



Introduction
It is well known that patients with Down syndrome (DS), which is a common chromosomal abnormality disease caused by the presence of an extra copy of chromosome 21, have an increased risk of developing early-onset Alzheimer's disease (AD) [1, 2]. The increased risk of AD in patients with DS is thought to be caused by the triplication and overexpression of the gene for the amyloid precursor protein (APP), located on chromosome 21, leading to altered production, aggregation, and deposition of amyloid beta-peptide (Aβ) in the brains of patients with DS [3, 4].
Due to the pathological role of Aβ in the onset and progression of AD, a large number of studies have analyzed blood and cerebrospinal fluid (CSF) Aβ levels in patients with late-onset AD in the general population. Although the results of these studies have been inconsistent, a high-profile systematic review and meta-analysis concluded that patients with AD did not have significantly altered blood Aβ1-42 and Aβ1-40 levels compared to those in healthy control (HC) subjects. Further, it indicated that the CSF Aβ1-42 levels were consistently reduced in the patients with AD patients compared to in HC subjects and suggested that CSF Aβ1-42 is a good biomarker for AD diagnosis [5]. Some studies have reported that patients with DS have higher blood Aβ1-42 and Aβ1-40 levels than those in HC subjects [6–10] while other studies did not find a significant difference in the Aβ1-42 levels between patients and HC subjects [11–13]. Blood Aβ1-42 and/or Aβ1-40 levels seem to alter with age and have been associated with gender in some studies [8, 9, 14] but not in others [15, 16]. Further, there have been inconsistent findings on changes in blood Aβ1-42 and Aβ1-40 levels after dementia onset [17–19]. Additionally, there have been inconsistent results regarding CSF Aβ1-42 and Aβ1-40 levels in patients with DS with dementia (DSD) or without dementia [20, 21].
Given the inconsistent findings, there is a need for a meta-analysis of these studies. Therefore, we performed a systematic review and meta-analysis to analyze aberrations in peripheral blood and CSF Aβ1-42 and Aβ1-40 levels in patients with DS and those with DSD. Further, we evaluated several potential moderators that contribute to the between-study heterogeneity.
Results
Blood Aβ1-42 and Aβ1-40 levels in patients with DS and those with DSD
27 articles were included in the current meta-analysis (Figure 1). First, we compared the peripheral blood Aβ1-42 and Aβ1-40 levels between patients with DS and HC subjects. For Aβ1-40, we used data extracted from 14 studies that included 1440 individuals while for Aβ1-42, we used data extracted from 17 studies that included 1587 individuals. Random-effects meta-analysis showed that patients with DS had significantly increased blood Aβ1-40 (Hedges’ g = 1.997, 95% CI = 1.422 to 2.571, P < 0.001) and Aβ1-42 levels (Hedges’ g = 1.104, 95% CI = 0.445 to 1.763, P = 0.001) compared with HC subjects (Figure 2A, 2B). Sensitivity analysis showed that the significant associations between blood Aβ levels and DS were not affected by one particular study. However, we found significant heterogeneity among studies comparing blood Aβ1-40 (Q = 248.253, d.f. = 13, I2 = 94.763, P < 0.001) and Aβ1-42 levels (Q = 475.084, d.f. = 16, I2 = 96.632, P < 0.001) between patients with DS and HC subjects. Further, meta-analysis of the blood Aβ1-42/Aβ1-40 ration reported in patients with DS by 5 studies encompassing 424 individuals revealed no significant difference between patients with DS and HC subjects (Hedges’ g = -0.830, 95% CI = -1.919 to 0.259, P = 0.135, Supplementary Figure 1A).
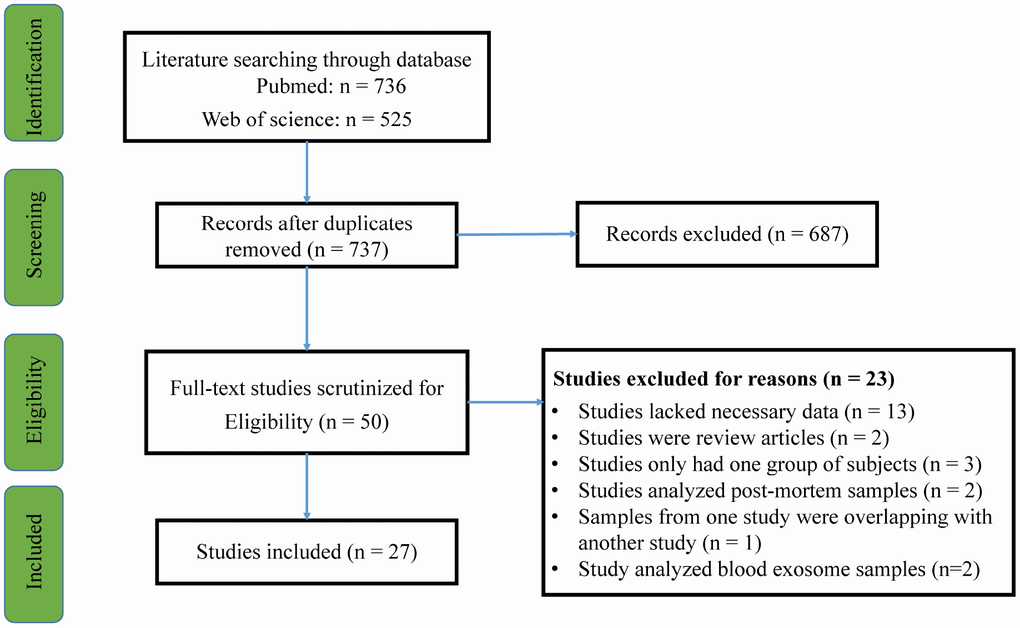
Figure 1. PRISMA flowchart of the literature search.
