



Introduction
Major depressive disorder (MDD), the second leading cause of disability worldwide, affects about 6.7% of the US population aged 18 years and older in any given calendar year and poses a huge burden on public health and economics [1]. MDD is a major contributor to suicide [2] and has been associated with excess morbidity and mortality [3-5]. Depression also constitutes a significant health problem in the American Indian community [6,7]. Based on a survey conducted in 2006, American Indians/Alaska Natives experienced a much higher rate of major depressive episodes compared to Caucasians (12.1% vs. 7.8%) [8]. Unraveling the molecular mechanisms underlying depression is the key to lead to novel diagnostic or therapeutic strategies for this debilitating disorder and its co-morbidities.
Telomeres are repetitive DNA sequences on the distal ends of the chromosomes. They are critical in maintaining chromosomal stability during mitotic cell division. Telomere length shortens progressively during each round of cell division and declines significantly with age, thus providing a biomarker for biological aging. Shorter leukocyte telomere length (LTL) has been associated with a wide range of aging-related disorders, such as diabetes, cardiovascular disease, and cancer [9-13]. Among American Indians participating in the Strong Heart Family Study (SHFS), our group has also reported associations of shorter LTL with diabetes [14], carotid atherosclerosis [15], obesity [16], and arterial aging [17].
Previous studies have suggested a strong link between depression, aging and aging-related disorders. For instance, depressed individuals have increased risk for cognitive aging [18], Alzheimer’s disease [19], cardiovascular disease [20], diabetes [21], obesity [22], as well as cancer [23]. In addition, a few studies have reported an association of telomere length with depression, although these studies had relatively small sample size and were largely conducted in Caucasian populations [24,25]. We are not aware of prior studies examining the association between LTL and depression in a sample of American Indians. Given that both LTL and depression are genetically determined, the relationship between depression may be racially/ethnical specific [26]. In addition, there is support in the literature that women are two times as likely to be diagnosed with depressive disorders than men [27,28]. However, it is unclear whether the association between depression and telomere length differs by gender. As such, the goals of this study were to examine the relationship between depressive symptoms and LTL, and to test whether gender modulates this association in a group of American Indians, a population that experiences high rates of both depression and aging-related disorders.
Results
Characteristics of study participants
Table 1 shows the characteristics of the study participants. Nearly 50% of the study participants reported mild or more severe depressive symptoms with the Center for Epidemiologic Studies of Depression Scale (CES-D) score ≥ 10. Compared to women, men were younger, had lower body mass index (BMI), were physically more active, and more likely to be current drinkers. Moreover, men had lower CES-D scores and a lower rate of antidepressant drug use compared to women. There were no significant differences in the education level and current smoking rate between men and women.
Table 1. Characteristics of study participants
| Total (N=2,175) | Men (N=847) | Women (N=1,328) | P value* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years | 40.4 (17.0) | 39.2 (16.9) | 41.1 (17.0) | 0.0060 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education (high school or higher), % | 10.3 | 9.3 | 11.0 | 0.1553 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, kg/m2 | 31.3 (7.5) | 30.6 (7.0) | 31.8 (7.7) | 0.0010 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker, % | 36.4 | 36.7 | 36.1 | 0.6721 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current drinker, % | 58.0 | 65.7 | 53.1 | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical activity, steps/d | 5845.3 (3899.9) | 7150.9 (4321.4) | 5059.3 (3390.0) | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LTL (T/S ratio ) | 0.994 (0.239) | 0.983 (0.237) | 1.000 (0.239) | 0.0266 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CES-D score | 12.1 (10.2) | 10.3 (8.4) | 13.2 (11.0) | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Categories of depressive symptoms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CES-D < 10 (none), % | 50.2 | 56.6 | 46.1 | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 10 ≤ CES-D < 16 (mild) , % | 21.9 | 22.3 | 21.7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 16 ≤ CES-D ≤ 24 (moderate) , % | 15.6 | 13.9 | 16.7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CES-D > 24 (severe) , % | 12.3 | 7.2 | 15.5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antidepressant drug use, % | 5.2 | 1.9 | 7.2 | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: BMI, body mass index; LTL, leukocyte telomere length. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data are presented as mean (standard deviation) or percentage. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *P values for differences between men and women; correlation among family members was corrected by GEE. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Association between traditional risk factors and LTL
Table 2 presents the age-adjusted associations of several risk factors with LTL. It shows that LTL was significantly and inversely associated with age (P < 0.0001) and BMI (P < 0.0001). Men had shorter LTL compared to women (P =0.0035). We did not observe associations of education level, smoking, drinking, and physical activity with LTL in our study population.
