



Introduction
A 2016 statistical report indicated that the global lifetime stroke risk, for individuals ≥25 years old, is approximately 25% for both men and women; China had the highest estimated risk, at 39.3% [1]. Globally, there is a huge burden associated with strokes; there are an estimated 10.3 million new strokes, annually, accounting for 113 million disability-adjusted life years (DALYs) [2]. The stroke burden is particularly high in low- and middle-income countries where deaths associated with strokes account for approximately 75% of global stroke deaths and for >80% of DALYs; further, these countries have experienced increases in stroke incidence [3–5]. Our previous studies revealed that the incidence of first-ever stroke has been dramatically increasing in China’s rural population, especially among men aged 35–64 years, with an annual increase of 12% [6, 7].
High blood pressure (BP) is common in China, with the latest report indicating that the current prevalence of hypertension (defined as systolic BP [SBP]≥140 mmHg, diastolic BP [DBP]≥90 mmHg, or self-reported antihypertensive medication use within the previous 2 weeks) is 44.7% among residents 35–75 years old [8] and 23.2% among adults aged ≥18 years [9]. Our previous study demonstrated that the prevalence of hypertension in a rural population in 2011 was 51.7% among adults aged 35–74 years [10]. However, hypertension treatment and control rates are <50% and 20%, respectively, across different studies in China [11–14]; similarly, our study determined the treatment and control rates to be 43.8% and 12%, respectively [10].
BP is a powerful determinant of risk for both ischemic stroke (IS) and intracerebral hemorrhage (ICH). The evidence-based 2017 American College of Cardiology (ACC)/American Heart Association (AHA) Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults recommends intensive BP control for primary and secondary stroke prevention [15]. The guideline further proposes a target BP of <130/80 mmHg. In a recent meta-analysis, strong evidence indicated that BP control to <150/90 mmHg reduced stroke risk (relative risk [RR], 0.74;95% confidence interval [CI], 0.65–0.84]) and low- to moderate-strength evidence indicated that lower targets (≤140/85 mmHg) were associated with significant decreases in stroke risk (RR, 0.79;95% CI, 0.59–0.99) [16]. Recently, another report indicated that the new guidelines for the diagnosis and management of hypertension will likely influence hypertension management, globally, but especially in countries already facing an enormous public health challenge (using the previous definition of hypertension as BP ≥140/90 mmHg) [17]. However, data regarding the BP control target for reducing the stroke burden in China are scarce. In this study, we explored the optimal BP control target, according to the 2017 guideline, to decrease the risk of stroke in a population in China.
Results
Overall, 5147 individuals were ≥15yearsold, and 4218 were recruited into this survey (response rate, 82%). Of these, 4017 individuals were ultimately enrolled, after excluding 201 individuals <18 years old. During the course of the study, 108 participants were lost to follow-up, and three with missing baseline BP data were removed from the BP analysis. Finally, a total of 3906 participants were evaluated to determine the association between BP and the incidence of first-ever stroke (Figure 1).
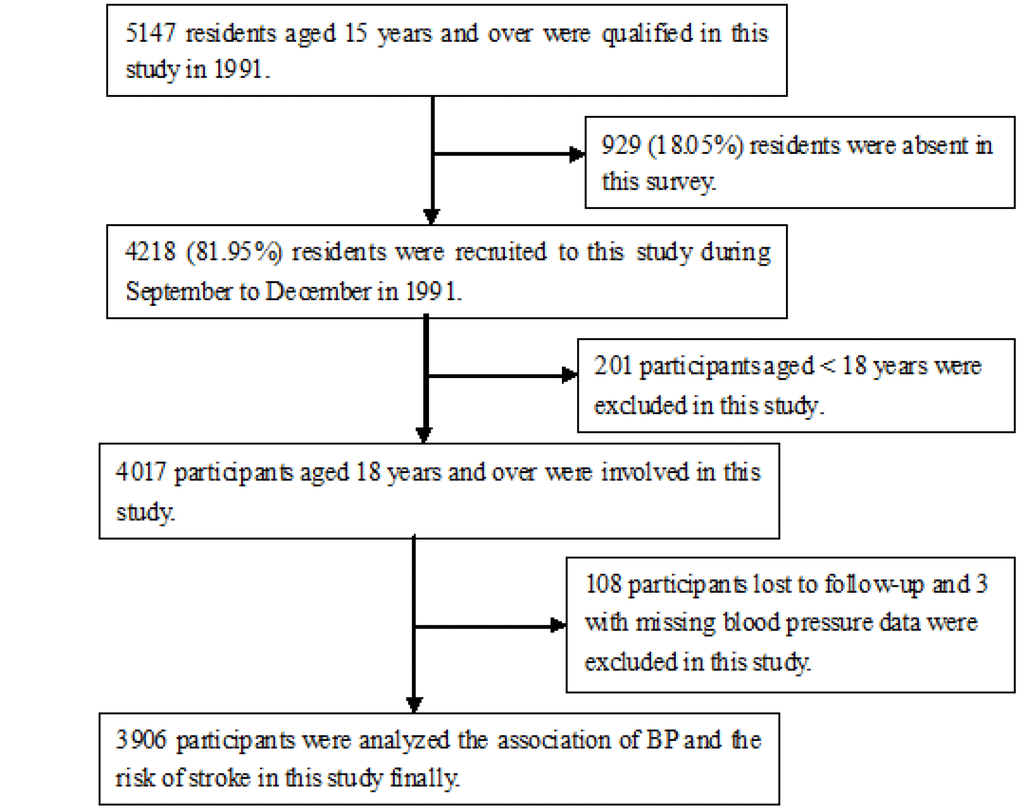
Figure 1. Flow chart of participants.
Demographic features and baseline risk factors
During a mean following-up of 21.85 years (85,346 person-years), 3906 participants were involved in this cohort study; men accounted for 47% of the participants. The mean age of the participants was 41.7 years, overall; the average age of the men was 42.5 years and that of the women was 41.0 years. More than 60% of the individuals were <45 years old and had <7 years of education, only 3.5% of the individuals had a high school education. The mean SBP and DBP levels were 127.4 and 80 mmHg, respectively, overall; the corresponding levels were 127.9 and 80.6 mmHg in men and 126.9 and 79.4 mmHg in women. Using the 2017 hypertension guideline definitions, 21.4% of the participants had normal BPs and >70% participants had hypertension, at baseline. Moreover, the prevalence of overweight/obese individuals, current smoking, and current alcohol consumption was 25.9%, 25.7, and 15.4%, respectively (Table 1).