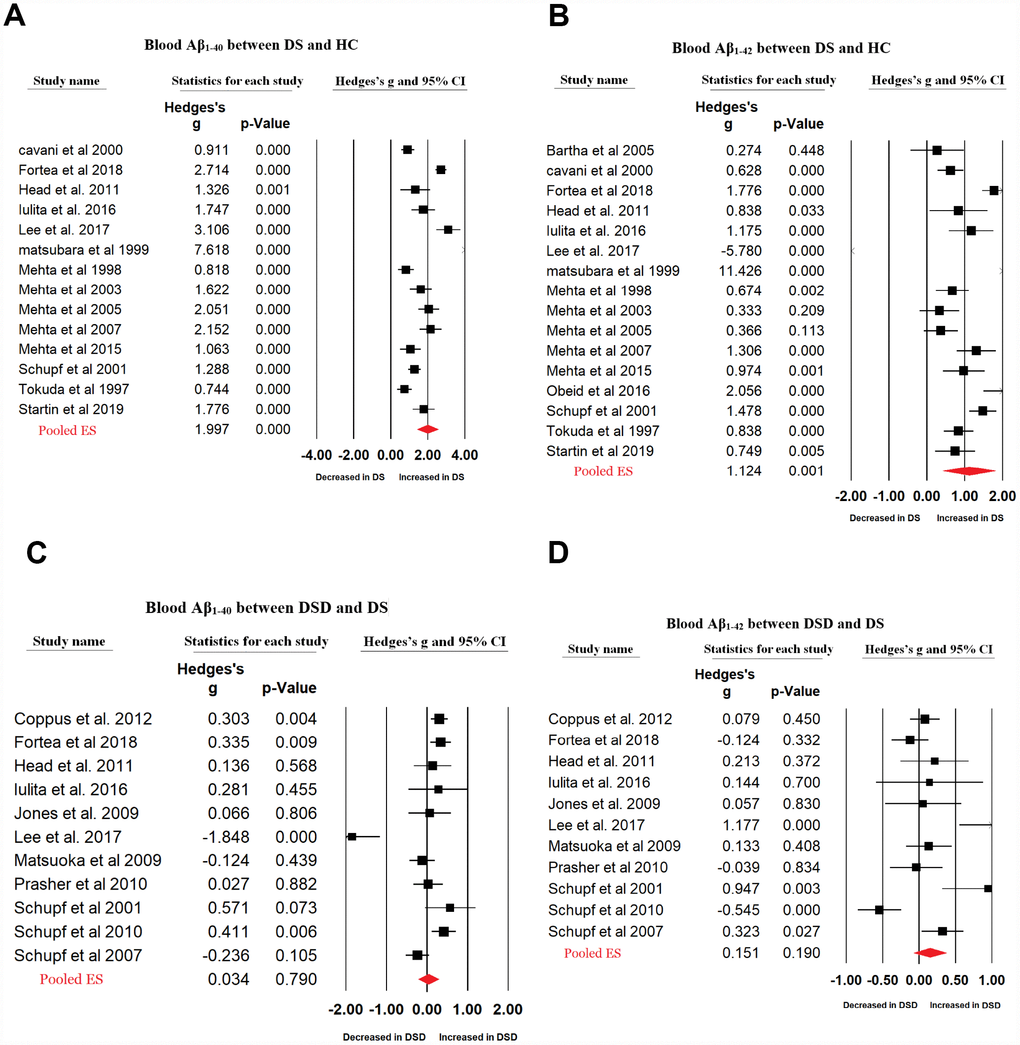
Figure 2. Forest plot for random-effects meta-analysis on difference in blood Aβ1-40 (A) and Aβ1-42 (B) concentrations between DS patients and HC subjects; blood Aβ1-40 (C) and Aβ1-42 (D) concentrations between DSD and DS patients. DS, Down syndrome. DSD, Down syndrome with dementia. HC, healthy control. CI, confidence interval.
