



Introduction
Given the high prevalence rate and the prohibitive spending of maintenance renal replacement therapy, chronic kidney disease (CKD) has become a major public health problem and received increasing attention worldwide [1]. Subjects with CKD are at risk of accelerated cardiovascular disease and related death, even in the early stage. Screening for individuals at high risk of renal impairment is an effective strategy for CKD management.
Several epidemiological studies have shown that increasing parity may affect the health of women later in life. Vaidya et al. [2] reported a strong association of parity history with lower carotid artery distensibility. Their findings suggested that arterial remodeling lasts beyond giving birth, which may explain the association of parity with cardiovascular events in later life. It is reported that parity degree was associated with increased risk of metabolic syndrome in women aged 50 years or older [3]. Recent studies also indicated that parity degree is independently associated with increased risk of both hypertension and diabetes, which will result in a greater burden of CKD among parous women [4, 5]. Compared with non-pregnant values, GFR was reduced in early pregnancy but increased significantly during the final trimester of pregnancy due to the volume expansion in the stage [6]. Consequently, in women with previous preexisting kidney damage, glomerular hyper-filtration in the last trimester of pregnancy would go beyond the scope of renal compensation and trigger rapid progression of nephropathy [1]. In addition, multiparous women had marked fluctuation in estrogen and other anti-insulin hormones, and could promote the development and pathogenesis of kidney damage [7–10].
In light of the above perspectives, we assumed that parity degree may have potential effect on the presence and progression of renal impairment. However, little is known concerning the association between parity degree and CKD. Therefore, in the present study, we analyzed data from a Chinese population to explore the possible association of parity with albuminuria and CKD.
Results
Clinical characteristics of the study population
The mean age was 55.2 ± 7.7 years among the 6,946 enrolled women. In total, 64.6% (4,489) of women were one-child birth and 12.5% (869) of women were nulliparous. There were 451 (6.5%) subjects categorized as increased urinary albumin excretion and 511 (7.4%) subjects categorized as CKD, respectively. Table 1 shows the clinical and biochemical characteristics of the participants according to parity degree. Parous women with higher parity number had increased age, BMI, WC, SBP, FPG, fasting insulin, and decreased HDL-C, eGFR and education levels. Compared with women giving one live birth in their life, nulliparous women were older and had higher TC, LDL-C, γ-GGT, proportions of current smokers, proportions of current drinkers and decreased eGFR levels.
Table 1. Characteristics of study population by parity degree.
| Number of Parity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | 1 | 2 | ≥ 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| n (%) | 869 (12.5) | 4489 (64.6) | 1069 (15.4) | 519 (7.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Urinary ACR (mg/g) | 8.25 (5.92 – 12.25) | 8.33 (5.97 – 12.19) | 9.16 (6.51 – 13.73)#, & | 10.46 (6.66 – 16.32)#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | 54.4 ± 7.2# | 53.4 ± 5.7& | 58.2 ± 8.8#, & | 65.6 ± 10.9#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 23.3 ± 3.3 | 23.4 ± 3.4 | 24.2 ± 3.3#, & | 24.6 ± 3.8#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WC (cm) | 79.5 ± 10.0 | 79.5 ± 8.8 | 82.6 ± 9.3#, & | 84.9 ± 9.4#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP (mmHg) | 124.2 ± 15.6 | 123.4 ± 15.8 | 128.2 ± 16.9#, & | 133.0 ± 17.4#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DBP (mmHg) | 74.4 ± 9.3 | 74.1 ± 9.6 | 75.0 ± 9.7# | 74.7 ± 9.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoking [n (%)] | 22 (2.8)# | 42 (1.0)& | 12 (1.1)& | 11 (2.1)# | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current drinking [n (%)] | 15 (2.1)# | 48 (1.1)& | 17 (1.6) | 6 (1.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG (mmol/L) | 1.28 (0.94 – 1.81)# | 1.20 (0.88 – 1.71)& | 1.31 (0.98 – 1.86) # | 1.44 (1.00 – 2.01) #, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC (mmol/L) | 5.44 ± 1.25# | 5.24 ± 1.28& | 5.25 ± 1.27 | 5.23 ± 1.26& | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C (mmol/L) | 1.41 ± 0.36 | 1.38 ± 0.37 | 1.35 ± 0.35& | 1.28 ± 0.34#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C (mmol/L) | 3.26 ± 0.96# | 3.16 ± 0.98& | 3.17 ± 0.96 | 3.15 ± 0.95 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FPG (mmol/L) | 5.37 (4.94 – 5.88) | 5.35 (4.96 – 5.81) | 5.51 (5.07 – 6.03)#, & | 5.63 (5.14 – 6.20)#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fasting insulin (μIU/ml) | 7.20 (5.20 – 9.90) | 7.10 (5.30 – 9.80) | 7.90 (5.90 – 11.00)#, & | 8.20 (5.90 – 11.30)#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| γ-GGT (U/L) | 19.0 (14.0 – 27.0)# | 17.0 (13.0 – 25.0)& | 19.0 (14.0 – 27.0) | 19.0 (14.0 – 26.