Table 1. Description of the demographical features at baseline among all participants by BP levels.
| Features | Total | Men | Women | P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Participants | 3906 (100) | 1834 (47.0) | 2072 (53.0) | — | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Person-year | 85346.51 | 38766.04 | 46580.47 | — | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Follow-up time, years | 21.85 | 21.14 | 22.48 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years | 41.74 (16.58) | 42.51 (16.89) | 41.07 (16.28) | 0.007 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age groups: | 0.004 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18~34 years | 1582 (40.5) | 720 (39.3) | 862 (41.6) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 35~44 years | 906 (23.2) | 401 (21.9) | 505 (24.4) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 45~54 years | 466 (11.9) | 238 (13.0) | 228 (11.0) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 55~64 years | 470 (12.0) | 222 (12.1) | 248 (12.0) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 65~74 years | 320 (8.2) | 168 (9.2) | 152 (7.3) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 75 years | 162 (4.1) | 85 (4.6) | 77 (3.7) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education attainment: | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 year | 1588 (40.7) | 675 (36.8) | 913 (44.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1~6 years | 978 (25.0) | 508 (27.7) | 470 (22.7) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7~9 years | 1203 (30.8) | 584 (31.8) | 619 (29.9) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 10 years | 137 (3.5) | 67 (3.7) | 70 (3.4) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP, mmHg | 127.39 (20.27) | 127.92 (17.57) | 126.92 (22.39) | 0.120 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DBP, mmHg | 79.95 (11.41) | 80.60 (10.59) | 79.37 (12.06) | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BP groups: | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Normal BP | 835 (21.4) | 291 (15.9) | 544 (26.3) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Elevated BP | 314 (8.0) | 146 (8.0) | 168 (8.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage 1 Hypertension | 1559 (39.9) | 820 (44.7) | 739 (35.7) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage 2 Hypertension | 1198 (30.7) | 577 (31.5) | 621 (30.0) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, Kg/m2 | 22.59 (2.80) | 22.32 (2.37) | 22.83 (3.11) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI groups: | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Normal | 2897 (74.2) | 1466 (79.9) | 1431 (69.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Over weight | 847 (21.7) | 332 (18.1) | 515 (24.9) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity | 162 (4.1) | 36 (2.0) | 126 (6.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status: | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never | 2792 (71.5) | 812 (44.3) | 1980 (95.6) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ever | 112 (2.9) | 101 (5.5) | 11 (0.5) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 1002 (25.7) | 921 (50.2) | 81 (3.9) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Drinking status: | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never | 3288 (84.2) | 1241 (67.7) | 2047 (98.8) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ever | 16 (0.4) | 16 (0.9) | 0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 602 (15.4) | 577 (31.5) | 25 (1.2) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SD, standard deviation; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Distribution of stroke risk factors, by BP group
Table 2 shows that the elevated BP levels were significantly associated with sex, age group, educational attainment, and BMI group (all, P<0.01). However, BP levels were not significantly associated with smoking or alcohol consumption.
Table 2. Distribution characteristics of stroke risk factors in this cohort study during 27-years following–up periods by BP groups.
| Characteristics | Normal BP | Elevated BP | Stage 1 hypertension | Stage 2 hypertension | P |
| Gender, n (%): | <0.001 | ||||
| Men | 291 (15.9) | 146 (8.0) | 820 (44.7) | 577 (31.5) | |
| Women | 544 (26.3) | 168 (8.1) | 739 (35.7) | 621 (30.0) | |
| Total | |||||
| Age groups, n (%): | <0.001 | ||||
| < 60 years | 785 (24.6) | 286 (9.0) | 1405 (44.1) | 712 (22.3) | |
| ≥ 60 years | 50 (7.0) | 28 (3.9) | 154 (21.4) | 486 (67.7) | |
| Education attainment, n (%): | <0.001 | ||||
| 0 years | 236 (14.9) | 143 (9.0) | 528 (33.2) | 681 (42.9) | |
| 1~6 years | 239 (24.4) | 82 (8.4) | 385 (39.4) | 272 (27.8) | |
| 7~9 years | 316 (26.3) | 83 (6.9) | 585 (48.6) | 219 (18.2) | |
| > 9 years | 44 (32.1) | 6 (4.4) | 61 (44.5) | 26 (19.0) | |
| BMI groups, n (%): | <0.001 | ||||
| Normal | 679 (23.4) | 249 (8.6) | 1199 (41.4) | 770 (26.6) | |
| Over weight | 137 (16.2) | 54 (6.4) | 316 (37.3) | 340 (40.1) | |
| Obesity | 19 (11.7) | 11 (6.8) | 44 (27.2) | 88 (54.3) | |
| Smoking status, n (%): | 0.089 | ||||
| Never | 182 (18.2) | 91 (9.1) | 457 (45.6) | 272 (27.1) | |
| Ever | 7 (6.3) | 3 (2.7) | 43 (38.4) | 59 (52.7) | |
| Current | 646 (23.1) | 220 (7.9) | 1059 (37.9) | 867 (31.1) | |
| Drinking status, n (%): | 0.118 | ||||
| Never | 105 (17.4) | 47 (7.8) | 276 (45.8) | 174 (28.9) | |
| Ever | 2 (12.5) | 1 (6.3) | 10 (62.5) | 3 (18.8) | |
| Current | 728 (22.1) | 266 (8.1) | 1273 (38.7) | 1021 (31.1) |
Incidence of first-ever stroke, based on demographic features, risk factors, and stroke type
Over the 27-year study period, 638 first-ever strokes were reported, including 404 ISs 121 ICHs, and 113 undetermined strokes. Thus, the overall incidence of first-ever stroke was 7.7/1000 person-years, including 9.7/1000 person-years for men and 5.8/1000 person-years for women; the incidence of IS was 4.5/1000 person-years and that of ICH was 1.4/1000 person-years. The incidences of normal BP (3.9/1000 person-years; 95% CI, 3.0–4.7), elevated BP (7.0/1000 person-years; 95% CI, 5.1–8.9), stage 1 hypertension (5.68/1000 person-years; 95% CI, 4.92–6.46), and stage 2 hypertension (15.53/1000 person-years; 95% CI, 13.85–17.21) were also determined. Moreover, the incidence of first-ever stroke, per 1000 person-years, increased with increasing BP and BMI levels, but decreased with increasing educational attainment (Table 3).