Next, we compared the peripheral blood Aβ1-42 and Aβ1-40 levels between patients with DS and those with DSD using data extracted from 11 studies including 1771 individuals. Random-effects meta-analysis indicated no significant difference in the blood Aβ1-40 (Hedges’ g = 0.034, 95% CI = -0.218 to 0.286, P = 0.790) and Aβ1-42 levels (Hedges’ g = 0.151, 95% CI = -0.075 to 0.378, P = 0.190) between patients with DS and those with DSD (Figure 2C, 2D). Sensitivity analysis showed that the results for Aβ1-42, but not Aβ1-40, were influenced by one particular study (Supplementary Figure 2B, 2C). There was significant heterogeneity between studies analyzing blood Aβ1-40 (Q = 52.125, d.f. = 10, I2 = 80.815, P < 0.001) and Aβ1-42 levels (Q = 42.055, d.f. = 10, I2 = 76.222, P < 0.001) in patients with DS and those with DSD. Further, analysis of data extracted from 5 studies encompassing 886 individuals indicated no significant difference in the blood Aβ1-42/ Aβ1-40 ratio between patients with DSD and those with DS (Hedges’ g = 0.029, 95% CI = -0.458 to 0.516, P = 0.907) (Supplementary Figure 1D).
CSF Aβ1-42 and Aβ1-40 levels in patients with DS and those with DSD
Fewer data were available for CSF Aβ levels in patients with DS and those with DSD. Random-effects meta-analysis did not show a significant difference between patients with DS and HC subjects in the CSF Aβ1-40 levels (3 studies, Hedges’ g = 0.128, 95% CI = -0.079 to 0.336, P = 0.226) while CSF Aβ1-42 levels were significantly decreased in patients with DS compared with those in HC subjects (5 studies, Hedges’ g = -0.336, 95% CI = -0.530 to -0.143, P = 0.001). In addition, compared with patients with DS, random-effects meta-analysis showed that CSF Aβ1-42 levels were significantly decreased in patients with DSD (2 studies, Hedges’ g = -1.235, 95% CI = -1.523 to -0.946, P < 0.001, Figure 3) with a large ES, but not CSF Aβ1-40 levels (Hedges’ g = -0.153, 95% CI = -0.535 to 0.229, P = 0.433) (Figure 3). There were no between-study heterogeneities in the studies analyzing CSF Aβ1-40 and Aβ1-42 levels.
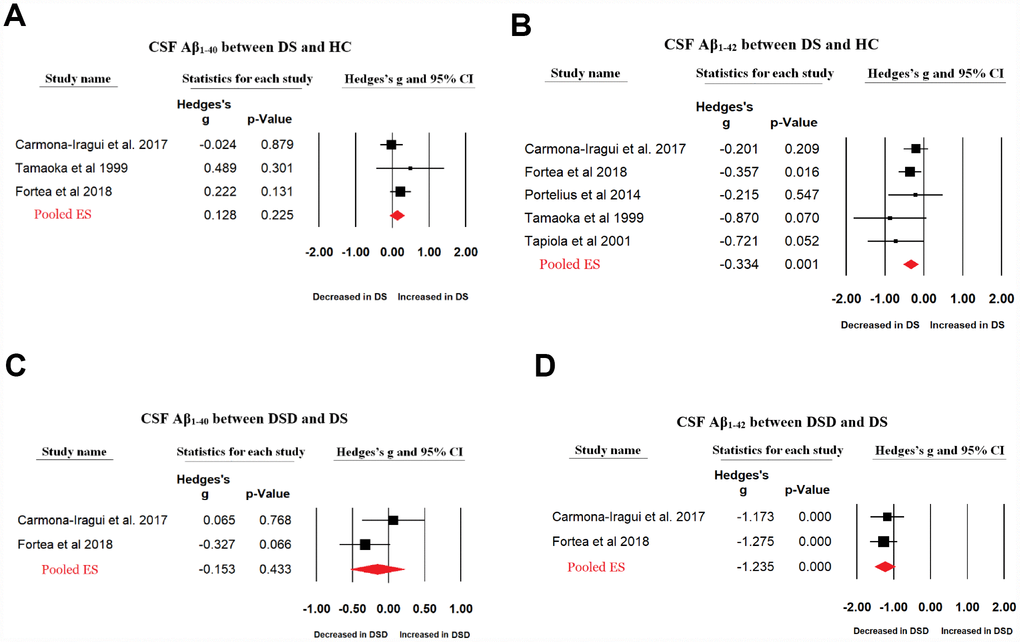
Figure 3. Forest plot for random-effects meta-analysis on difference in CSF Aβ1-40 (A) and Aβ1-42 (B) concentrations between DS patients and HC subjects; CSF Aβ1-40 (C) and Aβ1-42 (D) concentrations between DSD and DS patients. CSF, Cerebrospinal fluid. DS, Down syndrome. DSD, Down syndrome with dementia. HC, healthy control. CI, confidence interval.
