



Introduction
Coronary atherosclerotic heart disease (CHD) remains a major cause of global death [1, 2]. Currently in China, only about 0.2% of adults can be said to be in ideal cardiovascular health, and there are 11 million patients with CHD, which remains the second leading cause of premature death [3–5]. Although attention has been paid to alleviating the burden of CHD, efforts have focused primarily on treatment of the disease, not its prevention [6, 7]. Consequently, there is a tremendous opportunity to a shift to equal emphasis on intervention and prevention of CHD.
To formulate and optimize preventive strategies for CHD, it is essential to understand and appropriately quantify the contributions of its key risk factors. Evaluating and managing risk factors for CHD can be complex, however, as they include biological, behavioral and psychological factors [8–10]. According to Framingham study, it is estimated that over 90% of CHD events occur in persons with at least one high-risk factor (hypertension, hyperlipidemia, smoking, etc.) [11]. In addition, studies have revealed that lowering the systolic blood pressure and lipoprotein cholesterol, stopping smoking, maintaining a healthy weight, exercising, and eating a healthy diet are all associated with lower CHD risk [12–17]. Recently, the relationship between psychological stress (stressful life events, depression and demoralization) and CHD has begun to attract attention [18–21]. However, few studies have assessed the various influencing factors at the same time, making it difficult to estimate the risk of CHD poses by combinations of various types of influencing factors.
In addition, the nomogram is undergoing a resurgence as a visualization tool for disease prevention [22–24]. However, there have been few studies combining biological, behavioral, and psychological factors to establish nomograms with which to assess the risk of CHD, especially in China.
To address this knowledge gap, we performed a case-control study in southeast China. The specific goal of this study was to cover a broad spectrum of biological, behavioral and psychological factors in order to identify those that show significant associations with CHD and to clarify the comprehensive predictive value of CHD risk. The next objective, then, was to develop a nomogram with which to estimate the probability of CHD in those with risk factors.
Results
Baseline characteristics and risk factors of CHD
Among the 4392 participants in this study, 1,578 (35.9%) suffered from CHD. The biological characteristics of cases and controls are shown in Tables 1 and 2. At baseline, patients with CHD showed were significantly older; had a higher education level; higher body mass index (BMI), waist hip ratio (WHR) and waist to height ratio (WHtR); were most likely male with family history of diabetes, CHD and stroke; and had hypertension, hyperlipidemia and/or diabetes.
Table 1. Baseline characteristics of the analyzed participants.
| Variables | Non-CHD, n(%) | CHD, n(%) | χ2 | *P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | Female | 1478(52.5) | 591(37.5) | 92.161 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 1336(47.5) | 987(62.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | ≤65 | 1662(59.1) | 689(43.7) | 96.379 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >65 | 1152(40.9) | 889(56.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Marital status | Marriage | 2529 (89.9) | 1404(89) | 0.873 | 0.350 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single and others | 285(10.1) | 174(11) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education years | ≤6 | 1371(48.7) | 721(45.7) | 7.408 | 0.025 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7-12 | 1188(42.2) | 678(43.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >12 | 255(9.1) | 179(11.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *The P value was calculated by the Chi-square test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CHD, coronary atherosclerotic heart disease. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. Family history, clinical disease, and physical characteristics of the participants.
| Variables | Non-CHD, n(%) | CHD, n(%) | χ2 | *P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Family history | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | Yes | 1106(39.3) | 658(41.7) | 2.413 | 0.120 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes | Yes | 456(16.2) | 311(19.7) | 8.611 | 0.003 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CHD | Yes | 392(13.9) | 315(20.0) | 27.234 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stroke | Yes | 283(10.1) | 212(13.4) | 11.536 | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical diseases | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | Yes | 1459 (51.8) | 1188 (75.3) | 231.931 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperlipidemia | Yes | 462 (16.4) | 400 (25.3) | 51.118 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes | Yes | 384 (13.6) | 434 (27.5) | 128.095 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical characteristics | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body mass index | < 18.50 | 138 (4.9) | 48 (3.0) | 19.706 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18.50–23.99 | 1371 (48.7) | 709 (44.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 24-27.99 | 1026 (36.5) | 626 (39.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 28.00 | 279 (9.9) | 195 (12.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist hip ratio | Normal | 576 (20.5) | 262 (16.6) | 9.786 | 0.002 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abdominal obesity | 2238 (79.5) | 1316 (83.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist to height ratio | <0.5 | 590 (21.0) | 279 (17.6) | 7.153 | 0.007 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥0.5 | 2224 (79.0) | 1300 (82.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *The P value was calculated by the Chi-square test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CHD, coronary atherosclerotic heart disease. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The behavioral characteristics of the two groups are provided in Table 3. Smoking and a high-salt diet were related to high risk of CHD. In addition, the frequency of tea drinking and the type of edible oil consumed correlated significantly correlation with CHD.
Table 3. Behavioral variables of the participants.