Table 3. Age-standardized incidence incidences of first-ever stroke in this cohort study during 27-years following–up periods by stroke subtypes (per 1000 person-year)*.
| Features | Stroke | Ischemic stroke | Hemorrhagic stroke | P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Men | 9.83 (5.87, 7.54) | 5.95 (5.19, 6.73) | 2.06 (1.61, 2.52) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Women | 5.57 (4.89, 6.24) | 3.71 (3.16, 4.27) | 0.88 (0.61, 1.15) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total | 7.53 (6.90, 8.05) | 4.73 (4.27, 5.19) | 1.42 (1.17, 1.67) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age groups: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| < 60 years | 5.35 (4.83, 5.87) | 3.92 (3.48, 4.36) | 1.11 (0.87, 1.34) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 60 years | 26.64 (23.22, 30.06) | 12.08 (9.77, 14.41) | 4.23 (2.85, 5.60) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education attainment, years | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | 11.57 (10.24, 12.65) | 6.46 (5.55, 7.38) | 2.30 (1.76, 2.85) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1~6 | 8.75 (7.52, 9.99) | 5.83 (4.83, 6.84) | 1.78 (1.22, 2.34) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7~9 | 3.22 (2.59, 3.86) | 2.63 (2.06, 3.21) | 0.43 (0.20, 0.66) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| > 9 | 1.73 (0.35, 3.13) | 1.45 (0.18, 2.72) | 0.29 (-0.28, 0.86) | 0.219 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BP groups: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Normal BP | 2.87 (2.14, 3.60) | 2.09 (1.51, 2.77) | 0.53 (0.22, 0.85) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Elevated BP | 6.53 (4.64, 8.29) | 4.85 (3.27, 6.43) | 1.08 (0.33, 1.83) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage 1 Hypertension | 5.68 (4.92, 6.46) | 3.69 (3.07, 4.31) | 1.23 (0.87, 1.59) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage 2 Hypertension | 15.53 (13.85, 17.21) | 9.09 (7.80, 10.38) | 2.74 (2.03, 3.45) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI groups: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Normal | 6.53 (5.90, 7.14) | 4.11 (3.61, 4.61) | 0.66 (0.86, 1.38) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Over weight | 9.86 (8.36, 11.17) | 6.08 (4.97, 7.21) | 2.42 (1.72, 3.13) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity | 12.63 (8.77, 16.44) | 9.23 (5.94, 12.51) | 1.54 (0.19, 2.89) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never | 6.57 (5.94, 7.23) | 4.11 (3.60, 4.62) | 1.21 (0.94, 1.49) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ever | 16.33 (11.02, 21.60) | 13.13 (8.39, 17.90) | 2.27 (0.28, 4.25) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 9.08 (7.81, 10.30) | 5.61 (4.63, 6.60) | 1.90 (1.33, 2.48) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Drinking status: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never | 7.24 (6.54, 7.78) | 4.42 (3.93, 4.91) | 1.41 (1.13, 1.68) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ever | 27.64 (9.73, 45.49) | 21.49 (5.65, 37.29) | 6.14 (-2.39, 14.66) | 0.177 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 8.59 (7.07, 10.14) | 5.95 (4.68, 7.23) | 1.36 (0.75, 1.98) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *presented as age-standardized incidence using WHO standardized population; 95%CI, 95% confidence interval; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
BP levels and incidence of first-ever stroke by sex, age, and stroke type
Table 4 shows that, relative to the normal BP group, the stroke risk increased significantly in the elevated BP group (increased 89%, P=0.001), the stage 1 hypertension group (increased 69%, P<0.001), and in the stage 2 hypertension group (increased 248%, P<0.001); the incidence of IS increased by 96% (P=0.003), 53% (P=0.014), and 225% (P<0.001), in the respective groups. Similar trends were found for the overall stroke risk for men in the elevated BP (HR, 2.08; 95% CI, 1.18–3.64; P=0.011), stage 1 hypertension(HR, 2.12; (5% CI,1.37–3.27; P=0.001), and stage 2 hypertension (HR, 4.36; 95% CI,2.82–6.75; P<0.001) groups. Among men, the trend also persisted for IS in those in the elevated BP (HR,2.14; 95% CI,1.10–4.16; P=0.025), stage 1 hypertension (HR, 1.87; 95% CI,1.11–3.16; P=0.019), and stage 2 hypertension (HR, 4.19; 95% CI,2.48–7.07; P<0.001) groups. However, among women, a significant association of BP levels with the risk of developing first-ever stroke was found only in the elevated BP and stage 2 hypertension groups, both for overall stroke and IS. Stage 2 hypertension increased the ICH risk in both men and women, increasing the stroke risk 2.8-fold in men and 1.6-fold in women.
Table 4. Adjusted hazard ratio of BP levels for the incidence of the first-ever stroke by sex and stroke types in this cohort study (95% CI).
| BP category | Stroke | IS | ICH |
| Total: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 1.89 (1.29, 2.78)* | 1.96 (1.26, 3.04)* | 1.58 (0.64, 3.94) |
| Stage 1 Hypertension | 1.69 (1.27, 2.27)* | 1.53 (1.09, 2.16)* | 1.86 (0.96, 3.61) |
| Stage 2 Hypertension | 3.48 (2.61, 4.64)* | 3.25 (2.31, 4.57)* | 3.16 (1.62, 6.16)* |
| Men: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 2.08 (1.18, 3.64)* | 2.14 (1.10, 4.16)* | 1.97 (0.57, 6.82) |
| Stage 1 Hypertension | 2.12 (1.37, 3.27)* | 1.87 (1.11, 3.16)* | 2.54 (0.99, 6.51) |
| Stage 2 Hypertension | 4.36 (2.82, 6.75)* | 4.19 (2.48, 7.07)* | 3.81 (1.46, 9.96)* |
| Women: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 1.89 (1.11, 3.20)* | 2.00 (1.10, 3.64)* | 1.25 (0.31, 5.05) |
| Stage 1 Hypertension | 1.43 (0.95, 2.14) | 1.39 (0.87, 2.22) | 1.18 (0.43, 3.22) |
| Stage 2 Hypertension | 2.91 (1.96, 4.32)* | 2.70 (1.70, 4.29)* | 2.60 (1.00, 6.78)* |
Among men aged <60 years, the risk of developing first-ever stroke increased significantly in those with elevated BP, stage 1 hypertension, and stage 2 hypertension, for both stroke and IS. However, the risk of developing ICH increased significantly only for those with stage 2 hypertension (HR, 2.73; 95% CI,1.31–5.66; P=0.007). Similar findings were observed in men aged ≥60 years old. The risk of developing IS increased by 2.15-fold for those with elevated BP, 1.62-fold for those with stage 1 hypertension, and 4.4-fold for those with stage 2 hypertension (all P<0.05), respectively; the risk of developing ICH increased nearly 3-fold (P=0.014). The risk of developing the first-ever stroke in women <60 years old increased 1.5-fold for stroke and 1.7-fold for IS among those with stage 2 hypertension (P<0.001), but a similar correlation was not observed for ICH. Moreover, the IS risk among women aged ≥60 years only increased in those with stage 2 hypertension(HR, 2.98;95%CI, 1.08–8.26; P=0.035) (Table 5).