Investigation of heterogeneity
Next, we investigated the potential sources that influenced the observed heterogeneity and analyzed the studies comparing the blood Aβ1-40 and Aβ1-42 levels in patients with DS and HC subjects. First, we performed sub-group analysis based on age and the patients were classified into two groups as follows: old (age above 45 years old) and young group (age below 45 years old). Compared with HC subjects, blood Aβ1-40 (4 studies, Hedges’ g = 1.331, 95% CI = 1.077 to 1.585, P < 0.001) and Aβ1-42 (4 studies, Hedges’ g = 1.065, 95% CI= 0.676 to 1.455, P <0.001) levels were significantly increased in the old group of patient with DS with reduced between-study heterogeneities for both Aβ1-40 (Q3 = 3.041, I2 = 1.338, P = 0.385) and Aβ1-42 (Q3 = 6.56, I2= 54.313, P = 0.087). In contrast, compared with HC subjects, blood Aβ1-40 levels were significantly increased in the young group of patients with DS (9 studies, Hedges’ g = 1.750, 95% CI = 1.145 to 2.355, P < 0.001) but not Aβ1-42 levels (12 studies, Hedges’ g = 0.443, 95% CI = -0.200 to 1.087, P = 0.177) with between-study heterogeneities remaining high for both Aβ1-40 (Q8 = 122.948, I2 = 93.493, P < 0.001) and Aβ1-42 (Q11 = 235.814, I2 = 95.759, P < 0.001).
Next, we performed meta-regression analyses to assess whether continuous variables, including gender (proportion of males), sample size, and publication year, could explain the between-study heterogeneity. We found that gender, sample size, and publication year did not significantly affect the outcomes of the meta-analysis comparing blood Aβ1-40 and Aβ1-42 levels between patients with DS and HC subjects (P > 0.05 in all the analyses).
Publication bias
Visual inspection of funnel plots suggested no significant publication bias among studies comparing blood Aβ1-40 (Figure 4A) and Aβ1-42 (Figure 4B) levels between patients with DS and HC subjects, which was confirmed by Egger’s test (P > 0.05). Further, we used the classic fail-safe N to evaluate potential publication bias and found that 2499 missing studies on blood Aβ1-40 and 1027 missing studies on blood Aβ1-42 would be required to make p > 0.05, indicating that the significant differences in the blood Aβ levels between patients with DS and HC subjects were unlikely caused by publication bias.
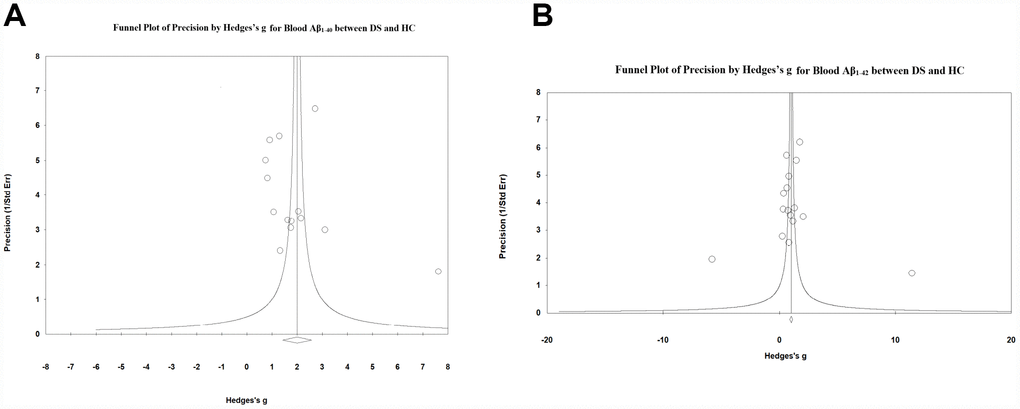
Figure 4. Visual inspection of funnel plots suggested no significant publication bias among studies comparing (A) blood Aβ1-40 and (B) Aβ1-42 levels between DS patients and HC subjects.
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis of clinical studies on Aβ levels in patients with DS and those with DSD. We found significantly increased blood Aβ1-42 and Aβ1-40 levels in the patients with DS compared with those in HC subjects. However, there were no significant differences in the blood Aβ1-42 and Aβ1-40 levels between patients with DSD and those with DS. Further, we found that CSF Aβ1-42, but not Aβ1-40, levels were significantly decreased in patients with DS compared to those in HC subjects while CSF Aβ1-42 levels were significantly decreased in patients with DSD compared to those in patients with DS. Taken together, the meta-analysis demonstrated that blood Aβ1-40 and Aβ1-42 levels were significantly increased in patients with DS while CSF Aβ1-42, but not Aβ1-40, levels were significantly decreased in patients with DS. These findings may enhance our knowledge of the molecular mechanism underlying the development and/or progression of dementia in patients with DS.