| Variables | Non-CHD, n(%) | CHD, n(%) | χ2 | *P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pack-year Smoking | No | 1982(70.4) | 954 (60.5) | 66.984 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0-20 | 266 (9.5) | 144 (9.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 20-40 | 367 (13.0) | 275 (17.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >40 | 199 (7.1) | 205 (13.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcohol drinking | No | 2378 (84.5) | 1289 (81.7) | 5.859 | 0.053 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <3 time/week | 156 (5.5) | 105 (6.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥3 time/week | 280 (10.0) | 184 (11.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tea drinking | No | 1790 (63.6) | 944 (59.8) | 8.582 | 0.014 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <3 time/week | 282 (10.0) | 153 (9.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥3 time/week | 742 (26.4) | 481 (30.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical exercise | No | 952 (33.8) | 527 (33.4) | 4.347 | 0.226 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <3 time/week | 393 (14.0) | 194 (12.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥3 time/week | 1469 (52.2) | 857 (54.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Food intake | Eight full | 1982 (70.4) | 1069 (67.7) | 3.887 | 0.274 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Less | 233 (8.3) | 151 (9.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Full | 486 (17.3) | 290 (18.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not fixed | 113 (4.0) | 68 (4.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Edible oils | Vegetable oil | 2444 (86.8) | 1419 (89.9) | 17.537 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Animal oil | 78 (2.8) | 16 (1.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Animal and vegetable | 292 (10.4) | 143 (9.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High-salt diet | No | 2003 (71.2) | 1059 (67.1) | 7.931 | 0.005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 811 (28.8) | 519 (32.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vegetable | <1 day/week | 30 (2.4) | 21 (2.9) | 4.978 | 0.173 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1-2 day/week | 58 (4.7) | 44 (6.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3-4 day/week | 80 (6.5) | 33 (4.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥5 day/week | 1068 (86.4) | 626 (86.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fruit | <1 day/week | 271 (22.0) | 179 (24.8) | 2.788 | 0.426 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1-2 day/week | 341 (27.7) | 200 (27.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3-4 day/week | 138 (11.2) | 83 (11.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥5 day/week | 481 (39.1) | 259 (35.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fried food | <1 day/week | 878 (75.0) | 519 (74.7) | 0.753 | 0.861 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1-2 day/week | 223 (19.0) | 139 (20.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3-4 day/week | 48 (4.1) | 27 (3.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥5 day/week | 22 (1.9) | 10 (1.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fat meat | <1 day/week | 814 (70.8) | 483 (69.2) | 6.840 | 0.077 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1-2 day/week | 209 (18.2) | 154 (22.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3-4 day/week | 91 (7.9) | 39 (5.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥5 day/week | 36 (3.1) | 22 (3.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Video duration | <1h/day | 217 (21.6) | 103 (17.0) | 5.868 | 0.053 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1-3h/day | 522 (52.0) | 321 (53.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >3h/day | 264 (26.4) | 181 (29.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep duration | 7-8h//day | 480 (39.5) | 262 (36.6) | 3.028 | 0.220 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <7h//day | 577 (47.5) | 369 (51.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >8h//day | 159 (13.1) | 85 (11.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sleep quality | General | 267 (21.7) | 159 (22.0) | 1.416 | 0.493 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Poor | 373 (30.3) | 201 (27.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Good | 590 (48.0) | 362 (50.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *The P value was calculated by the Chi-square test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CHD, coronary atherosclerotic heart disease. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The psychological features of cases and controls listed in Table 4 indicate that people who have recently experienced major events and/or had depression or anxiety were prone to CHD.
Table 4. Psychological variables of the participants.
| Variables | Non-CHD, n(%) | CHD, n(%) | χ2 | *P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Major events encountering | No | 2272 (80.7) | 1226 (77.7) | 5.786 | 0.016 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 542 (19.3) | 352 (22.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Life satisfaction | General | 889 (31.6) | 482 (30.5) | 2.738 | 0.434 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dissatisfied | 83 (2.9) | 45 (2.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Satisfied | 1842 (65.5) | 1051 (66.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Character type | A type | 1045 (37.1) | 621 (39.4) | 0.589 | 0.745 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| B type | 1574 (55.9) | 842 (53.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| C type | 146 (5.2) | 87 (5.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| D type | 49 (1.7) | 28 (1.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Depression | No | 1095 (69.9) | 547 (64.3) | 7.940 | 0.005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 472 (30.1) | 304 (35.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anxiety | No | 1296 (82.7) | 627 (73.7) | 27.608 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 271 (17.3) | 224 (26.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *The P value was calculated by the Chi-square test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CHD, coronary atherosclerotic heart disease. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Development and validation of a CHD-predictive nomogram
According to the “Backwald: Wald” logistic regression model, after excluding variables with P-values >0.05, eight predictors were associated with CHD: sex, age, family history of CHD, hypertension, hyperlipidemia, diabetes, encounters with major events, and anxiety (Figure 1). The results from logistic regression analyses were then used to construct a nomogram to predict the probability of CHD (Figure 2). To estimate the risk of CHD, the observed value of each predictor was assigned a certain number of points by drawing a vertical line towards the top points scale. The sum of the points for each variable corresponded to the individual risk of developing CHD.
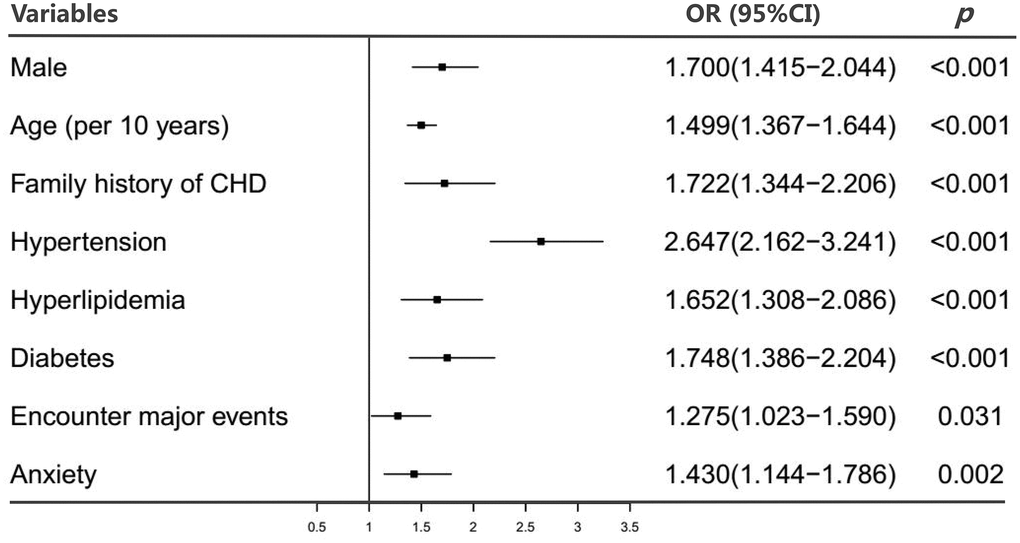
Figure 1. Estimated odds ratios determined in a logistic regression model (Backwald: Wald). Abbreviations: OR, odds ratio; CI, confidence interval.
