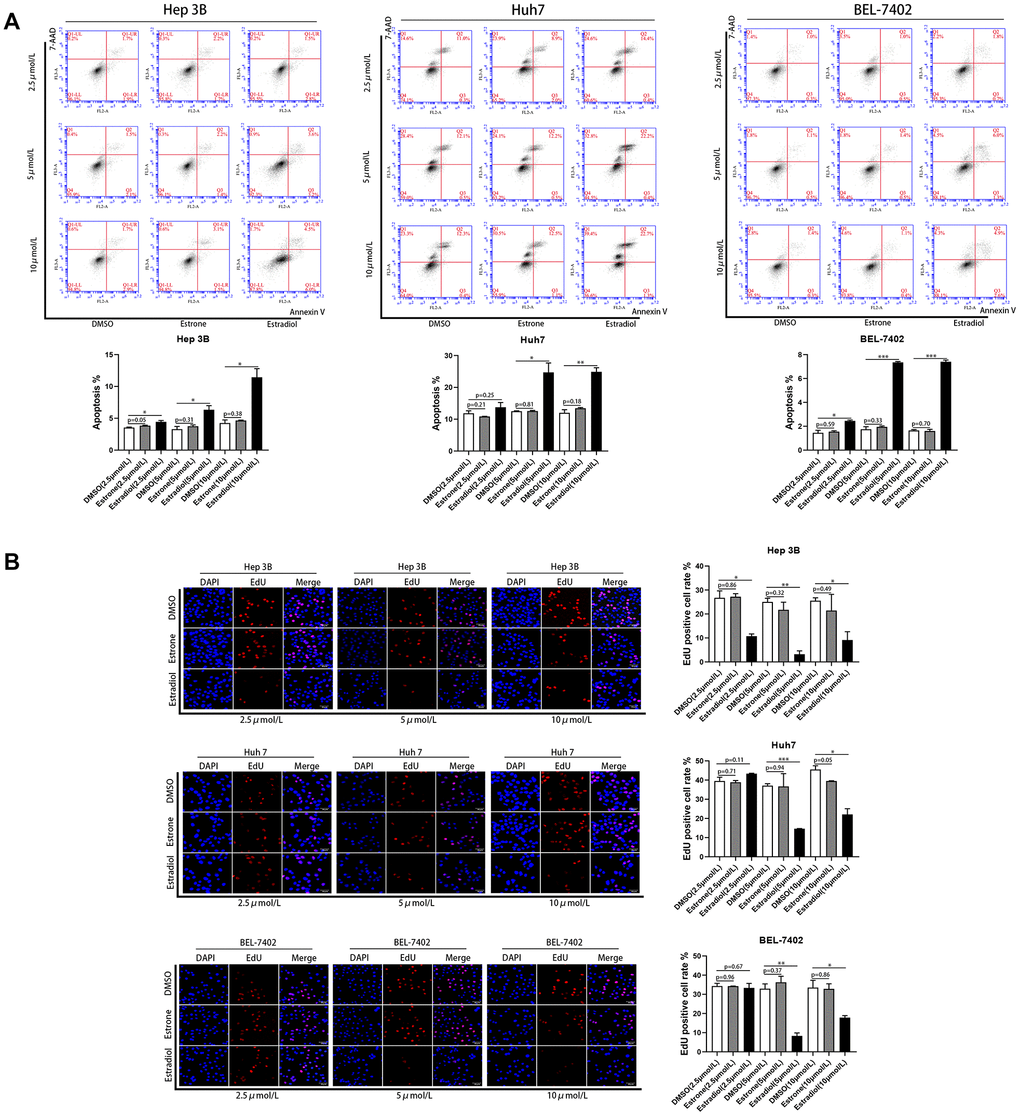
Figure 5. Estradiol inhibited the proliferation and increased the apoptosis of liver cancer cell lines. (A) Quantification of the apoptotic HCC cells population by flow cytometry. (B) Cell proliferation in HCC cells with different treatments was assessed using Cell-Light EdU Apollo 567 (catalog no· C10310-1; RiboBio). EdU positive cell rates were calculated; scale bar 50μm. Control (DMSO). *p<0.05, **p < 0·01, ***p<0·001. P < 0·05 was considered statistically significant. P values were calculated with Student's t-test.
