



Introduction
Colorectal cancer is the third most common cancer in the world, and its global burden is projected to be increased by 60% to over 2.2 million new cases and 11 million deaths by 2030 [1]. Clinical studies indicate that colorectal cancer predominantly metastasizes to the liver and lung [2-4]. It is estimated that approximately one in four patients have metastatic colorectal cancer at initial diagnosis, and almost half of colorectal cancer patients will develop metastases [5]. Over the past decade, considerable advances have been made in the treatment of metastatic colorectal cancer using chemotherapy and effective biotherapy, with great success [6-8]. It is well exemplified by the fact that median survival of metastatic colorectal cancer increased from 5 months to 2 years between 1993 and 2009 [9].
Bevacizumab, a humanized anti-vascular endothelial growth factor (VEGF) monoclonal antibody, is increasingly recognized as standard of care for the treatment of metastatic colorectal cancer in a first-line setting, with reasonable biological implications [10,11]. However, a problem facing global oncologists is that the clinical benefits of bevacizumab are seen in some, but not all, patients with metastatic colorectal cancer [12,13]. Given the enormous economic burden for bevacizumab-based treatment, the identification of a surrogate marker to gauge the usefulness of bevacizumab treatment in metastatic colorectal cancer is of particular importance to select patients who are more likely to benefit from the treatment. Many candidate predictive markers have been tested, and arterial hypertension is one of the most intensively researched [14,15]. Two previous meta-analyses have interrogated the usefulness of hypertension, by showing that bevacizumab-induced hypertension may be a prognostic factor for metastatic colorectal cancer [16,17]. However, an inherent drawback gripping the two meta-analyses is the under-explored heterogeneity and publication bias, likely due to the limited number of studies synthesized. With accumulating data on this subject in recent years, we sought to update the results of two previous meta-analyses by incorporating more studies and providing additional information. Specifically, we examined the hypothesis that bevacizumab-induced hypertension may be a useful predictor for objective response rate and survival outcomes (progression-free and overall survival) in patients with metastatic colorectal cancer.
Results
Qualified studies
In total, 632 articles were identified after searching the medical literature, as well as the reference lists of retrieved major articles and reviewers. Of them, only 13 articles including 14 independent studies and 2292 study subjects were qualified for the final analysis [12-15,18-26]. The process for excluding articles with specific reasons was presented as a PRISMA flowchart (Figure 1). In terms of research outcomes, 8 of 14 qualitied studies provided data on objective response rate, 9 studies on progression-free survival and 7 studies on overall survival, when gauging the usefulness of bevacizumab-induced hypertension in patients with metastatic colorectal cancer.
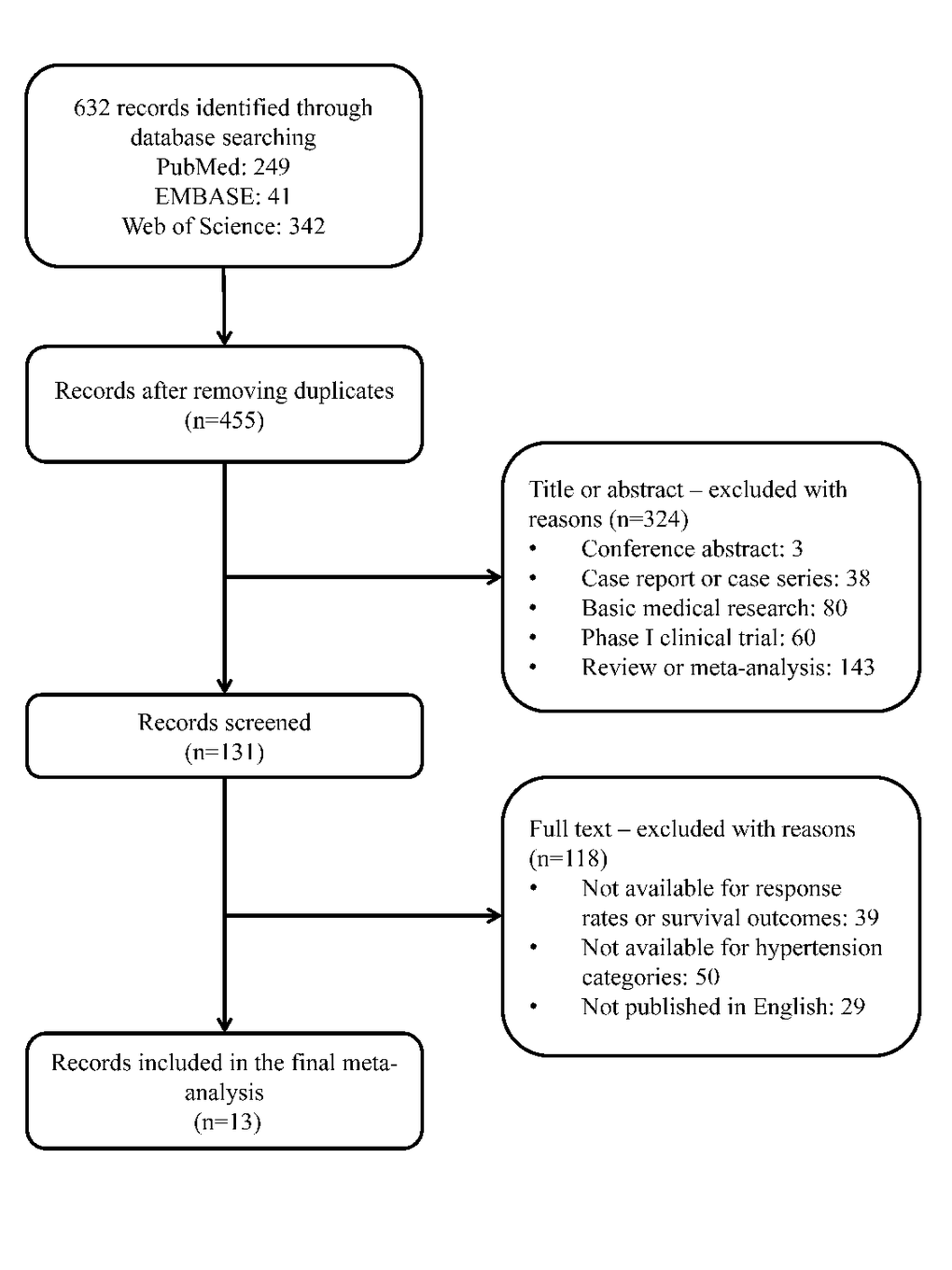
Figure 1. The flowchart for article selection in this meta-analysis.
Baseline characteristics
The baseline characteristics of 14 qualified studies published from 2009 to 2016 are listed in Table 1. Total sample size of each study ranged from 39 to 699. All but one study (in Japan) [25] were conducted in European countries and the United States of America. Ten studies used bevacizumab in the first-line setting [12,14,18-20,22-25]. Bevacizumab dose was either 2.5 mg/kg every week or 5 mg/kg every 2 weeks or 7.5 mg/kg every three weeks. Hypertension was diagnosed using the CTC AE (common terminology criteria; AE: adverse events) version 2.0 or 3.0 or 4.0. Male gender of each study ranged from 50% to 67.1%.