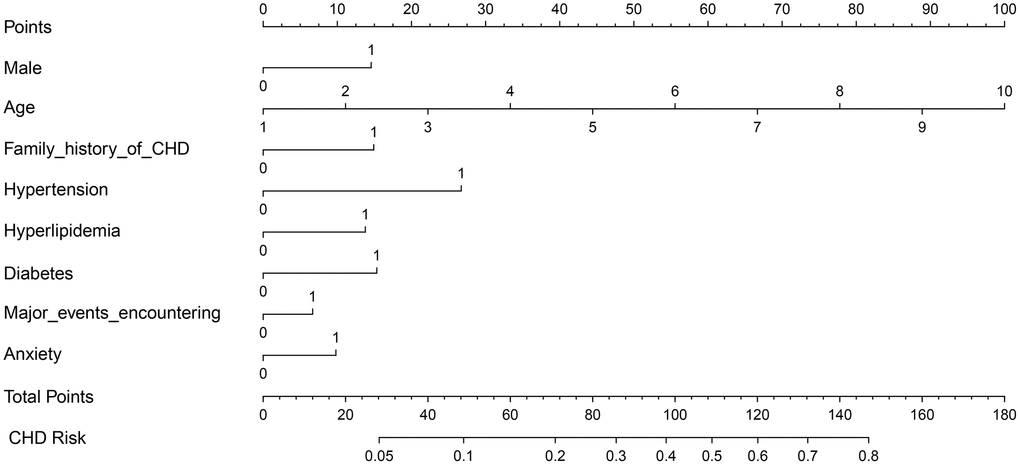
Figure 2. Nomogram for predicting CHD risk. The value of each variable was scored on a point scale from 0 to 100, after which the scores for each variable were added together. That sum is located on the total points axis, which enables us to predict the probability of CHD risk. For age categories, 1= 10 to 20, 2 = 21 to 30, 3 = 31 to 40, 4 = 41 to 50, 5 = 51 to 60, 6 = 61 to 70, 7 = 71 to 80, 8 = 81 to 90, 9 = 91 to 100, 10 = 101 to 110 year. For other variables, 0 = no and 1 = yes.
We next divided the total points into four subgroups by quartile. Figure 3 shows that the risk of CHD increased with the total points, and participants in quartile four (total points: 107.93-154.78) had a higher CHD risk than those in the lower quartiles (odds ratio [OR]: 8.917, 95% confidence interval [CI]: 6.734-11.809).
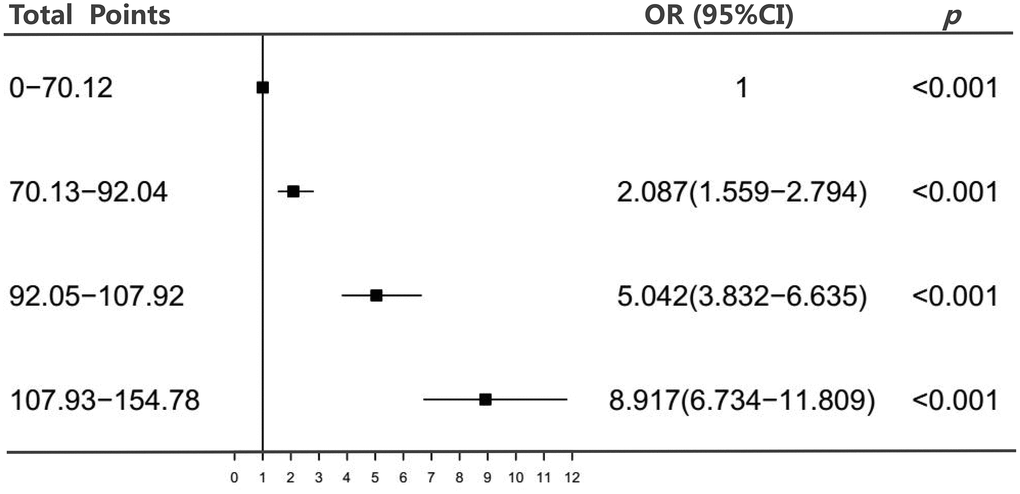
Figure 3. Association between the total points of the nomogram and CHD. Abbreviations: OR, odds ratio; CI, confidence interval.
Finally, we verified the accuracy of the nomogram. Using a bootstrap method with 500 resamples, the area under curve (AUC) for the nomogram was determined to be 0.726 (95%CI = 0.709-0.747) (Figure 4A). Among them, the AUC value of the non-modifiable variables (sex, age and family history of CHD) was 0.649 (95% CI: 0.630-0.668), and the modifiable variables (hypertension, hyperlipidemia, diabetes, encounters with major events, and anxiety) was 0.681 (95% CI: 0.662-0.700). The analysis showed that the AUC value of the modifiable variables was higher than that of the non-modifiable variables (Z = 2.053, P = 0.040). In addition, the probabilities predicted by the nomogram matched well with the clinical outcomes (Figure 4B), and the decision curve shows that the model has potential clinical application value (Figure 4C).
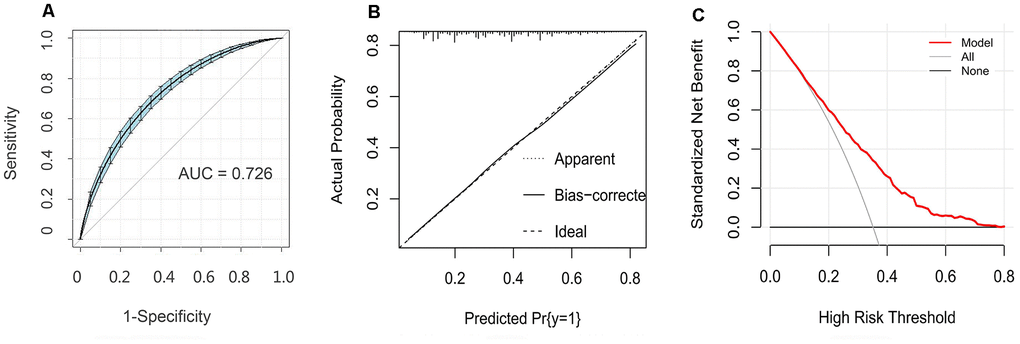
Figure 4. Evaluation of the nomogram model. (A) Receiver operating characteristic curve for the nomogram generated using bootstrap resampling (500 times). (B) Nomogram calibration plot. When the solid line (performance nomogram) was closer to the dotted line (ideal model), the prediction accuracy of the nomogram was better. (C) Decision curve analysis for the prediction model. The red solid line is from the prediction model, the gray line is for all patients with CHD, and the solid horizontal line indicates no patients have CHD. The graph depicts the expected net benefit per patient relative to the nomogram prediction of CHD risk. The net benefit increases as the model curve is extended.