Discussion
Although hepatic resection or liver transplantation is the optimal treatment for liver cancer [17], most patients with liver cancer are diagnosed at an intermediate-to-advanced stage when surgery is not suitable [18]. The proportion of surgical candidates is 5–10% due to multi-centric tumors, portal hypertension, vascular invasion, and dissemination [17]. Therefore, it is particularly important to design treatment plans for patients with liver cancer who cannot undergo surgery. Previous studies have hypothesized that women will benefit from estrones in liver cancer pathogenesis [11], epidemiological studies show that oophorectomy can increase the risk of liver cancer risk [19]. Interestingly, our study found that the gender differences in the prognosis of liver cancer patients always existed regardless of whether they were pre-menopausal (age ≤ 55 years) or post-menopausal (age > 55 years). Especially before menopause, there was a huge difference in survival between men and women but narrowed after menopause. Previous researches have shown that postmenopausal hormone replacement therapy is a protective factor in liver cancer [20, 21], and consistent with animal studies [20]. It means that as estrogen levels dropped, women’s benefits from hormones decreased and the dropped estrogen levels made the survival difference between men and women narrowed, and the benefits can be rescued by use postmenopausal hormone replacement therapy [20]. It reminds us that gender differences in the prognosis of liver cancer patients may be primarily attributable to estrogen [22].
In this study, meta-analysis revealed that females with liver cancer would live longer than males, which was consistent with the multivariate Cox regression analyses of the SEER database. The SEER database reported that age ≤ 55 years, white race, female sex, clinical grade 1, married status, and tumor size ≤ 30 mm were factors for a good prognosis in non-surgical liver cancer patients. We developed a prognostic nomogram for non-surgical liver cancer patients to predict 3-and 5-year OS rates, the AUROCs for this model was 0.730, and calibration curve performed well. Also, we found an extreme gap between males and females in terms of survival probability before menopause (age ≤ 55 years), and this gap persisted after menopause (age > 55 years). And we found that there was a significant difference in steroid hormone biosynthesis between male and female liver cancer patients. More importantly, we demonstrated that gender difference in the prognosis of liver cancer patients may be attributable to estradiol, but not estrone.
Previous research has suggested that men are more likely to experience liver cancer and have a worse prognosis than women [1, 2]; however, other studies have drawn contradictory conclusions [8]. Unfortunately, before our study, no meta-analysis had been performed to determine the association between sex and liver cancer risk. To confirm the influence of gender on the prognosis of liver cancer patients and eliminate bias, we analyzed previous studies and conducted a meta-analysis. The results revealed that female liver cancer patients would live longer than male patients (n = 98,010; p < 0.001). Our findings provide some epidemiological support that female liver cancer patients have a better prognosis than males with the disease.
Although some previous retrospective studies had investigated factors affecting the prognosis of liver cancer [6, 23], it is worth noting that all of them were performed using mixed cohorts of non-surgical and surgical patients, despite that is a vital factor influencing patient prognosis [13]. To eliminate confounding by surgery, we conducted a retrospective study using data from 12,312 liver cancer patients who had not undergone surgery between 2010 and 2015 from the SEER database. Multivariate Cox analysis revealed that under non-surgical conditions, the prognosis of female liver cancer patients is still better than that of males, which was consistent with the results of the meta-analysis. It is the largest retrospective study of non-surgical liver cancer patients, to our knowledge. Therefore, we can be relatively certain that gender has an impact on the prognosis of liver cancer patients and, perhaps, resolve the dispute in this regard.