Table 2. Association of LTL with traditional risk factors in American Indians in the SHFS
| Variable | β (SE)* | P value* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | -0.0048 (0.0005) | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Men | -0.0308 (0.0106) | 0.0035 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education (high school or higher) | 0.0207 (0.0191) | 0.2790 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | -0.0024 (0.0006) | < 0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 0.0020 (0.0085) | 0.8121 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current drinker | -0.0155 (0.0114) | 0.1723 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical activity | 0.0006 (0.0043)† | 0.8803 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: BMI, body mass index; LTL, leukocyte telomere length. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| * Results of multivariate GEE, adjusting for age, sites, male sex, education, body mass index, current smoking, current drinking, and physical activity. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| † Associated with 1-standard deviation increase in steps per day. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Association between depressive symptoms and LTL
Table 3 shows the multivariate-adjusted LTL (95% CI) across the four categories of severity for depressive symptoms. After adjusting for age, gender, and education, individuals with more severe depressive symptoms had a significantly shorter LTL (Model 1: P for trend = 0.0322). The association between depressive symptoms and LTL remained statistically significant after further adjustments for lifestyle factors (Model 2: P for trend = 0.0356), or antidepressant uses and chronic conditions (Model 3: P for trend = 0.0278).
Table 3. Multivariate association between LTL and severity of depressive symptoms in American Indians in the SHFS (N=2,175)
| Model * | Multivariate-adjusted LTL (95% CI) | P for trend | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| None CES-D < 10 (N=1,091) | Mild 10 ≤ CES-D < 16 (N=477) | Moderate 16 ≤ CES-D ≤ 24 (N=340) | Severe CES-D > 24 (N=267) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 1: Age, gender, site, and education | 0.974 (0.948, 1.000) | 0.964 (0.937, 0.991) | 0.963 (0.932,0.995) | 0.942 (0.912,0.973) | 0.0322 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 2: Age, gender, site, education, BMI, smoking, drinking, and physical activity | 0.987 (0.962, 1.012) | 0.986 (0.959, 1.013) | 0.976 (0.943, 1.009) | 0.955 (0.925, 0.986) | 0.0356 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 3: Age, gender, site, education, BMI, smoking, drinking, physical activity, use of antidepressants, and presence/absence of chronic diseases | 1.000 (0.967, 1.033) | 0.999 (0.965, 1.032) | 0.988 (0.957, 1.020) | 0.966 (0.932, 1.001) | 0.0278 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: BMI, body mass index; LTL, leukocyte telomere length. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Correlation among family members was adjusted in all three GEE models. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Gender difference in the association between depressive symptoms and LTL
We identified a significant interactive effect between gender and severe depressive symptoms on LTL (Table 4). Even after adjusting for all covariates, men with severe depressive symptoms (CES-D > 24) had significant shorter LTL than those without (CES-D ≤ 24), whereas no significant association was found in women (Figure 1). In a fully adjusted model (Model 3), LTL were 1.0048 (95% CI: 0.9224, 1.0872) and 0.9301 (95% CI: 0.8425, 1.0178) for men with and without severe depressive symptoms, respectively (P = 0.0021). In women, LTL were 1.0059 (95% CI: 0.9224, 1.0872) and 0.9886 (95% CI: 0.9534, 1.0237) for individuals with and without severe depressive symptoms, respectively (P = 0.2244).