Discussion
Key findings
In this retrospective study, our results illustrated the significant contributions of sex, age, family history of CHD, hypertension, hyperlipidemia, diabetes, recent major events, and anxiety to the risk of CHD. Using these variables, a nomogram to assess the risk of CHD was established and validated, which we suggest is of potentially great significance for the primary prevention of CHD.
Comparison with other studies
In contrast to earlier studies, which focused on specific factors associated with CHD [11–17], we combined biological, behavioral and psychological factors, and found that the aforementioned eight variables associated with high CHD risk. Among those, were three non-modifiable factors (sex, age and family history), which is in good agreement with earlier reports [25, 26]. In addition, hypertension, dyslipidemia and diabetes are also well-established risk factors for CHD [27–29]. Our findings are consistent with the earlier findings, but extend their scope by providing data on psychological factors. We reported an OR of 1.430 (95%CI: 1.144-1.789) for relation between anxiety and CHD risk, which is consistent with previous studies [30, 31]. We also found that people who have recently experienced major events that cause traumatic stress are prone to CHD. The causal pathways between the physiological responses to psychological stress involving two regulatory axes (hypothalamic-pituitary-adrenocortical and sympatho-adrenomedullary axes) are well established, but its association with the progression of CHD remains unclear [32]. One possible mechanism by which psychological stress leads to CHD may be that the resultant imbalance between sympathetic and parasympathetic activity causes hypertension and tachycardia leading to CHD [33].
A study similar to this one also found that changes in biological, behavioral and psychosocial factors could alter the CHD five-year risk [34]. That study recruited 35- to 55-year-old office workers from 20 London-based civil service departments between 1985 to 1988. Research factors were limited to six risk factors (cholesterol level, hypertension, smoking, overweight, psychological disturbance and relationship problems), with age, sex, race, marital status and other factors as covariates. By contrast, our study was conducted in China, the participants' ages included those over 55, involved multiple occupations, included thirty-three biological, behavioral and physiological variables, and assessed these at the same time. Our study is thus a more suitable reflection of the situation of Chinese people, irrespective of their age or occupation, and can simultaneously assess the biological, behavioral and physiological factors contributing to CHD risk.
Implications for clinicians and policymakers
A well-validated tool for predicting disease risk is important for appropriate clinical care, especially for primary prevention [35]. As part of the advances made in CHD prevention and management, the Framingham prediction algorithm has been widely used to estimate CHD risk [36, 37]. However, in some populations, including the Chinese, this algorithm would overestimate the risk of CHD [38–41]. This highlights the need to establish an effective CHD risk assessment tool in China. In addition, several recent studies used nomograms to evaluate CHD risk based on the results of various tests, including coronary computed tomography angiography, carotid ultrasound, and coronary artery calcium scoring [42–44]. These studies provided strong clinical evidence for diagnosis, but were useless for identification and evaluation of the factors that can alter CHD risk, which is more important for primary prevention. Our study, carried out in southeast China, identified five modifiable variables (hypertension, hyperlipidemia, diabetes, recent experience of major events, and anxiety) based on a logistic regression model and constructed a nomogram risk prediction model for practical application. The validation results for the nomogram show that the model has good predictive ability and clinical application value. As these factors are readily available, our risk assessment model could potentially be widely accepted.
Strengths and limitations
A key strength of this study was our ability to simultaneously evaluate an wide range of predictors, including biological, behavioral and psychological factors. In addition, previous studies have confirmed that substantial mitigation of CHD prevention could be achieved in clinical practice through improvements in modifiable risk factors [45, 46]. We have created an easy-to-use nomogram in China that includes five modifiable variables, which are especially important for the prevention of CHD in China. Moreover, for non-modifiable variables, it is also beneficial for the public to be aware of CHD risk. That knowledge provides the public with the opportunity to voluntarily enhance early screening and promote secondary prevention. Consequently, the combination of modifiable variables and non-modifiable variables is more conducive to the prevention of CHD. Finally, our model included psychological factors, suggesting that psychological factors may not be ignored in the construction of risk models. Our research hopes to bring new hints to future model building, that is, psychological factors can be considered in constructing CHD risk assessment models based on prospective studies.
However, interpretation of these findings has three important caveats. First, like previous retrospective case-control studies, causal inference is limited. Consequently, our results and conclusions can only be used to assess the risk of CHD in the general population, and should be validated by strictly designed subsequent cohort studies. In addition, biological, behavioral and psychological factors are numerous. Although we took thirty-three variables into account, that does not cover everything. Future studies with broader variables are needed to further validate the findings of our study. Finally, this was a single-center study of only Chinese patients from a single region, which may limit its generalizability. Although our nomogram was validated using bootstraps with 500 resamples, future prospective multicenter studies are still needed to externally validate our results.
Conclusions
This analysis shows that being male and/or elderly, having a family history of CHD, hypertension, hyperlipidemia, diabetes, recent experience of major traumatic events, and anxiety are associated with high CHD risk. We developed a user-friendly nomogram that could potentially be of benefit to the public and to policymakers in formulating effective strategies for CHD risk assessment and primary prevention.
Materials and Methods
Study design and participants
The participants in this case-control study were enrolled from the Affiliated Union Hospital and the First Affiliated Hospital of Fujian Medical University (Fuzhou, China) between October 2014 and August 2019. A total of 4392 participants (1578 CHD cases and 2814 controls) confirmed their participation by signing an informed consent form. Our research program was in line with the Helsinki declaration and was approved by the review board of Fujian Medical University.
Case-Control selection
The diagnosis of CHD was made by at least two experienced cardiologists based on coronary angiography. A patient was deemed to have CHD if at least one of the three major coronary arteries or major branches had significant coronary stenosis ≥ 50% [47]. Excluded were patients with other severe heart diseases, autoimmune diseases, diseases of other organs, or cancers. The corresponding control participants were deemed to be free of CHD after a series of evaluations, including clinical examinations and medical history assessments.