Table 5. Adjusted hazard ratio of BP levels for the incidence of the first-ever stroke by age, sex, and stroke types in this cohort study (95% CI).
| BP Category | Stroke | IS | ICH |
| Total: | |||
| < 60 years: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 2.03 (1.34, 3.08)* | 2.22 (1.37, 3.59)* | 1.50 (0.57, 3.95) |
| Stage 1 Hypertension | 1.70 (1.23, 2.35)* | 1.71 (1.17, 2.50)* | 1.73 (0.86, 3.51) |
| Stage 2 Hypertension | 3.29 (2.36, 4.59)* | 3.54 (2.40, 5.22)* | 2.73 (1.31, 5.66)* |
| ≥ 60 years | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 1.30 (0.48, 3.53) | 1.11 (0.34, 3.63) | 2.59 (0.16, 41.92) |
| Stage 1 Hypertension | 1.36 (0.71, 2.63) | 0.70 (0.32, 1.53) | 2.66 (0.33, 21.21) |
| Stage 2 Hypertension | 2.28 (1.24, 4.21)* | 1.23 (0.61, 2.47) | 3.74 (0.51, 27.78) |
| Men: | |||
| < 60 years: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 2.71 (1.45, 5.09)* | 3.15 (1.47, 6.73)* | 2.03 (0.50, 8.15) |
| Stage 1 Hypertension | 2.49 (1.49, 4.16)* | 2.62 (1.39, 4.96)* | 2.79 (0.97, 8.01) |
| Stage 2 Hypertension | 4.72 (2.79, 7.98)* | 5.40 (2.83, 10.31)* | 3.96 (1.33, 11.79)* |
| ≥ 60 years: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 0.62 (0.13, 3.02) | 0.40 (0.05, 3.32) | 2.01 (0.12, 32.67) |
| Stage 1 Hypertension | 1.15 (0.50, 2.63) | 0.45 (0.17, 1.22) | 1.64 (0.20, 13.48) |
| Stage 2 Hypertension | 2.06 (0.95, 4.47) | 1.06 (0.45, 2.52) | 2.16 (0.28, 16.42) |
| Women: | |||
| < 60 years: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 1.74 (0.98, 3.09) | 1.87 (0.98, 3.58) | 1.21 (0.30, 4.87) |
| Stage 1 Hypertension | 1.25 (0.80, 1.96) | 1.30 (0.78, 2.15) | 0.93 (0.33, 2.66) |
| Stage 2 Hypertension | 2.47 (1.57, 3.86)* | 2.67 (1.60, 4.45)* | 1.84 (0.65, 5.19) |
| ≥ 60 years: | |||
| Normal BP | 1.00 | 1.00 | 1.00 |
| Elevated BP | 3.35 (0.82, 13.66) | 3.00 (0.58, 15.35) | --- |
| Stage 1 Hypertension | 2.10 (0.70, 6.34) | 1.58 (0.42, 5.92) | --- |
| Stage 2 Hypertension | 2.98 (1.08, 8.26)* | 1.63 (0.49, 5.46) | --- |
Additionally, elevated BP levels were associated with total stroke risk, as well as for IS and ICH risk, with respective log-rank values of 286.270,147.023, and 41.761 (all, P<0.001) (Figure 2).
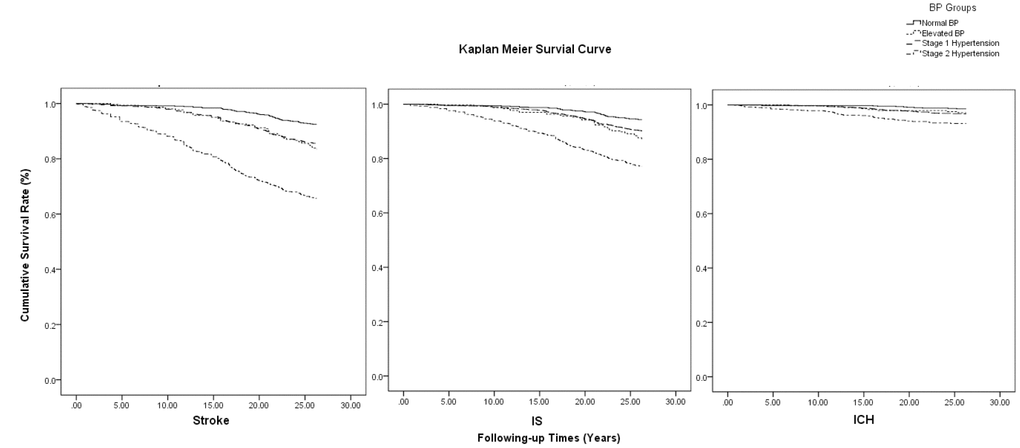
Figure 2. Kaplan-Meier survival curve on association of BP levels with the risk of stroke by types.
PAR% of abnormal BP on the incidence of first-ever stroke
Figure 3 shows that the PAR% for the incidence of first-ever stroke associated with abnormal BP (including elevated BP and stages 1 and 2 hypertension) was 49.4%, overall; the values for men and women were 38.5% and 53.3%, respectively. Among individuals <60 years old, the PAR was 54.8%, overall (63.6% for men and 41.7% for women). Among those aged ≥60 years, the corresponding PAR% values were 46.0% (overall risk), 34.4% (men), and 54.9% (women), respectively.