Table 4. Gender-specific association between LTL and severe depressive symptoms (CES-D > 24)
| Model* | Men | Women | P value for interaction between gender and severe depressive symptoms | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β (SE) | P value | β (SE) | P value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 1: Age, site, and education | -0.0653 (0.0210) | 0.0019 | -0.0147 (0.0138) | 0.2872 | 0.0469 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 2: Age, site, education, BMI, smoking, drinking, and physical activity | -0.0724 (0.0245) | 0.0031 | -0.0168 (0.0142) | 0.2375 | 0.0329 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Model 3: Age, site, education, BMI, smoking, drinking, physical activity, use of antidepressants, and presence/absence of chronic diseases | -0.0746 0.0243) | 0.0021 | -0.0173 (0.0142) | 0.2244 | 0.0346 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: BMI, body mass index; LTL, leukocyte telomere length. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Correlation among family members was adjusted in GEE models. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
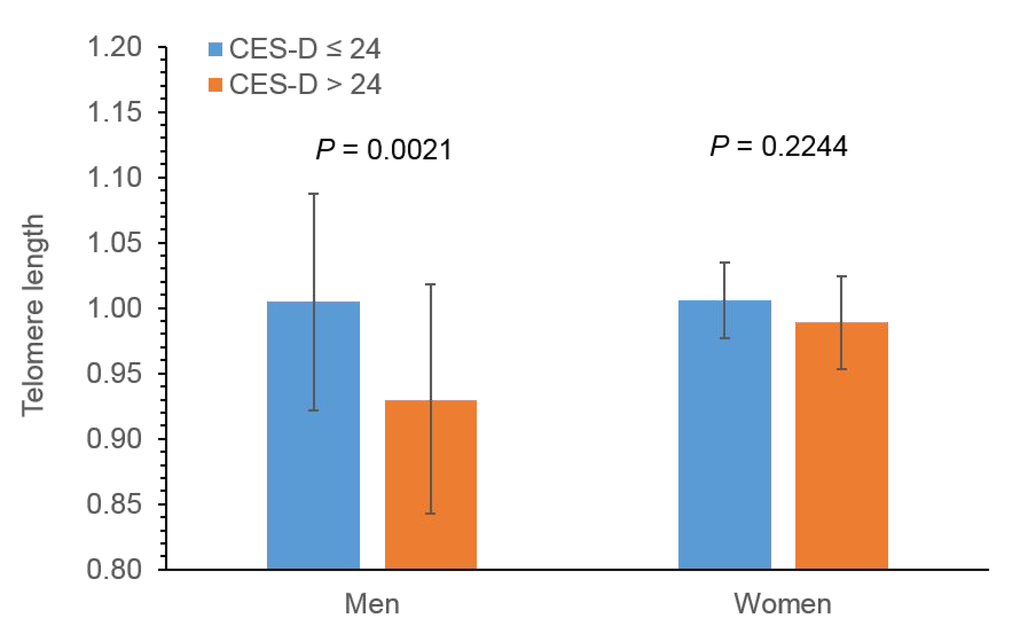
Figure 1. Sex-specific effect of severe depressive symptoms on LTL in American Indians.P-values were adjusted for age, site, education, BMI, smoking, drinking, physical activity, use of antidepressants chronic conditions, study sites using GEE.
Discussion
This study provides initial evidence for an association between depressive symptoms and LTL in a large sample of geographically diverse American Indians. We found that a higher level of depressive symptoms was significantly associated with shorter LTL, independent of many known risk factors. Moreover, gender appears to modulate the relationship between severe depressive symptoms and LTL. Specifically, severe depressive symptoms were associated with shortened LTL in men, but not in women.
Several previous studies have investigated the relationship between MDD and LTL [24,25]. For example, MDD was found to be significantly associated with shortened telomere length in a study comprising 15 MDD patients and 44 nondepressed controls [29], but this association was unable to be replicated in another cross-sectional study comprising 1,164 participants [30]. The relationship between depressive symptoms and LTL was also reported in other studies. However, those studies were largely conducted in Caucasians and results were inconsistent [24,25]. Given that both LTL and MDD are under genetic control [26], results identified in Caucasians are unlikely to be generalized to American Indians. American Indians may have different risk profiles from the Caucasian population. To date, little is known about the relationship between depression and telomeres in American Indians. In a large sample of American Indians, here we provide initial evidence that is supporting a relationship between depressive symptoms and accelerated cellular aging. Moreover, there appears a dose-response relationship between the severity of depressive symptoms and LTL, with participants with more severe depressive symptoms exhibiting shorter LTL in our study population.
While the precise mechanisms linking depression to LTL shortening remain to be determined, it is possible that depression could contribute to shortened LTL through one or more biological pathways known to be involved in depression, such as inflammation [31,32], oxidative stress [33,34], hyperactivity of the hypothalamic-pituitary-adrenal axis [35,36], and increased activity of the autonomic nervous system [37,38]. It has been demonstrated that depression is accompanied by oxidative stress dysregulation, including increased levels of free radicals and oxidative damage products as well as decreased levels of antioxidants [34]. Meanwhile, oxidative stress could induce the formation of 8-oxodG at the GGG triplet in telomere sequence. Human 8-oxodG-DNA glycosylase introduces a chain break in a double-stranded oligonucleotide specifically at an 8-oxodG residue, leading to telomere shortening [39]. These lines of evidence support the hypothesis that aforementioned dysregulations accumulated in depression may mediate its effect on telomere attrition.