Table 1. Characteristics of the 14 selected studies in this meta-analysis.
| Author (year) | No. of patients | No. of patients with HTN (%) | Gender (M/F) | Line of treatment | Bevacizumab dose | Chemotherapy regiments | HTN criteria | Cut-off point | Median PFS (months) HTN/non-HTN | Median OS (months) HTN/non-HTN | ORR (%) HTN/non-HTN | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ryanne (2009) | 84 | 36 (42.9) | 42/42 | First | NA | NA | CTC AE V3.0 | Grade = 0 | NA | NA | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Scartozzi (2009) | 39 | 8 (20.5) | 25/14 | First | 5 mg/kg/2w | FOLFIRI | CTC AE V2.0 | Grade < 2 | 14.5/3.1 | NA/15.1 | 75/32 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| De Stefano (2011) | 74 | 13 (17.6) | 42/32 | First | 5 mg/kg/2w or 7.5 mg/kg/3w | FOLFIRI, FOLFOX, XELOX, XELIRI, FOLFOXIRI | CTC AE V3.0 | Grade = 0 | 15.1/8.3 | 35.5/26.7 | 84.6/42.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mir (2011) | 119 | 65 (54.6) | 63/56 | NA | 2.5 mg/kg/w | 5-FU-based | CTC AE V3.0 | Grade = 0 | NA | NA | 76.9/79.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Osterlund (2011) | 101 | 57 (56.4) | 54/47 | Combined | 5 mg/kg/2w or 7.5 mg/kg/3w | FOLFIRI, irinotecan-, oxaliplatin- or 5-FU-based | CTC AE V3.0 | Grade = 0 | 10.5/5.3 | 25.8/11.7 | 52.6/45.5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dewdney (2012) | 45 | 7 (15.6) | NA | First | 7.5 mg/kg/3w | CAPOX | CTC AE V3.0 | Grade = 0 | NA | NA | 71/78 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Budai (2013) | 232 | NA | 126/106 | First | 5 mg/kg/2w | modified FOLFIRI | CTC AE V3.0 | Grade ≤ 1 | NA | NA | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hurwitz (2013) | 402 | NA | 237/165 | First | 5 mg/kg/2w | IFL | CTC AE V2.0 | SBP/DBP increase 20/10 mmHg | NA | NA | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hurwitz (2013) | 699 | NA | 418/281 | First | 5 mg/kg/2w | FOLFOX-4 | CTC AE V3.0 | SBP/DBP increase 20/10 mmHg | NA | NA | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Morita (2013) | 60 | 16 (26.7) | 38/22 | First | 5 mg/kg/2w | mFOLFOX6, FOLFIRI, sLV5FU2, XELOX | CTC AE V4.0 | Grade ≤ 2 | NA | NA | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tahover (2013) | 181 | 81 (44.8) | 95/86 | First | 2.5 mg/kg/w | oxaliplatin, 5FU combination, irinotecan, 5FU combination, both combinations | CTC AE V4.0 | Grade ≤ 1 | 17.2/29.9 | 36.8/NA | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Khoja (2014) | 50 | 7 (14) | NA | Combined | NA | tyrosine kinase inhibitor (TKI) | CTC AE V3.0 | Grade ≤ 1 | 10.9/9.4 | 25.2/21.6 | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Feliu J (2015) | 127 | 20 (15.7) | 78/49 | NA | 7.5 mg/kg/3w | capecitabine in BECA, oxaliplatin, capecitabine in BECOX | CTC AE V2.0 | Grade = 0 | NA | NA/16.9 | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| de Sousa (2016) | 79 | 41 (51.9) | 53/26 | First | 5 mg/kg/2w | FOLFIRI or FOLFOX regimen | CTC AE V4.0 | Grade ≤ 1 | NA | 33/21 | NA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: HTN: hypertension; M: male; F: female; NA: not available; SBP: systolic blood pressure; DBP: diastolic blood pressure; ORR: objective response rate; OS: overall survival; PFS: progression free survival; CTC: common terminology criteria; AE: adverse events. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Objective response rate
As shown in Figure 2, pooled relative risk of objective response rate for bevacizumab-induced hypertension was 2.03 (95% confidence interval [CI]: 1.18 – 3.48, p=0.01), whereas this risk was clouded by the significance of between-study heterogeneity (I2: 77.1%).
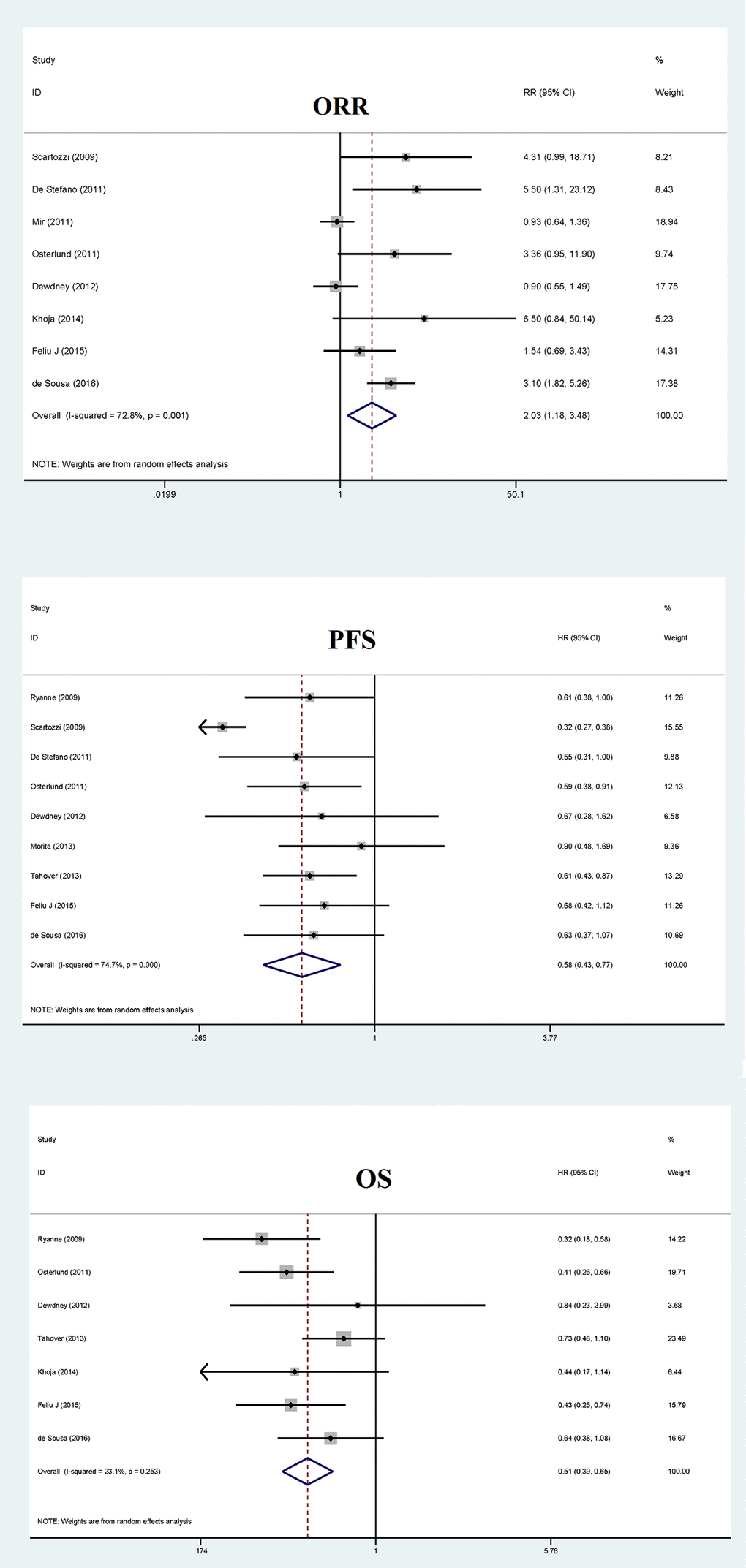
Figure 2. Overall forest plots of objective response rate (ORR), progression-free survival (PFS) and overall survival (OS) for bevacizumab-induced hypertension in patients with metastatic colorectal cancer.