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR (ml/min per 1.73 m2) | 102.9 ± 23.0# | 105.9 ± 24.2& | 102.1 ± 21.4# | 96.5 ± 23.0#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical activity (MET-h/week) | 10.5 (0.0 – 36.0) | 25.0 (12.0 – 49.0) | 28.0 (12.0 – 49.0) | 21.0 (10.5 – 42.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Spontaneous abortion [n (%)] | 30 (3.5)# | 279 (6.2)& | 76 (7.1)& | 63 (12.1)#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Menopause [n (%)] | 431 (75.0) | 3247 (73.4) | 847 (80.4)#, & | 456 (88.2)#, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High school or higher education [n (%)] | 490 (70.8) | 3057 (68.7) | 399 (37.9) #, & | 62 (12.1) #, & | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1. Data were means ± SD or medians (interquartile ranges) for skewed variables or numbers (proportions) for categorical variables; P values were for the ANOVA or χ2 analyses across the groups. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2. # P < 0.05 compared with participants with one live birth (parity number = 1 group); & P < 0.05 compared with participants with no live birth (parity number = 0 group). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3. ACR, albumin to creatinine ratio; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; FPG, fasting plasma glucose; γ-GGT, γ-glutamyltransferase; eGFR, estimated glomerular filtration rate. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Associations of parity degree with increased urinary albumin excretion and CKD
Among parity number in 0, 1, 2 and ≥ 3 groups, the prevalence of increased urinary albumin excretion were 5.6%, 5.6%, 8.2% and 11.8% while the prevalence of CKD were 6.9%, 6.0%, 9.5% and 15.2%, respectively (Figure 1A and 1B). Compared with women with one-child birth (parity number = 1), subjects with more than 2 live births (parity number ≥ 3) were independently associated with a greater prevalence of increased urinary albumin excretion (ORs 1.53, 95% CI, 1.03 - 2.28) and CKD (ORs 1.79, 95% CI, 1.24 - 2.58) in multivariate logistic regression analyses (Table 2). When compared nulliparous women (parity number = 0) with women with one-child birth (parity number = 1), no statistically significant difference of such associations was found.
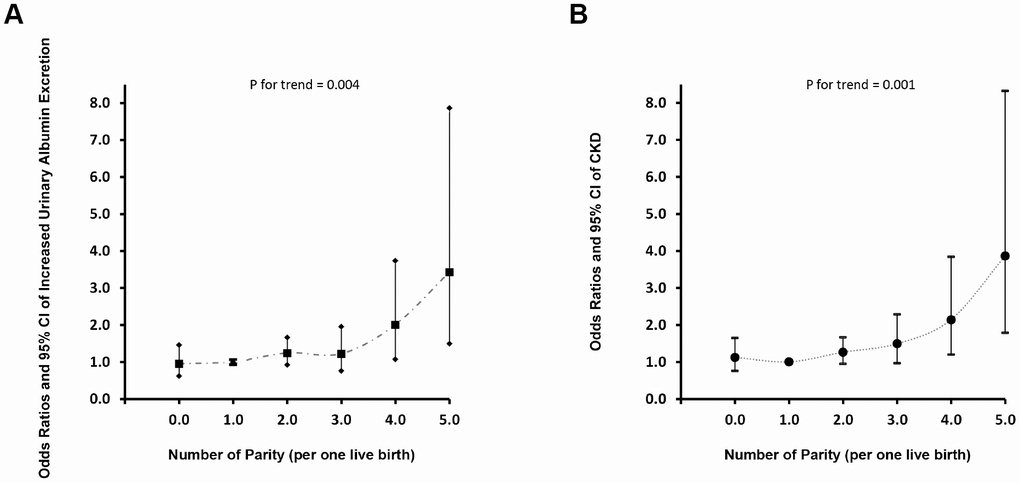
Figure 1. Dose-response analyses of parity number with increased urinary albumin excretion and CKD. (A) Increased Urinary Albumin Excretion; (B) CKD.
Table 2. The risk of prevalent increased urinary albumin excretion and CKD according to parity degree.
| Number of Parity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | 1 | 2 | ≥ 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increased urinary albumin excretion | Model 1 | 1.00 (0.73 – 1.37) | 1 | 1.50 (1.17 – 1.93) | 2.23 (1.66 – 3.00) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 2 | 0.99 (0.72 – 1.35) | 1 | 1.42 (1.09 – 1.84) | 1.91 (1.36 – 2.69) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 3 | 0.96 (0.63 – 1.47) | 1 | 1.23 (0.92 – 1.65) | 1.55 (1.06 – 2.28) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 4 | 0.95 (0.62 – 1.45) | 1 | 1.22 (0.91 – 1.64) | 1.53 (1.03 – 2.28) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CKD | Model 1 | 1.15 (0.86 – 1.54) | 1 | 1.62 (1.28 – 2.06) | 2.80 (2.14 – 3.66) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 2 | 1.12 (0.84 – 1.50) | 1 | 1.42 (1.10 – 1.82) | 2.10 (1.53 – 2.88) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 3 | 1.13 (0.77 – 1.66) | 1 | 1.26 (0.95 – 1.66) | 1.86 (1.30 – 2.64) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 4 | 1.11 (0.75 – 1.64) | 1 | 1.25 (0.94 – 1.66) | 1.79 (1.24 – 2.58) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data are odds ratios (95% confidence interval). Participants without increased urinary albumin excretion or CKD are defined as 0 and with increased urinary albumin excretion or CKD as 1. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 1 is unadjusted. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 2 is adjusted for age. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 3 is further adjusted for BMI, current smoking status, current drinking status, education levels and physical activity. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 4 is further adjusted for SBP, TG, LDL-C, FPG and fasting insulin. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Subgroups and dose-response analysis of parity degree with increased urinary albumin excretion and CKD
The associations of parity degree with increased urinary albumin excretion and CKD were inconsistent in subgroups analyses (Table 3). In overweight and no spontaneous abortion history subgroup, women with more than 2 live births were independently associated with a greater prevalence of increased urinary albumin excretion and CKD when compared with those with one-child birth. In dose-response analysis, nonlinear associations of parity degree with both increased urinary albumin excretion and CKD were found and higher parity number seems to remarkably increased prevalent albuminuria and CKD (Figure 2A and 2B).