Our analysis revealed a gender difference in the association between depressive symptoms and shortened LTL. The effect of severe depressive symptoms on LTL was much stronger in men than in women. This finding appears to be consistent with a recent study showing that depression was associated with LTL in men, but not in women [40]. Despite the fact that women are more likely to be depressed than men, there has been evidence that men with mental disorders tend to have worse outcomes than women [41–43]. For example, in a cohort of Netherlands, men with minor depression defined by CES-D ≥ 16 had a 1.8-fold higher risk of death during follow-up than non-depressed men. However, minor depression did not significantly increase mortality risk in women [41]. According to a national survey of the US, the hazard ratios for all-cause mortality associated with major depression were 3.1 and 1.7 for men and women, respectively [42]. The mechanisms underlying this gender difference are unknown. It is possible that estrogens may play a role in these observed gender differences because they have been implicated in increasing the activity of telomerase [44]. Further research is needed to confirm this gender-specific association and to elucidate the potential role of estrogens in the association.
The major strengths of our study include a large sample size, the high-quality telomere and clinical data, as well as the sophisticated statistical models with extensive adjustments of known covariables. However, some limitations of this study should also be discussed. First, as all cross-sectional studies, the causal relationship between depressive symptoms and shortened telomere length could not be determined in our analysis. Second, due to lack of fresh blood samples, we did not measure the activity of telomerase, which may mediate the effect of depressive symptoms on telomere length. Third, as our study participants were exclusively American Indians, our results may not be generalized to other ethnic groups. And lastly, although our sample size in this study is considerable, American Indians are a very geographically and culturally diverse group of people. In the US, there are over 550 recognized tribal groups; therefore this study may also be limited in its applicability or generalization to American Indians throughout the population of the US.
Nonetheless, in this large epidemiological study of American Indians, we provide the first evidence that depressive symptoms were associated with shorter LTL, independent of many known risk factors. The effect of severe depressive symptoms on accelerated telomere shortening could be more prominent in men than in women. These findings need to be replicated in large-scale populations of different races/ethnicities. Longitudinal studies are warranted to establish the causal relationship between depression and telomere erosion in future investigations.
Methods
Study subjects
The current study included a total of 2,175 American Indians (847 men and 1,328 women) participating in the SHFS, a family-based prospective study of genetic, metabolic, and behavioral factors for cardiovascular disease (CVD), diabetes, and their risk factors. The SHFS participants were recruited from 12 tribes residing in Arizona, Oklahoma, and South/North Dakota in 2001-2003. A detailed description of the study design and methods of the SHFS has been reported previously [45]. In brief, information on demographic factors, socioeconomic status, lifestyle factors, medical history, and medication use was collected by personal interview using standard questionnaires. A physical examination was conducted and fasting blood samples were collected for laboratory tests. The SHFS study protocol was approved by the Institutional Reviews Boards from the Indian Health Service and the participating centers. All subjects gave informed consent.
LTL measurement
Genomic DNA from peripheral blood was isolated according to standard methods. The LTL measurements were performed by Dr. Blackburn’s laboratory at the University of California, San Francisco using a high-throughput telomere length assay system. The LTL assay determines the ratio of telomeric product (T) to a single copy gene (S) obtained using quantitative polymerase chain reaction (qPCR) according to protocols described previously [46,47]. The rationale of this method is that the longer the telomeres are in each sample, the more PCR product will be generated in PCR reactions using primers specific for the telomeric DNA. The T/S ratio reflects the average length of the telomeres. For quality control, seven control DNA samples from various cancer cell lines were included in each assay plate. These control samples allowed us to create standard curves, which were then integrated into a composite standard curve used for T and S concentration calculations. In addition, 4.1% of the total sample was assayed in duplicate. Telomere length of the replicate samples were highly correlated (r = 0.95, P<0.0001). Lab technicians were blinded to any knowledge of clinical data. In our analysis, the intra-assay coefficient of variation was 4.6% and the inter-assay coefficient of variation (assay-to-assay) was 6.9%.
Assessment of depressive symptoms
In the SHFS, we assessed depressive symptoms using the CES-D, which comprised of 20 items and was administered as a self-report instrument [48]. The CES-D has been widely used in large-scale epidemiological studies, such as the Honolulu Heart Program, the Inter-Tribal Heart Project, Coronary Artery Risk Development in Young Adults, and the Stanford Coronary Prevention Project [49]. It has also been used in studies including American Indians with good internal consistency [50-52].