The baseline elevation of blood Aβ1-40 and Aβ1-42 levels in patients with DS is a reasonable finding given their overexpression of the APP protein. Increased blood Aβ1-40 and Aβ1-42 levels in patients with DS was reported in all the included studies except that by Lee et al., which reported decreased blood Aβ1-42 levels in patients with DS compared with those in HC subjects [17]. Use of different assay types might explain the inconsistent results regarding blood Aβ1-42 levels in patients with DS. This is because Lee et al. used a non-ELISA method to measure Aβ1-42 levels while the other studies employed ELISA assay to assess Aβ1-42 levels. It remains unclear whether increased blood Aβ1-42 and Aβ1-40 levels in patients with DS are associated with the development of AD pathology. However, the observed non-significant differences in blood Aβ1-42 and Aβ1-40 levels between patients with DS and those with DSD suggest that blood Aβ is unlikely to be a key factor in the development of dementia in these patients. This is supported by the findings of a previous systematic review and meta-analysis that reported no significant change in blood Aβ1-42 and Aβ1-40 levels in the general population of patients with AD [5].
Contrastingly to the observed increased blood Aβ levels in patients with DS, CSF Aβ showed a differential expression profile in the patients. The finding of decreased CSF Aβ1-42 levels in patients with DS is consistent with previous reports of Aβ plaque formation in the brains of patients with DS without dementia symptoms [22, 23]. It is unknown why Aβ accumulation and deposition does not lead to dementia before middle age in patients with DS. The small ES of decreased CSF Aβ1-42 levels in patients with DS implies that Aβ1-42 accumulation in the brains of patients with DS was not detrimental enough to cause global cell death in the central nervous system, and thus lead to dementia onset. This is supported by a previous meta-analysis indicated that CSF Aβ1-42 levels were significantly associated with AD in the general population with medium ES [5]. In addition, patients with DSD showed significantly decreased CSF Aβ1-42 levels compared with those in patients with DS and with a large ES. This suggests a significant accumulation of Aβ1-42 in the brains of patients with DSD, which might explain the early onset of dementia in patients with DS. In contrast to the decreased CSF Aβ1-42 levels in patients with DS and those with DSD, there was no significant difference in the CSF Aβ1-40 levels among these patients. These results are reasonable since Aβ1-42 is the major form of Aβ aggregated and deposited in the brains of patients with DS.
We found significantly increased blood Aβ1-40 and Aβ1-42 levels in patients with DS and significantly decreased CSF Aβ1-42, but not Aβ1-40, levels in patients with DS. However, this meta-analysis had several limitations. First, there was a small number of studies analyzing CSF Aβ levels in patients with DS; therefore, future studies are necessary to strengthen our conclusions. Notably, CSF Aβ1-42 levels were significant reduced in patients with DSD compared with those in patients with DS and with a large ES, suggesting that CSF Aβ1-42 might be a biomarker for the prediction and/or diagnosis of dementia in patients with DS. Future studies are required to validate this hypothesis. Second, it is unclear how age affected the between-study heterogeneity in the meta-analysis of blood Aβ levels. It is possible that the low between-study heterogeneities observed in the old group were due to the small number of studies measuring blood Aβ1-42 and Aβ1-40 levels in this sub-group. Third, despite exhaustively searching PubMed and Web of Science, we might have missed some eligible studies. However, our analyses suggested that publication bias was unlikely to affect the outcomes of our meta-analysis, indicating the robustness of our findings.
Materials and Methods
We used the guidelines recommended by the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statement to perform this meta-analysis [24].
Search strategy and study selection
Two investigators independently performed a systematic review of English-language articles from the PubMed and Web of Science databases through April 2019. We searched the databases without year limitation and used the following search terms: (Down syndrome) AND (amyloid-beta OR Abeta OR Aβ). We included studies that compared circulating Aβ1-42 and/or Aβ1-40 levels between patients with DS and HC subjects or between patients with DS and those with DSD. The original search identified a total of 736 publications from PubMed and 525 publications from Web of Science. After reviewing titles and abstracts, 50 full-text articles were identified and assessed for quantitative analysis eligibility. Among the 50 articles, 23 articles were excluded for the following reasons: 13 lacked the necessary data, 2 were review articles, 3 only had one subject group, 2 analyzed post-mortem samples, 2 analyzed blood exosome samples, and 1 had overlapping samples with another study. Thus, we included a final 27 articles in the current meta-analysis [6–21, 25–35] (Flowchart see Figure 4).
Data extraction
We extracted data on sample size, mean Aβ1-42 and Aβ1-40 levels, Aβ1-42/Aβ1-40 ratio, standard deviation (s.d), and p-values as primary outcomes. We also extracted data on the average ages, gender distribution, sample sources (blood or cerebrospinal fluid), assay type, region of studies, and publication year. Two investigators independently extracted the data and any inconsistencies in the extracted data were settled by discussion. Supplementary Table 1 summarizes the demographic and clinical characteristics in the included studies.