Table 3. Association of prevalent increased urinary albumin excretion and CKD with parity degree in different subgroups.
| Number of Parity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | 1 | 2 | ≥ 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increased urinary albumin excretion | BMI | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Normal | 0.90 (0.49 – 1.64) | 1 | 1.08 (0.67 – 1.72) | 1.72 (0.92 – 3.20) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overweight | 0.90 (0.44 – 1.87) | 1 | 1.05 (0.66 – 1.67) | 2.04 (1.15 – 3.59) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity | 1.38 (0.41 – 4.70) | 1 | 2.29 (1.10 – 4.75) | 0.32 (0.09 – 1.17) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Spontaneous abortion | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 2.28 (0.43 – 12.02) | 1 | 0.92 (0.23 – 3.73) | 2.49 (0.59 – 10.51) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 0.90 (0.58 – 1.40) | 1 | 1.27 (0.94 – 1.71) | 1.53 (1.01 – 2.31) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Menopause | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 1.04 (0.63 – 1.71) | 1 | 1.10 (0.78 – 1.54) | 1.23 (0.78 – 1.95) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 0.81 (0.31 – 2.13) | 1 | 1.39 (0.73 – 2.66) | 2.01 (0.77 – 5. 25) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR (ml/min per 1.73 m2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR ≥ 90 | 0.74 (0.42 – 1.31) | 1 | 1.27 (0.90 – 1.79) | 1.29 (0.77 – 2.17) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 90 > eGFR ≥ 60 | 1.59 (0.78 – 3.24) | 1 | 1.19 (0.64 – 2.20) | 2.45 (1.18 – 5.09) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR < 60 | 0.19 (0.01 – 3.55) | 1 | 0.25 (0.03 – 2.07) | 0.01 (0.00 – 0.40) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CKD | BMI | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Normal | 1.03 (0.60 – 1.78) | 1 | 1.03 (0.66 – 1.62) | 2.27 (1.30 – 3.98) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overweight | 1.22 (0.64 – 2.34) | 1 | 1.17 (0.76 – 1.83) | 2.09 (1.21 – 3.61) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity | 1.23 (0.36 – 4.17) | 1 | 2.21 (1.09 – 4.50) | 0.42 (0.13 – 1.37) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Spontaneous abortion | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 2.18 (0.42 – 11.44) | 1 | 0.98 (0.27 – 3.59) | 2.52 (0.64 – 9.98) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 1.08 (0.72 – 1.61) | 1 | 1.28 (0.96 – 1.71) | 1.79 (1.22 – 2.63) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Menopause | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 1.02 (0.63 – 1.65) | 1 | 1.16 (0.84 – 1.60) | 1.59 (1.04 – 2.43) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 0.81 (0.31 – 2.13) | 1 | 1.39 (0.73 – 2.66) | 2.01 (0.77 – 5.25) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data are odds ratios (95% confidence interval). Participants without increased urinary albumin excretion or CKD are defined as 0 and with increased urinary albumin excretion or CKD as 1. Odds ratios were adjusted for age, BMI, current smoking status, current drinking status, education levels, physical activity, SBP, TG, LDL-C, FPG and fasting insulin. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
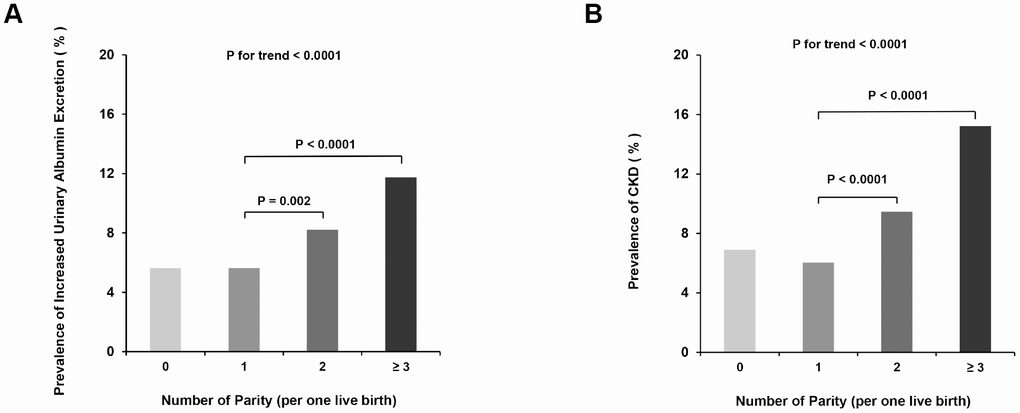
Figure 2. Prevalence of increased urinary albumin excretion and CKD according to elevated parity degree. (A) Increased Urinary Albumin Excretion; (B) CKD.
Discussion
In summary, we found that parity degree is associated with higher prevalence of albuminuria and CKD among Chinese women aged 40 years or older. To the best of our knowledge, this is the first population-based study to reveal associations of parity degree with prevalent albuminuria and CKD.