The CES-D was designed to measure the current level of depressive symptoms [48]. The 20 items represent all major components of depressive symptoms, including depressed mood, feeling of guilt and worthlessness, feeling of helplessness and hopelessness, loss of appetite, sleep disturbance, and psychomotor retardation. The 20 items were rated on a four-point Likert scale, ranging from “rarely, or not at all,” scored as 0, to “most of the time,” scored as 3. Four positively worded items were reversed when scored. Item scores were then summed for a total depression score with higher scores indicating increased reported depressive symptoms. Depressive symptoms were categorized into four levels: none (CES-D < 10), mild (10 ≤ CES-D < 16), moderate (16 ≤ CES-D ≤ 24), and severe (CES-D > 24). These cut-offs have been widely used in previous epidemiological studies [48,49].
Assessments of covariates
BMI was calculated as weight divided by squared height (kg/m2). Current smokers were defined as who reported smoking 100 or more cigarettes in their lifetime and were currently smoking every day or some days. Current drinkers were those who had consumed any alcohol during the past year [53]. The level of physical activity was assessed by the average steps per day during a 7-day step recording by a pedometer. Information on diagnosis and treatment of CVD, diabetes, hypertension, and chronic kidney disease was also collected.
Statistical analyses
To examine the association between depressive symptoms and LTL, we constructed multivariate hierarchical generalized estimating equation (GEE) models in which continuous LTL (T/S ratio) was the dependent variable and severity of depressive symptoms (categorized into none, mild, moderate, severe) was the independent variable: Model 1, adjusted for sociodemographic factors (age, gender, and education); Model 2, additionally adjusted for lifestyle factors (BMI, smoking, drinking, and physical activity); and Model 3, further adjusted for antidepressant use (yes/no), and presence or absence of chronic conditions (CVD, diabetes, hypertension, and chronic kidney disease). The GEE model was used to account for the correlations among family members. To examine whether gender modulates the association between depressive symptoms and LTL, we included an interaction term of gender and the categorical variable for depressive symptoms in the GEE models. Gender-stratified analyses were also conducted if any interaction term was significant. All analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC).
Acknowledgements
The authors would also like to thank the Strong Heart Study participants, Indian Health Service facilities, and participating tribal communities for their extraordinary cooperation and involvement, which has contributed to the success of the Strong Heart Study. The views expressed in this article are those of the authors and do not necessarily reflect those of the Indian Health Service.
Conflicts of Interest
No potential conflicts of interest relevant to this article were reported.
Funding
This study was supported by NIH grants R01DK091369, K01AG034259, R21HL092363 and cooperative agreement grants U01-HL-65520, U01-HL-41642, U01-HL-41652, U01-HL-41654, and U01-HL-65521.
References
- 1. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005; 62:617–27. https://doi.org/10.1001/archpsyc.62.6.617 [PubMed]
- 2. Ferrari AJ, Charlson FJ, Norman RE, Patten SB, Freedman G, Murray CJ, Vos T, Whiteford HA. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013; 10:e1001547. https://doi.org/10.1371/journal.pmed.1001547 [PubMed]
- 3. Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR, Nemeroff CB, Bremner JD, Carney RM, Coyne JC, Delong MR, Frasure-Smith N, Glassman AH, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry. 2005; 58:175–89. https://doi.org/10.1016/j.biopsych.2005.05.001 [PubMed]
- 4. Everson-Rose SA, House JS, Mero RP. Depressive symptoms and mortality risk in a national sample: confounding effects of health status. Psychosom Med. 2004; 66:823–30. https://doi.org/10.1097/01.psy.0000145903.75432.1f [PubMed]
- 5. Gump BB, Matthews KA, Eberly LE, Chang YF, Group MR, and MRFIT Research Group. Depressive symptoms and mortality in men: results from the Multiple Risk Factor Intervention Trial. Stroke. 2005; 36:98–102. https://doi.org/10.1161/01.STR.0000149626.50127.d0 [PubMed]
- 6. Urban Indian Health Institute. Addressing depression among American Indians and Alaska Natives: a literature review. 2012. .
- 7. Finkbonner B. Depression in American Indians and Alaska Natives: A review of Indian Health Service Policy and Services. 2002. .
- 8. The 2006 National Survey on Drug Use and Health: National Findings. Rockville, MD. http://www.samhsa.gov. 2007.