Heterogeneity sources were explored using both subgroup analysis and meta-regression analysis. In subgroup analysis, bevacizumab dose, sample size and hypertension grade of controls may account for the presence of significant heterogeneity based on significant differences in stratified relative risk (Table 2). For example, when analysis was restricted to studies with hypertension grade 1/2 of controls, the risk of objective response rate for bevacizumab-induced hypertension was statistically significant (relative risk: 3.35, 95% CI: 2.06 – 5.44, p<0.001) and was not impacted by heterogeneity (I2: 0.0%), with the effect estimate over twice as much as that in studies with hypertension grade 0 in controls (relative risk: 1.47, 95% CI: 0.82 – 2.64, p=0.195, I2: 69.3%). Moreover, no significance was detected after dividing studies using the median cutoff value of total sample size at 77, in spite of divergent difference in risk estimates. In univariate meta-regression analysis, gender was identified as a significant source of heterogeneity for overall response rate (p=0.037).
Table 2. Subgroup analyses of response rates and survival outcomes for the presence of hypertension in bevacizumab-treated patients with metastatic colorectal cancer.
| Outcomes | Groups and subgroups | Studies | Sample size | RE | 95% CI | P value | I2 (%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ORR | Bevacizumab dose | RR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2.5 mg/kg/w | 1 | 119 | 0.93 | 0.64 – 1.36 | 0.716 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 mg/kg/2w | 2 | 118 | 3.22 | 1.95 – 5.30 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 mg/kg/2w or 7.5 mg/kg/3w | 2 | 175 | 4.17 | 1.61 – 10.77 | 0.003 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7.5 mg/kg/3w | 2 | 172 | 1.10 | 0.62 – 1.94 | 0.753 | 37.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension diagnosis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V2.0 | 2 | 166 | 2.13 | 0.83 – 5.46 | 0.115 | 31.8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V3.0 | 5 | 389 | 1.82 | 0.85 – 3.93 | 0.126 | 76.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V4.0 | 1 | 79 | 3.10 | 1.82 – 5.26 | <0.001 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension cut-off point in controls | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade 0 | 5 | 466 | 1.47 | 0.82 – 2.64 | 0.195 | 69.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade 1/2 | 3 | 168 | 3.35 | 2.06 – 5.44 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of patients | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| < 77 | 4 | 208 | 3.07 | 0.69 – 13.76 | 0.142 | 82.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 77 | 4 | 426 | 1.84 | 0.87 – 3.89 | 0.110 | 81.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PFS | Bevacizumab dose | HR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2.5 mg/kg/w | 1 | 181 | 0.61 | 0.43 – 0.87 | 0.006 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 mg/kg/2w | 3 | 178 | 0.54 | 0.27 – 1.06 | 0.075 | 86.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 mg/kg/2w or 7.5 mg/kg/3w | 2 | 175 | 0.58 | 0.41 – 0.82 | 0.002 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7.5 mg/kg/3w | 2 | 172 | 0.68 | 0.44 – 1.05 | 0.078 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension diagnosis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V2.0 | 2 | 166 | 0.45 | 0.21– 0.95 | 0.037 | 88.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V3.0 | 4 | 304 | 0.60 | 0.46 – 0.78 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V4.0 | 3 | 320 | 0.66 | 0.51 – 0.86 | 0.002 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension cut-off point in controls | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade 0 | 5 | 431 | 0.62 | 0.49 – 0.78 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade 1/2 | 4 | 359 | 0.55 | 0.33 – 0.77 | 0.021 | 86.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of patients | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| < 79 | 4 | 218 | 0.54 | 0.30 – 0.95 | 0.032 | 79.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 79 | 5 | 572 | 0.62 | 0.51 – 0.76 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OS | Bevacizumab dose | HR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2.5 mg/kg/w | 1 | 181 | 0.73 | 0.48 – 1.10 | 0.128 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 mg/kg/2w | 1 | 79 | 0.64 | 0.38 – 1.08 | 0.096 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 mg/kg/2w or 7.5 mg/kg/3w | 1 | 101 | 0.41 | 0.26 – 0.66 | <0.001 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7.5 mg/kg/3w | 2 | 172 | 0.47 | 0.29 – 0.79 | 0.004 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension diagnosis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V2.0 | 1 | 127 | 0.43 | 0.25 – 0.74 | 0.002 | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V3.0 | 4 | 280 | 0.40 | 0.29 – 0.56 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CTC AE V4.0 | 2 | 260 | 0.69 | 0.50 – 0.96 | 0.026 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension cut-off point in controls | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade 0 | 4 | 357 | 0.41 | 0.30 – 0.55 | <0.001 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade 1/2 | 3 | 310 | 0.66 | 0.49 – 0.90 | 0.008 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of patients | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| < 84 | 3 | 174 | 0.61 | 0.39 – 0.94 | 0.025 | 0.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥ 84 | 4 | 493 | 0.47 | 0.32 – 0.67 | <0.001 | 52.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: ORR: objective response rate; PFS: progression free survival; OS: overall survival; RE: risk estimate; 95% CI: 95% confidence interval; OR: odds ratio; HR: hazard ratio; I2: inconsistency index; CTC: common terminology criteria; AE: adverse events; NA: not available. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Publication bias was evaluated using both filled funnel plots (Figure 3) and Egger’s tests. Three missing studies were needed to ensure the symmetry of filled funnel plot, signaling a high probability of publication bias as reflected by Egger’s test (p=0.047). Analysis of incorporating the three missing studies showed that the unbiased relative risk of response rate was 1.55, which did not deviate significantly from 1 (95% CI: 0.95 – 2.54, p=0.081). Further cumulative meta-analysis indicated a stable trend in the risk estimates of objective response rate for bevacizumab-induced hypertension, as presented in Supplementary Figure S1.