We found that higher TNM stage and clinical-grade were associated with poor survival in liver cancer patients, as reported previously [24]. Tumor size remains an independent prognostic factor for liver cancer, and these results confirmed that patients with small HCC are essentially a heterogeneous group [25]. Among patients with liver cancer, those with white race have a better prognosis, consistent with the study by Zhang et al. [25]. Age, marital status, and histological type were all independent risk factors.
Nomograms have been widely used for cancer prognosis and displayed more accurate than conventional staging systems in the aspect of predicting prognosis in some cancers [26, 27]. Therefore, we conducted a prognostic nomogram for patients who had not undergone surgery. It is worth noting that this model had the most comprehensive index to predict the survival probability of non-surgical liver cancer patients at 3 and 5 years. The nomogram performed well, and its prediction was supported by the AUROCs (0.730 and 0.734 for the primary and validation cohorts, respectively). It was consistent with the observations by Zhang et al. [8], but they had too little data to find more valuable information.
Previous study supposed that estradiol is the main source of endogenous estrogen in postmenopausal women [16]. Whether the gender differences in the prognosis of liver cancer are attributable to estrogen still has not been resolved clearly. Unfortunately, previous studies focused only on the superficial aspects of retrospective research. But in our study, we used meta-analysis, cohort research, in vitro experiments, etc. to confirm our results. We proved that estradiol may, in large part, explain gender differences in the prognosis of liver cancer patients, and demonstrated that estradiol—but not estrone—inhibited the development of liver cancer, from bench to bedside. Because estradiol can inhibit tumor growth and increase tumor cell apoptosis rate, so as a protective factor, women may benefit from estradiol [28] and got longer survival than men. Our research provides the possibility of using hormone replacement therapy for liver cancer patients, which is supported by Zhong et al. [10] and McGlynn KA et. al [29].
In conclusion, we determined that gender differences in prognosis of liver cancer patients and the effect of sex hormones on the disease by used meta-analysis, retrospective analysis, and in vitro experiments. More importantly, we demonstrated that estradiol inhibited the proliferation of HCC cell lines and increased apoptosis, but estrone exerted no effect. This may explain why there was a gender difference in the prognosis of liver cancer patients. Future investigations should aim to elucidate the mechanisms of action of estradiol in those with liver cancer.
Materials and Methods
Search strategy and selection criteria
A literature search of the PubMed database, performed using a combination of the keywords ((gender OR sex) AND “Marital status” AND race AND (cancer OR tumor)), retrieved a total of 424 relevant studies. After reviewing abstracts, 337 articles were excluded, and 87 tumor-related articles were used to verify the relationship between gender and tumor prognosis. Among these, 7 studies investigating liver cancer were retained, and one addressed liver transplantation. Ultimately, 6 studies were used to identify and appraise the effect of sex on overall survival (OS) in patients with liver cancer.
Data sources and patient selection
The Surveillance, Epidemiology, and End Results (SEER) Program provides information regarding cancer statistics of the United States. SEER is supported by the Surveillance Research Program (SRP) in the National Cancer Institute’s Division of Cancer Control and Population Sciences (DCCPS) (https://seer.cancer.gov/). Data were based on Incidence-SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases (1973-2015), among which 123,806 liver cancer patients were screened. Excluding operable (n = 7188) and unknown (n = 118,682) liver cancer patients, data from 12,312 non-surgical liver cancer patients were analyzed using SEER*Stat software. 265 male and 139 female liver cancer patients were obtained from the TCGA database for differentially expressed genes (DEGs) and KEGG pathway analysis.
In vitro experiments
The HCC cell lines Huh 7, Hep 3B, and BEL-7402 were maintained at 37° C in a humidified incubator with a 5% CO2 atmosphere. After treatment with different concentrations of estrone, estradiol, and dimethyl-sulfoxide (as control) for 24 h, cell apoptosis and proliferation experiments were conducted. Apoptosis experiments were performed as previously described [30], and flow cytometry was performed using a commercially available kit (Annexin V PE apoptosis kit, BD Biosciences, San Jose, CA, USA). Cell proliferation was assessed using Cell-Light EdU Apollo 567 (catalog no. C10310-1; RiboBio, China), as previously described [31].