- 9. Zhao J, Zhu Y, Lin J, Matsuguchi T, Blackburn E, Zhang Y, Cole SA, Best LG, Lee ET, Howard BV. Short Leukocyte Telomere Length Predicts Risk of Diabetes in American Indians: The Strong Heart Family Study. Diabetes. 2014; 63:354–62 https://doi.org/10.2337/db13-0744 [PubMed]
- 10. Salpea KD, Talmud PJ, Cooper JA, Maubaret CG, Stephens JW, Abelak K, Humphries SE. Association of telomere length with type 2 diabetes, oxidative stress and UCP2 gene variation. Atherosclerosis. 2010; 209:42–50. https://doi.org/10.1016/j.atherosclerosis.2009.09.070 [PubMed]
- 11. Serrano AL, Andrés V. Telomeres and cardiovascular disease: does size matter? Circ Res. 2004; 94:575–84. https://doi.org/10.1161/01.RES.0000122141.18795.9C [PubMed]
- 12. Blasco MA. Telomeres and human disease: ageing, cancer and beyond. Nat Rev Genet. 2005; 6:611–22. https://doi.org/10.1038/nrg1656 [PubMed]
- 13. Willeit P, Willeit J, Mayr A, Weger S, Oberhollenzer F, Brandstätter A, Kronenberg F, Kiechl S. Telomere length and risk of incident cancer and cancer mortality. JAMA. 2010; 304:69–75. https://doi.org/10.1001/jama.2010.897 [PubMed]
- 14. Zhao J, Zhu Y, Lin J, Matsuguchi T, Blackburn E, Zhang Y, Cole SA, Best LG, Lee ET, Howard BV. Short leukocyte telomere length predicts risk of diabetes in american indians: the strong heart family study. Diabetes. 2014; 63:354–62. https://doi.org/10.2337/db13-0744 [PubMed]
- 15. Chen S, Lin J, Matsuguchi T, Blackburn E, Yeh F, Best LG, Devereux RB, Lee ET, Howard BV, Roman MJ, Zhao J. Short leukocyte telomere length predicts incidence and progression of carotid atherosclerosis in American Indians: the Strong Heart Family Study. Aging (Albany NY). 2014; 6:414–27. https://doi.org/10.18632/aging.100671 [PubMed]
- 16. Chen S, Yeh F, Lin J, Matsuguchi T, Blackburn E, Lee ET, Howard BV, Zhao J. Short leukocyte telomere length is associated with obesity in American Indians: the Strong Heart Family study. Aging (Albany NY). 2014; 6:380–89. https://doi.org/10.18632/aging.100664 [PubMed]
- 17. Peng H, Zhu Y, Yeh F, Cole SA, Best LG, Lin J, Blackburn E, Devereux RB, Roman MJ, Lee ET, Howard BV, Zhao J. Impact of biological aging on arterial aging in American Indians: findings from the Strong Heart Family Study. Aging (Albany NY). 2016; 8:1583–92. [PubMed]
- 18. McDermott LM, Ebmeier KP. A meta-analysis of depression severity and cognitive function. J Affect Disord. 2009; 119:1–8. https://doi.org/10.1016/j.jad.2009.04.022 [PubMed]
- 19. Green RC, Cupples LA, Kurz A, Auerbach S, Go R, Sadovnick D, Duara R, Kukull WA, Chui H, Edeki T, Griffith PA, Friedland RP, Bachman D, Farrer L. Depression as a risk factor for Alzheimer disease: the MIRAGE Study. Arch Neurol. 2003; 60:753–59. https://doi.org/10.1001/archneur.60.5.753 [PubMed]
- 20. Charlson FJ, Stapelberg NJ, Baxter AJ, Whiteford HA. Should global burden of disease estimates include depression as a risk factor for coronary heart disease? BMC Med. 2011; 9:47. https://doi.org/10.1186/1741-7015-9-47 [PubMed]
- 21. Mezuk B, Eaton WW, Albrecht S, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care. 2008; 31:2383–90. https://doi.org/10.2337/dc08-0985 [PubMed]
- 22. Luppino FS, de Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, Zitman FG. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 2010; 67:220–29. https://doi.org/10.1001/archgenpsychiatry.2010.2 [PubMed]
- 23. Penninx BW, Guralnik JM, Pahor M, Ferrucci L, Cerhan JR, Wallace RB, Havlik RJ. Chronically depressed mood and cancer risk in older persons. J Natl Cancer Inst. 1998; 90:1888–93. https://doi.org/10.1093/jnci/90.24.1888 [PubMed]