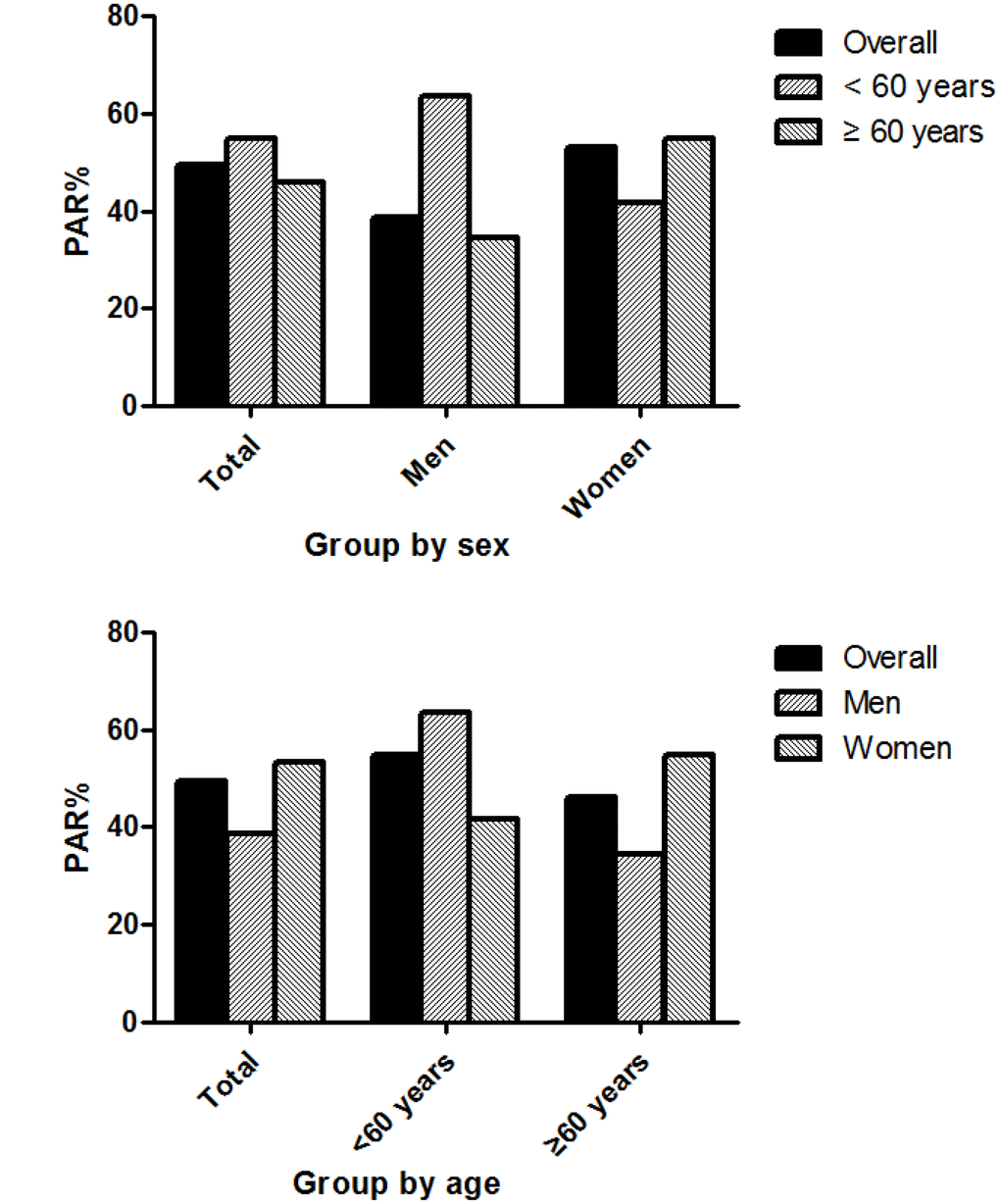
Figure 3. Population attributable risk percent for the incidence of first-ever stroke associated with abnormal BP.
Discussion
In this 27-year prospective cohort study, we assessed the risk of developing first-ever stroke, based on the BP definitions in the 2017 ACC/AHA hypertension guideline. The findings indicate that elevated BP, stage 1 hypertension, and stage 2 hypertension were associated with significantly increased first-ever stroke risks, compared with normal BP. Additionally, there were sex, age, and stroke type distinctions regarding the impact of BP categories on developing stroke. Among men <60 years old, the risk of the developing IS increased significantly among those in all three abnormal BP classifications; however, only stage 2 hypertension appeared to significantly increase the risk of ICH. Among women <60 years old, there was an increased risk of IS observed among only those with stage 2 hypertension; further, there was no evidence of an increased risk of ICH associated with any BP category. There were no obvious associations between BP classifications and the risk of developing stroke among individuals aged ≥60 years old for either IS or ICH. The PAR% was higher in men than in women among individuals aged <60 years, but the opposite trend was found among those aged ≥60 years.
The definition of hypertension in the 2017 ACC/AHA guideline has been the subject of significant interest, globally. There has been concern regarding the increased number of patients defined as having hypertension based on this new definition that was reached, by consensus, among representatives from many countries [9, 17, 18–21]. In China, the prevalence of hypertension, based on the 2017 guideline, is twice as high as that based on the 2010 Chinese guideline; with the additional people captured under the new guideline, the prevalence of hypertension in China rose to 46.4%, whereas the control rate fell to 3.0% [9]. Additionally, the effects of the new BP classification on cardiovascular risk within a population is critical, especially in China.
Recently, several reports assessed CVD risk using the new BP stratification. The latest research from the American Coronary Artery Risk Development in Young Adults study indicated that, among young adults, those developing elevated blood pressure, stage 1 hypertension, or stage 2 hypertension (as defined by the blood pressure classification in the 2017 ACC/AHA guideline) before reaching 40 years of age had a significantly higher risk of subsequent CVD events than those with normal BP at 40 years of age. Thus, the new BP classification system may help identify young adults at a higher risk of CVD events [22]. Additionally, Korean young adults, aged 20–39 years with stage 1 or 2 hypertension had higher CVD risks than those with normal BP. Both men and women with elevated baseline BP, stage 1, or stage 2 hypertension, as defined by the new criteria, had higher risks of stroke than those with normal BP [23].
Liu and colleagues demonstrated that the effect of the 2017 ACC/AHA stage 1 hypertension definition on cardiovascular risk was evidenced in young and middle-aged Chinese adults, but not in those ≥60 years old. Among 35–59-year-old participants, the HR for CVD incidence when comparing individuals with stage 1 hypertension to those with SBPs <120 mmHg and DBPs <80 mmHg was 1.78 (95% CI, 1.50–2.11); that for coronary heart disease was 1.77 (95% CI, 1.33–2.36); that for stroke incidence was 1.79 (95% CI, 1.45–2.22); and that for CVD mortality was 2.50 (95% CI, 1.66–3.77) [24]. Similar to their findings, we found an association between the newly defined BP categories and first-ever stroke risk in young and middle-aged men and women in a rural Chinese population. Thus, we propose stricter BP control targets (SBP <120 mmHg and DBP <80 mmHg) for reducing the burden of stroke among young and middle-aged men in such rural populations. In these rural populations, there is a high prevalence of hypertension and a high stroke incidence, combined with lower rates of hypertension awareness, treatment, and control [10]. Adopting this BP control target is expected to reduce the incidence of first-ever stroke by 68% in men <60 years old.
In China, stroke carries the nation’s highest disease burden and was the nation’s leading cause of death in 2010, with 1.7 million deaths [25]. Our previous studies revealed that the incidence of first-ever stroke has been dramatically increasing among rural populations in China, especially among men aged 35–64 years (12% annual increase) [6, 7]. Moreover, the mean age of stroke onset in men has been decreasing by 0.28 years, annually, including annual declines of 0.56 years for ICH and 0.22 years for IS during the period between1992 and 2014 [26]. Further, hypertension is an established risk factor for stroke, and controlling BP is the most effective approach for preventing strokes [27–29]. Nevertheless, poor hypertension awareness, treatment, and control among young and middle-aged individuals have been reported in our prior studies [10]. Thus, executing strict BP target management (SBP <120mmHg and DBP <80mmHg) in these populations is critical for decreasing the incidence of first-ever stroke and reducing the disease burden of stroke in China.