Statistical analyses
Statistical analyses were conducted using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA), GraphPad Prism 8 (GraphPad Inc, San Diego, CA, USA) and the package of meta, ggplot, survival, and rms of R version 3.6.1.
Meta-analysis was performed using the package meta in R. The 95% confidence intervals (CI) reported in the available articles were extracted and pooled after calculating TE, seTE, and log transformed. Study heterogeneity was assessed using the I2 statistic [32]. Survival curves for both the genders were plotted using the Kaplan-Meier method by R. Univariate and multivariate Cox regression analyses were used to estimate independent risk factors in non-surgical liver cancer patients on OS and to generate hazard ratios (HR) and corresponding 95% CI in SPSS version 25. All results were verified in the validation cohort. A prognostic nomogram was developed based on multivariate Cox regression analyses. The receiver operating characteristic (ROC) curve was plotted using SPSS version 25. All statistical tests were two-tailed and differences with p < 0.05 were considered as statistically significant.
Supplementary Materials
Author Contributions
Rangrang Wang, Yuan Liu, Hongze Sun, Junwei Fan, Zhaowen Wang conceived and designed the research study; Rangrang Wang, Yuan Liu, Hongze Sun, Tao Wang, Changcan Li analyzed the data and conducted the related experiments. Rangrang Wang, Hongze Sun, Yuan Liu, Tao Wang, Junwei Fan, Zhaowen Wang wrote and revised the manuscript. Rangrang Wang, Yuan Liu, Hongze Sun, and Tao Wang contributed equally to this study. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
This study was supported by National Natural Science Foundation of China (U1604282), the project of Shanghai Jiao Tong University School of Medicine (YG2017MS23), and the project of Shanghai General Hospital (CTCCR-2018BP01).
References
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. https://doi.org/10.3322/caac.21492 [PubMed]
- 2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020; 70:7–30. https://doi.org/10.3322/caac.21590 [PubMed]
- 3. Petrick JL, Florio AA, Zhang X, Zeleniuch-Jacquotte A, Wactawski-Wende J, Van Den Eeden SK, Stanczyk FZ, Simon TG, Sinha R, Sesso HD, Schairer C, Rosenberg L, Rohan TE, et al. Associations Between Prediagnostic Concentrations of Circulating Sex Steroid Hormones and Liver Cancer Among Postmenopausal Women. Hepatology. 2020; 72:535–547. https://doi.org/10.1002/hep.31057 [PubMed]
- 4. Zhao HY, Gong Y, Ye FG, Ling H, Hu X. Incidence and prognostic factors of patients with synchronous liver metastases upon initial diagnosis of breast cancer: a population-based study. Cancer Manag Res. 2018; 10:5937–50. https://doi.org/10.2147/CMAR.S178395 [PubMed]
- 5. Yang D, Hanna DL, Usher J, LoCoco J, Chaudhari P, Lenz HJ, Setiawan VW, El-Khoueiry A. Impact of sex on the survival of patients with hepatocellular carcinoma: a surveillance, epidemiology, and end results analysis. Cancer. 2014; 120:3707–16. https://doi.org/10.1002/cncr.28912 [PubMed]
- 6. Xiao Z, Yan Y, Zhou Q, Liu H, Huang P, Zhou Q, Lai C, Zhang J, Wang J, Mao K. Development and external validation of prognostic nomograms in hepatocellular carcinoma patients: a population based study. Cancer Manag Res. 2019; 11:2691–708. https://doi.org/10.2147/CMAR.S191287 [PubMed]