- 24. Schutte NS, Malouff JM. The association between depression and leukocyte telomere length: a meta-analysis. Depress Anxiety. 2015; 32:229–38. https://doi.org/10.1002/da.22351 [PubMed]
- 25. Ridout KK, Ridout SJ, Price LH, Sen S, Tyrka AR. Depression and telomere length: A meta-analysis. J Affect Disord. 2016; 191:237–47. https://doi.org/10.1016/j.jad.2015.11.052 [PubMed]
- 26. Zhu Y, Voruganti VS, Lin J, Matsuguchi T, Blackburn E, Best LG, Lee ET, MacCluer JW, Cole SA, Zhao J. QTL mapping of leukocyte telomere length in American Indians: the Strong Heart Family Study. Aging (Albany NY). 2013; 5:704–16. https://doi.org/10.18632/aging.100600 [PubMed]
- 27. Piccinelli M, Wilkinson G. Gender differences in depression. Critical review. Br J Psychiatry. 2000; 177:486–92. https://doi.org/10.1192/bjp.177.6.486 [PubMed]
- 28. Barrett EL, Richardson DS. Sex differences in telomeres and lifespan. Aging Cell. 2011; 10:913–21. https://doi.org/10.1111/j.1474-9726.2011.00741.x [PubMed]
- 29. Simon NM, Smoller JW, McNamara KL, Maser RS, Zalta AK, Pollack MH, Nierenberg AA, Fava M, Wong KK. Telomere shortening and mood disorders: preliminary support for a chronic stress model of accelerated aging. Biol Psychiatry. 2006; 60:432–35. https://doi.org/10.1016/j.biopsych.2006.02.004 [PubMed]
- 30. Needham BL, Mezuk B, Bareis N, Lin J, Blackburn EH, Epel ES. Depression, anxiety and telomere length in young adults: evidence from the National Health and Nutrition Examination Survey. Mol Psychiatry. 2015; 20:520–28. https://doi.org/10.1038/mp.2014.89 [PubMed]
- 31. Stewart JC, Rand KL, Muldoon MF, Kamarck TW. A prospective evaluation of the directionality of the depression-inflammation relationship. Brain Behav Immun. 2009; 23:936–44. https://doi.org/10.1016/j.bbi.2009.04.011 [PubMed]
- 32. Carrero JJ, Stenvinkel P, Fellström B, Qureshi AR, Lamb K, Heimbürger O, Bárány P, Radhakrishnan K, Lindholm B, Soveri I, Nordfors L, Shiels PG. Telomere attrition is associated with inflammation, low fetuin-A levels and high mortality in prevalent haemodialysis patients. J Intern Med. 2008; 263:302–12. https://doi.org/10.1111/j.1365-2796.2007.01890.x [PubMed]
- 33. von Zglinicki T. Oxidative stress shortens telomeres. Trends Biochem Sci. 2002; 27:339–44. https://doi.org/10.1016/S0968-0004(02)02110-2 [PubMed]
- 34. Liu T, Zhong S, Liao X, Chen J, He T, Lai S, Jia Y. A Meta-Analysis of Oxidative Stress Markers in Depression. PLoS One. 2015; 10:e0138904. https://doi.org/10.1371/journal.pone.0138904 [PubMed]
- 35. Pariante CM, Lightman SL. The HPA axis in major depression: classical theories and new developments. Trends Neurosci. 2008; 31:464–68. https://doi.org/10.1016/j.tins.2008.06.006 [PubMed]
- 36. Tomiyama AJ, O’Donovan A, Lin J, Puterman E, Lazaro A, Chan J, Dhabhar FS, Wolkowitz O, Kirschbaum C, Blackburn E, Epel E. Does cellular aging relate to patterns of allostasis? An examination of basal and stress reactive HPA axis activity and telomere length. Physiol Behav. 2012; 106:40–45. https://doi.org/10.1016/j.physbeh.2011.11.016 [PubMed]
- 37. Carney RM, Freedland KE, Veith RC. Depression, the autonomic nervous system, and coronary heart disease. Psychosom Med. 2005 (Suppl 1); 67:S29–33. https://doi.org/10.1097/01.psy.0000162254.61556.d5 [PubMed]
- 38. Epel ES, Lin J, Wilhelm FH, Wolkowitz OM, Cawthon R, Adler NE, Dolbier C, Mendes WB, Blackburn EH. Cell aging in relation to stress arousal and cardiovascular disease risk factors. Psychoneuroendocrinology. 2006; 31:277–87. https://doi.org/10.1016/j.psyneuen.2005.08.011 [PubMed]
- 39. Kawanishi S, Oikawa S. Mechanism of telomere shortening by oxidative stress. Ann N Y Acad Sci. 2004; 1019:278–84. https://doi.org/10.1196/annals.1297.047 [PubMed]