Pregnancy has a long-term influence on women’s health that result from the remarkable metabolic alterations in endocrine and immune system. In the field of kidney disease, only one study has reported on the relationship between parity and risk of death from chronic renal failure (CRF) at the present [11]. In that study, parity may have protective effect on the risk of death from CRF. However, in this particular study, there were only 225 CRF deaths during 34,980,246 person-years of follow-up. As data on the accuracy of CRF diagnosis is unavailable, the potential for misclassification of CRF is one serious limitation of the study. In fact, high parity degree is often cited as adverse risk factors for metabolic related diseases [3–5]. The finding of present study indicated that parity degree, as a risk factor for hypertension and diabetes, is associated with albuminuria and CKD in a dose-response manner, which should be considered in early prevention of renal disease.
Subgroup analysis of the association between parity degree and CKD highlights the importance of paying attention to BMI categories in multiparous women. In BMI < 28 subgroups (normal and overweight women), we found that higher parity degree was significantly associated with increasing prevalent CKD. As BMI ≥ 28 (obese) resulted in greater-grade manifestation of adipose tissue accumulation, it is likely that there are more unmeasured metabolic risk factors in this subgroup, some of which might correlate with parity degree and dilute the main findings of this study. Another possible reason for the inconsistent effect in BMI categories is that women who had more children and currently obese were general healthier than those who had less children, and also they had less risk of prevalent CKD. However, the underlying mechanism remains unexplained and requires further exploration. Seneviratne et al. [12] have recently reported that nulliparous and multiparous women may confer subtle metabolic disadvantage in overweight and obese mothers and their offspring. In our study, nulliparous women and women with two live birth may have similar magnitude of association with CKD, although the associations were not statistical significant. Therefore, caution should be taken in interpreting the results among these subgroups, especially in nulliparous overweight and obese women. Moreover, controversy remains regarding the underlying disease in nulliparous women. Possible conditions such as autoimmune and endocrine diseases were associated with albuminuria and CKD, which could preclude women from pregnancy or childbearing. Longitudinal studies performed through excluding such preexisting diseases will be necessary to verify the present findings in nulliparous women.
Mechanism responsible for elevated CKD risk caused by parity remains uncertain and some biologic hypotheses have been proposed. The balance between matrix metalloproteinases (MMP) and tissue inhibitors of metalloproteinases (TIMP) played a crucial role in degradation and remodeling of extracellular matrix and angiogenesis [13, 14]. During pregnancy, abnormalities of the matrix metalloproteinase system could result in hypoxia, oxidative stress, inflammatory response and proteinuria, which may be involved in the pathophysiology of systemic renal arteries remodeling [15–17]. Insulin resistance correlated linearly with decline in renal function and occurs in patients with CKD at different stages of kidney impairment [18, 19]. The levels of various anti-insulin hormones increased in fertile women and involved in promoting insulin resistance and the pathophysiology of arterial hypertension and angiogenesis [10, 20]. Accordingly, long lasting exposure to high levels of anti-insulin hormones during the multiple parity may therefore as a risk factor linking decreased renal function.
The study had several limitations that require further consideration. First, all clinical and biochemical measurements were collected at the same time of outcome measurement. Hence, owing to the nature of observational design of the current study, we should be cautious regarding the interpretation of whether parity is a causal factor of increased urinary albumin excretion and CKD. Second, the creatinine alteration present for more than 3 months is a part of the CKD definition. However, we evaluated serum creatinine and urinary albumin excretion on the basis of a single measurement, which may result in overestimation of the prevalence of CKD. Third, the original population of the present study is a female dominant population. Partially because participants in baseline the survey were all over 40 years and females were accounted for most proportion in this age range. Fourth, disorders during the pregnancies or abnormal obstetrical outcomes, i.e., preeclampsia, preterm labor, gestational diabetes mellitus and acute kidney injury are related to progressive renal function impairment. Preeclampsia is one of the challenge during pregnancy, which could cause transitory kidney damage and increased risk of developing CKD later in life [21, 22]. Moreover, acute kidney injury (AKI) in pregnancy is often caused by preeclampsia or eclampsia [23]. Although most patients with AKI are reported to have renal function recovery, more than 10% of these patients will still progress to CKD during follow-up [24, 25]. Missing of these data may influence result interpreting in the study. Fifth, incomplete data compilation may influence the interpretation of the result of this study. Therefore, more detailed information of previous nephropathy history, salt consumption, personal income levels and nutrition and lifestyle in pregnancy should be considered to collect to strength the findings of the present study.
In conclusion, our study highlights the importance of paying more attention to early kidney damage in women with higher frequency of pregnancy. Further prospective studies are necessary to verify our findings in other countries and ethnic groups.
Materials and Methods
Study population and design
The study population was taken from the Risk Evaluation of Cancers in Chinese Diabetic Individuals: A Longitudinal Study (the REACTION Study), and details of this cohort have been published previously [26–28]. Baseline survey of the REACTION study recruited nearly 260,000 subjects from 25 communities across mainland China between the year 2011 and 2012. The communities were selected from different regions in both urban and rural sites, with distinct degrees of economic and urbanization development status. All individuals with self-care ability aged 40 years and older were allowed to participate in the baseline survey and included in the study.
We performed the present retrospective study in one of the centers from June to November, 2011 for the community located in Guangzhou, China. During the recruiting phase, a total of 10,104 residents aged 40 years or older were invited to participate by examination notices or home visits. In total, 9,916 subjects agreed to participate in the survey, and the participation rate was 98.1%. In data analyses, men (n = 2,854) were first excluded from the study. Subjects who failed to provide information (urinary albumin-to-creatinine ratio [ACR]: n = 149; serum creatinine: n = 10) were then excluded from the analyses. Accordingly, a total of 6,946 eligible women were included in the final data analyses. The details of the selection of study participants are presented in a flow diagram (Figure 3).