The updated recommendations for defining and treating hypertension received a mixed response from several clinical societies [18–21, 30]. In part, this is because adopting the new guideline will result in a substantial increase in the reported prevalence of hypertension, in both the US and China. This would be accompanied by a marked increase in the number of individuals recommended to begin hypertension treatment and treatment would need to be intensified for several million patients [30]. However, a recent systematic review and meta-analysis indicated that lowering BP is associated with reduced risks of death and CVD if the baseline SBP is ≥140mmHg; at lower BP levels, treatment is not associated with any primary prevention benefit but might offer additional protection in patients with coronary heart disease [31]. We reported the BP levels just obtained at baseline in 1991, not a dynamic BP values. These may limited the popularization of these findings to board population. However, given that lower rates of hypertension awareness, treatment, and control, and poor health consciousness in this rural population, even though the dynamic BP values were absent, the stricter BP management target should be remained.
This study has several limitations. First, the study population was from a township in northern China, which is not representative of the overall national population. Further, the results may not necessarily be generalizable to other racial or ethnic populations. However, the prospective study design and lengthy study period may have reduced the impact of the study’s limited generalization. Second, the 85,000 person-years in the follow-up period did not fulfill the criteria of at least 100,000 person-years of observations recommended for population studies [32]. Third, we only assessed the risk of stroke using BP levels at baseline, without dynamic BP measurements. However, the low rates of hypertension awareness, treatment, and control, as well as the overall lack of health consciousness in this rural population, suggest that the strict BP management target should still be used, despite the lack of reporting of dynamic BP values. Finally, we did not collect detailed information regarding fasting glucose and lipids levels, dietary habits, or medication use; therefore, other possible determinants of stroke could not be assessed in this study.
Materials and Methods
Study population and sampling method
This analysis was based on a 27-year population-based cohort study that began in1991 and was conducted in Tianjin, China; the study design was previously described [10]. Briefly, the study involved individuals participating in the Tianjin Brain Study, a population-based stroke surveillance study. The participants resided in 18 administrative villages in Tianjin, and 95% were low-income farmers. The primary source of income was grain production, with the residents having an annual per capita income of <100 USD in 1991 and <1000 USD in 2010 [33].
The sampling method used in this cohort study was also previously reported [34]. Briefly, the villages were grouped according to their geographic location (east, south, and north) and two villages from each geographic location were randomly sampled, using a stratified cluster sampling method. In these six villages, all adults aged ≥18years and without histories of cardiovascular disease (CVD) or stroke were recruited into the study.
The study protocol was approved by the ethics committee of Tianjin Medical University General Hospital (TMUGH); written informed consent was obtained from each participant.
Baseline information
Individual demographic characteristics (including sex, age, and educational attainment), disease history (including hypertension, diabetes, stroke, and CVD), and lifestyle factors (including smoking and alcohol consumption status and physical activity), at baseline, were collected in 1991. All information was collected by local, trained research staff who conducted face-to-face interviews; the interviews also included physical examinations to determine BPs, heights, and body weights.
Risk factor measurement and categorization
In this study, we assessed the association of stroke risk with baseline BP levels. BP was measured as previously described [10]. Briefly, standardized BP measurements were performed using a calibrated mercury sphygmomanometer, with the cuff size adjusted to the individual’s arm circumference. The cuff was placed on the arm at the level of the heart, and the BP was recorded as the mean of two measurements, 5 min apart, with the participant resting in the supine position. Each patient avoided caffeine, exercise, and smoking for at least 30 min prior to the measurements. The SBP and DBP values were determined according to Korotkoff sounds I and V. If the difference between the two consecutive readings was not within 10 mmHg (SBP) and/or 5mmHg (DBP), or if the measurement reached the criteria for hypertension, two further readings were obtained after the participant rested for an additional 20 min.
To evaluate stroke risk associated with the BP categories, individuals were stratified, according to the new guideline: normal BP (SBP,<120 mmHg; DBP,<80 mmHg), elevated BP (SBP, 120–129 mmHg; DBP,<80 mmHg), stage 1 hypertension (SBP, 130–139 mmHg; DBP, 80–89 mmHg), and stage 2 hypertension (SBP, ≥140mmHg or DBP, ≥90 mmHg). Diabetes, stroke, and CVD determinations were based on self-reported disease histories. Body mass indexes (BMIs) were calculated and used to categorize individuals as being normal weight (BMI <24 kg/m2), overweight (BMI = 24–27.9 kg/m2), or obese (BMI ≥28 kg/m2) [34].
Stroke diagnosis and types
Stroke was defined as an acute-onset, focal neurological deficit of vascular etiology persisting for >24 h, including both ischemic and hemorrhagic subtypes [35]. Hemorrhagic stroke was defined as an ICH;IS was defined as a thrombotic brain infarction, cardioembolic stroke, or lacunar infarct; an undetermined stroke was defined as a stroke that could not be classified into either subtype. All strokes were symptomatic, with significant clinical symptoms and signs. Transient ischemic attacks and silent strokes (diagnosed by imaging, only) were excluded, but stroke patients with histories of transient ischemic attacks prior to a defined stroke were included. Patients demonstrating transient symptoms and having concurrent neuroimaging evidence of brain infarctions were considered as stroke cases, based on the “tissue” definition [36]. In the early phase of this study (1992–1998), the events were confirmed primarily based on clinical examinations by senior neurologists for non-hospitalized patients and using medical records for hospitalized patients.
Stroke reporting
Stroke events were reported using thepredefined procedures reported previously [6]. Briefly, local, licensed village physicians reported initial stroke events to the community hospital within 24 h of onset. Within 72 h, community hospital physicians visited the surviving patients’ homes to confirm stroke events and obtain clinical feature information. Confirmed stroke events (imaging diagnosis) were reported monthly to TMUGH, and suspected events (no imaging performed) were reported in a timely manner. Finally, a TMUGH neurologist identified suspected cases through door-to-door interviews, as soon as possible.