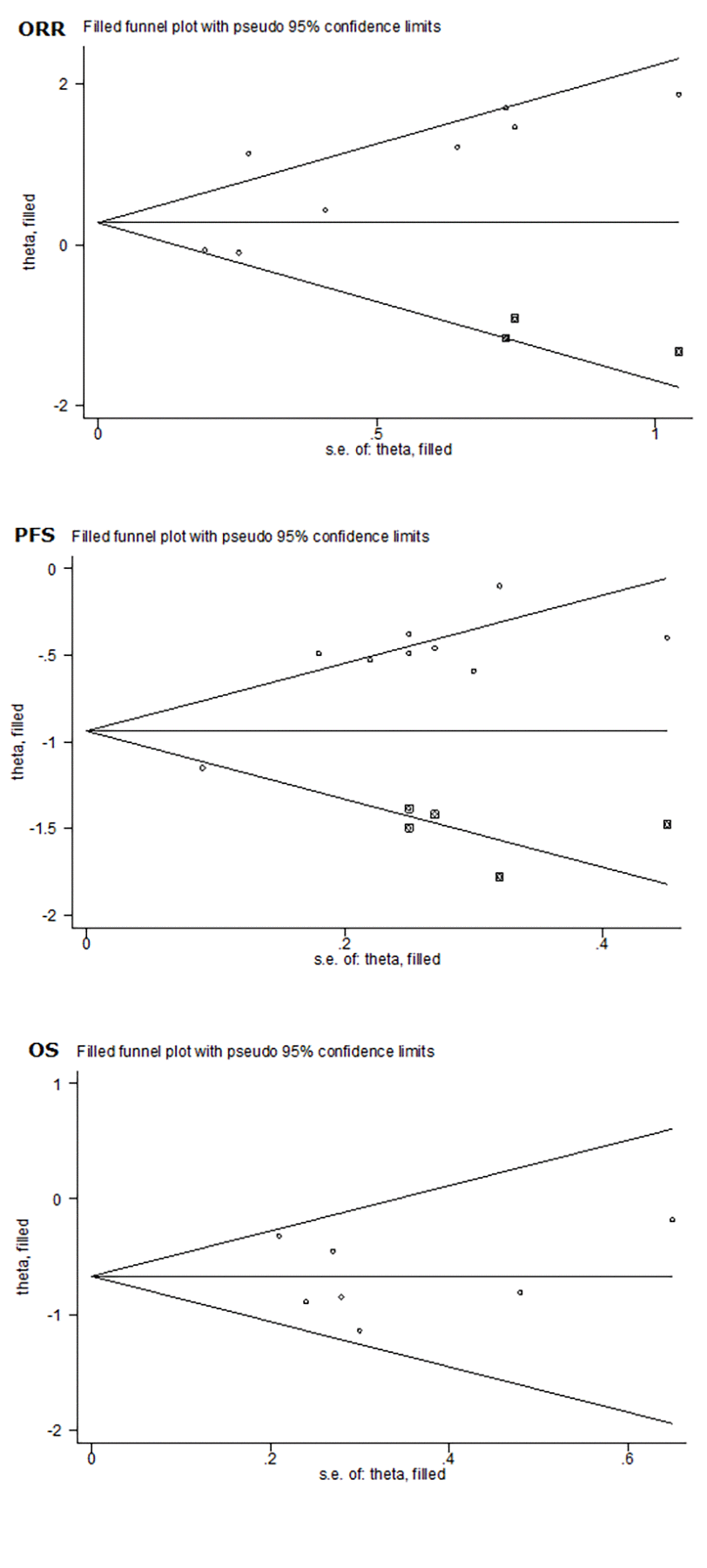
Figure 3. Overall funnel plots of objective response rate (ORR), progression-free survival (PFS) and overall survival (OS) for bevacizumab-induced hypertension in patients with metastatic colorectal cancer.
Progression-free survival
Analysis of all qualified studies showed that pooled hazard ratio of bevacizumab-induced hypertension for progression-free survival was 0.58 (95% CI: 0.43 – 0.77, p<0.001), with significant heterogeneity (I2: 74.7%) (Figure 2).
Subgroup analysis showed that hypertension grade of controls and sample size may confound the prediction of bevacizumab-induced hypertension in patients with metastatic colorectal cancer based on the differences in hazard ratio between subgroups (Table 2). The risk estimates were more obvious in subgroups with hypertension grade 0 in controls and with total sample size over the median cutoff value 79 of total sample size, and were not impacted by heterogeneity (both I2: 0.0%). In meta-regression analysis, age and gender were identified as significant confounders for the prediction of bevacizumab-induced hypertension for progression-free survival (p=0.011 and 0.002, respectively).
As shown in Figure 3, filled funnel plot for progression-free survival detected five potentially missing studies, and the associated Egger’s test was remarkably significant (p=0.001). After adjusting for the five missing studies, the hazard ratio of progression-free survival was still significant (hazard ratio: 0.52, 95% CI: 0.41 – 0.66, p<0.001). In cumulative meta-analysis, a stable trend in risk estimates was noted for progression-free survival (SSupplementary Figure S1).
Overall survival
The pooled hazard ratio for overall survival of bevacizumab-induced hypertension was 0.51 (95% CI: 0.39 – 0.65, p<0.001), and this estimate was not likely confounded by heterogeneity (I2: 23.1%), as presented in Figure 2. Subgroup analysis showed that sample size and hypertension grade of controls were possible causes of heterogeneity in view of the differences in hazard ratio between subgroups (Table 2). The risk estimates were reinforced when analysis was done using studies with hypertension grade 0 in controls (hazard ratio: 0.41, p<0.001) and with total sample size over the median cutoff value of total sample size at 84 (hazard ratio: 0.47, p<0.001). Meta-regression analysis showed that age and gender might be other causes of heterogeneity (p=0.024 and 0.015, respectively).
No missing study was reported by filled funnel plot in Figure 3, and no evidence of publication bias was detected by the Egger’s test (p=0.83). Risk estimates were stabilized in cumulative meta-analysis, as shown in SSupplementary Figure S1.
Trial sequential analysis
Finally, trial sequential analysis was employed to minimize random errors for objective response rate, progression-free survival and overall survival, respectively (Figure 4). The three cumulative z-curves were noticed to cross trial sequential monitoring boundaries prior to reaching the required information sizes, which suggested adequate cumulative evidence and the robustness of our conclusions.