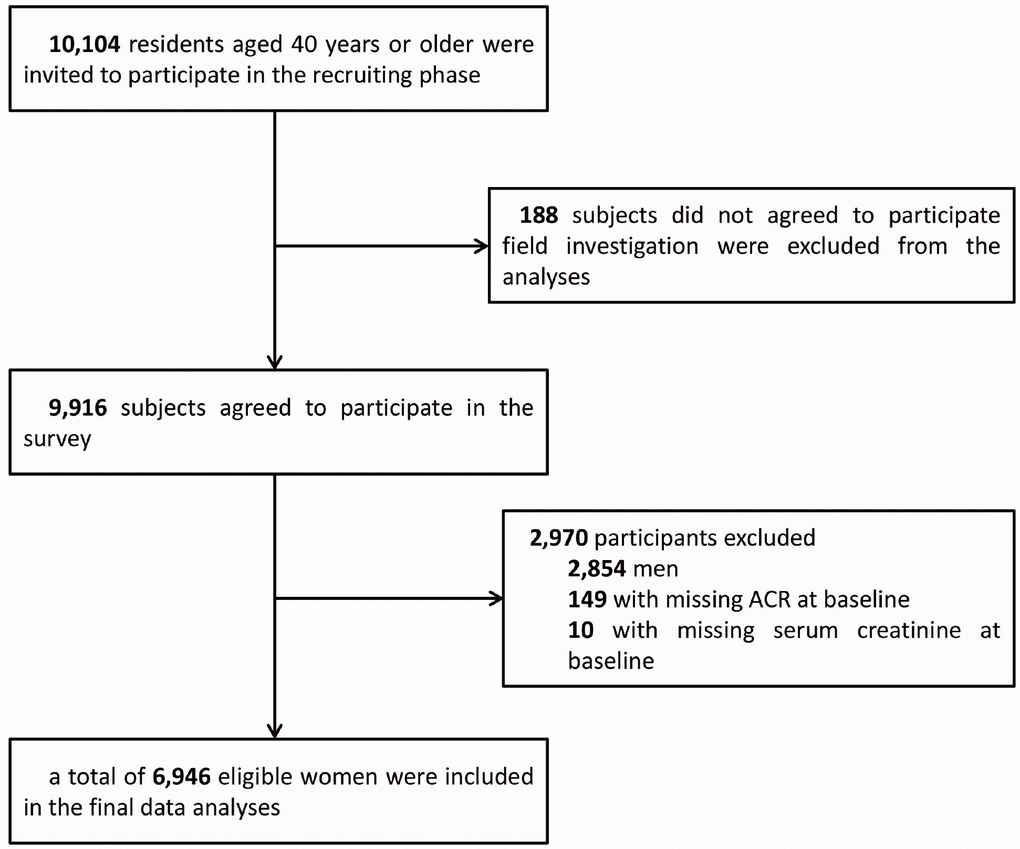
Figure 3. Flowchart of the selection of the study participant.
The study protocol was approved by the Institutional Review Board of the Sun Yat-sen Memorial Hospital, Sun Yat-sen University and was in accordance with the principle of the Helsinki Declaration II. Written informed consent was obtained from each participant before data collection.
Questionnaire investigation
Through a detailed questionnaire, we collected information on lifestyle factors and sociodemographic characteristics of each participant. Information on reproductive history was self-reported. Women were asked to recall the number of pregnancies and parity. Smoking or drinking habit was classified as ‘never’, ‘current’ (smoking or drinking regularly in the past 6 months) or ‘ever’ (cessation of smoking or drinking more than 6 months) [29]. A short form of the International Physical Activity Questionnaire (IPAQ) was used to estimate physical activity at leisure time by adding questions on frequency and duration of moderate or vigorous activities and walking [30]. Separate metabolic equivalent hours per week (MET-h/week) were calculated for evaluation of total physical activity. Education levels were categorized as less than middle school, middle school graduate and high school graduate or higher.
Clinical and biochemical measurements
All participants completed anthropometrical measurements with the assistance of trained staff by using standard protocols. Three consecutive blood pressure measurements were obtained within a 5-minute interval with automated electronic device (OMRON, Omron Company, China). The average of three measurements of blood pressure was used for analysis. Body height and weight were recorded to the nearest 0.1 cm and 0.1 kg, respectively. Participants were required to remove their shoes and wear light indoor clothing during the measurement. BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2). Reference to the local population prevalence of obesity and for the BMI threshold was used to define obesity in the study [31–34]. Accordingly, obesity was defined as BMI ≥ 28 and overweight was defined as BMI ≥ 24 and < 28. WC was measured at the umbilical level with participant in standing position, at the end of gentle expiration. Venous blood samples were collected for laboratory tests after an overnight fasting of at least 10 hours. Measurement of fasting plasma glucose (FPG), fasting serum insulin, triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), creatinine, and γ-glutamyltransferase (γ-GGT) was done using an autoanalyser (Beckman CX-7 Biochemical Autoanalyser, Brea, CA, USA).