Predictors
We specified the most likely temporal associations between variables based on prior biological and epidemiologic knowledge and derived predictors, including biological, behavioral and psychological factors (Figure 5). Among potential predictors, the biological variables were sex; age; marital status; educational level; family history of hypertension, diabetes, CHD or stroke; hypertension; hyperlipidemia; diabetes; BMI; WHR; and WHtR. The behavioral variables were smoking, alcohol drinking, tea drinking, diet, physical exercise, video duration, sleep duration and sleep quality. The psychological variables were major events in the last year, life satisfaction, character type, anxiety and depression. The definitions of these variables are listed in Table 5.
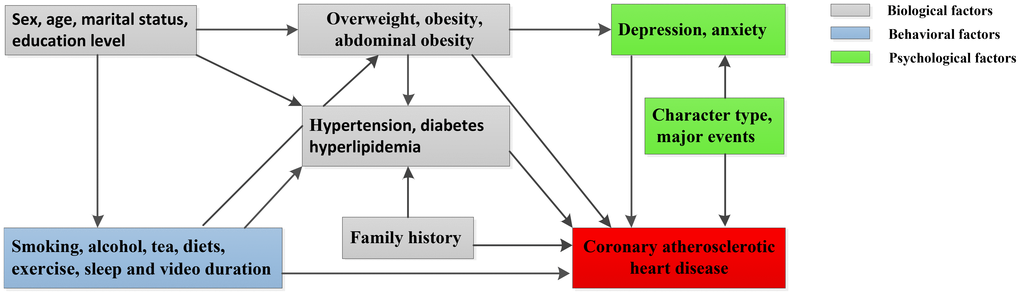
Figure 5. Hypothesized association between CHD and potential predictors in our study.
Table 5. The definition of variables in this study.
| Variables | Definition |
| Body mass index (BMI) | BMI = weight (kg) / [height (m)]2. <18.50 kg/m2 (underweight), 18.5–23.99 kg/m2 (normal), 24-27.99 kg/m2 (overweight), ≥28.00 kg/m2 (obese) [48]. |
| Waist hip ratio (WHR) | WHR = waist / hip. Abdominal obesity: ≥0.85 (women); ≥0.90 (men) [49]. |
| Waist to height ratio (WHtR) | WHtR= waist (m) / height (m), and WHtR ≥0.5 was defined as obesity [50]. |
| Pack- year Smoking | Pack- year Smoking= (No. of years of smoking * average no. of cigarette smoked per day) / 20 cigarettes in a pack [51]. |
| Alcohol drinking | Alcohol drinkers were defined according to literature [52], and divided into the following three levels: no drinking, <3 time/week and ≥3 time/week. |
| High-salt diet | Daily salt intake was calculated by averaging a family's annual salt consumption with the number of members [53], and a high-salt diet means eating more than 6 grams of salt per day. |
| Food | Vegetable, fruit, fried food and fat meat eaten 1 or more times a day were recorded as 1 day, and the weekly vegetable, fruit, fried food and fat meat of all subjects were determined. |
| Physical exercise | Effective physical activity referred to exercise that lasts for least 20 minutes each time, and was used to define weekly physical activity for all subjects. |
| Sleep quality | Sleep quality was defined by asking whether the respondents had difficulty falling asleep or/and staying asleep during the past year. They were divided into 5 levels: very good (<1 day/month), good (1-3 days/month), general (4-7 days/month), poor (8-15 days/month) and every poor (≥16 days/month or need to take medicine to sleep), which are filled out by the respondents themselves. |
| Encountering major events | Encountering major events referred to accidents such as death or serious illness of family members, family bankruptcy, unemployment, marital barriers in the past year. |
| Anxiety | Anxiety was evaluated by self-rating anxiety scale (SAS). SAS scores ≥50 was used to indicate anxiety, and the Cronbach’s α in this study was 0.85 [54]. |
| Depression | A self-rating depression scale (SDS) was performed to estimate depression. SDS ≥53 was defined as depression, and the Cronbach’s α in this study was 0.86 [54]. |
Statistical analysis
The characteristic differences between the case and control groups were evaluated using the Chi-square test. Variables with P-values <0.05 in the univariate analyses were introduced as independent predictors into a multivariate logistic regression. We estimated the strength of the association between CHD risk and predictors by OR and 95% CI. Significant variables were selected using the “Backwald: Wald” method and were used to construct a nomogram. The total score of the nomogram was classified by quartile to assess the association of the total score with CHD risk. The discriminative ability, predictive accuracy and clinical application value of the model was assessed using a receiver operating characteristic (ROC) curve, calibration plot, and decision curve analysis. A total of 500 bootstrap resamples were employed to reduce over-fit bias. Statistical analyses were performed using SPSS version 25.0, R version 3.5, MedCalc and EmpowerStats for Windows. Two-sided P values < 0.05 was considered significant.
Author Contributions
S.H., X.Xie., S.W., and H.L. contributed to the study design. X.Xie., S.H., Y.S. performed statistical analysis, interpretation, and drafted the manuscript. T.Z., Y.C., X.Xu. contributed to data collection. Y.S., S.H., X.Xie. revised the manuscript. All authors contributed to critical revision of the final manuscript and approved the final version of the manuscript. S.W. and X.Xie. provided financial support and study supervision.
Acknowledgments
The authors thank the participants and participating physicians from First Affiliated Hospital of Fujian Medical University and Fujian Medical University Union Hospital, China, as the staff that made this research possible.
Conflicts of Interest
The authors declare no potential conflicts of interest.
Funding
This research was funded by Joint Funds for the Innovation of Science and Technology, Fujian Province (2018Y9089), the Natural Science Foundation of Fujian Province (Grant No. 2019J01315), Fujian Medical University talent research funding (XRCZX2019031), and Professor Development Fund Project of Fujian Medical University (JS15002).