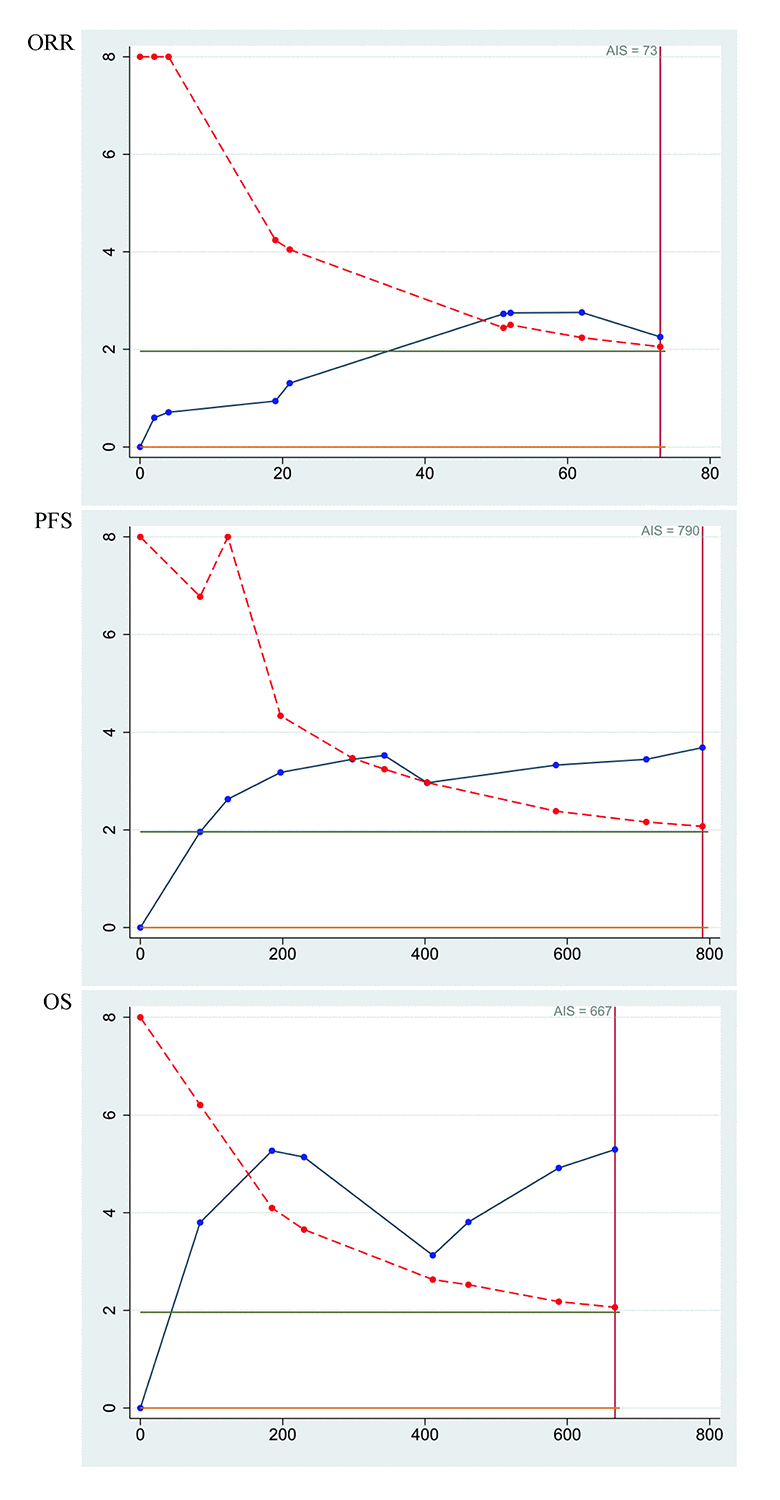
Figure 4. Trial sequential analysis of objective response rate (ORR), progression-free survival (PFS) and overall survival (OS) for bevacizumab-induced hypertension in patients with metastatic colorectal cancer.
Discussion
The aim of this present study was to update the results of two previous meta-analyses [16,17] by incorporating more studies and analyzing data more comprehensively. The key finding of this study was that bevacizumab-induced hypertension can significantly predict progress-free survival and overall survival in patients with metastatic colorectal cancer, whereas its prediction for objective response rate was nonsignificant. Moreover, our findings indicated that sample size and hypertension grade of controls, as well as age and gender, may be possible causes of between-study heterogeneity. To the authors’ knowledge, this study is thus far the largest report for gauging the usefulness of bevacizumab-induced hypertension in patients with metastatic colorectal cancer.
It is widely recognized that VEGF is a key mediator of angiogenesis and an effective biological target for patients with metastatic colorectal cancer, and its overexpression can accelerate tumor progression and metastatic spread of colorectal cancer [27,28]. Also, VEGF signaling cascade can lead to the suppression of nitric oxide production in endothelial cells, which, in turn, results in vasoconstriction and decrease in sodium renal excretion, with an ultimate end point of hypertension [29-32]. Bevacizumab is targeted at VEGF and blocks it from binding to its receptors, therefore impairing angiogenesis and detaining tumor growth and metastasis [33,34]. Hence, it is reasonable to propose that hypertension is a promising indicator for the clinical benefits of bevacizumab in treating patients with metastatic colorectal cancer.
Previously, two meta-analyses examined the validity of using hypertension to predict response rate and survival of patients with metastatic colorectal cancer, and both studies consistently demonstrated that bevacizumab-induced hypertension was associated with significant improvement in objective response rate, progression-free survival and overall survival [16,17]. Differing from the findings of two previous meta-analyses, we only confirmed the predictive role of bevacizumab-related hypertension in survival outcomes, and failed to manifest a significant contribution to objective response rate. The reasons behind this discrepancy may be multifold. One may be related to the inclusion criteria, as only articles published in English language were analyzed in this study, and by contrast the two previous meta-analyses involved two articles published in Japanese language. Another reason lied in the possible existence of publication bias, as our primary results in objective response rate were statistically significant, just as the two meta-analyses did, whereas the probability of publication bias was high and taking the impact of potential missing studies into consideration remarkably weakened the prediction of bevacizumab-induced hypertension for objective response rate. The third reason may be the insufficient power of previous studies, as we have replenished three new articles. The fourth reason may be due to unadjusted residual confounding, as our subgroup and meta-regression analyses indicated that bevacizumab dose, hypertension grade of controls, sample size and gender were possible causes of between-study heterogeneity. Importantly, the nonsignificant relationship between bevacizumab-induced hypertension and objective response rate was independent of the sample size involved, further supporting the claim that bevacizumab-induced hypertension may not be a predictor for objective response rate in patients with metastatic colorectal cancer.