Statistical analysis
The Comprehensive Meta-Analysis Version 2 software (Biostat, Englewood, NJ, USA) was used for the meta-analysis. We primarily used the sample sizes, mean Aβ levels, and s.d. to generate effective sizes (ESs). In some studies, sample sizes and P values were used to generate ESs as mean Aβ levels and the s.d. were not available. We calculated the ESs as the standardized between-group mean difference in the Aβ1-42 and Aβ1-40 levels and converted to Hedge's g, which provides an unbiased ES adjusted for sample size. The 95% confidence interval (CI) was used to assess statistical differences in the pooled ES. We chose random-effects models for the meta-analysis since we hypothesized that within-study and between-study moderators would result in differences in the true ES [24]. We performed sensitivity analysis by removing one study at a time to test whether a particular study significantly affected the outcomes of the meta-analysis.
Statistical differences in the across-study heterogeneity were assessed using Cochran Q test [36] with the statistical significance set at P value < 0.1. The across-study inconsistency was determined by the I2 index to evaluate the impact of heterogeneity. An I2 of 0.25, 0.50, and 0.75 suggested small, moderate, and high levels of heterogeneity, respectively [37]. Next, we used unrestricted maximum-likelihood random-effects meta-regression of the ES [38] to assess whether potential moderators including mean age, gender distribution (male proportion), and publication year affected the ES. Funnel plots generated by plotting the ES against the study precision (inverse of standard error) were used for visual inspection of publication bias. A statistical test for significance of publication bias was determined by Egger’s test [39], which assesses the degree of funnel plot asymmetry. Classic fail-safe N, which is an analysis of the number of missing (unpublished) studies that allow the observed P value to reach > 0.05, was also used to investigate publication bias.
All statistical significances were set at P value > 0.05 except where otherwise noted.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflicts of interest.
Funding
This study was supported by the National Natural Science Foundation of China (81703492), Beijing Natural Science Foundation (7182092), the Minzu University Research Fund (2018CXTD03) and the MUC 111 project.
References
- 1. Coppus A, Evenhuis H, Verberne GJ, Visser F, van Gool P, Eikelenboom P, van Duijin C. Dementia and mortality in persons with Down’s syndrome. J Intellect Disabil Res. 2006; 50:768–77. https://doi.org/10.1111/j.1365-2788.2006.00842.x [PubMed]
- 2. Schupf N, Sergievsky GH. Genetic and host factors for dementia in Down’s syndrome. Br J Psychiatry. 2002; 180:405–10. https://doi.org/10.1192/bjp.180.5.405 [PubMed]
- 3. Beyreuther K, Pollwein P, Multhaup G, Mönning U, König G, Dyrks T, Schubert W, Masters CL. Regulation and expression of the Alzheimer’s beta/A4 amyloid protein precursor in health, disease, and Down’s syndrome. Ann N Y Acad Sci. 1993; 695:91–102. https://doi.org/10.1111/j.1749-6632.1993.tb23035.x [PubMed]
- 4. Selkoe DJ. Normal and abnormal biology of the beta-amyloid precursor protein. Annu Rev Neurosci. 1994; 17:489–517. https://doi.org/10.1146/annurev.ne.17.030194.002421 [PubMed]
- 5. Olsson B, Lautner R, Andreasson U, Öhrfelt A, Portelius E, Bjerke M, Hölttä M, Rosén C, Olsson C, Strobel G, Wu E, Dakin K, Petzold M, et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: a systematic review and meta-analysis. Lancet Neurol. 2016; 15:673–84. https://doi.org/10.1016/S1474-4422(16)00070-3 [PubMed]
- 6. Cavani S, Tamaoka A, Moretti A, Marinelli L, Angelini G, Di Stefano S, Piombo G, Cazzulo V, Matsuno S, Shoji S, Furiya Y, Zaccheo D, Dagna-Bricarelli F, et al. Plasma levels of amyloid beta 40 and 42 are independent from ApoE genotype and mental retardation in Down syndrome. Am J Med Genet. 2000; 95:224–28. https://doi.org/10.1002/1096-8628(20001127)95:3<224::AID-AJMG7>3.0.CO;2-B [PubMed]