- 7. Wu W, Fang D, Shi D, Bian X, Li L. Effects of marital status on survival of hepatocellular carcinoma by race/ethnicity and gender. Cancer Manag Res. 2018; 10:23–32. https://doi.org/10.2147/CMAR.S142019 [PubMed]
- 8. Zhang L, Yan L, Niu H, Ma J, Yuan BY, Chen YH, Zhuang Y, Hu Y, Zeng ZC, Xiang ZL. A nomogram to predict prognosis of patients with unresected hepatocellular carcinoma undergoing radiotherapy: a population-based study. J Cancer. 2019; 10:4564–73. https://doi.org/10.7150/jca.30365 [PubMed]
- 9. Joshi S, Song YM, Kim TH, Cho SI. Socio-economic status and the risk of liver cancer mortality: a prospective study in Korean men. Public Health. 2008; 122:1144–51. https://doi.org/10.1016/j.puhe.2008.04.003 [PubMed]
- 10. Zhong GC, Liu Y, Chen N, Hao FB, Wang K, Cheng JH, Gong JP, Ding X. Reproductive factors, menopausal hormone therapies and primary liver cancer risk: a systematic review and dose-response meta-analysis of observational studies. Hum Reprod Update. 2016; 23:126–38. https://doi.org/10.1093/humupd/dmw037 [PubMed]
- 11. Zheng B, Zhu YJ, Wang HY, Chen L. Gender disparity in hepatocellular carcinoma (HCC): multiple underlying mechanisms. Sci China Life Sci. 2017; 60:575–84. https://doi.org/10.1007/s11427-016-9043-9 [PubMed]
- 12. Liu WC, Liu QY. Molecular mechanisms of gender disparity in hepatitis B virus-associated hepatocellular carcinoma. World J Gastroenterol. 2014; 20:6252–61. https://doi.org/10.3748/wjg.v20.i20.6252 [PubMed]
- 13. Cotton RT, Tran Cao HS, Rana AA, Sada YH, Axelrod DA, Goss JA, Wilson MA, Curley SA, Massarweh NN. Impact of the treating hospital on care outcomes for hepatocellular carcinoma. Hepatology. 2018; 68:1879–89. https://doi.org/10.1002/hep.30128 [PubMed]
- 14. Bohanes P, Yang D, Chhibar RS, Labonte MJ, Winder T, Ning Y, Gerger A, Benhaim L, Paez D, Wakatsuki T, Loupakis F, El-Khoueiry R, Zhang W, Lenz HJ. Influence of sex on the survival of patients with esophageal cancer. J Clin Oncol. 2012; 30:2265–72. https://doi.org/10.1200/JCO.2011.38.8751 [PubMed]
- 15. Hendifar A, Yang D, Lenz F, Lurje G, Pohl A, Lenz C, Ning Y, Zhang W, Lenz HJ. Gender disparities in metastatic colorectal cancer survival. Clin Cancer Res. 2009; 15:6391–97. https://doi.org/10.1158/1078-0432.CCR-09-0877 [PubMed]
- 16. Liu J, Flockhart PJ, Lu D, Lv W, Lu WJ, Han X, Cushman M, Flockhart DA. Inhibition of cytochrome p450 enzymes by the e- and z-isomers of norendoxifen. Drug Metab Dispos. 2013; 41:1715–20. https://doi.org/10.1124/dmd.113.052506 [PubMed]
- 17. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018; 391:1301–14. https://doi.org/10.1016/S0140-6736(18)30010-2 [PubMed]
- 18. Huo YR, Eslick GD. Transcatheter arterial chemoembolization plus radiotherapy compared with chemoembolization alone for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Oncol. 2015; 1:756–65. https://doi.org/10.1001/jamaoncol.2015.2189 [PubMed]
- 19. McGlynn KA, Sahasrabuddhe VV, Campbell PT, Graubard BI, Chen J, Schwartz LM, Petrick JL, Alavanja MC, Andreotti G, Boggs DA, Buring JE, Chan AT, Freedman ND, et al. Reproductive factors, exogenous hormone use and risk of hepatocellular carcinoma among US women: results from the Liver Cancer Pooling Project. Br J Cancer. 2015; 112:1266–72. https://doi.org/10.1038/bjc.2015.58 [PubMed]