Definition of increased urinary albumin excretion and CKD
The abbreviated Modification of Diet in Renal Disease (MDRD) formula recalibrated for Chinese population was used to calculate estimated glomerular filtration rate (GFR) expressed in ml/min per 1.73 m2 using a formula of eGFR = 175 × [serum creatinine × 0.011]-1.234 × [age]-0.179 × [0.79 if female], where serum creatinine was expressed as μmol/L [35]. Definitions of albuminuria were according to the latest guidelines of American Diabetes Association’s Standards of Medical Care [36]. The first morning spot urine samples were collected for assessing the ACR. Urine albumin and creatinine were measured by chemiluminescence immunoassay (Siemens Immulite 2000, United States) and the Jaffe’ s kinetic method (Biobase-Crystal, Jinan, China) on the automatic analyzer, respectively. ACR was calculated by dividing the urinary albumin concentrations by the urinary creatinine concentrations and expressed in mg/g. The outcome measures of the study were increased urinary albumin excretion and CKD. Increased urinary albumin excretion was defined according to the ACR ranges greater or equal than 30 mg/g. Chronic kidney disease (CKD) was defined as eGFR less than 60 mL/min per 1.73 m² or presence of albuminuria (ACR greater or equal than 30 mg/g) [37].
Statistical analysis
Continuous variables were presented as means ± standard deviation (S.D.) except for skewed variables, which were presented as medians (interquartile ranges). Categorical variables were expressed as numbers (proportions). FPG, fasting insulin, TG, γ-GGT and MET-h/week were logarithmically transformed before analysis due to a non-normal distribution. Differences among groups were tested by one-way ANOVA and post hoc comparisons were performed by using Bonferroni correction. Comparisons between categorical variables were performed with the χ2 test.
We analyzed the impact of parity on the prevalence of increased urinary albumin excretion and CKD. The unadjusted and multivariate-adjusted logistic regression analysis was used to assess the risk of prevalent increased urinary albumin excretion and CKD in relation to degree of parity. The covariates included in the multivariate-adjusted logistic regression analysis were selected based on previous publications and potential risk factors that associated with the progression of renal disease [37–39]. Model 1 is unadjusted. Model 2 is adjusted for age. Model 3 is further adjusted for BMI, current smoking status, current drinking status, education levels and physical activity. Model 4 is further adjusted for SBP, TG, LDL-C, FPG and fasting insulin. Odds ratios (ORs) and the corresponding 95% confidence intervals (95% CI) were calculated. In all logistic regression analysis, test for linear trend across groups was treating number of parity as a continuous variable. Relationship of parity with albuminuria and CKD in model 4 of logistic regression analysis was explored in subgroups stratified degree of obesity (normal/ overweight/ obese), spontaneous abortion history (yes/ no) and menopause (yes/ no). For relationship between parity and albuminuria, subgroup analysis stratified by eGFR level (≥ 90; 60-89; < 60 ml/min per 1.73 m2) was also conducted. The dose-response relationship between parity and prevalent increased urinary albumin excretion and CKD were further performed by using multivariate adjusted logistic regression analyses in model 4. In dose-response analysis, number of parities were classified as follows: 0, 1, 2, 3, 4 and ≥ 5 (per one live birth).
All statistical analysis was performed using SAS version 9.3 (SAS Institute Inc, Cary, NC, USA). Statistical tests were two-sided, and a P value < 0.05 was considered statistically significant.
Ethical standards
Protocol of the present study involved human participant was approved by the Institutional Review Board of the Sun Yat-sen Memorial Hospital, Sun Yat-sen University and was in accordance with the principle of the Helsinki Declaration II. We obtained written informed consent with permission to use the data from each participant before data collection.
Author Contributions
Conceiving ideas and experiment design: Y. L., C. Y. and K. S. Actual experimentation: F. L., Y. Q., W. F., C. H., K. S. and Q. F. Data analysis: K. S. and M. R. Manuscript writing: K.S. and M. R.
Acknowledgments
We are indebted to the participants in the present study for their outstanding support and to our colleagues for their valuable assistance.
Conflicts of Interest
The authors have declared no conflicts of interest.
Funding
This work was supported by grants from: 1. National Key R&D Program of China (No. 2016YFC0901204); 2. The National Natural Science Foundation of China (81970696, 81600642, 81471034, 8137091, 81300675); 3. Natural Science Foundation of Guangdong Province, China (2015A030310433, 2017A030313831); 4. Sun Yat-sen University Medical 2016 Youth Teacher Research Funding Project (16ykpy27); 5. Sun Yat-sen Clinical Research Cultivating Program (SYS-Q-201801); 6. Major project of the people's livelihood science and technology in Guangzhou (201300000102); 7. The 863 project of Young Scientist (SS2015 AA020927); 8. The Zhu jiang Star of science and technology Foundation in Guang Zhou (2014J220 0046); 9. Grants from the Chinese Society of Endocrinology and National Clinical Research Center for Metabolic Diseases; 10. State Key Clinical Specialty Construction Project (2011); 11. Science and Technology Planning Project of Guangdong Province, China (2014A020212161). 12. Sun Yat-sen University Clinical Research 5010 Program (2018021). These funding associations had no role in study design, data collection and analysis, decision to publish, or in the preparation of the manuscript.