Besides objective response rate, we have assessed the association of bevacizumab-induced hypertension with two survival outcomes. Consistent with the results of two previous studies, our findings consolidated the prognostic contribution of bevacizumab-induced hypertension to both progression-free survival and overall survival. However, extending the results of the two studies, we found that sample size and hypertension grade of controls, as well as age and gender, may be possible causes of between-study heterogeneity. In particular, after grouping studies per the median cutoff point of total sample size, the prediction of bevacizumab-induced hypertension for survival outcomes was more obvious when analysis was restricted to the large studies, indicating the robustness of our findings. In fact, the difference between progression-free survival and overall survival is whether the incorporation of patients who get worse. Just because of this difference, another aspect worth noting was that risk magnitude of overall survival was more obvious in studies with hypertension grade 0 of controls than studies with hypertension grade 1/2, whereas this situation was slightly reversed for that of progression-free survival. In other words, the protective effect of bevacizumab indexed by overall survival was more obvious for a lower grade of hypertension, whereas that by progression-free survival was more obvious for a higher grade of hypertension. Generally, the probability of tumor aggressiveness is higher during early treatment of bevacizumab for metastatic colorectal cancer than the late treatment. A higher grade of bevacizumab-induced hypertension may surrogate a longer treatment period. So the findings of this study further demonstrated the usefulness of using hypertension to signal bevacizumab treatment in metastatic colorectal cancer. Moreover, it is not surprising to notice that the prediction of bevacizumab-induced hypertension for survival outcomes was age- and gender-dependent. As evidenced, aging-related methylation can influence the gene expression of key control genes in colorectal cancer and adenoma [35], and hormone replacement therapy was significantly associated with reduced risk of colorectal cancer incidence and improved colorectal cancer-specific survival in female patients [36]. We agree that further studies are needed to obtain the biological proof and confirm the current findings.
Some limitations deserve special considerations for this meta-analysis. Firstly, only articles published in the English language were identified and the exclusion of gray literature from this meta-analysis can lead to the exaggerated estimates of intervention effectiveness [37]. Secondly, some subgroups involved a limited number of studies, and the probability of heterogeneity cannot be further interrogated. Thirdly, the overall sample size may not be sufficient enough to derive more accurate estimates. Fourthly, only the results of objective response rate, progression-free survival and overall survival were synthesized. Fifthly, data on genomic and epigenomic alterations were not available for us, because it is increasingly recognized that colorectal cancer is a molecularly heterogeneous disease. These alterations can help enhance our understanding of potential personalized therapies for molecularly specific colorectal cancer subtypes [38]. Finally, although we have statistically adjusted for potential missing studies, the jury must refrain from drawing a conclusion until future large, well-designed studies reproduce our findings.
Taken together, through a comprehensive analysis of 14 independent studies and 2292 study subjects, our findings indicate that bevacizumab-induced hypertension can predict progress-free survival and overall survival in patients with metastatic colorectal cancer, whereas its prediction for objective response rate was nonsignificant. Meanwhile, several issues from this meta-analysis remain to be clarified, and yet other areas warrant further investigation. If the usefulness of bevacizumab-induced hypertension were successfully validated in the future, it will be clinically important to administrate bevacizumab agents to patients with metastatic colorectal cancer who are more likely to benefit from the treatment.
Materials and Methods
Research guideline
The conduct of this meta-analysis was consistent with the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (SPRISMA checklist: Supplementary Table S1).
Search strategy
A systematic literature search was conducted in the following electronic bibliographic databases: PubMed (Medline), EMBASE (Excerpta Medica dataBASE) and Web of Science (Science Citation Index and Social Sciences Citation Index). Search strategy was expressed in the Boolean style, that is, (“colon” or “colorectal” or “rectal” or “rectum”) and (“cancer” or “tumor” or “tumour” or “carcinoma” or “neoplasm”) and (“bevacizumab” or “avastin”) and (“hypertension” or “blood pressure”). The literature search was completed on February 17, 2018. The reference lists of two previous meta-analyses [16,17] and retrieved major articles were also checked for potential missing hits. A final reference list of 632 articles was determined.
Selection criteria
Articles were retained for analysis pending the simultaneous satisfaction of following criteria: (i) metastatic colorectal cancer patients receiving bevacizumab treatment were grouped according to the presence or severity of hypertension determined by the Common Terminology Criteria for Adverse Events (CTC AE); (ii) information on objective response rate or its associated odds ratio, or hazard ratio for progression-free survival or overall survival, or survival curves was available for extraction or inference; (iii) articles were written in the English language. Meanwhile, conference abstract, case report or case series, review or meta-analysis, basic medical research and phase I clinical trial were not included in this study.
Two investigators (Chun-Jing Zhang and Shu-Ying Zhang) of this present study independently assessed the eligibility of all potential articles according to above criteria. A third investigator (Hai-Tao Yu) solved the disagreements, if exist, from literature screening.
Data extraction
The following variables were extracted from each eligible article: the first author’s surname, published year, country where study was conducted, CTC AE version, combined chemotherapy, bevacizumab dose, age, gender, metastatic position of metastatic colorectal cancer, objective response rate, progression-free survival, overall survival, odds ratio (95% CI) and hazard ratio (95% CI). Survival rate was used to estimate progression-free survival or overall survival from survival curves in case of no available risk estimates by aid of the Engauge Digitizer software Release 4.0.
Data extraction was independently completed by two investigators (Chun-Jing Zhang and Shu-Ying Zhang) of the present study, and a third investigator (Hai-Tao Yu) checked table entries for accuracy by referring to original context.
Trial sequential analysis
According to a previous publication [39], trial sequential analysis was performed to calculate the simple accrued information size after assuming a significance level of 5% for type I error and 20% for type II error. In addition, a monitoring boundary was also generated in trial sequential analysis.
Statistical analysis
Odds ratio and its 95% CI for objective response rate, as well as hazard ratio and its 95% CI for progression-free survival or overall survival were calculated between metastatic colorectal cancer patients with and without bevacizumab-induced hypertension.
From a statistical standpoint, in the absence of between-study heterogeneity, effect estimates based on the fixed-effects model and the random-effects model are exactly the same, whereas in the presence of heterogeneity, effect estimates are more reliable based on the random-effects model, relative to the fixed-effects model. Thus, in this meta-analysis, random-effects model using the DerSimonian & Laird method [40,41] was used for effect estimates.
Between-study heterogeneity was quantified using the inconsistency index (I2) on the basis of the Cochrane Q-test. Heterogeneity is reported to be low if I2 ranges from 0% to 25%, moderate from 25% to 75% and high from 75% to 100% [42].
Regardless of the magnitude of heterogeneity, subgroup analysis and meta-regression analysis were conducted to assess the impact of categorical and continuous study variables on the overall heterogeneity.
The presence of publication bias, the bias resulting from the possibly unpublished studies due to the negative results or extreme deviations from previous results, was visually appraised by filled funnel plots. The statistical evidence of publication bias was assessed by the Egger’s test, a weighted regression test that can help justify the asymmetry of funnel plots. In case of evident publication bias, a trim and fill method was employed to derive an unbiased estimate after considering potentially missing studies. In addition, to evaluate whether later studies impacted previous studies, a cumulative meta-analysis was conducted accordingly.