- 20. Yeh SH, Chen PJ. Gender disparity of hepatocellular carcinoma: the roles of sex hormones. Oncology. 2010 (Suppl 1); 78:172–79. https://doi.org/10.1159/000315247 [PubMed]
- 21. Yu MW, Chang HC, Chang SC, Liaw YF, Lin SM, Liu CJ, Lee SD, Lin CL, Chen PJ, Lin SC, Chen CJ. Role of reproductive factors in hepatocellular carcinoma: impact on hepatitis B- and C-related risk. Hepatology. 2003; 38:1393–400. https://doi.org/10.1016/j.hep.2003.09.041 [PubMed]
- 22. Xu H, Wei Y, Zhang Y, Xu Y, Li F, Liu J, Zhang W, Han X, Tan R, Shen P. Oestrogen attenuates tumour progression in hepatocellular carcinoma. J Pathol. 2012; 228:216–29. https://doi.org/10.1002/path.4009 [PubMed]
- 23. Robbins AS, Daily MF, Aoki CA, Chen MS
Jr , Troppmann C, Perez RV. Decreasing disparity in liver transplantation among white and Asian patients with hepatocellular carcinoma : california, 1998-2005. Cancer. 2008; 113:2173–79. https://doi.org/10.1002/cncr.23766 [PubMed] - 24. Lai HC, Lee MS, Lin C, Lin KT, Huang YH, Wong CS, Chan SM, Wu ZF. Propofol-based total intravenous anaesthesia is associated with better survival than desflurane anaesthesia in hepatectomy for hepatocellular carcinoma: a retrospective cohort study. Br J Anaesth. 2019; 123:151–60. https://doi.org/10.1016/j.bja.2019.04.057 [PubMed]
- 25. Zhang W, Wang X, Jiang R, Hou J, Mu X, Li G, Sun B. Effect of tumor size on cancer-specific survival in small hepatocellular carcinoma. Mayo Clin Proc. 2015; 90:1187–95. https://doi.org/10.1016/j.mayocp.2015.06.018 [PubMed]
- 26. Wang Y, Li J, Xia Y, Gong R, Wang K, Yan Z, Wan X, Liu G, Wu D, Shi L, Lau W, Wu M, Shen F. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin Oncol. 2013; 31:1188–95. https://doi.org/10.1200/JCO.2012.41.5984 [PubMed]
- 27. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008; 26:1364–70. https://doi.org/10.1200/JCO.2007.12.9791 [PubMed]
- 28. Naugler WE, Sakurai T, Kim S, Maeda S, Kim K, Elsharkawy AM, Karin M. Gender disparity in liver cancer due to sex differences in MyD88-dependent IL-6 production. Science. 2007; 317:121–24. https://doi.org/10.1126/science.1140485 [PubMed]
- 29. McGlynn KA, Hagberg K, Chen J, Braunlin M, Graubard BI, Suneja N, Jick S, Sahasrabuddhe VV. Menopausal hormone therapy use and risk of primary liver cancer in the clinical practice research datalink. Int J Cancer. 2016; 138:2146–53. https://doi.org/10.1002/ijc.29960 [PubMed]
- 30. Sun H, Ou B, Zhao S, Liu X, Song L, Liu X, Wang R, Peng Z. USP11 promotes growth and metastasis of colorectal cancer via PPP1CA-mediated activation of ERK/MAPK signaling pathway. EBioMedicine. 2019; 48:236–47. https://doi.org/10.1016/j.ebiom.2019.08.061 [PubMed]
- 31. Xu Q, Xiang Y, Wang Q, Wang L, Brind’Amour J, Bogutz AB, Zhang Y, Zhang B, Yu G, Xia W, Du Z, Huang C, Ma J, et al. SETD2 regulates the maternal epigenome, genomic imprinting and embryonic development. Nat Genet. 2019; 51:844–56. https://doi.org/10.1038/s41588-019-0398-7 [PubMed]
- 32. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557–60. https://doi.org/10.1136/bmj.327.7414.557 [PubMed]