References
- 1. Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, Abdollahpour I, Abdulkader RS, Abebe HT, et al, and GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392:1736–88. https://doi.org/10.1016/S0140-6736(18)32203-7 [PubMed]
- 2. Zhu KF, Wang YM, Zhu JZ, Zhou QY, Wang NF. National prevalence of coronary heart disease and its relationship with human development index: A systematic review. Eur J Prev Cardiol. 2016; 23:530–43. https://doi.org/10.1177/2047487315587402 [PubMed]
- 3. Bi Y, Jiang Y, He J, Xu Y, Wang L, Xu M, Zhang M, Li Y, Wang T, Dai M, Lu J, Li M, Chen CS, et al, and 2010 China Noncommunicable Disease Surveillance Group. Status of cardiovascular health in Chinese adults. J Am Coll Cardiol. 2015; 65:1013–25. https://doi.org/10.1016/j.jacc.2014.12.044 [PubMed]
- 4. Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, Li X, Wang L, Wang L, Liu Y, Liu J, Zhang M, Qi J, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019; 394:1145–58. https://doi.org/10.1016/S0140-6736(19)30427-1 [PubMed]
- 5. Liu S, Li Y, Zeng X, Wang H, Yin P, Wang L, Liu Y, Liu J, Qi J, Ran S, Yang S, Zhou M. Burden of cardiovascular diseases in China, 1990-2016: findings from the 2016 global Burden of disease study. JAMA Cardiol. 2019; 4:342–52. https://doi.org/10.1001/jamacardio.2019.0295 [PubMed]
- 6. Acharya D, Gulack BC, Loyaga-Rendon RY, Davies JE, He X, Brennan JM, Thourani VH, Williams ML. Clinical characteristics and outcomes of patients with myocardial infarction and cardiogenic shock undergoing coronary artery bypass surgery: data from the society of thoracic surgeons national database. Ann Thorac Surg. 2016; 101:558–66. https://doi.org/10.1016/j.athoracsur.2015.10.051 [PubMed]
- 7. Shapiro MD, Maron DJ, Morris PB, Kosiborod M, Sandesara PB, Virani SS, Khera A, Ballantyne CM, Baum SJ, Sperling LS, Bhatt DL, Fazio S. Preventive cardiology as a subspecialty of cardiovascular medicine: JACC council perspectives. J Am Coll Cardiol. 2019; 74:1926–42. https://doi.org/10.1016/j.jacc.2019.08.1016 [PubMed]
- 8. Li N, Katzmarzyk PT, Horswell R, Zhang Y, Li W, Zhao W, Wang Y, Johnson J, Hu G. BMI and coronary heart disease risk among low-income and underinsured diabetic patients. Diabetes Care. 2014; 37:3204–12. https://doi.org/10.2337/dc14-1091 [PubMed]
- 9. Degerud E, Ariansen I, Ystrom E, Graff-Iversen S, Høiseth G, Mørland J, Davey Smith G, Næss Ø. Life course socioeconomic position, alcohol drinking patterns in midlife, and cardiovascular mortality: analysis of Norwegian population-based health surveys. PLoS Med. 2018; 15:e1002476. https://doi.org/10.1371/journal.pmed.1002476 [PubMed]
- 10. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. 2017; 14:145–55. https://doi.org/10.1038/nrcardio.2016.181 [PubMed]
- 11. Vasan RS, Sullivan LM, Wilson PW, Sempos CT, Sundström J, Kannel WB, Levy D, D’Agostino RB. Relative importance of borderline and elevated levels of coronary heart disease risk factors. Ann Intern Med. 2005; 142:393–402. https://doi.org/10.7326/0003-4819-142-6-200503150-00005 [PubMed]
- 12. Pencina MJ, Navar AM, Wojdyla D, Sanchez RJ, Khan I, Elassal J, D’Agostino RB
Sr , Peterson ED, Sniderman AD. Quantifying importance of major risk factors for coronary heart disease. Circulation. 2019; 139:1603–11. https://doi.org/10.1161/CIRCULATIONAHA.117.031855 [PubMed] - 13. Chomistek AK, Chiuve SE, Eliassen AH, Mukamal KJ, Willett WC, Rimm EB. Healthy lifestyle in the primordial prevention of cardiovascular disease among young women. J Am Coll Cardiol. 2015; 65:43–51. https://doi.org/10.1016/j.jacc.2014.10.024 [PubMed]
- 14. Satija A, Bhupathiraju SN, Spiegelman D, Chiuve SE, Manson JE, Willett W, Rexrode KM, Rimm EB, Hu FB. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J Am Coll Cardiol. 2017; 70:411–22. https://doi.org/10.1016/j.jacc.2017.05.047 [PubMed]
- 15. Li Y, Hruby A, Bernstein AM, Ley SH, Wang DD, Chiuve SE, Sampson L, Rexrode KM, Rimm EB, Willett WC, Hu FB. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort study. J Am Coll Cardiol. 2015; 66:1538–48. https://doi.org/10.1016/j.jacc.2015.07.055 [PubMed]
- 16. Moholdt T, Lavie CJ, Nauman J. Sustained physical activity, not weight loss, associated with improved survival in coronary heart disease. J Am Coll Cardiol. 2018; 71:1094–101. https://doi.org/10.1016/j.jacc.2018.01.011 [PubMed]
- 17. Farvid MS, Ding M, Pan A, Sun Q, Chiuve SE, Steffen LM, Willett WC, Hu FB. Dietary linoleic acid and risk of coronary heart disease: a systematic review and meta-analysis of prospective cohort studies. Circulation. 2014; 130:1568–78. https://doi.org/10.1161/CIRCULATIONAHA.114.010236 [PubMed]
- 18. Rafanelli C, Roncuzzi R, Milaneschi Y, Tomba E, Colistro MC, Pancaldi LG, Di Pasquale G. Stressful life events, depression and demoralization as risk factors for acute coronary heart disease. Psychother Psychosom. 2005; 74:179–84. https://doi.org/10.1159/000084003 [PubMed]