Above statistical analyses were completed using the STATA/SE software Release 11.2.
Supplementary Materials
Author Contributions
H.T.Y conceived and designed the experiments; C.J.Z and S.Y.Z performed the experiments; C.J.Z and C.D.Z analyzed the data; C.D.Z, C.R.L. X.Y.L and Q.Y.L contributed materials/analysis tools; C.J.Z and H.T.Y wrote the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
This study was supported by the Natural Science Foundation of Heilongjiang Province, China (Grant Nos. LC2011C34 and ZD2016020).
References
- 1. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017; 66:683–91. https://doi.org/10.1136/gutjnl-2015-310912 [PubMed]
- 2. Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007; 18:581–92. https://doi.org/10.1093/annonc/mdl498 [PubMed]
- 3. Shah SA, Haddad R, Al-Sukhni W, Kim RD, Greig PD, Grant DR, Taylor BR, Langer B, Gallinger S, Wei AC. Surgical resection of hepatic and pulmonary metastases from colorectal carcinoma. J Am Coll Surg. 2006; 202:468–75. https://doi.org/10.1016/j.jamcollsurg.2005.11.008 [PubMed]
- 4. Bhome R, Goh RW, Bullock MD, Pillar N, Thirdborough SM, Mellone M, Mirnezami R, Galea D, Veselkov K, Gu Q, Underwood TJ, Primrose JN, De Wever O, et al. Exosomal microRNAs derived from colorectal cancer-associated fibroblasts: role in driving cancer progression. Aging (Albany NY). 2017; 9:2666–94. [PubMed]
- 5. Van Cutsem E, Cervantes A, Nordlinger B, Arnold D, and ESMO Guidelines Working Group. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014 (Suppl 3); 25:iii1–9. https://doi.org/10.1093/annonc/mdu260 [PubMed]
- 6. Ma J, Yang QL, Ling Y. Rechallenge and maintenance therapy using cetuximab and chemotherapy administered to a patient with metastatic colorectal cancer. BMC Cancer. 2017; 17:132. https://doi.org/10.1186/s12885-017-3133-8 [PubMed]
- 7. Yamaguchi K, Taniguchi H, Komori A, Narita Y, Nitta S, Nomura M, Kadowaki S, Takahari D, Ura T, Andoh M, Muro K, Mori K, Igarashi Y. A single-arm phase II trial of combined chemotherapy with S-1, oral leucovorin, and bevacizumab in heavily pre-treated patients with metastatic colorectal cancer. BMC Cancer. 2015; 15:601. https://doi.org/10.1186/s12885-015-1606-1 [PubMed]
- 8. Price TJ, Peeters M, Kim TW, Li J, Cascinu S, Ruff P, Suresh AS, Thomas A, Tjulandin S, Zhang K, Murugappan S, Sidhu R. Panitumumab versus cetuximab in patients with chemotherapy-refractory wild-type KRAS exon 2 metastatic colorectal cancer (ASPECCT): a randomised, multicentre, open-label, non-inferiority phase 3 study. Lancet Oncol. 2014; 15:569–79. https://doi.org/10.1016/S1470-2045(14)70118-4 [PubMed]
- 9. Gallagher DJ, Kemeny N. Metastatic colorectal cancer: from improved survival to potential cure. Oncology. 2010; 78:237–48. https://doi.org/10.1159/000315730 [PubMed]
- 10. Dionísio de Sousa IJ, Ferreira J, Rodrigues J, Bonito N, Jacinto P, Marques M, Ribeiro J, Pais A, Gervásio H. Association between bevacizumab-related hypertension and response to treatment in patients with metastatic colorectal cancer. ESMO Open. 2016; 1:e000045. https://doi.org/10.1136/esmoopen-2016-000045 [PubMed]
- 11. Raouf S, Bridgewater J, Ellis R, Ferry D, Hill M, Wasan H. Use of bevacizumab in the treatment of metastatic colorectal cancer. Br J Hosp Med (Lond). 2012; 73:25–30. https://doi.org/10.12968/hmed.2012.73.1.25 [PubMed]
- 12. de Sousa IJ, Ferreira J, Rodrigues J, Bonito N, Jacinto P, Marques M, Ribeiro J, Pais A, Gervasio H. Association between bevacizumabrelated hypertension and response to treatment in patients with metastatic colorectal cancer. ESMO Open. 2016; 1.
- 13. Feliu J, Salud A, Safont MJ, García-Girón C, Aparicio J, Losa F, Bosch C, Escudero P, Casado E, Jorge M, Bohn U, Pérez-Carrión R, Carmona A, et al. Correlation of hypertension and proteinuria with outcome in elderly bevacizumab-treated patients with metastatic colorectal cancer. PLoS One. 2015; 10:e0116527. https://doi.org/10.1371/journal.pone.0116527 [PubMed]
- 14. Tahover E, Uziely B, Salah A, Temper M, Peretz T, Hubert A. Hypertension as a predictive biomarker in bevacizumab treatment for colorectal cancer patients. Med Oncol. 2013; 30:327. https://doi.org/10.1007/s12032-012-0327-4 [PubMed]
- 15. Österlund P, Soveri LM, Isoniemi H, Poussa T, Alanko T, Bono P. Hypertension and overall survival in metastatic colorectal cancer patients treated with bevacizumab-containing chemotherapy. Br J Cancer. 2011; 104:599–604. https://doi.org/10.1038/bjc.2011.2 [PubMed]
- 16. Cai J, Ma H, Huang F, Zhu D, Bi J, Ke Y, Zhang T. Correlation of bevacizumab-induced hypertension and outcomes of metastatic colorectal cancer patients treated with bevacizumab: a systematic review and meta-analysis. World J Surg Oncol. 2013; 11:306. https://doi.org/10.1186/1477-7819-11-306 [PubMed]
- 17. Chen C, Sun P, Ye S, Weng HW, Dai QS. Hypertension as a predictive biomarker for efficacy of bevacizumab treatment in metastatic colorectal cancer: a meta-analysis. J BUON. 2014; 19:917–24. [PubMed]
- 18. Ryanne Wu R, Lindenberg PA, Slack R, Noone AM, Marshall JL, He AR. Evaluation of hypertension as a marker of bevacizumab efficacy. J Gastrointest Cancer. 2009; 40:101–08. https://doi.org/10.1007/s12029-009-9104-9 [PubMed]
- 19. Scartozzi M, Galizia E, Chiorrini S, Giampieri R, Berardi R, Pierantoni C, Cascinu S. Arterial hypertension correlates with clinical outcome in colorectal cancer patients treated with first-line bevacizumab. Ann Oncol. 2009; 20:227–30. https://doi.org/10.1093/annonc/mdn637 [PubMed]
- 20. De Stefano A, Carlomagno C, Pepe S, Bianco R, De Placido S. Bevacizumab-related arterial hypertension as a predictive marker in metastatic colorectal cancer patients. Cancer Chemother Pharmacol. 2011; 68:1207–13. https://doi.org/10.1007/s00280-011-1604-1 [PubMed]