References
- 1. Romagnani P, Remuzzi G, Glassock R, Levin A, Jager KJ, Tonelli M, Massy Z, Wanner C, Anders HJ. Chronic kidney disease. Nat Rev Dis Primers. 2017; 3:17088. https://doi.org/10.1038/nrdp.2017.88 [PubMed]
- 2. Vaidya D, Bennett WL, Sibley CT, Polak JF, Herrington DM, Ouyang P. Association of parity with carotid diameter and distensibility: multi-ethnic study of atherosclerosis. Hypertension. 2014; 64:253–58. https://doi.org/10.1161/HYPERTENSIONAHA.114.03285 [PubMed]
- 3. Lao XQ, Thomas GN, Jiang CQ, Zhang WS, Yin P, Schooling M, Heys M, Leung GM, Adab P, Cheng KK, Lam TH. Parity and the metabolic syndrome in older Chinese women: the Guangzhou Biobank Cohort Study. Clin Endocrinol (Oxf). 2006; 65:460–69. https://doi.org/10.1111/j.1365-2265.2006.02615.x [PubMed]
- 4. Giubertoni E, Bertelli L, Bartolacelli Y, Origliani G, Modena MG. Parity as predictor of early hypertension during menopausal transition. J Hypertens. 2013; 31:501–07. https://doi.org/10.1097/HJH.0b013e32835c1742 [PubMed]
- 5. Guo P, Zhou Q, Ren L, Chen Y, Hui Y. Higher parity is associated with increased risk of Type 2 diabetes mellitus in women: A linear dose-response meta-analysis of cohort studies. J Diabetes Complications. 2017; 31:58–66. https://doi.org/10.1016/j.jdiacomp.2016.10.005 [PubMed]
- 6. Dunlop W. Serial changes in renal haemodynamics during normal human pregnancy. Br J Obstet Gynaecol. 1981; 88:1–9. https://doi.org/10.1111/j.1471-0528.1981.tb00929.x [PubMed]
- 7. Suzuki H, Kondo K. Chronic kidney disease in postmenopausal women. Hypertens Res. 2012; 35:142–47. https://doi.org/10.1038/hr.2011.155 [PubMed]
- 8. Doublier S, Lupia E, Catanuto P, Elliot SJ. Estrogens and progression of diabetic kidney damage. Curr Diabetes Rev. 2011; 7:28–34. https://doi.org/10.2174/157339911794273982 [PubMed]
- 9. Iliescu R, Reckelhoff JF. Sex and the kidney. Hypertension. 2008; 51:1000–01. https://doi.org/10.1161/HYPERTENSIONAHA.107.101345 [PubMed]
- 10. Sattar N, Greer IA. Pregnancy complications and maternal cardiovascular risk: opportunities for intervention and screening? BMJ. 2002; 325:157–60. https://doi.org/10.1136/bmj.325.7356.157 [PubMed]
- 11. Kuo CC, Lee CT, Chen CC, Tsai SS, Yang CY. Parity, age at first birth, and risk of death from chronic renal failure: a cohort study of parous women in Taiwan. J Nephrol. 2013; 26:273–80. https://doi.org/10.5301/jn.5000171 [PubMed]
- 12. Seneviratne SN, Derraik JG, Jiang Y, McCowan LM, Gusso S, Biggs JB, Parry GK, Chiavaroli V, Cutfield WS, Hofman PL. Nulliparity is associated with subtle adverse metabolic outcomes in overweight/obese mothers and their offspring. Clin Endocrinol (Oxf). 2017; 87:545–51. https://doi.org/10.1111/cen.13426 [PubMed]
- 13. Jackson C. Matrix metalloproteinases and angiogenesis. Curr Opin Nephrol Hypertens. 2002; 11:295–99. https://doi.org/10.1097/00041552-200205000-00005 [PubMed]
- 14. Raffetto JD, Khalil RA. Matrix metalloproteinases and their inhibitors in vascular remodeling and vascular disease. Biochem Pharmacol. 2008; 75:346–59. https://doi.org/10.1016/j.bcp.2007.07.004 [PubMed]
- 15. Ab Hamid J, Mohtarrudin N, Osman M, Andi Asri AA, Wan Hassan WH, Aziz R. Matrix metalloproteinase-9 and tissue inhibitors of metalloproteinases 1 and 2 as potential biomarkers for gestational hypertension. Singapore Med J. 2012; 53:681–83. [PubMed]
- 16. Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science. 2005; 308:1592–94. https://doi.org/10.1126/science.1111726 [PubMed]
- 17. Tayebjee MH, Karalis I, Nadar SK, Beevers DG, MacFadyen RJ, Lip GY. Circulating matrix metalloproteinase-9 and tissue inhibitors of metalloproteinases-1 and -2 levels in gestational hypertension. Am J Hypertens. 2005; 18:325–29. https://doi.org/10.1016/j.amjhyper.2004.09.014 [PubMed]
- 18. Kobayashi S, Maesato K, Moriya H, Ohtake T, Ikeda T. Insulin resistance in patients with chronic kidney disease. Am J Kidney Dis. 2005; 45:275–80. https://doi.org/10.1053/j.ajkd.2004.09.034 [PubMed]
- 19. Fliser D, Pacini G, Engelleiter R, Kautzky-Willer A, Prager R, Franek E, Ritz E. Insulin resistance and hyperinsulinemia are already present in patients with incipient renal disease. Kidney Int. 1998; 53:1343–47. https://doi.org/10.1046/j.1523-1755.1998.00898.x [PubMed]
- 20. Ernst S, Demirci C, Valle S, Velazquez-Garcia S, Garcia-Ocaña A. Mechanisms in the adaptation of maternal β-cells during pregnancy. Diabetes Manag (Lond). 2011; 1:239–48. [PubMed]