Statistical analysis
Continuous variables (age, SBP, DBP, and BMI) are presented as means and standard deviations (SDs); categorical variables are presented as frequencies with 95% CIs. Subgroup analyses were conducted to evaluate the first-ever stroke risk by age group (18–34 years, 35–44 years, 45–54 years, 55–64 years, 65–74 years, and ≥75 years), education level (illiterate [no formal education], 1–6 years, 7–9 years, and ≥10 years of formal education), BMI group (normal, overweight, and obese), smoking status (never smoked, previous smoker, and current smoker), and drinking status (never consumed alcohol, previously consumed alcohol, and currently consumes alcohol). Adjusted hazard ratios (HRs) for the incidence of overall stroke and each type, by BP category, were estimated using Cox proportional hazards models adjusted for age, sex, education level, BMI, smoking status, and drinking status. Moreover, a subgroup analysis was performed to detect the association of BP levels with stroke risk, by age (simplified to <60 years and ≥60 years). Diabetes was not analyzed in this study because there were too few patients with diabetes (n = 4), at baseline. Population attributable risk percent (PAR%) was used to estimate the proportion of incident stroke events attributable to abnormal BPs (including elevated BP, stage 1 hypertension, and stage 2 hypertension), which was calculated using the formula: PAR%=(It-I0)/It, where It denotes the total stroke incidence in the whole population during the study period; I0 denotes the stroke incidence among those with normal BP. All statistical analyses were performed using SPSS for Windows (version 15.0; SPSS, Chicago, IL, USA); a P-value < 0.05 was considered statistically significant.
Summary
To the best of our knowledge, this is the first prospective study aimed at quantitatively determining the first-ever stroke risk associated with the new hypertension guideline. Elevated BP can increase the risk of developing stroke if people do not undergo routine BP measurements and treat any detected hypertension. The BP management target for reducing the risk of incident IS and ICH in young and middle-aged men in China is an SBP <120mmHg and a DBP <80mmHg. However, for young and middle-aged women, we recommend a BP management target of SBP <140mmHg and DBP <90mmHg to decrease the incident IS risk. Therefore, an urgent focus on the early adoption of lifestyle interventions among young and middle-aged adults, especially for men, is needed to decrease the incidence of stroke in China. In addition, the recommended BP control target for reducing the burden of stroke among young and middle-aged men provides a valuable reference for other developing countries experiencing the serious disease burdens associated with chronic, non-infectious diseases, such as hypertension and stroke.
Acknowledgments
We thank all participants of the Tianjin Brain Study, and local medical care professionals for their valuable contributions.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This study was supported in part by Tianjin Medical University General Hospital.
References
- 1. GBD 2016 Lifetime Risk of Stroke Collaborators. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N Engl J Med. 2018; 379:2429–37. https://doi.org/10.1056/NEJMoa1804492 [PubMed]
- 2. Feigin VL, Krishnamurthi RV, Parmar P, Norrving B, Mensah GA, Bennett DA, Barker-Collo S, Moran AE, Sacco RL, Truelsen T, Davis S, Pandian JD, Naghavi M, et al, and GBD 2013 Writing Group, and GBD 2013 Stroke Panel Experts Group. Update on the global burden of ischemic and haemorrhagic stroke in 1990–2013: the GBD 2013 study. Neuroepidemiology. 2015; 45:161–76. https://doi.org/10.1159/000441085 [PubMed]
- 3. Feigin VL, Roth GA, Naghavi M, Parmar P, Krishnamurthi R, Chugh S, Mensah GA, Norrving B, Shiue I, Ng M, Estep K, Cercy K, Murray CJ, Forouzanfar MH, and Global Burden of Diseases, Injuries and Risk Factors Study 2013 and Stroke Experts Writing Group. Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016; 15:913–24. https://doi.org/10.1016/S1474-4422(16)30073-4 [PubMed]
- 4. Hata J, Kiyohara Y. Epidemiology of stroke and coronary artery disease in Asia. Circ J. 2013; 77:1923–32. https://doi.org/10.1253/circj.CJ-13-0786 [PubMed]
- 5. Feigin VL, Norrving B. A new paradigm for primary prevention strategy in people with elevated risk of stroke. Int J Stroke. 2014; 9:624–26. https://doi.org/10.1111/ijs.12300 [PubMed]
- 6. Wang J, An Z, Li B, Yang L, Tu J, Gu H, Zhan C, Liu B, Su TC, Ning X. Increasing stroke incidence and prevalence of risk factors in a low-income Chinese population. Neurology. 2015; 84:374–81. https://doi.org/10.1212/WNL.0000000000001175 [PubMed]
- 7. Ning X, Sun J, Jiang R, Lu H, Bai L, Shi M, Tu J, Wu Y, Wang J, Zhang J. Increased Stroke Burdens Among the Low-Income Young and Middle Aged in Rural China. Stroke. 2017; 48:77–83. https://doi.org/10.1161/STROKEAHA.116.014897 [PubMed]
- 8. Lu J, Lu Y, Wang X, Li X, Linderman GC, Wu C, Cheng X, Mu L, Zhang H, Liu J, Su M, Zhao H, Spatz ES, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1·7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet. 2017; 390:2549–58. https://doi.org/10.1016/S0140-6736(17)32478-9 [PubMed]
- 9. Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, Shao L, Tian Y, Dong Y, Zheng C, Wang J, Zhu M, Weintraub WS, Gao R, and China Hypertension Survey Investigators. Status of Hypertension in China: Results From the China Hypertension Survey, 2012-2015. Circulation. 2018; 137:2344–56. https://doi.org/10.1161/CIRCULATIONAHA.117.032380 [PubMed]
- 10. Wang J, Ning X, Yang L, Lu H, Tu J, Jin W, Zhang W, Su TC. Trends of hypertension prevalence, awareness, treatment and control in rural areas of northern China during 1991-2011. J Hum Hypertens. 2014; 28:25–31. https://doi.org/10.1038/jhh.2013.44 [PubMed]
- 11. Li W, Gu H, Teo KK, Bo J, Wang Y, Yang J, Wang X, Zhang H, Sun Y, Jia X, He X, Zhao X, Cheng X, et al, and PURE China Investigators. Hypertension prevalence, awareness, treatment, and control in 115 rural and urban communities involving 47 000 people from China. J Hypertens. 2016; 34:39–46. https://doi.org/10.1097/HJH.0000000000000745 [PubMed]
- 12. Lewington S, Lacey B, Clarke R, Guo Y, Kong XL, Yang L, Chen Y, Bian Z, Chen J, Meng J, Xiong Y, He T, Pang Z, et al, and China Kadoorie Biobank Consortium. The burden of hypertension and associated risk for cardiovascular mortality in China. JAMA Intern Med. 2016; 176:524–32. https://doi.org/10.1001/jamainternmed.2016.0190 [PubMed]