- 19. Vaccarino V, Goldberg J, Rooks C, Shah AJ, Veledar E, Faber TL, Votaw JR, Forsberg CW, Bremner JD. Post-traumatic stress disorder and incidence of coronary heart disease: a twin study. J Am Coll Cardiol. 2013; 62:970–78. https://doi.org/10.1016/j.jacc.2013.04.085 [PubMed]
- 20. Nabi H, Hall M, Koskenvuo M, Singh-Manoux A, Oksanen T, Suominen S, Kivimäki M, Vahtera J. Psychological and somatic symptoms of anxiety and risk of coronary heart disease: the health and social support prospective cohort study. Biol Psychiatry. 2010; 67:378–85. https://doi.org/10.1016/j.biopsych.2009.07.040 [PubMed]
- 21. Watkins LL, Koch GG, Sherwood A, Blumenthal JA, Davidson JR, O’Connor C, Sketch MH
Jr . Association of anxiety and depression with all-cause mortality in individuals with coronary heart disease. J Am Heart Assoc. 2013; 2:e000068. https://doi.org/10.1161/JAHA.112.000068 [PubMed] - 22. Wang K, Gong M, Xie S, Zhang M, Zheng H, Zhao X, Liu C. Nomogram prediction for the 3-year risk of type 2 diabetes in healthy mainland China residents. EPMA J. 2019; 10:227–37. https://doi.org/10.1007/s13167-019-00181-2 [PubMed]
- 23. Dong X, Zhang R, He J, Lai L, Alolga RN, Shen S, Zhu Y, You D, Lin L, Chen C, Zhao Y, Duan W, Su L, et al. Trans-omics biomarker model improves prognostic prediction accuracy for early-stage lung adenocarcinoma. Aging (Albany NY). 2019; 11:6312–35. https://doi.org/10.18632/aging.102189 [PubMed]
- 24. Wang Z, Gao L, Guo X, Feng C, Lian W, Deng K, Xing B. Development and validation of a nomogram with an autophagy-related gene signature for predicting survival in patients with glioblastoma. Aging (Albany NY). 2019; 11:12246–69. https://doi.org/10.18632/aging.102566 [PubMed]
- 25. Hyvärinen M, Qiao Q, Tuomilehto J, Söderberg S, Eliasson M, Stehouwer CD. The difference between acute coronary heart disease and ischaemic stroke risk with regard to gender and age in Finnish and Swedish populations. Int J Stroke. 2010; 5:152–56. https://doi.org/10.1111/j.1747-4949.2010.00423.x [PubMed]
- 26. Veronesi G, Gianfagna F, Giampaoli S, Chambless LE, Mancia G, Cesana G, Ferrario MM. Improving long-term prediction of first cardiovascular event: the contribution of family history of coronary heart disease and social status. Prev Med. 2014; 64:75–80. https://doi.org/10.1016/j.ypmed.2014.04.007 [PubMed]
- 27. Murray MK, Bode K, Whittaker P. Gender-specific associations between coronary heart disease and other chronic diseases: cross-sectional evaluation of national survey data from adult residents of Germany. J Geriatr Cardiol. 2019; 16:663–70. https://doi.org/10.11909/j.issn.1671-5411.2019.09.004 [PubMed]
- 28. Rämö JT, Ripatti P, Tabassum R, Söderlund S, Matikainen N, Gerl MJ, Klose C, Surma MA, Stitziel NO, Havulinna AS, Pirinen M, Salomaa V, Freimer NB, et al. Coronary Artery Disease Risk and Lipidomic Profiles Are Similar in Hyperlipidemias With Family History and Population-Ascertained Hyperlipidemias. J Am Heart Assoc. 2019; 8:e012415. https://doi.org/10.1161/JAHA.119.012415 [PubMed]
- 29. Mansoor H, Jo A, Beau De Rochars VM, Pepine CJ, Mainous AG
3rd . Novel Self-Report Tool for Cardiovascular Risk Assessment. J Am Heart Assoc. 2019; 8:e014123. https://doi.org/10.1161/JAHA.119.014123 [PubMed] - 30. Thurston RC, Kubzansky LD, Kawachi I, Berkman LF. Do depression and anxiety mediate the link between educational attainment and CHD? Psychosom Med. 2006; 68:25–32. https://doi.org/10.1097/01.psy.0000195883.68888.68 [PubMed]
- 31. Roest AM, Martens EJ, de Jonge P, Denollet J. Anxiety and risk of incident coronary heart disease: a meta-analysis. J Am Coll Cardiol. 2010; 56:38–46. https://doi.org/10.1016/j.jacc.2010.03.034 [PubMed]
- 32. Steptoe A, Kivimäki M. Stress and cardiovascular disease. Nat Rev Cardiol. 2012; 9:360–70. https://doi.org/10.1038/nrcardio.2012.45 [PubMed]
- 33. Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation. 1999; 99:2192–217. https://doi.org/10.1161/01.CIR.99.16.2192 [PubMed]
- 34. Virtanen M, Vahtera J, Singh-Manoux A, Elovainio M, Ferrie JE, Kivimäki M. Unfavorable and favorable changes in modifiable risk factors and incidence of coronary heart disease: the Whitehall II cohort study. Int J Cardiol. 2018; 269:7–12. https://doi.org/10.1016/j.ijcard.2018.07.005 [PubMed]
- 35. Li W, Xie B, Qiu S, Huang X, Chen J, Wang X, Li H, Chen Q, Wang Q, Tu P, Zhang L, Yan S, Li K, et al. Non-lab and semi-lab algorithms for screening undiagnosed diabetes: A cross-sectional study. EBioMedicine. 2018; 35:307–16. https://doi.org/10.1016/j.ebiom.2018.08.009 [PubMed]
- 36. Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998; 97:1837–47. https://doi.org/10.1161/01.CIR.97.18.1837 [PubMed]
- 37. Chen G, Levy D. Contributions of the Framingham Heart Study to the Epidemiology of Coronary Heart Disease. JAMA Cardiol. 2016; 1:825–30. https://doi.org/10.1001/jamacardio.2016.2050 [PubMed]
- 38. Hense HW, Schulte H, Löwel H, Assmann G, Keil U. Framingham risk function overestimates risk of coronary heart disease in men and women from Germany—results from the MONICA Augsburg and the PROCAM cohorts. Eur Heart J. 2003; 24:937–45. https://doi.org/10.1016/S0195-668X(03)00081-2 [PubMed]