- 7. Mehta PD, Mehta SP, Fedor B, Patrick BA, Emmerling M, Dalton AJ. Plasma amyloid beta protein 1-42 levels are increased in old Down Syndrome but not in young Down Syndrome. Neurosci Lett. 2003; 342:155–58. https://doi.org/10.1016/S0304-3940(03)00275-1 [PubMed]
- 8. Mehta PD, Capone G, Jewell A, Freedland RL. Increased amyloid beta protein levels in children and adolescents with Down syndrome. J Neurol Sci. 2007; 254:22–27. https://doi.org/10.1016/j.jns.2006.12.010 [PubMed]
- 9. Schupf N, Patel B, Silverman W, Zigman WB, Zhong N, Tycko B, Mehta PD, Mayeux R. Elevated plasma amyloid beta-peptide 1-42 and onset of dementia in adults with Down syndrome. Neurosci Lett. 2001; 301:199–203. https://doi.org/10.1016/S0304-3940(01)01657-3 [PubMed]
- 10. Tokuda T, Fukushima T, Ikeda S, Sekijima Y, Shoji S, Yanagisawa N, Tamaoka A. Plasma levels of amyloid beta proteins Abeta1-40 and Abeta1-42(43) are elevated in Down’s syndrome. Ann Neurol. 1997; 41:271–73. https://doi.org/10.1002/ana.410410220 [PubMed]
- 11. Bartha JL, Soothill PW. Plasma amyloid beta protein 1-42 levels in fetuses with Down syndrome. Early Hum Dev. 2005; 81:351–54. https://doi.org/10.1016/j.earlhumdev.2004.09.003 [PubMed]
- 12. Mehta PD, Patrick BA, Dalton AJ, Patel B, Mehta SP, Pirttila T, Coyle PK. Increased serum neopterin levels in adults with Down syndrome. J Neuroimmunol. 2005; 164:129–33. https://doi.org/10.1016/j.jneuroim.2005.03.010 [PubMed]
- 13. Obeid R, Hübner U, Bodis M, Geisel J. Plasma Amyloid Beta 1-42 and DNA Methylation Pattern Predict Accelerated Aging in Young Subjects with Down Syndrome. Neuromolecular Med. 2016; 18:593–601. https://doi.org/10.1007/s12017-016-8413-y [PubMed]
- 14. Schupf N, Patel B, Pang D, Zigman WB, Silverman W, Mehta PD, Mayeux R. Elevated plasma beta-amyloid peptide Abeta(42) levels, incident dementia, and mortality in Down syndrome. Arch Neurol. 2007; 64:1007–13. https://doi.org/10.1001/archneur.64.7.1007 [PubMed]
- 15. Jones EL, Hanney M, Francis PT, Ballard CG. Amyloid beta concentrations in older people with Down syndrome and dementia. Neurosci Lett. 2009; 451:162–64. https://doi.org/10.1016/j.neulet.2008.12.030 [PubMed]
- 16. Matsuoka Y, Andrews HF, Becker AG, Gray AJ, Mehta PD, Sano MC, Dalton AJ, Aisen PS. The relationship of plasma Abeta levels to dementia in aging individuals with Down syndrome. Alzheimer Dis Assoc Disord. 2009; 23:315–18. https://doi.org/10.1097/WAD.0b013e3181aba61e [PubMed]
- 17. Lee NC, Yang SY, Chieh JJ, Huang PT, Chang LM, Chiu YN, Huang AC, Chien YH, Hwu WL, Chiu MJ. Blood Beta-Amyloid and Tau in Down Syndrome: A Comparison with Alzheimer’s Disease. Front Aging Neurosci. 2017; 8:316. https://doi.org/10.3389/fnagi.2016.00316 [PubMed]
- 18. Iulita MF, Ower A, Barone C, Pentz R, Gubert P, Romano C, Cantarella RA, Elia F, Buono S, Recupero M, Romano C, Castellano S, Bosco P, et al. An inflammatory and trophic disconnect biomarker profile revealed in Down syndrome plasma: relation to cognitive decline and longitudinal evaluation. Alzheimers Dement. 2016; 12:1132–48. https://doi.org/10.1016/j.jalz.2016.05.001 [PubMed]
- 19. Schupf N, Zigman WB, Tang MX, Pang D, Mayeux R, Mehta P, Silverman W. Change in plasma Aß peptides and onset of dementia in adults with Down syndrome. Neurology. 2010; 75:1639–44. https://doi.org/10.1212/WNL.0b013e3181fb448b [PubMed]
- 20. Fortea J, Carmona-Iragui M, Benejam B, Fernández S, Videla L, Barroeta I, Alcolea D, Pegueroles J, Muñoz L, Belbin O, de Leon MJ, Maceski AM, Hirtz C, et al. Plasma and CSF biomarkers for the diagnosis of Alzheimer’s disease in adults with Down syndrome: a cross-sectional study. Lancet Neurol. 2018; 17:860–69. https://doi.org/10.1016/S1474-4422(18)30285-0 [PubMed]
- 21. Carmona-Iragui M, Balasa M, Benejam B, Alcolea D, Fernández S, Videla L, Sala I, Sánchez-Saudinós MB, Morenas-Rodriguez E, Ribosa-Nogué R, Illán-Gala I, Gonzalez-Ortiz S, Clarimón J, et al. Cerebral amyloid angiopathy in Down syndrome and sporadic and autosomal-dominant Alzheimer’s disease. Alzheimers Dement. 2017; 13:1251–60. https://doi.org/10.1016/j.jalz.2017.03.007 [PubMed]