- 21. Piccoli GB, Cabiddu G, Castellino S, Gernone G, Santoro D, Moroni G, Spotti D, Giacchino F, Attini R, Limardo M, Maxia S, Fois A, Gammaro L, Todros T, and Kidney and Pregnancy Study Group of Italian Society of Nephrology. A best practice position statement on the role of the nephrologist in the prevention and follow-up of preeclampsia: the Italian study group on kidney and pregnancy. J Nephrol. 2017; 30:307–17. https://doi.org/10.1007/s40620-017-0390-1 [PubMed]
- 22. Lopes van Balen VA, Spaan JJ, Cornelis T, Spaanderman ME. Prevalence of chronic kidney disease after preeclampsia. J Nephrol. 2017; 30:403–09. https://doi.org/10.1007/s40620-016-0342-1 [PubMed]
- 23. Fakhouri F, Deltombe C. Pregnancy-related acute kidney injury in high income countries: still a critical issue. J Nephrol. 2017; 30:767–71. https://doi.org/10.1007/s40620-017-0440-8 [PubMed]
- 24. Aggarwal RS, Mishra VV, Jasani AF, Gumber M. Acute renal failure in pregnancy: our experience. Saudi J Kidney Dis Transpl. 2014; 25:450–55. https://doi.org/10.4103/1319-2442.128621 [PubMed]
- 25. Prakash J, Ganiger VC, Prakash S, Iqbal M, Kar DP, Singh U, Verma A. Acute kidney injury in pregnancy with special reference to pregnancy-specific disorders: a hospital based study (2014-2016). J Nephrol. 2018; 31:79–85. https://doi.org/10.1007/s40620-017-0466-y [PubMed]
- 26. Bi Y, Lu J, Wang W, Mu Y, Zhao J, Liu C, Chen L, Shi L, Li Q, Wan Q, Wu S, Yang T, Yan L, et al. Cohort profile: risk evaluation of cancers in Chinese diabetic individuals: a longitudinal (REACTION) study. J Diabetes. 2014; 6:147–57. https://doi.org/10.1111/1753-0407.12108 [PubMed]
- 27. Ning G, and Reaction Study Group. Risk Evaluation of cAncers in Chinese diabeTic Individuals: a lONgitudinal (REACTION) study. J Diabetes. 2012; 4:172–73. https://doi.org/10.1111/j.1753-0407.2012.00182.x [PubMed]
- 28. Sun K, Li F, Qi Y, Lin D, Ren M, Xu M, Li F, Li Y, Yan L. Sex difference in the association between habitual daytime napping and prevalence of diabetes: a population-based study. Endocrine. 2016; 52:263–70. https://doi.org/10.1007/s12020-015-0772-x [PubMed]
- 29. Sun K, Liu J, Ning G. Active smoking and risk of metabolic syndrome: a meta-analysis of prospective studies. PLoS One. 2012; 7:e47791. https://doi.org/10.1371/journal.pone.0047791 [PubMed]
- 30. Tomioka K, Iwamoto J, Saeki K, Okamoto N. Reliability and validity of the International Physical Activity Questionnaire (IPAQ) in elderly adults: the Fujiwara-kyo Study. J Epidemiol. 2011; 21:459–65. https://doi.org/10.2188/jea.JE20110003 [PubMed]
- 31. Group of China Obesity Task Force. [Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents]. Zhonghua Liu Xing Bing Xue Za Zhi. 2004; 25:97–102. [PubMed]
- 32. Xi B, Liang Y, He T, Reilly KH, Hu Y, Wang Q, Yan Y, Mi J. Secular trends in the prevalence of general and abdominal obesity among Chinese adults, 1993-2009. Obes Rev. 2012; 13:287–96. https://doi.org/10.1111/j.1467-789X.2011.00944.x [PubMed]
- 33. Consultation WH, and WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004; 363:157–63. https://doi.org/10.1016/S0140-6736(03)15268-3 [PubMed]
- 34. Hu L, Huang X, You C, Li J, Hong K, Li P, Wu Y, Wu Q, Wang Z, Gao R, Bao H, Cheng X. Prevalence of overweight, obesity, abdominal obesity and obesity-related risk factors in southern China. PLoS One. 2017; 12:e0183934. https://doi.org/10.1371/journal.pone.0183934 [PubMed]
- 35. Ma YC, Zuo L, Chen JH, Luo Q, Yu XQ, Li Y, Xu JS, Huang SM, Wang LN, Huang W, Wang M, Xu GB, Wang HY. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006; 17:2937–44. https://doi.org/10.1681/ASN.2006040368 [PubMed]
- 36. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014 (Suppl 1); 37:S14–80. https://doi.org/10.2337/dc14-S014 [PubMed]
- 37. Zhang L, Wang F, Wang L, Wang W, Liu B, Liu J, Chen M, He Q, Liao Y, Yu X, Chen N, Zhang JE, Hu Z, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet. 2012; 379:815–22. https://doi.org/10.1016/S0140-6736(12)60033-6 [PubMed]
- 38. Fan F, Qi L, Jia J, Xu X, Liu Y, Yang Y, Qin X, Li J, Li H, Zhang Y, Huo Y. Noninvasive Central Systolic Blood Pressure Is More Strongly Related to Kidney Function Decline Than Peripheral Systolic Blood Pressure in a Chinese Community-Based Population. Hypertension. 2016; 67:1166–72. https://doi.org/10.1161/HYPERTENSIONAHA.115.07019 [PubMed]
- 39. Wang F, Zhang L, Wang H, and China National Survey of CKD Working Group. Awareness of CKD in China: a national cross-sectional survey. Am J Kidney Dis. 2014; 63:1068–70. https://doi.org/10.1053/j.ajkd.2014.01.012 [PubMed]