- 39. van der Heijden AA, Ortegon MM, Niessen LW, Nijpels G, Dekker JM. Prediction of coronary heart disease risk in a general, pre-diabetic, and diabetic population during 10 years of follow-up: accuracy of the Framingham, SCORE, and UKPDS risk functions: The Hoorn Study. Diabetes Care. 2009; 32:2094–98. https://doi.org/10.2337/dc09-0745 [PubMed]
- 40. Empana JP, Ducimetière P, Arveiler D, Ferrières J, Evans A, Ruidavets JB, Haas B, Yarnell J, Bingham A, Amouyel P, Dallongeville J, and PRIME Study Group. Are the Framingham and PROCAM coronary heart disease risk functions applicable to different European populations? The PRIME Study. Eur Heart J. 2003; 24:1903–11. https://doi.org/10.1016/j.ehj.2003.09.002 [PubMed]
- 41. Liu J, Hong Y, D’Agostino RB
Sr , Wu Z, Wang W, Sun J, Wilson PW, Kannel WB, Zhao D. Predictive value for the Chinese population of the Framingham CHD risk assessment tool compared with the Chinese Multi-Provincial Cohort Study. JAMA. 2004; 291:2591–99. https://doi.org/10.1001/jama.291.21.2591 [PubMed] - 42. Naoum C, Berman DS, Ahmadi A, Blanke P, Gransar H, Narula J, Shaw LJ, Kritharides L, Achenbach S, Al-Mallah MH, Andreini D, Budoff MJ, Cademartiri F, et al. Predictive value of age- and sex-specific nomograms of global plaque burden on coronary computed tomography angiography for major cardiac events. Circ Cardiovasc Imaging. 2017; 10:e004896. https://doi.org/10.1161/CIRCIMAGING.116.004896 [PubMed]
- 43. Wu N, Chen X, Li M, Qu X, Li Y, Xie W, Wu L, Xiang Y, Li Y, Zhong L. Predicting obstructive coronary artery disease using carotid ultrasound parameters: A nomogram from a large real-world clinical data. Eur J Clin Invest. 2018; 48:e12956. https://doi.org/10.1111/eci.12956 [PubMed]
- 44. Ó Hartaigh B, Gransar H, Callister T, Shaw LJ, Schulman-Marcus J, Stuijfzand WJ, Valenti V, Cho I, Szymonifka J, Lin FY, Berman DS, Chang HJ, Min JK. Development and validation of a simple-to-use nomogram for predicting 5-, 10-, and 15-year survival in asymptomatic adults undergoing coronary artery calcium scoring. JACC Cardiovasc Imaging. 2018; 11:450–58. https://doi.org/10.1016/j.jcmg.2017.03.018 [PubMed]
- 45. Benner JS, Erhardt L, Flammer M, Moller RA, Rajicic N, Changela K, Yunis C, Cherry SB, Gaciong Z, Johnson ES, Sturkenboom MC, García-Puig J, Girerd X, and REACH OUT Investigators. A novel programme to evaluate and communicate 10-year risk of CHD reduces predicted risk and improves patients’ modifiable risk factor profile. Int J Clin Pract. 2008; 62:1484–98. https://doi.org/10.1111/j.1742-1241.2008.01872.x [PubMed]
- 46. Chiuve SE, McCullough ML, Sacks FM, Rimm EB. Healthy lifestyle factors in the primary prevention of coronary heart disease among men: benefits among users and nonusers of lipid-lowering and antihypertensive medications. Circulation. 2006; 114:160–67. https://doi.org/10.1161/CIRCULATIONAHA.106.621417 [PubMed]
- 47. Nomenclature and criteria for diagnosis of ischemic heart disease. Report of the Joint International Society and Federation of Cardiology/World Health Organization task force on standardization of clinical nomenclature. Circulation. 1979; 59:607–09. https://doi.org/10.1161/01.CIR.59.3.607 [PubMed]
- 48. Kokkinos P, Faselis C, Myers J, Pittaras A, Sui X, Zhang J, McAuley P, Kokkinos JP. Cardiorespiratory fitness and the paradoxical BMI-mortality risk association in male veterans. Mayo Clin Proc. 2014; 89:754–62. https://doi.org/10.1016/j.mayocp.2014.01.029 [PubMed]
- 49. Sharma S, Batsis JA, Coutinho T, Somers VK, Hodge DO, Carter RE, Sochor O, Kragelund C, Kanaya AM, Zeller M, Park JS, Køber L, Torp-Pedersen C, Lopez-Jimenez F. Normal-weight central obesity and mortality risk in older adults with coronary artery disease. Mayo Clin Proc. 2016; 91:343–51. https://doi.org/10.1016/j.mayocp.2015.12.007 [PubMed]
- 50. Machado Arruda SP, da Silva AA, Kac G, Vilela AA, Goldani M, Bettiol H, Barbieri MA. Dietary patterns are associated with excess weight and abdominal obesity in a cohort of young Brazilian adults. Eur J Nutr. 2016; 55:2081–91. https://doi.org/10.1007/s00394-015-1022-y [PubMed]
- 51. Lasebikan V, Lasebikan T, Adepoju S. Outdoor smoking in Nigeria: prevalence, correlates and predictors. BMC Public Health. 2019; 19:1313–24. https://doi.org/10.1186/s12889-019-7601-8 [PubMed]
- 52. Kaluza J, Harris HR, Linden A, Wolk A. Alcohol consumption and risk of chronic obstructive pulmonary disease: a prospective cohort study of men. Am J Epidemiol. 2019; 188:907–16. https://doi.org/10.1093/aje/kwz020 [PubMed]
- 53. Wu D, Chen Y, Guan H, Sun Y, Sun Y. Association of abnormal serum electrolyte levels with hypertension in a population with high salt intake. Public Health Nutr. 2019; 22:1635–45. https://doi.org/10.1017/S1368980019000260 [PubMed]
- 54. Xie YH, Xie HT, Wang TS, Shu YP, Dai XL. Perioperative holistic care more significantly reduces levels of anxiety and depression of pituitary tumor patients versus conventional care. Medicine (Baltimore). 2019; 98:e14411. https://doi.org/10.1097/MD.0000000000014411 [PubMed]