- 21. Mir O, Coriat R, Cabanes L, Ropert S, Billemont B, Alexandre J, Durand JP, Treluyer JM, Knebelmann B, Goldwasser F. An observational study of bevacizumab-induced hypertension as a clinical biomarker of antitumor activity. Oncologist. 2011; 16:1325–32. https://doi.org/10.1634/theoncologist.2010-0002 [PubMed]
- 22. Dewdney A, Cunningham D, Barbachano Y, Chau I. Correlation of bevacizumab-induced hypertension and outcome in the BOXER study, a phase II study of capecitabine, oxaliplatin (CAPOX) plus bevacizumab as peri-operative treatment in 45 patients with poor-risk colorectal liver-only metastases unsuitable for upfront resection. Br J Cancer. 2012; 106:1718–21. https://doi.org/10.1038/bjc.2012.152 [PubMed]
- 23. Budai B, Nagy T, Láng I, Hitre E. The use of high dose d,l-leucovorin in first-line bevacizumab+mFOLFIRI treatment of patients with metastatic colorectal cancer may enhance the antiangiogenic effect of bevacizumab. Angiogenesis. 2013; 16:113–21. https://doi.org/10.1007/s10456-012-9303-z [PubMed]
- 24. Hurwitz HI, Douglas PS, Middleton JP, Sledge GW, Johnson DH, Reardon DA, Chen D, Rosen O. Analysis of early hypertension and clinical outcome with bevacizumab: results from seven phase III studies. Oncologist. 2013; 18:273–80. https://doi.org/10.1634/theoncologist.2012-0339 [PubMed]
- 25. Morita S, Uehara K, Nakayama G, Shibata T, Oguri T, Inada-Inoue M, Shimokata T, Sugishita M, Mitsuma A, Ando Y. Association between bevacizumab-related hypertension and vascular endothelial growth factor (VEGF) gene polymorphisms in Japanese patients with metastatic colorectal cancer. Cancer Chemother Pharmacol. 2013; 71:405–11. https://doi.org/10.1007/s00280-012-2028-2 [PubMed]
- 26. Khoja L, Kumaran G, Zee YK, Murukesh N, Swindell R, Saunders MP, Clamp AR, Valle JW, Wilson G, Jayson GC, Hasan J. Evaluation of hypertension and proteinuria as markers of efficacy in antiangiogenic therapy for metastatic colorectal cancer. J Clin Gastroenterol. 2014; 48:430–34. [PubMed]
- 27. Des Guetz G, Uzzan B, Nicolas P, Cucherat M, Morere JF, Benamouzig R, Breau JL, Perret GY. Microvessel density and VEGF expression are prognostic factors in colorectal cancer. Meta-analysis of the literature. Br J Cancer. 2006; 94:1823–32. https://doi.org/10.1038/sj.bjc.6603176 [PubMed]
- 28. Jürgensmeier JM, Schmoll HJ, Robertson JD, Brooks L, Taboada M, Morgan SR, Wilson D, Hoff PM. Prognostic and predictive value of VEGF, sVEGFR-2 and CEA in mCRC studies comparing cediranib, bevacizumab and chemotherapy. Br J Cancer. 2013; 108:1316–23. https://doi.org/10.1038/bjc.2013.79 [PubMed]
- 29. Tanaka M, Abe K, Oka M, Saku K, Yoshida K, Ishikawa T, McMurtry IF, Sunagawa K, Hoka S, Tsutsui H. Inhibition of nitric oxide synthase unmasks vigorous vasoconstriction in established pulmonary arterial hypertension. Physiol Rep. 2017; 5:e13537. https://doi.org/10.14814/phy2.13537 [PubMed]
- 30. Seo YS, Shah VH. Pathophysiology of portal hypertension and its clinical links. J Clin Exp Hepatol. 2011; 1:87–93. https://doi.org/10.1016/S0973-6883(11)60127-8 [PubMed]
- 31. Weissmann N. VEGF receptor inhibition as a model of pulmonary hypertension in mice. Am J Respir Crit Care Med. 2011; 184:1103–05. https://doi.org/10.1164/rccm.201109-1662ED [PubMed]
- 32. Longo A, Casuccio A, Pani L, Avitabile T, Cillino S, Uva MG, Bonfiglio V, Russo A, Parisi G, Cennamo G, Furino C, Parravano M, Xoxi E, Reibaldi M. Association of neovascular age-related macular degeneration with month and season of birth in Italy. Aging (Albany NY). 2016; 9:133–41. https://doi.org/10.18632/aging.101137 [PubMed]
- 33. Vasudev NS, Reynolds AR. Anti-angiogenic therapy for cancer: current progress, unresolved questions and future directions. Angiogenesis. 2014; 17:471–94. https://doi.org/10.1007/s10456-014-9420-y [PubMed]
- 34. Chen CT, Hung MC. Beyond anti-VEGF: dual-targeting antiangiogenic and antiproliferative therapy. Am J Transl Res. 2013; 5:393–403. [PubMed]
- 35. Galamb O, Kalmár A, Barták BK, Patai AV, Leiszter K, Péterfia B, Wichmann B, Valcz G, Veres G, Tulassay Z, Molnár B. Aging related methylation influences the gene expression of key control genes in colorectal cancer and adenoma. World J Gastroenterol. 2016; 22:10325–40. https://doi.org/10.3748/wjg.v22.i47.10325 [PubMed]
- 36. Symer MM, Wong NZ, Abelson JS, Milsom JW, Yeo HL. Hormone Replacement Therapy and Colorectal Cancer Incidence and Mortality in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Clin Colorectal Cancer. 2018; 17:e281–88. https://doi.org/10.1016/j.clcc.2018.01.003 [PubMed]
- 37. McAuley L, Pham B, Tugwell P, Moher D. Does the inclusion of grey literature influence estimates of intervention effectiveness reported in meta-analyses? Lancet. 2000; 356:1228–31. https://doi.org/10.1016/S0140-6736(00)02786-0 [PubMed]
- 38. Inamura K. Colorectal Cancers: An Update on Their Molecular Pathology. Cancers (Basel). 2018; 10:E26. https://doi.org/10.3390/cancers10010026 [PubMed]
- 39. Fu W, Zhuo ZJ, Chen YC, Zhu J, Zhao Z, Jia W, Hu JH, Fu K, Zhu SB, He J, Liu GC. NFKB1 -94insertion/deletion ATTG polymorphism and cancer risk: evidence from 50 case-control studies. Oncotarget. 2017; 8:9806–22. [PubMed]
- 40. DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. 2015; 45:139–45. https://doi.org/10.1016/j.cct.2015.09.002 [PubMed]
- 41. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986; 7:177–88. https://doi.org/10.1016/0197-2456(86)90046-2 [PubMed]
- 42. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557–60. https://doi.org/10.1136/bmj.327.7414.557 [PubMed]