- 13. Li D, Lv J, Liu F, Liu P, Yang X, Feng Y, Chen G, Hao M. Hypertension burden and control in mainland China: analysis of nationwide data 2003-2012. Int J Cardiol. 2015; 184:637–44. https://doi.org/10.1016/j.ijcard.2015.03.045 [PubMed]
- 14. Wang J, Zhang L, Wang F, Liu L, Wang H, and China National Survey of Chronic Kidney Disease Working Group. Prevalence, awareness, treatment, and control of hypertension in China: results from a national survey. Am J Hypertens. 2014; 27:1355–61. https://doi.org/10.1093/ajh/hpu053 [PubMed]
- 15. Whelton PK, Carey RM, Aronow WS, Casey DE
Jr , Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018; 71:2199–269. https://doi.org/10.1016/j.jacc.2017.11.005 [PubMed] - 16. Weiss J, Freeman M, Low A, Fu R, Kerfoot A, Paynter R, Motu’apuaka M, Kondo K, Kansagara D. Benefits and harms of intensive blood pressure treatment in adults aged 60 years or older: a systematic review and metaanalysis. Ann Intern Med. 2017; 166:419–29. https://doi.org/10.7326/M16-1754 [PubMed]
- 17. Kim HC, Jeon YW, Heo ST. Global Impact of the 2017 American College of Cardiology/American Heart Association Hypertension Guidelines. Circulation. 2018; 138:2312–14. https://doi.org/10.1161/CIRCULATIONAHA.118.036312 [PubMed]
- 18. Wander GS, Ram CV. Global Impact of 2017 American Heart Association/American College of Cardiology Hypertension Guidelines: A Perspective From India. Circulation. 2018; 137:549–50. https://doi.org/10.1161/CIRCULATIONAHA.117.032877 [PubMed]
- 19. Schiffrin EL. Global Impact of the 2017 American College of Cardiology/American Heart Association Hypertension Guidelines: A Perspective From Canada. Circulation. 2018; 137:883–85. https://doi.org/10.1161/CIRCULATIONAHA.117.032849 [PubMed]
- 20. Wang JG, Liu L. Global Impact of 2017 American College of Cardiology/American Heart Association Hypertension Guidelines: A Perspective From China. Circulation. 2018; 137:546–48. https://doi.org/10.1161/CIRCULATIONAHA.117.032890 [PubMed]
- 21. Mancia G, Corrao G. Global Impact of the 2017 American College of Cardiology/American Heart Association Hypertension Guidelines: A Perspective From Italy. Circulation. 2018; 137:889–90. https://doi.org/10.1161/CIRCULATIONAHA.117.032850 [PubMed]
- 22. Yano Y, Reis JP, Colangelo LA, Shimbo D, Viera AJ, Allen NB, Gidding SS, Bress AP, Greenland P, Muntner P, Lloyd-Jones DM. Association of Blood Pressure Classification in Young Adults Using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline With Cardiovascular Events Later in Life. JAMA. 2018; 320:1774–82. https://doi.org/10.1001/jama.2018.13551 [PubMed]
- 23. Son JS, Choi S, Kim K, Kim SM, Choi D, Lee G, Jeong SM, Park SY, Kim YY, Yun JM, Park SM. Association of Blood Pressure Classification in Korean Young Adults According to the 2017 American College of Cardiology/American Heart Association Guidelines With Subsequent Cardiovascular Disease Events. JAMA. 2018; 320:1783–92. https://doi.org/10.1001/jama.2018.16501 [PubMed]
- 24. Qi Y, Han X, Zhao D, Wang W, Wang M, Sun J, Liu J, Li Y, Gao S, Hao Y, Deng Q, Liu J. Long-Term Cardiovascular Risk Associated With Stage 1 Hypertension Defined by the 2017 ACC/AHA Hypertension Guideline. J Am Coll Cardiol. 2018; 72:1201–10. https://doi.org/10.1016/j.jacc.2018.06.056 [PubMed]
- 25. Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, Wan X, Yu S, Jiang Y, Naghavi M, Vos T, Wang H, Lopez AD, Murray CJ. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013; 381:1987–2015. https://doi.org/10.1016/S0140-6736(13)61097-1 [PubMed]
- 26. Wang J, Bai L, Shi M, Yang L, An Z, Li B, Zhao W, Gu H, Zhan C, Tu J, Ning X. Trends in Age of First-Ever Stroke Following Increased Incidence and Life Expectancy in a Low-Income Chinese Population. Stroke. 2016; 47:929–35. https://doi.org/10.1161/STROKEAHA.115.012466 [PubMed]
- 27. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC
Jr , Svetkey LP, Taler SJ, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014; 311:507–20. https://doi.org/10.1001/jama.2013.284427 [PubMed] - 28. Wright JT
Jr , Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, Reboussin DM, Rahman M, Oparil S, Lewis CE, Kimmel PL, Johnson KC, Goff DCJr , et al, and SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015; 373:2103–16. https://doi.org/10.1056/NEJMoa1511939 [PubMed] - 29. Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, Chalmers J, Rodgers A, Rahimi K. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016; 387:957–67. https://doi.org/10.1016/S0140-6736(15)01225-8 [PubMed]
- 30. Khera R, Lu Y, Lu J, Saxena A, Nasir K, Jiang L, Krumholz HM. Impact of 2017 ACC/AHA guidelines on prevalence of hypertension and eligibility for antihypertensive treatment in United States and China: nationally representative cross sectional study. BMJ. 2018; 362:k2357. https://doi.org/10.1136/bmj.k2357 [PubMed]
- 31. Brunström M, Carlberg B. Association of Blood Pressure Lowering With Mortality and Cardiovascular Disease Across Blood Pressure Levels: A Systematic Review and Meta-analysis. JAMA Intern Med. 2018; 178:28–36. https://doi.org/10.1001/jamainternmed.2017.6015 [PubMed]
- 32. Coull AJ, Silver LE, Bull LM, Giles MF, Rothwell PM, and Oxford Vascular (OXVASC) Study. Direct assessment of completeness of ascertainment in a stroke incidence study. Stroke. 2004; 35:2041–45. https://doi.org/10.1161/01.STR.0000137605.48864.2f [PubMed]
- 33. The Ministry of Health of the People’s Republic of China. The causes of death, disease, and hurt in residents. China Health Statistics yearbook 2011. Beijing: China Union Medical University Press; 2011. pp. 287–338.
- 34. Disease control, Ministry of Health of the People’s Republic of China. The Guidelines of Chinese Adult Overweight and Obesity Prevention and Control. Beijing: People's Medical Publishing House; 2006. pp. 1–3.
- 35. Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ. 1980; 58:113–30. [PubMed]
- 36. Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, Hatsukami TS, Higashida RT, Johnston SC, Kidwell CS, Lutsep HL, Miller E, Sacco RL. Definition and Evaluation of Transient Ischemic Attack A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. Stroke. 2009; 40:2276–93. https://doi.org/10.1161/STROKEAHA.108.192218 [PubMed]