- 22. Lemere CA, Blusztajn JK, Yamaguchi H, Wisniewski T, Saido TC, Selkoe DJ. Sequence of deposition of heterogeneous amyloid beta-peptides and APO E in Down syndrome: implications for initial events in amyloid plaque formation. Neurobiol Dis. 1996; 3:16–32. https://doi.org/10.1006/nbdi.1996.0003 [PubMed]
- 23. Leverenz JB, Raskind MA. Early amyloid deposition in the medial temporal lobe of young Down syndrome patients: a regional quantitative analysis. Exp Neurol. 1998; 150:296–304. https://doi.org/10.1006/exnr.1997.6777 [PubMed]
- 24. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009; 62:e1–34. https://doi.org/10.1016/j.jclinepi.2009.06.006 [PubMed]
- 25. Conti E, Galimberti G, Piazza F, Raggi ME, Ferrarese C. Increased soluble APPalpha, Abeta 1-42, and anti-Abeta 1-42 antibodies in plasma from down syndrome patients. Alzheimer Dis Assoc Disord. 2010; 24:96–100. https://doi.org/10.1097/WAD.0b013e3181aba63a [PubMed]
- 26. Coppus AM, Schuur M, Vergeer J, Janssens AC, Oostra BA, Verbeek MM, van Duijn CM. Plasma β amyloid and the risk of Alzheimer’s disease in Down syndrome. Neurobiol Aging. 2012; 33:1988–94. https://doi.org/10.1016/j.neurobiolaging.2011.08.007 [PubMed]
- 27. Head E, Doran E, Nistor M, Hill M, Schmitt FA, Haier RJ, Lott IT. Plasma amyloid-β as a function of age, level of intellectual disability, and presence of dementia in Down syndrome. J Alzheimers Dis. 2011; 23:399–409. https://doi.org/10.3233/JAD-2010-101335 [PubMed]
- 28. Bourque PR, Lach B, Carpenter S, Rippstein P. Myopathy with hexagonally cross-linked tubular arrays: a new autosomal dominant or sporadic congenital myopathy. Ann Neurol. 1999; 45:512–15. https://doi.org/10.1002/1531-8249(199904)45:4<512::AID-ANA13>3.0.CO;2-5 [PubMed]
- 29. Mehta PD, Dalton AJ, Mehta SP, Kim KS, Sersen EA, Wisniewski HM. Increased plasma amyloid beta protein 1-42 levels in Down syndrome. Neurosci Lett. 1998; 241:13–16. https://doi.org/10.1016/S0304-3940(97)00966-X [PubMed]
- 30. Mehta PD, Patrick BA, Barshatzky M, Mehta SP, Frackowiak J, Mazur-Kolecka B, Miller DL. Generation of Rabbit Monoclonal Antibody to Amyloid-β38 (Aβ38): Increased Plasma Aβ38 Levels in Down Syndrome. J Alzheimers Dis. 2015; 46:1021–32. https://doi.org/10.3233/JAD-142592 [PubMed]
- 31. Portelius E, Soininen H, Andreasson U, Zetterberg H, Persson R, Karlsson G, Blennow K, Herukka SK, Mattsson N. Exploring Alzheimer molecular pathology in Down’s syndrome cerebrospinal fluid. Neurodegener Dis. 2014; 14:98–106. https://doi.org/10.1159/000358800 [PubMed]
- 32. Prasher VP, Sajith SG, Mehta P, Zigman WB, Schupf N. Plasma beta-amyloid and duration of Alzheimer’s disease in adults with Down syndrome. Int J Geriatr Psychiatry. 2010; 25:202–07. https://doi.org/10.1002/gps.2321 [PubMed]
- 33. Startin CM, Ashton NJ, Hamburg S, Hithersay R, Wiseman FK, Mok KY, Hardy J, Lleó A, Lovestone S, Parnetti L, Zetterberg H, Hye A, Strydom A, and LonDownS Consortium. Plasma biomarkers for amyloid, tau, and cytokines in Down syndrome and sporadic Alzheimer’s disease. Alzheimers Res Ther. 2019; 11:26. https://doi.org/10.1186/s13195-019-0477-0 [PubMed]
- 34. Tamaoka A, Sekijima Y, Matsuno S, Tokuda T, Shoji S, Ikeda SI. Amyloid beta protein species in cerebrospinal fluid and in brain from patients with Down’s syndrome. Ann Neurol. 1999; 46:933. https://doi.org/10.1002/1531-8249(199912)46:6<933::AID-ANA20>3.0.CO;2-4 [PubMed]
- 35. Tapiola T, Soininen H, Pirttilä T. CSF tau and Abeta42 levels in patients with Down’s syndrome. Neurology. 2001; 56:979–80. https://doi.org/10.1212/WNL.56.7.979 [PubMed]
- 36. Bowden J, Tierney JF, Copas AJ, Burdett S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med Res Methodol. 2011; 11:41. https://doi.org/10.1186/1471-2288-11-41 [PubMed]
- 37. Masi A, Quintana DS, Glozier N, Lloyd AR, Hickie IB, Guastella AJ. Cytokine aberrations in autism spectrum disorder: a systematic review and meta-analysis. Mol Psychiatry. 2015; 20:440–46. https://doi.org/10.1038/mp.2014.59 [PubMed]
- 38. Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. 1997; 127:820–26. https://doi.org/10.7326/0003-4819-127-9-199711010-00008 [PubMed]
- 39. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34. https://doi.org/10.1136/bmj.315.7109.629 [PubMed]