- 40. Shalev I, Moffitt TE, Braithwaite AW, Danese A, Fleming NI, Goldman-Mellor S, Harrington HL, Houts RM, Israel S, Poulton R, Robertson SP, Sugden K, Williams B, Caspi A. Internalizing disorders and leukocyte telomere erosion: a prospective study of depression, generalized anxiety disorder and post-traumatic stress disorder. Mol Psychiatry. 2014; 19:1163–70. https://doi.org/10.1038/mp.2013.183 [PubMed]
- 41. Penninx BW, Geerlings SW, Deeg DJ, van Eijk JT, van Tilburg W, Beekman AT. Minor and major depression and the risk of death in older persons. Arch Gen Psychiatry. 1999; 56:889–95. https://doi.org/10.1001/archpsyc.56.10.889 [PubMed]
- 42. Zheng D, Macera CA, Croft JB, Giles WH, Davis D, Scott WK. Major depression and all-cause mortality among white adults in the United States. Ann Epidemiol. 1997; 7:213–18. https://doi.org/10.1016/S1047-2797(97)00014-8 [PubMed]
- 43. Chang CK, Hayes RD, Broadbent M, Fernandes AC, Lee W, Hotopf M, Stewart R. All-cause mortality among people with serious mental illness (SMI), substance use disorders, and depressive disorders in southeast London: a cohort study. BMC Psychiatry. 2010; 10:77. https://doi.org/10.1186/1471-244X-10-77 [PubMed]
- 44. Bayne S, Jones ME, Li H, Liu JP. Potential roles for estrogen regulation of telomerase activity in aging. Ann N Y Acad Sci. 2007; 1114:48–55. https://doi.org/10.1196/annals.1396.023 [PubMed]
- 45. North KE, Howard BV, Welty TK, Best LG, Lee ET, Yeh JL, Fabsitz RR, Roman MJ, MacCluer JW. Genetic and environmental contributions to cardiovascular disease risk in American Indians: the strong heart family study. Am J Epidemiol. 2003; 157:303–14. https://doi.org/10.1093/aje/kwf208 [PubMed]
- 46. Cawthon RM. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002; 30:e47. https://doi.org/10.1093/nar/30.10.e47 [PubMed]
- 47. Lin J, Epel E, Cheon J, Kroenke C, Sinclair E, Bigos M, Wolkowitz O, Mellon S, Blackburn E. Analyses and comparisons of telomerase activity and telomere length in human T and B cells: insights for epidemiology of telomere maintenance. J Immunol Methods. 2010; 352:71–80. https://doi.org/10.1016/j.jim.2009.09.012 [PubMed]
- 48. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977; 1:385–401. https://doi.org/10.1177/014662167700100306
- 49. Calhoun D, Beals J, Carter EA, Mete M, Welty TK, Fabsitz RR, Lee ET, Howard BV. Relationship between glycemic control and depression among American Indians in the Strong Heart Study. J Diabetes Complications. 2010; 24:217–22. https://doi.org/10.1016/j.jdiacomp.2009.03.005 [PubMed]
- 50. Somervell PD, Beals J, Kinzie JD, Boehnlein J, Leung P, Manson SM. Criterion validity of the Center for Epidemiologic Studies Depression Scale in a population sample from an American Indian village. Psychiatry Res. 1993; 47:255–66. https://doi.org/10.1016/0165-1781(93)90083-S [PubMed]
- 51. Dick RW, Beals J, Keane EM, Manson SM. Factorial Structure of the CES-D among American Indian alolescents. J Adolesc. 1994; 17:73–79. https://doi.org/10.1006/jado.1994.1007
- 52. Manson SM, Ackerson LM, Dick RW, Baron AE, Fleming CM. Depressive Symptomes among American Indian Adolescents: Psychometric Characteristics of the Center for Epidemiologic Studies Depression Scale (CES-D). Psychol Assess. 1990; 2:231–37. https://doi.org/10.1037/1040-3590.2.3.231
- 53. Fretts AM, Howard BV, Kriska AM, Smith NL, Lumley T, Lee ET, Russell M, Siscovick D. Physical activity and incident diabetes in American Indians: the Strong Heart Study. Am J Epidemiol. 2009; 170:632–39. https://doi.org/10.1093/aje/kwp181 [PubMed]